

Abstract
Background
Trials have demonstrated the efficacy of rigorous diet and physical activity promotion (D&PA) programs for adults at increased risk for type 2 diabetes to reduce diabetes incidence and improve measures of glycemia.
Purpose
To evaluate D&PA programs for individuals at increased risk for type 2 diabetes primarily to lower diabetes risk, lower body weight, and improve glycemia.
Data Sources
MEDLINE, Cochrane Central Register of Controlled Trials, CAB Abstracts, Global Health, and Ovid HealthStar from 1991 through 27 February 2015, with no language restriction.
Study Selection
8 researchers screened articles for single group or comparative studies of combined D&PA programs with at least 2 sessions of at least 3 month duration in participants at increased risk for type 2 diabetes.
Data Extraction
7 researchers extracted data—on study design, participant, intervention, outcome descriptions, and results—and assessed study quality.
Data Synthesis
53 studies (30 D&PA vs. control, 13 more vs. less intensive, 13 in single programs) evaluated 66 programs. Compared with usual care, D&PA reduced type 2 diabetes incidence (RR = 0.59; 95% CI 0.51, 0.66; 16 studies), lowered body weight (net change = −2.2%; 95% CI −2.9, −1.4; 24 studies) and fasting blood glucose (net change = −0.12 mmol/L; 95% CI −0.20, −0.05; 17 studies), and improved other cardiometabolic risk factors. There was limited evidence for clinical events. More intensive programs were more effective.
Limitations
The wide variation in D&PA programs limited identification of features most relevant to effectiveness. Evidence on clinical outcomes and in children was sparse.
Conclusions
Combined D&PA promotion programs are effective to decrease diabetes incidence and improve cardiometabolic risk factors for patients at increased risk. More intensive programs are more effective.
Primary Funding Source
Centers for Disease Control and Prevention Community Preventive Services Task Force.
Keywords: pre-diabetes, type 2 diabetes, diet, exercise, primary prevention
Diabetes is a large and growing medical problem and the costs to society are high and escalating. According to the latest figures from the Centers for Disease Control and Prevention (CDC), 29.1 million people or 9.3% of the U.S. population have diabetes and 1.7 million new cases are diagnosed annually (1). Worldwide, it is estimated that 387 million adults are living with diabetes and this number is projected to increase to 592 million by 2035 (2). Prevalence of diabetes and related costs are expected to more than double in the next quarter century (3), as more than 86 million Americans (37% of the adult population) are at risk of developing diabetes (1). Effective prevention strategies are, therefore, critically important to slow the diabetes tide and its associated burden.
Nearly 9 out of 10 new cases of diabetes are due to type 2 diabetes, whose natural history is characterized by a gradual rise in glycemia. Identifying those at increased risk can allow the implementation of interventions to lower the risk of progressing to clinical diabetes. The American Diabetes Association has defined pre-diabetes as a high-risk category, based on a level of glycemia that does not meet criteria for diabetes but is too high to be considered normal (4). People with pre-diabetes progress to type 2 diabetes at a rate of about 5–10% per year without any intervention (5). Three large clinical trials from the US (6), Finland (7), and China (8) have shown that the main components of diabetes prevention in adults are weight loss and increased physical activity. In these trials, among people at risk for type 2 diabetes, rigorous application of combined diet and physical activity (D&PA) promotion programs, with the goals of weight loss and increased physical activity were successful at reducing risk of diabetes by 50–60% during the active intervention period (3 to 6 years). Although attenuated, the effect of the intervention can persist long-term (9–11). The results of these trials are well known; however, wide-scale implementation in clinical and community-based settings has recently begun, but requires further progress (12).
Combined D&PA promotion programs aim to prevent type 2 diabetes among people who are at increased risk for the disease. These programs actively encourage people to improve their diet and increase their physical activity using trained providers in various settings who work with clients for at least 3 months, providing some combination of counseling, coaching, and extended support in multiple sessions related to diet and physical activity, delivered in-person, or by other methods. Programs may also include numerous other features, including specialized counselors, a range of number and frequency of sessions, different session types, and different diet, weight loss, or exercise goals.
The purpose of this review was to assess the effectiveness of D&PA promotion programs implemented in a wide range of clinical or community settings to reduce risk of new-onset diabetes among adults and children at risk for type 2 diabetes. The Community Preventive Services Task Force (Task Force, www.thecommunityguide.org) used this review to update its guidance in diabetes prevention and to identify current gaps in the evidence to inform future research. Potential effect modifiers such as intensity and specificity of the programs, settings and implementers were evaluated. Furthermore, the potential benefit of the diabetes prevention programs extending to other cardiometabolic risk factors, such as overweight, high cholesterol and high blood pressure, was also assessed.
Methods
The review was conducted in accordance with the methodology of the Task Force (13;14) and the highest standards for conducting systematic reviews (15;16). We convened a panel of domain experts and stakeholders (Coordination Team), which together with our Community Guide Technical Monitor and Task Force members provided input regarding the protocol, feedback on the findings, conclusions, and evidence gaps.
Data Sources
We searched MEDLINE, the Cochrane Central Register of Controlled Trials, CAB Abstracts, Global Health, and Ovid HealthStar from 1991 through 27 February 2015 with no language restrictions. Supplemental Table 1 shows the search strategy. We also screened through reference lists of related systematic and narrative reviews, and suggestions from the expert panel.
Study Selection
We included randomized controlled trials and prospective non-randomized comparative studies with at least 30 participants per group, and prospective single group intervention studies with at least 100 participants. The population of interest was focused on adults or children at increased risk for type 2 diabetes (i.e., with pre-diabetes) as determined by glycemia measures or diabetes risk assessment tools. We included studies of participants with metabolic syndrome (who are at increased risk of both diabetes and cardiovascular disease) or whose participants were chosen because they were at risk for either type 2 diabetes or cardiovascular disease. However, we excluded studies of participants with established type 2 diabetes or whose only risk factor was obesity or increased risk for cardiovascular disease (without explicit inclusion of participants with pre diabetes). The implied or explicit intent of the D&PA programs had to be to prevent diabetes and had to include at least 2 contact sessions (in-person or virtually) over a minimum period of 3 months. Programs had to include both dietary and increased physical activity components and could be conducted in any outpatient setting. We allowed any type of advice to improve diet and increase physical activity (except single food or supplement dietary changes such as adding fish oil). We excluded interventions that included antidiabetic medications. The comparative studies had to include a usual care arm (no active D&PA program) or a lower-intensity D&PA program (e.g., with fewer contact sessions or a more liberal diet). We required at least 6 month follow-up for any of the following outcomes: incident diabetes, reversion to normoglycemia, body weight, glycemia measures (fasting glucose [FG], 2 hour glucose after a 75-gram oral glucose tolerance test [2hG], hemoglobin A1c [HbA1c]), all-cause death, diabetes-related clinical outcomes (e.g., cardiovascular events, end-stage renal disease, nephropathy, amputation, retinopathy, neuropathy, skin ulcers, periodontitis), blood pressure (BP), and lipids (total cholesterol, low and high density lipoprotein cholesterol [LDL, HDL], and triglycerides).
Data Extraction and Quality Assessment
We screened titles and abstracts using Abstrackr (17). Eight researchers double-screened the abstracts after iterative training of all reviewers on the same batches of abstracts. Discordant decisions and queries were resolved at group meetings. Full-text articles were retrieved for all potentially relevant abstracts and rescreened by the same researchers.
Each study was extracted by one of seven experienced methodologists and confirmed by a senior methodologist; the same methodologists assessed study quality. Data extraction was conducted in SRDR (18), and included elements for study design including eligibility criteria, population characteristics, detailed descriptions of the D&PA programs and comparison interventions, outcomes, and results. We assessed each study’s quality based on 12 Community Guide quality of execution questions (Supplemental Table 2, footnotes) (14;19). Per Community Guide protocol, we excluded studies with “limited quality of execution,” defined as having at least five major limitations.
Data Synthesis and Analysis
All extracted data were tabulated into Summary Evidence Tables (available in the Supporting Materials at the URL listed at the beginning of the Results section). Because only two studies were conducted in children, we report these separately and do not include them in the meta-analyses. For outcomes with data from at least three comparative studies of D&PA vs. usual care, we performed profile likelihood random effects model meta-analysis of risk ratio (RR) or net change (20). For non-randomized studies, we preferentially used adjusted analysis results. Meta-analyses were conducted with the metaan package in Stata 13.1 (StataCorp, College Station, TX). For the overall meta-analyses of incident diabetes and reversion to normoglycemia, we used the longest reported duration of follow-up data. For continuous outcomes, we used the data closest to 1 year of follow-up, data restricted to <2 years of follow-up, and longest followup. We evaluated differences in effect (for incident diabetes and weight only) based on any direct comparisons of different D&PA programs within studies, any reported within-study subgroup analyses, and across-study random effects model metaregression across all D&PA programs based on predetermined study setting and D&PA program features. Incident diabetes and weight change were chosen for metaregression based on their relative importance in determining the effectiveness of D&PA programs. Metaregressions were conducted with the metareg package in Stata and were considered to be potentially significant if P<0.10. For each outcome with at least 10 studies, the possibility of publication bias was examined with funnel plots and the Harbord test for diabetes incidence and the Egger test for continuous outcomes using the metabias and metafunnel packages in Stata (21).
Role of the Funding Source
One member of the Coordination Team and our Technical Monitor are employed by the CDC; none of the Task Force members are. The Coordination Team, Technical Monitor, and members of the Community Preventive Services Task Force participated in formulating the study questions and developing the protocol but did not participate in the literature search, determination of study eligibility criteria, data analysis or interpretation. The Coordination Team, Technical Monitor, and CDC personnel were provided with an opportunity to provide feedback on the manuscript and the decision to submit the manuscript for publication, but the research team retained final determination of the content and decision to publish.
Results
Supplemental Figure 1 summarizes the search yield. Of 11,317 citations (plus articles from other existing systematic reviews and domain experts), 53 studies described 66 D&PA programs in 104 articles (6–11;22–119). One additional study was excluded for limited quality of execution (with six major limitations) (120). The included studies described 26 randomized and 4 nonrandomized comparisons of D&PA programs versus usual care, 12 randomized and 1 nonrandomized comparisons of two or more D&PA programs (3 of which also had usual care arms), and 13 single group studies of D&PA programs. Thirty-three studies were of good quality (0 to 1 limitation) and 20 were of fair quality (2 to 4 limitations) (Supplemental Table 2). The most common limitations were poor descriptions of the study populations or intervention programs; problems with data measurement or interpretation; and high dropout rates. While half the studies (n=27) analyzed all enrolled participants, nine had more than 20% drop-out (or loss-to-follow-up) rates.
The characteristics of the D&PA programs are summarized in Table 1 (with details in (Supplemental Tables 3–5). All but five programs (in four studies) ran for at least 6 months. Programs offered a wide range of number of contact sessions (0 [virtual contacts only] to 72, median 15) and most programs included both a core period (with frequent contact sessions) and a maintenance period (when participants were contacted less frequently). With the exception of seven programs that were delivered entirely over the internet, by video, telephone, or email, programs used in-person individual or group sessions, or both, on diet or exercise, or both. Sessions were led by different combinations of trained diet counselors including dietitians, nutritionists, or others; trained exercise counselors including physical trainers or others; nurses; physicians or psychologists; or trained laypeople. Many programs included specific weight loss, diet, or physical activity goals (Table 1). Some programs included individually tailored plans for diet and physical activity.
Table 1.
Characteristics of Combined Diet and Physical Activity Promotion Programs
| Category, No. Programs/Studies | Characteristic | Median (IQI) [Range] or No. of Programs (%) |
|---|---|---|
| No. sessions, 67 programs | Core | 10 (6–16) [0*–72] |
| Maintenance, 28 programs | 6 (1.5–12) [0*–24] | |
| Total | 15 (6.5–24.5) [0*–72]] | |
| Program duration, 67 programs | Core | 6 mo (5–12) [1–60] |
| Maintenance, 28 programs | 12 (7–18) [4–68] | |
| Total | 12 mo (10–27) [3–72] | |
| Program design†, 67 programs | Nominally based on DPP or DPS | 27 (40%) |
| Weight loss goal†, 67 programs | 42 (63%) | |
| Diet intervention†, 67 programs | Individual sessions | 40 (60%) |
| Group sessions | 41 (61%) | |
| Individual and group | 24 (36%) | |
| Individually tailored diet plan | 16 (24%) | |
| Diet goal | 19 (28%) | |
| Diet counselor | 29 (43%) | |
| Physical activity intervention†, 67 programs | Individual sessions | 41 (61%) |
| Group sessions | 39 (58%) | |
| Individual and group | 24 (36%) | |
| Individually tailored exercise plan | 23 (34%) | |
| Exercise goal | 32 (48%) | |
| Exercise counselor | 18 (27%) | |
| Counselors†, 51 programs | Dietitian | 37 (73%) |
| Exercise therapist | 26 (51%) | |
| Nurse | 15 (29%) | |
| Layperson | 13 (25%) | |
| Physician | 8 (16%) | |
| Diabetes educator | 3 (6%) | |
| Country, 53 studies | U.S. / Canada | 22 (42%) |
| Western Europe/Australia | 22 (42%) | |
| Japan | 3 (6%) | |
| Middle income‡ | 6 (11%) | |
| Setting, 41 studies | Community | 12 (29%) |
| Healthcare system | 25 (61%) | |
| Worksite | 0 | |
| Multiple | 4 (10%) | |
| Location, 53 studies | Urban | 25 (47%) |
| Regional | 21 (40%) | |
| Suburban | 2 (4%) | |
| Rural | 1 (2%) | |
| Mixed | 4 (8%) |
DPP = U.S. Diabetes Prevention Program Trial, DPS = Finnish Diabetes Prevention Study, IQI = interquartile interval, mo = months.
In some programs, the contacts were by telephone, email, internet, or video only.
Likely underestimates due to inadequate or unclear reporting in articles.
India 3, Brazil 1, China 1, Pakistan 1.
Table 2 summarizes the patient characteristics (with details in Supplemental Table 6). Thirty (57%) studies were restricted to participants with prediabetes, of which 21 studies used standard diagnostic criteria; 12 (23%) studies included only participants at increased risk of diabetes based on a risk score. More than three-quarters of studies included mostly overweight or obese participants and most study participants were female and at least middle-aged. Two studies were conducted in adolescents at increased risk of type 2 diabetes. These two studies are analyzed separately. None of the studies reported any long-term harms directly related to the D&PA programs.
Table 2.
Characteristics of Study Participants
| Category, No. Studies | Characteristic | Median (IQI) [Range] or No. of Studies (%) |
|---|---|---|
| Eligibility criteria, 53 studies | Prediabetes, IGT, or IFG | 30 (57%) |
| By ADA/WHO criteria | 21 (40%) | |
| At increased risk for DM (by risk score) | 12 (23%) | |
| Prediabetes or at increased risk for DM | 4 (8%) | |
| Prediabetes or at increased risk for CVD | 4 (8%) | |
| Metabolic syndrome ± prediabetes | 3 (6%) | |
| Body weight, 47 studies | Mean BMI, kg/m2 | 31.2 (28.1, 33.6) [23.8, 39.7] |
| Hypertension, 4 studies | % participants | 34.5 [30.6, 50] |
| Female, 39 studies | % participants | 65.3 (50.3, 73.9) [13.5, 90.5] |
| Age, 39 studies† | Mean years | 53.6 (48, 57) [43.1, 65.0] |
| Ethnicity‡ | ||
| 13 studies | White, % participants | 74 [18, 89] |
| 10 studies | Black/African-American, % participants | 18 [12, 39] |
| 8 studies | Hispanic/Latino, % participants | 13 [3, 38] |
| 5 studies | East Asian, % participants | 100 |
| 6 studies | Southeast Asian, % participants | 100 |
| 4 studies | Asian/Pacific Islander, % participants | 4, 5, 15, 17§ |
| 4 studies | Native American, % participants | 1, 3, 6, 100§ |
| Education | ||
| 9 studies | <High school (or equivalent), % participants | 14 (11, 33) [5, 64] |
| 20 studies | High school (or some college), % participants | 30 (21, 48) [10, 69] |
| 11 studies | Bachelors degree (or equivalent), % participants | 28 (20, 37) [14, 52] |
| 4 studies | Graduate degree (or equivalent), % participants | 13, 15, 16, 35§ |
DPP = U.S. Diabetes Prevention Program Trial, DPS = Finnish Diabetes Prevention Study, IQI = interquartile interval, mo = months.
In some programs, the maintenance period contacts were by telephone or email only.
Excluding 2 studies in adolescents.
Excluding counts of studies with 0% of an ethnicity.
List of percentages among relevant studies.
Incident Diabetes
Sixteen studies that compared D&PA to usual care reported new-onset diabetes (6–9;22–33); two studies compared two programs each to usual care. All but three were randomized trials (9;22;26). Incident diabetes was reported between 1 and 23 years from the start of the programs (Figure 1). Across studies, between 0% (at 1 year) and 73% (at 23 years) of participants in the D&PA programs developed diabetes. At all time points participants in the D&PA programs were less likely to develop diabetes. Across all studies, the summary RR for incident diabetes was 0.59 (95% CI 0.51, 0.66) with no statistical heterogeneity. The median risk difference across studies was −11 percentage points (IQI −16, −5). Funnel plot analysis did not find different effects between larger and smaller studies (Harbord test P=0.27).
Figure 1.
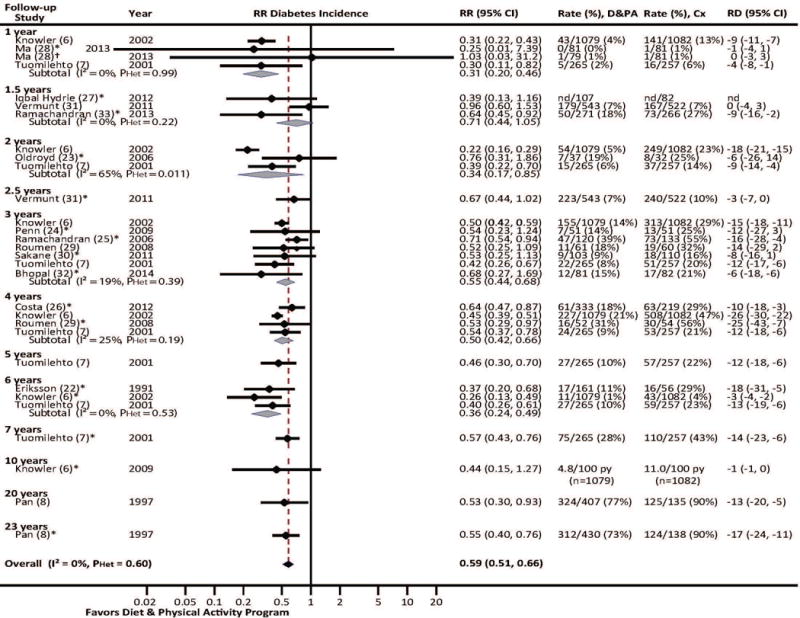
Random-effects model meta-analysis of RR of incident diabetes in at-risk participants in combined diet and physical activity promotion programs vs. usual care.
For the meta-analysis of the overall summary risk ratio (RR) of incident diabetes (black diamond), the longest duration of follow-up from each study was used, as indicated by the asterisks and the grey boxes which correspond to the weight of each study in the overall meta-analysis. Subgroup meta-analyses by follow-up time (open diamonds) were conducted for time points with data from at least three studies. CI = confidence interval, Cx = control (usual care), D&PA = combined diet and physical activity promotion program, PHet = Chi-squared P value of heterogeneity, RD = risk difference, RR = risk ratio.
* Included in overall meta-analysis.
† To avoid biased meta-analyses due to including correlated analyses, this comparison between the lower intensity intervention and control was excluded from meta-analysis.
Both the U.S. Diabetes Prevention Program (DPP) (6) and the Finnish Diabetes Prevention Study (DPS) (7) found statistically larger effects in older participants; but while DPS found a nonsignificant effect in the youngest age group (<51 years), DPP found statistically significant effects in all age groups. Neither study found differences by sex. The DPP found no difference by race or ethnicity and DPS found no difference by educational attainment. The Japan DPP study reported a significant effect of D&PA among participants with baseline HbA1c ≥5.7% in contrast with participants with lower baseline HbA1c, but they did not provide a statistical analysis of the difference between subgroups (34).
Comparing across studies, no significant differences were found by setting; number of sessions; program duration; whether the D&PA program was based on the DPP or DPS approach; inclusion of a weight loss goal, individual or group diet or exercise sessions (analyzed separately); or individually tailored diet plans, diet or exercise counselors (analyzed separately). The 11 programs that included an individually tailored exercise plan (RR 0.53; 95% CI 0.45, 0.63) had a possibly greater effect than the five that did not (RR 0.67; 95% CI 0.55, 0.81; P for interaction=0.070).
Six studies directly compared more versus less intensive D&PA programs (28;45;47;48;50;56). Compared with less intensive programs, more intensive programs had more sessions (four studies); weight loss, diet, or exercise goals (three studies), or—in one study each—a maintenance phase, more intensive diet and exercise plans, an exercise physiologist, individual contact sessions, or in-person (vs. DVD) sessions. All five studies that reported at least one case of incident diabetes found lower diabetes incidence with more intensive program (RR 0.28 to 0.56), but in only one study was this statistically significant (50) (Supplemental Figure 2).
Reversion to Normoglycemia
Six studies (five trials, one non-randomized study) that compared D&PA to usual care reported reversion to normoglycemia as early as 1 year from the start of the intervention (Figure 2) (6;22–25;32). Across studies, between 20% (at 2 years) and 52% (at 6 years) of participants in the D&PA programs reverted to normoglycemia. At 3 years (four studies) and across time points, the summary RR for achieving normoglycemia were statistically significant, with an overall summary RR of 1.53 (95% CI 1.26, 1.71), with no statistical heterogeneity. The median risk difference across studies was 12 percentage points (IQI 6, 14). No within-study subgroup differences were reported and no between-study subgroup differences were found. Three studies directly compared more versus less intensive programs (45;47;48), all of which favored more intensive programs (RR 1.58 to 2.11), two of which were statistically significant (47:48) (Supplemental Figure 3).
Figure 2.
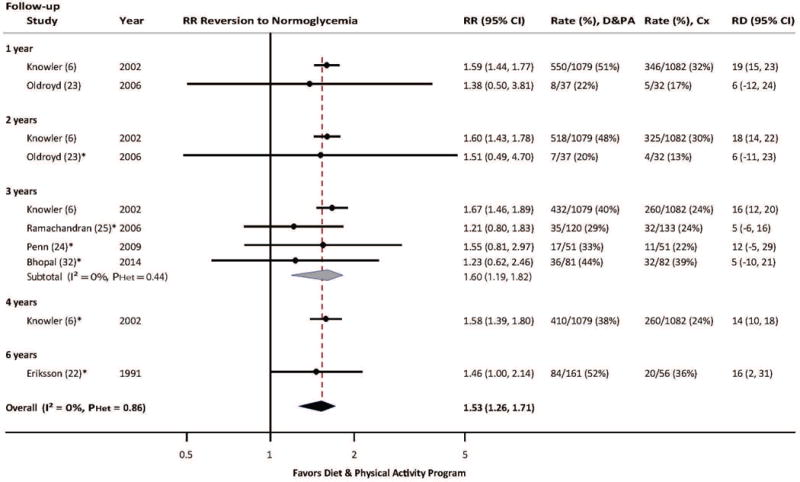
Random-effects model meta-analysis of RR of reversion to normoglycemia in at-risk participants in combined diet and physical activity promotion programs vs. usual care.
See Figure 1 legend.
* Included in overall meta-analysis.
Clinical events
Three long-term studies reported all-cause mortality, two of which also reported cardiovascular mortality with no consistent pattern of results. The Da Qing study reported lower risk for all-cause mortality (hazard ratio [HR] 0.71; 95% CI 0.51, 0.99) with D&PA after 23 years (10), but this effect was restricted to women and was not significant at earlier time points (HR 1.33 at 6 years and 0.96 at 20 years) (8). Knowler et al. (DPP) found no effect at 3 years (RD −0.6/1000 person-years) and Tuomilehto et al. (DPS) found no effect at 10 years (HR 0.57; 95% CI 0.21, 1.58) (6;105). Regarding cardiovascular death, neither Da Qing (HR 0.83; 95% CI 0.48, 1.40) at 20 years nor DPP (RR 0.50; 95% CI 0.09, 2.73) at 3 years found significant effects (10; 105). The Da Qing study reported a reduction in severe retinopathy (HR 0.53; 95% CI 0.29, 0.99) (71). Limited evidence found no significance for other clinical outcomes (cardiovascular events [2 studies], nephropathy, neuropathy, and retinopathy [1 study each]), often due to lack of power.
Body weight and glycemia
The 24 studies that compared D&PA programs to usual care and reported weight change all found net weight loss with D&PA programs (6;7;9;22–24;27–33;35–41,52–55), ranging from −0.2% to −10.5% of initial body weight (summary net change −2.2%; 95% CI −2.9, −1.4); however, the studies were highly statistically heterogeneous (I2 = 89%, PHeterogeneity <0.001) (Figure 3). Funnel plot analysis did not find different effects between larger and smaller studies (Egger test P=0.51). By meta-regression, we tested the same covariables examined for Incident Diabetes and the only variable for which there were different effects across studies was for program based on DPP or DPS. The 12 programs based on DPP or DPS yielded a net change of −3.0% (95% CI −4.1, −1.9) compared with the 13 other programs (net change −1.6%; 95% CI −2.5, −0.6; P = 0.051 for interaction). However, heterogeneity across studies remained high (residual I2=95%). Across all 42 D&PA programs (not compared with usual care) (6;7;22;23;27–33;35–51;54–58), none of the factors explored by meta-regression yielded statistically significant differences across studies. In contrast to the across-studies analysis, six of the nine studies that directly compared more versus less intensive D&PA programs found statistically significant greater weight loss with the more intensive programs (28;44;45;47–50;56;58) (Supplemental Figure 4).
Figure 3.
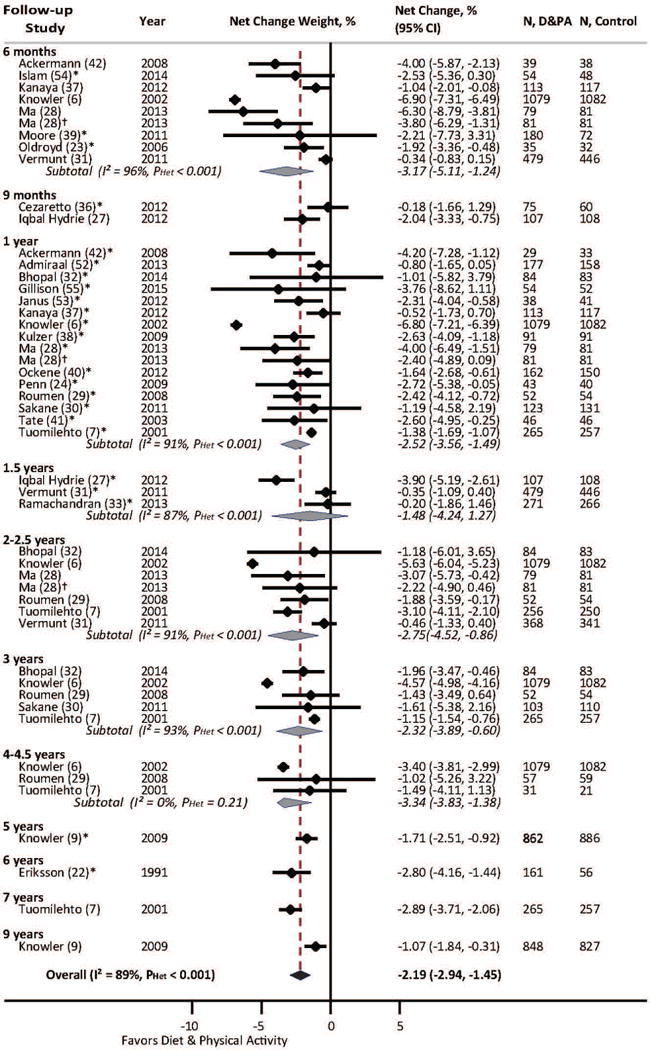
Random-effects model meta-analysis of net percent change in weight (from baseline) in at-risk participants in combined diet and physical activity promotion programs vs. usual care.
See Figure 1 legend. Study data closest to 1 year follow-up were included in the overall meta-analysis.
* Included in overall meta-analysis.
† To avoid biased meta-analyses due to including correlated analyses, this comparison between the lower intensity intervention and control was excluded from meta-analysis.
Eighteen studies that compared D&PA programs to usual care reported glycemia outcomes (6–9;23;28–32;35–40;52;53). Overall, D&PA programs improved measures of glycemia. Across studies, at follow-up durations closest to 1 year, FG improved with a summary net change of −0.12 mmol/L (95% CI −0.20, −0.05; 17 studies; I2 =77%) (−2.2 mg/dL; 95% CI −3.6, −0.9), 2hG improved by −0.48 mmol/L (95% CI −0.86, −0.17; 11 studies; I2 =87%) (−8.6 mg/dL (95% CI −15.5, −3.1), and HbA1c improved by −0.08% (95% CI −0.12, −0.04; 8 studies; I2 = 0%) (Supplemental Table 7). Funnel plot analysis found no significant small study effect with FG (Egger test P=0.54), but smaller studies were more likely to have large net reductions in 2hG (P=0.003); however, studies reporting significant effects on FG were no more likely to report 2hG results than those with nonsignificant FG effects (P=0.21). Across eight studies that compared more versus less intensive D&PA programs (28;43–45;48–50;56) (Supplemental Table 8), the median net change in FG was −0.11 mmol/L (full range −0.20, 0.17) (−2.0 mg/dL; full range −3.6, 1.8), favoring more intensive programs; however, in only one study was the difference statistically significant (56). Four studies found a median net change of −0.37 mmol/L (full range −0.6, −0.2) (−6.7 mg/dL; full range −11, −3.6) in 2hG, favoring more intensive programs (44;45;48;50); in two studies the difference was significant (48;50). None of these studies reported on HbA1c.
Across the 31 D&PA programs (not compared with usual care) in 24 studies that reported FG (6–9;23;28–32;36–39;43–46;48–50;52;53;56), there were differences based on whether individual diet sessions and diet counselors were included. Adjusting for follow-up duration, programs with individual diet sessions (n=25/31) or with diet counselors (n=22/31) yielded larger decrements in FG (individual sessions: −0.24 vs. −0.02 mmol/L [−4.3 vs. −0.4 mg/dL], P=0.020; counselors: −0.25 vs. −0.07 mmol/L [−4.5 vs. −1.3 mg/dL; P=0.034).
Blood pressure and lipids
Across 17 studies comparing D&PA programs to usual care (6;7;9;22;23;28;29;32;33;35–39;52–54), at follow-up durations closest to 1 year, D&PA improved BP (systolic: net change = −1.6 mmHg; 95% CI −2.7, −0.5; I2 = 45%) (diastolic: net change = −1.6 mmHg; 95% CI −2.5, −0.8; I2 =73%) (Supplemental Table 9). No evidence of small study effects was found (Egger test = 0.51 systolic, 0.83 diastolic) Across 14 studies, D&PA also statistically significantly improved lipid levels (7;9;22;23;28;29;33;35–39;52;53): total cholesterol (net change = −0.05 mmol/L; 95% CI −0.12, −0.002 [−1.8 mg/dL (95% CI −4.6, −0.1]; 12 studies; I2 = 0%), LDL (net change = −0.09 mmol/dL; 95% CI −0.17, −0.01 [−3.3 mg/dL; 95% CI −6.4, −0.3]; 8 studies; I2 = 0%), HDL (net change = 0.03 mmol/L; 95% CI 0.02, 0.05 [1.2 mg/dL; 95% CI 0.7, 1.7]; 12 studies; I2 = 0%), and triglycerides (net change = −0.07 mmol/L; 95% CI −0.14, −0.02 [−6.5 mg/dL; 95% CI −12.7, −1.8; 13 studies; I2 =38%) (Supplemental Table 10). No evidence of small study effects was found (Egger test = 0.17 total cholesterol, 0.75 HDL, 0.12 triglycerides).
Virtual programs
Five studies evaluated programs that were conducted via web-tools, social networking, email, text messaging, video, or a combination of these, with no in-person sessions (28;33;41;42;88). One study (28) found smaller, but still significant improvements in weight and FG with a DVD compared with an in-person program: weight −5% vs. −7% from baseline; FG −2.7 versus −4.2 mg/dL. Two studies (41;42) found similar effects on weight loss as found in studies with in-person sessions: −3% to −5% from baseline. One study in India (33) found that an intervention relying on text messages was effective compared to usual care, with lesser diabetes incidence over 2 years (18% vs. 27%; HR=0.64; 95% CI 0.45, 0.92) with statistically significant net differences in HDL and triglycerides, but not weight, BP, or total cholesterol. The fifth study (88), in adolescents, however, found no effect on weight (although, this was also true for a similar program with group sessions).
Programs in Adolescents
Two studies were conducted in adolescents. In the study by Savoye et al. (102), adolescents who participated in twice-a-week group sessions were significantly more likely to revert to normoglycemia, lose weight, and have lower FG and BP compared with a control group, but there was no change in lipid profile, except triglycerides. None developed diabetes during the 6 month follow-up period. The study by Patrick et al. (88) evaluated three different programs (web, web and text message, and web and group session programs) and reported no difference in weight loss compared with a control group after 6 and 12 months. The study did not report incident diabetes or FG outcomes.
Discussion
Across the wide spectrum of D&PA programs, there is strong evidence of effectiveness in reducing new-onset diabetes Across 16 studies, participants in D&PA programs were consistently about 40% less likely to develop diabetes, but this outcome was evaluated in only a minority (30%) of studies. D&PA programs also increase the likelihood of reverting to normoglycemia and they improve diabetes and cardiometabolic risk factors, including overweight, high blood glucose, high blood pressure, and abnormal lipid profile. The effectiveness of these programs on cardiovascular disease, diabetes-related complications, and death is yet to be determined since few studies reported these outcomes.
During protocol development, we searched Medline and the Cochrane Database of Systematic Reviews for pertinent systematic reviews; none was found that was sufficiently up-to-date and that evaluated the breadth of outcomes and range of analyses evaluated in the current review. The most comprehensive review was a health technology assessment by Gillett et al. whose search was conducted in 2011 (121), but also included diet or exercise interventions (not in combination); nine randomized trials were included. An updated search found three similar, but more restrictive reviews published since 2013. They focused on narrower subsets of studies in adults. Schellenberg et al. included nine randomized trial of D&PA programs that had at least one other component (122). Dunkley et al. included 25 studies (11 randomized trials) of D&PA programs that explicitly translated previous efficacy trials into the community settings (123), but included studies of a broader population (e.g., obese or sedentary). Aguiar et al. included only eight studies (5 randomized trials) of D&PA interventions that included both aerobic and resistance training (124). Both reviews found similar effects on weight loss, and the latter also on FG. In meta-regression, Dunkley et al. found larger changes in weight with better alignment with lifestyle intervention attributes (123).
The evidence suggests that higher intensity programs lead to greater weight loss and reduction in new-onset diabetes. While evaluated programs were too different from each other to draw firm conclusions about the unique contributions of specific program components, results from 12 studies that directly compared programs showed that people who received more intensive programs (based on features such as number of sessions, individual sessions, and additional personnel) lost more weight and were less likely to develop diabetes. The studies that compared programs with controls had very similar effects on diabetes risk across studies; therefore, no differences based on differences in their programs could be ascertained. However, across all studies, programs that provided individual (vs. group) diet sessions resulted in greater reductions in FG, as did programs that used diet counselors (vs. no diet counselors). Programs based on DPP or DPS (which were more intensive than many other programs) resulted in greater weight loss. More information on virtual delivery will be useful to increase the reach of effective D&PA programs.
Based on evidence from two of the larger studies (the U.S. DPP and the Finnish DPS), findings appear to be applicable to wide populations (in Western countries) across race and ethnicity, socioeconomic status, risk factor status, and other demographic features. With the exception of programs in two studies, all programs were applied in adults; therefore, our results may not apply in children and adolescents. However, it is likely that the benefit of D&PA programs is applicable to younger individuals at risk for type 2 diabetes because the disease mechanisms are shared between adults and children. Although most cases of diabetes in children are due to type 1 diabetes, nearly all cases of diabetes that develop from pre-diabetes (being at increased risk of diabetes) are due to type 2 diabetes. Key aspects of the pathophysiology of type 2 diabetes are similar in individuals of all ages; thus, the programs are likely to be effective regardless of age, assuming the programs are effective at changing children’s diet and physical activity. The one in-person program conducted in adolescents was similarly effective as programs conducted in adults; however, the other study in adolescents of various virtual programs found no effect on weight.
Additional studies comparing D&PA programs to usual care (no program), will likely not change the overall conclusion about the D&PA programs’ effectiveness with the exception of programs for children and adolescents and, possibly, in specific populations or settings where there are gaps in data. However, there are several areas that would benefit from future research in this area. Because the available programs were highly heterogeneous with many features included, all of which likely interacted with each other, we were unable to explain the observed heterogeneity by whether programs included specific features. Furthermore, despite often protracted descriptions of the interventions, articles often failed to clearly identify who led the interventions, what the goals were, or to provide other details to one to reproduce the intervention. Future studies that compare specific program features are needed to clarify which features (eg, individual versus group sessions, few versus many sessions, differently trained counselors) optimize the effectiveness of the programs and which are less critical. It is also unclear what is the most effective way to structure the maintenance phase to help program participants maintain their improvements. Additionally, with the proliferation of mobile devices and applications, the effectiveness of virtual programs needs to be further investigated. Importantly, long-term follow-up of (existing) community-based programs are needed to evaluate the durability of the programs’ effects and their effects on clinical outcomes. Although this review did not specifically address participant attrition, a better understanding is needed of what typical attrition rates are, to understand the reasons program participants drop out, and to develop methods to retain them in the programs.
In conclusion, combined D&PA promotion programs are effective for people at increased risk of type 2 diabetes for reducing new-onset diabetes, increasing reversion to normoglycemia and improving diabetes and cardiometabolic risk factors. Programs are effective across a wide range of program features but more intensive interventions appear to be more effective. Further research is needed to discern which specific program features are most important.
Supplementary Material
Supplemental Figure 1. Literature flow.
*Not already screened.
†Not a population of interest (n=71), diet or physical activity alone (n=58), protocol or baseline data only (n=26), no outcome of interest reported (n=25), not intervention of interest (n=20), cost-effectiveness analysis only (n=17), not a primary study (n=12), >10% of participants do not meet eligibility criteria (n=12), miscellaneous (n=7: prediction model, retrospective study, duplicate article).
‡plus 1 not analyzed due to limited quality of execution.
Supplemental Figure 2. Forest plot of RR of incident diabetes in at-risk participants in more vs. less intensive combined diet and physical activity promotion programs.
CI = confidence interval, RD = risk difference, RR = risk ratio.
Supplemental Figure 3. Forest plot of RR of reversion to normoglycemia in at-risk participants in more vs. less intensive combined diet and physical activity promotion programs.
CI = confidence interval, RD = risk difference, RR = risk ratio.
Supplemental Figure 4. Forest plot of net percent change in weight (from baseline) in at-risk participants in more vs. less intensive combined diet and physical activity promotion programs. CI = confidence interval, N = number of participants.
Supplemental Table 1. Search strategy.
Supplemental Table 2. Quality assessment of studies.
Supplemental Table 3. Study characteristics.
Supplemental Table 4. Intervention characteristics.
Supplemental Table 5. Studies using trainers or dietitians.
Supplemental Table 6. Participant characteristics.
Supplemental Table 7. Meta-analyses of glycemia measures, combined diet and physical activity promotion programs vs. usual care.
Supplemental Table 8. Meta-analyses of glycemia measures, more vs. less intensive combined diet and physical activity promotion programs.
Supplemental Table 9. Meta-analyses of blood pressure, combined diet and physical activity promotion programs vs. usual care.
Supplemental Table 10. Meta-analyses of lipids, combined diet and physical activity promotion programs vs. usual care.
Acknowledgements1
We would like to thank the Community Preventive Services Task Force for their contributions and assistance with developing the protocol and suggestions on assessing the body of evidence; in particular, the Community Guide Technical Monitor (David P. Hopkins, MD, MPH), Coordination Team panel of stakeholders (Ann Albright, PhD, RD, Elizabeth B. Daniels, PhD, RN, Judith Fradkin, MD, Todd S. Harwell, MPH, Matt Longjohn, MD, MPH, Melinda Maryniuk RD, MEd, CDE, Nicolaas P. Pronk, PhD, and Patrick L. Remington MD, MPH) and members of the Community Preventive Services Task Force. We also want to thank other members of our research team who participated in various stages of the review (Denish Moorthy, MBBS, MS; Fadi Obeid, MD; Rebecca Persson, BA; Katrin Uhlig, MD, MS). Additional thanks to technical editors Kate W. Harris, BA, and Krista Hopkins Cole, MPH.
Financial support:
By a contract from the Centers for Disease Control and Prevention (Contract No. 200-2012-53787)
Footnotes
Disclaimer: The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the CDC or of the Community Preventive Services Task Force.
Conflict of Interest: None of the authors have any affiliations or financial involvement (e.g., employment, consultancies, honoraria, stock options, expert testimony, grants or patents received or pending, or royalties) that conflict with material presented in this article.
Albright: Centers for Disease Control and Prevention, Atlanta, GA
Daniels: Centers for Disease Control and Prevention, Atlanta, GA
Fradkin: National Institute of Diabetes and Digestive and Kidney Diseases, NIH, Bethesda, MD
Harris: The Community Guide, Atlanta, GA
Harwell: Public Health and Safety Division, State of Montana Department of Public Health and Human Services, Helena, MT
Hopkins Cole: Karna, Atlanta, GA
Hopkins: Centers for Disease Control and Prevention, Atlanta, GA
Longjohn: YMCA of the USA, Chicago, IL
Maryniuk: Joslin Diabetes Center. Boston, MA
Moorthy: Micronutrients, SPRING Project, Washington, DC (Current)
Obeid: Tufts Medical Center, Boston, MA
Persson: Boston University School of Public Health, Boston, MA (Current)
Pronk: HealthPartners, Minneapolis, MN and Harvard School of Public Health, Boston, MA
Remington: School of Medicine and Public Health, University of Wisconsin, Madison, WI
Uhlig: Tufts University School of Medicine, Boston, MA
References
- 1.Centers for Disease Control and Prevention (CDC) National Diabetes Statistics Report: Estimates of Diabetes and Its Burden in the United States. Atlanta, GA: US Department of Health and Human Services; 2014. 2014. [Google Scholar]
- 2.International Diabetes Federation. IDF Diabetes Atlas. (6th) 2014 http://www.idf.org/diabetesatlas (last accessed 5/3/2015)
- 3.Huang ES, Basu A, O’Grady M, Capretta JC. Projecting the future diabetes population size and related costs for the US. Diabetes Care. 2009;32(12):2225–2229. doi: 10.2337/dc09-0459. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.American Diabetes Association. Diagnosis and Classification of Diabetes Mellitus. Diabetes Care. 2010;33(Suppl 1):S62–S69. doi: 10.2337/dc10-S062. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Gerstein HC, Santaguida P, Raina P, Morrison KM, Balion C, Hunt D, et al. Annual incidence and relative risk of diabetes in people with various categories of dysglycemia: a systematic overview and meta-analysis of prospective studies. Diabetes Res Clin Pract. 2007;78(3):305–312. doi: 10.1016/j.diabres.2007.05.004. [DOI] [PubMed] [Google Scholar]
- 6.Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002;346(6):393–403. doi: 10.1056/NEJMoa012512. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Tuomilehto J, Lindstrom J, Eriksson JG, Valle TT, Hamalainen H, Ilanne-Parikka P, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001;344(18):1343–1350. doi: 10.1056/NEJM200105033441801. [DOI] [PubMed] [Google Scholar]
- 8.Pan XR, Li GW, Hu YH, Wang JX, Yang WY, An ZX, et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care. 1997;20(4):537–544. doi: 10.2337/diacare.20.4.537. [DOI] [PubMed] [Google Scholar]
- 9.Diabetes Prevention Program Research Group. Knowler WC, Fowler SE, Hamman RF, Christophi CA, Hoffman HJ, et al. 10-year follow-up of diabetes incidence and weight loss in the Diabetes Prevention Program Outcomes Study. Lancet. 2009;374(9702):1677–1686. doi: 10.1016/S0140-6736(09)61457-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Li G, Zhang P, Wang J, An Y, Gong Q, Gregg EW, et al. Cardiovascular mortality, all-cause mortality, and diabetes incidence after lifestyle intervention for people with impaired glucose tolerance in the Da Qing Diabetes Prevention Study: a 23-year followup study. Lancet Diabetes Endocrinol. 2014;2(6):474–480. doi: 10.1016/S2213-8587(14)70057-9. [DOI] [PubMed] [Google Scholar]
- 11.Lindstrom J, Ilanne-Parikka P, Peltonen M, Aunola S, Eriksson JG, Hemio K, et al. Sustained reduction in the incidence of type 2 diabetes by lifestyle intervention: followup of the Finnish Diabetes Prevention Study. Lancet. 2006;368(9548):1673–1679. doi: 10.1016/S0140-6736(06)69701-8. [DOI] [PubMed] [Google Scholar]
- 12.Albright AL, Gregg EW. Preventing type 2 diabetes in communities across the U.S: the National Diabetes Prevention Program. Am J Prev Med. 2013;44(4 Suppl 4):S346–S351. doi: 10.1016/j.amepre.2012.12.009. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Briss PA, Zaza S, Pappaioanou M, Fielding J, Wright-De AL, Truman BI, et al. Developing an evidence-based Guide to Community Preventive Services–methods. The Task Force on Community Preventive Services. Am J Prev Med. 2000;18(1 Suppl):35–43. doi: 10.1016/s0749-3797(99)00119-1. [DOI] [PubMed] [Google Scholar]
- 14.Zaza S, Wright-De Aguero LK, Briss PA, Truman BI, Hopkins DP, Hennessy MH, et al. Data collection instrument and procedure for systematic reviews in the Guide to Community Preventive Services. Task Force on Community Preventive Services. Am J Prev Med. 2000;18(1 Suppl):44–74. doi: 10.1016/s0749-3797(99)00122-1. [DOI] [PubMed] [Google Scholar]
- 15.IOM (Institute of Medicine) Finding What Works in Health Care: Standards for Systematic Reviews. Washington, DC: The National Academic Press; 2011. [PubMed] [Google Scholar]
- 16.Methods Guide for Effectiveness and Comparative Effectiveness Reviews. Rockville, MD: Agency for Healthcare Research Quality; 2012. (AHRQ Publication 10(12)-EHC063-EF). [Google Scholar]
- 17.Wallace B, Small K, Brodley C, Lau J, Trikalinos T. Deploying an interactive machine learning system in an evidence-based practice center: Abstrackr. Proc of the ACM International Health Informatics Symposium (IHI) 2012:819–824. http://abstrackr.cebm.brown.edu/ (last accessed 5/3/2015)
- 18.Systematic Review Data Repository. http://srdr.ahrq.gov/. (last accessed 5/3/2015)
- 19.The Community Guide. Data Abstraction Form. http://www.thecommunityguide.org/methods/abstractionform.pdf. (last accessed 5/3/2015)
- 20.Hardy RJ, Thompson SG. A likelihood approach to meta-analysis with random effects. Stat Med. 1996;15(6):619–29. doi: 10.1002/(SICI)1097-0258(19960330)15:6<619::AID-SIM188>3.0.CO;2-A. [DOI] [PubMed] [Google Scholar]
- 21.Harbord RM, Harris RJ, Sterne JAC. Updated tests for small-study effects in meta-analyses. Stata J. 2009;9(2):197–210. [Google Scholar]
- 22.Eriksson KF, Lindgarde F. Prevention of type 2 (non-insulin-dependent) diabetes mellitus by diet and physical exercise. The 6-year Malmo feasibility study. Diabetologia. 1991;34(12):891–898. doi: 10.1007/BF00400196. [DOI] [PubMed] [Google Scholar]
- 23.Oldroyd JC, Unwin NC, White M, Mathers JC, Alberti KG. Randomised controlled trial evaluating lifestyle interventions in people with impaired glucose tolerance. Diabetes Res Clin Pract. 2006;72(2):117–127. doi: 10.1016/j.diabres.2005.09.018. [DOI] [PubMed] [Google Scholar]
- 24.Penn L, White M, Oldroyd J, Walker M, Alberti KG, Mathers JC. Prevention of type 2 diabetes in adults with impaired glucose tolerance: the European Diabetes Prevention RCT in Newcastle upon Tyne, UK. BMC Public Health. 2009;9:342. doi: 10.1186/1471-2458-9-342. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Ramachandran A, Snehalatha C, Mary S, Mukesh B, Bhaskar AD, Vijay V, et al. The Indian Diabetes Prevention Programme shows that lifestyle modification and metformin prevent type 2 diabetes in Asian Indian subjects with impaired glucose tolerance (IDPP-1) Diabetologia. 2006;49(2):289–297. doi: 10.1007/s00125-005-0097-z. [DOI] [PubMed] [Google Scholar]
- 26.Costa B, Barrio F, Cabre JJ, Pinol JL, Cos X, Sole C, et al. Delaying progression to type 2 diabetes among high-risk Spanish individuals is feasible in real-life primary healthcare settings using intensive lifestyle intervention. Diabetologia. 2012;55(5):1319–1328. doi: 10.1007/s00125-012-2492-6. [DOI] [PubMed] [Google Scholar]
- 27.Iqbal Hydrie MZ, Basit A, Shera AS, Hussain A. Effect of intervention in subjects with high risk of diabetes mellitus in Pakistan. J Nutr Metab. 2012;2012:867604. doi: 10.1155/2012/867604. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ma J, Yank V, Xiao L, Lavori PW, Wilson SR, Rosas LG, et al. Translating the Diabetes Prevention Program lifestyle intervention for weight loss into primary care: a randomized trial. JAMA Intern Med. 2013;173(2):113–121. doi: 10.1001/2013.jamainternmed.987. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Roumen C, Corpeleijn E, Feskens EJ, Mensink M, Saris WH, Blaak EE. Impact of 3-year lifestyle intervention on postprandial glucose metabolism: the SLIM study. Diabet Med. 2008;25(5):597–605. doi: 10.1111/j.1464-5491.2008.02417.x. [DOI] [PubMed] [Google Scholar]
- 30.Sakane N, Sato J, Tsushita K, Tsujii S, Kotani K, Tsuzaki K, et al. Prevention of type 2 diabetes in a primary healthcare setting: three-year results of lifestyle intervention in Japanese subjects with impaired glucose tolerance. BMC Public Health. 2011;11(1):40. doi: 10.1186/1471-2458-11-40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Vermunt PW, Milder IE, Wielaard F, de Vries JH, van Oers HA, Westert GP. Lifestyle counseling for type 2 diabetes risk reduction in Dutch primary care: results of the APHRODITE study after 0.5 and 15 years. Diabetes Care. 2011;34(9):1919–1925. doi: 10.2337/dc10-2293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Bhopal RS, Douglas A, Wallia S, Forbes JF, Lean ME, Gill JM, et al. Effect of a lifestyle intervention on weight change in south Asian individuals in the UK at high risk of type 2 diabetes: a family-cluster randomised controlled trial. Lancet Diabetes Endocrinol. 2014;2(3):218–27. doi: 10.1016/S2213-8587(13)70204-3. [DOI] [PubMed] [Google Scholar]
- 33.Ramachandran A, Snehalatha C, Ram J, Selvam S, Simon M, Nanditha A, et al. Effectiveness of mobile phone messaging in prevention of type 2 diabetes by lifestyle modification in men in India: a prospective, parallel-group, randomised controlled trial. Lancet Diabetes Endocrinol. 2013;1(3):191–8. doi: 10.1016/S2213-8587(13)70067-6. [DOI] [PubMed] [Google Scholar]
- 34.Sakane N, Sato J, Tsushita K, Tsujii S, Kotani K, Tominaga M, et al. Effect of baseline HbA1c level on the development of diabetes by lifestyle intervention in primary healthcare settings: insights from subanalysis of the Japan Diabetes Prevention Program. BMJ Open Diabetes Res Care. 2014;2(1):e000003. doi: 10.1136/bmjdrc-2013-000003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ackermann RT, Finch EA, Brizendine E, Zhou H, Marrero DG. Translating the Diabetes Prevention Program into the community. The DEPLOY Pilot Study. Am J Prev Med. 2008;35(4):357–363. doi: 10.1016/j.amepre.2008.06.035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Cezaretto A, Siqueira-Catania A, de Barros CR, Salvador EP, Ferreira SR. Benefits on quality of life concomitant to metabolic improvement in intervention program for prevention of diabetes mellitus. Qual Life Res. 2012;21(1):105–113. doi: 10.1007/s11136-011-9919-2. [DOI] [PubMed] [Google Scholar]
- 37.Kanaya AM, Santoyo-Olsson J, Gregorich S, Grossman M, Moore T, Stewart AL. The Live Well, Be Well study: a community-based, translational lifestyle program to lower diabetes risk factors in ethnic minority and lower-socioeconomic status adults. Am J Public Health. 2012;102(8):1551–1558. doi: 10.2105/AJPH.2011.300456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Kulzer B, Hermanns N, Gorges D, Schwarz P, Haak T. Prevention of diabetes self-management program (PREDIAS): effects on weight, metabolic risk factors, and behavioral outcomes. Diabetes Care. 2009;32(7):1143–1146. doi: 10.2337/dc08-2141. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Moore SM, Hardie EA, Hackworth NJ, Critchley CR, Kyrios M, Buzwell SA, et al. Can the onset of type 2 diabetes be delayed by a group-based lifestyle intervention? A randomised control trial. Psychol Health. 2011;26(4):485–499. doi: 10.1080/08870440903548749. [DOI] [PubMed] [Google Scholar]
- 40.Ockene IS, Tellez TL, Rosal MC, Reed GW, Mordes J, Merriam PA, et al. Outcomes of a Latino community-based intervention for the prevention of diabetes: the Lawrence Latino Diabetes Prevention Project. Am J Public Health. 2012;102(2):336–342. doi: 10.2105/AJPH.2011.300357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Tate DF, Jackvony EH, Wing RR. Effects of Internet behavioral counseling on weight loss in adults at risk for type 2 diabetes: a randomized trial. JAMA. 2003;289(14):1833–1836. doi: 10.1001/jama.289.14.1833. [DOI] [PubMed] [Google Scholar]
- 42.Ackermann RT, Sandy LG, Beauregard T, Coblitz M, Norton KL, Vojta D. A randomized comparative effectiveness trial of using cable television to deliver diabetes prevention programming. Obesity (Silver Spring) 2014;22(7):1601–1607. doi: 10.1002/oby.20762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Cole RE, Boyer KM, Spanbauer SM, Sprague D, Bingham M. Effectiveness of prediabetes nutrition shared medical appointments: prevention of diabetes. Diabetes Educ. 2013;39(3):344–353. doi: 10.1177/0145721713484812. [DOI] [PubMed] [Google Scholar]
- 44.Dunbar J, Davis-Lameloise N, Philpot B, Reddy P, Bunker S, Heistaro S, et al. Sustained gains from a diabetes prevention program and the role of telephone support. Int J Diabetes Mellitus. 2010;2(2):95–100. [Google Scholar]
- 45.Gagnon C, Brown C, Couture C, Kamga-Ngande CN, Hivert MF, Baillargeon JP, et al. A cost-effective moderate-intensity interdisciplinary weight-management programme for individuals with prediabetes. Diabetes Metab. 2011;37(5):410–418. doi: 10.1016/j.diabet.2011.01.003. [DOI] [PubMed] [Google Scholar]
- 46.Jiang L, Manson SM, Beals J, Henderson WG, Huang H, Acton KJ, et al. Translating the Diabetes Prevention Program into American Indian and Alaska Native communities: results from the Special Diabetes Program for Indians Diabetes Prevention demonstration project. Diabetes Care. 2013;36(7):2027–2034. doi: 10.2337/dc12-1250. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Kosaka K, Noda M, Kuzuya T. Prevention of type 2 diabetes by lifestyle intervention: a Japanese trial in IGT males. Diabetes Res Clin Pract. 2005;67(2):152–162. doi: 10.1016/j.diabres.2004.06.010. [DOI] [PubMed] [Google Scholar]
- 48.Liao D, Asberry PJ, Shofer JB, Callahan H, Matthys C, Boyko EJ, et al. Improvement of BMI, body composition, and body fat distribution with lifestyle modification in Japanese Americans with impaired glucose tolerance. Diabetes Care. 2002;25(9):1504–1510. doi: 10.2337/diacare.25.9.1504. [DOI] [PubMed] [Google Scholar]
- 49.Nilsen V, Bakke PS, Gallefoss F. Effects of lifestyle intervention in persons at risk for type 2 diabetes mellitus - results from a randomised, controlled trial. BMC Public Health. 2011;11:893. doi: 10.1186/1471-2458-11-893. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Saito T, Watanabe M, Nishida J, Izumi T, Omura M, Takagi T, et al. Lifestyle modification and prevention of type 2 diabetes in overweight Japanese with impaired fasting glucose levels: a randomized controlled trial. Arch Intern Med. 2011;171(15):1352–1360. doi: 10.1001/archinternmed.2011.275. [DOI] [PubMed] [Google Scholar]
- 51.Sepah SC, Jiang L, Peters AL. Translating the Diabetes Prevention Program into an Online Social Network: Validation against CDC Standards. Diabetes Educ. 2014;40(4):435–443. doi: 10.1177/0145721714531339. [DOI] [PubMed] [Google Scholar]
- 52.Admiraal WM, Vlaar EM, Nierkens V, Holleman F, Middelkoop BJ, Stronks K, et al. Intensive lifestyle intervention in general practice to prevent type 2 diabetes among 18 to 60-year-old South Asians: 1-year effects on the weight status and metabolic profile of participants in a randomized controlled trial. PLoS ONE. 2013;8(7):e68605. doi: 10.1371/journal.pone.0068605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Janus ED, Best JD, Davis-Lameloise N, Philpot B, Hernan A, Bennett CM, et al. Scaling-up from an implementation trial to state-wide coverage: results from the preliminary Melbourne Diabetes Prevention Study. Trials. 2012;13:152. doi: 10.1186/1745-6215-13-152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Islam NS, Zanowiak JM, Wyatt LC, Kavathe R, Singh H, Kwon SC, et al. Diabetes prevention in the New York City Sikh Asian Indian community: a pilot study. Int J Environ Res Public Health. 2014;11(5):5462–86. doi: 10.3390/ijerph110505462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Gillison F, Stathi A, Reddy P, Perry R, Taylor G, Bennett P, et al. Processes of behavior change and weight loss in a theory-based weight loss intervention program: a test of the process model for lifestyle behavior change. Int J Behav Nutr Phys Act. 2015;12(1):2. doi: 10.1186/s12966-014-0160-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Katula JA, Vitolins MZ, Rosenberger EL, Blackwell CS, Morgan TM, Lawlor MS, et al. One-year results of a community-based translation of the Diabetes Prevention Program: Healthy-Living Partnerships to Prevent Diabetes (HELP PD) Project. Diabetes Care. 2011;34(7):1451–1457. doi: 10.2337/dc10-2115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Penn L, Ryan V, White M. Feasibility, acceptability and outcomes at a 12-month followup of a novel community-based intervention to prevent type 2 diabetes in adults at high risk: mixed methods pilot study. BMJ Open. 2013;3(11):e003585. doi: 10.1136/bmjopen-2013-003585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Weinstock RS, Trief PM, Cibula D, Morin PC, Delahanty LM. Weight loss success in metabolic syndrome by telephone interventions: results from the SHINE Study. J Gen Intern Med. 2013;28(12):1620–8. doi: 10.1007/s11606-013-2529-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Absetz P, Valve R, Oldenburg B, Heinonen H, Nissinen A, Fogelholm M, et al. Type 2 diabetes prevention in the “real world”: one-year results of the GOAL Implementation Trial. Diabetes Care. 2007;30(10):2465–2470. doi: 10.2337/dc07-0171. [DOI] [PubMed] [Google Scholar]
- 60.Absetz P, Oldenburg B, Hankonen N, Valve R, Heinonen H, Nissinen A, et al. Type 2 diabetes prevention in the real world: three-year results of the GOAL lifestyle implementation trial. Diabetes Care. 2009;32(8):1418–1420. doi: 10.2337/dc09-0039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Bouchard DR, Baillargeon JP, Gagnon C, Brown C, Langlois MF. Impact of health professionals’ contact frequency on response to a lifestyle intervention with individuals at high risk for diabetes. Diabetes Res Clin Pract. 2012;96(2):129–134. doi: 10.1016/j.diabres.2011.12.019. [DOI] [PubMed] [Google Scholar]
- 62.Carr DB, Utzschneider KM, Boyko EJ, Asberry PJ, Hull RL, Kodama K, et al. A reduced-fat diet and aerobic exercise in Japanese Americans with impaired glucose tolerance decreases intra-abdominal fat and improves insulin sensitivity but not beta-cell function. Diabetes. 2005;54(2):340–347. doi: 10.2337/diabetes.54.2.340. [DOI] [PubMed] [Google Scholar]
- 63.Critchley CR, Hardie EA, Moore SM. Examining the psychological pathways to behavior change in a group-based lifestyle program to prevent type 2 diabetes. Diabetes Care. 2012;35(4):699–705. doi: 10.2337/dc11-1183. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.De la Rosa A, Tahsin B, Sanghani R, Pikelny I, Fogelfeld L, Stroger J. Detecting and managing metabolic syndrome: a feasibility study in a general medicine clinic. Ethn Dis. 2008;18:S16–S18. [Google Scholar]
- 65.Delahanty LM, Peyrot M, Shrader PJ, Williamson DA, Meigs JB, Nathan DM, et al. Pretreatment, psychological, and behavioral predictors of weight outcomes among lifestyle intervention participants in the Diabetes Prevention Program (DPP) Diabetes Care. 2013;36(1):34–40. doi: 10.2337/dc12-0733. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Diabetes Prevention Program Research Group. The Diabetes Prevention Program. Design and methods for a clinical trial in the prevention of type 2 diabetes. Diabetes Care. 1999;22(4):623–634. doi: 10.2337/diacare.22.4.623. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Diabetes Prevention Program Research Group. Crandall J, Schade D, Ma Y, Fujimoto WY, Barrett-Connor E, et al. The influence of age on the effects of lifestyle modification and metformin in prevention of diabetes. J Gerontol A Biol Sci Med Sci. 2006;61(10):1075–1081. doi: 10.1093/gerona/61.10.1075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Eriksson J, Lindstrom J, Valle T, Aunola S, Hamalainen H, Ilanne-Parikka P, et al. Prevention of Type II diabetes in subjects with impaired glucose tolerance: the Diabetes Prevention Study (DPS) in Finland. Study design and 1-year interim report on the feasibility of the lifestyle intervention programme. Diabetologia. 1999;42(7):793–801. doi: 10.1007/s001250051229. [DOI] [PubMed] [Google Scholar]
- 69.Eriksson KF, Lindgarde F. No excess 12-year mortality in men with impaired glucose tolerance who participated in the Malmo Preventive Trial with diet and exercise. Diabetologia. 1998;41(9):1010–1016. doi: 10.1007/s001250051024. [DOI] [PubMed] [Google Scholar]
- 70.Gilis-Januszewska A, Szybinski Z, Kissimova-Skarbek K, Piwonska-Solska B, Pach D, Topor-Madry R, et al. Prevention of type 2 diabetes by lifestyle intervention in primary health care setting in Poland: Diabetes in Europe Prevention using Lifestyle, physical Activity and Nutritional intervention (DE-PLAN) project. Br J Diabetes Vasc Dis. 2011;11:198–203. [Google Scholar]
- 71.Gong Q, Gregg EW, Wang J, An Y, Zhang P, Yang W, et al. Long-term effects of a randomised trial of a 6-year lifestyle intervention in impaired glucose tolerance on diabetes-related microvascular complications: the China Da Qing Diabetes Prevention Outcome Study. Diabetologia. 2011;54(2):300–307. doi: 10.1007/s00125-010-1948-9. [DOI] [PubMed] [Google Scholar]
- 72.Haffner S, Temprosa M, Crandall J, Fowler S, Goldberg R, Horton E, et al. Intensive lifestyle intervention or metformin on inflammation and coagulation in participants with impaired glucose tolerance. Diabetes. 2005;54(5):1566–1572. doi: 10.2337/diabetes.54.5.1566. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Hosper K, Deutekom M, Stronks K. The effectiveness of “Exercise on Prescription” in stimulating physical activity among women in ethnic minority groups in the Netherlands: protocol for a randomized controlled trial. BMC Public Health. 2008;8:406. doi: 10.1186/1471-2458-8-406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Ilanne-Parikka P, Eriksson JG, Lindstrom J, Peltonen M, Aunola S, Hamalainen H, et al. Effect of lifestyle intervention on the occurrence of metabolic syndrome and its components in the Finnish Diabetes Prevention Study. Diabetes Care. 2008;31(4):805–807. doi: 10.2337/dc07-1117. [DOI] [PubMed] [Google Scholar]
- 75.Katula JA, Vitolins MZ, Morgan TM, Lawlor MS, Blackwell CS, Isom SP, et al. The Healthy Living Partnerships to Prevent Diabetes study: 2-year outcomes of a randomized controlled trial. Am J Prev Med. 2013;44(4 Suppl 4):S324–S332. doi: 10.1016/j.amepre.2012.12.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Kyrios M, Moore SM, Hackworth N, Buzwell SA, Crafti N, Critchley C, et al. The influence of depression and anxiety on outcomes after an intervention for prediabetes. Med J Aust. 2009;190(7 Suppl):S81–S85. doi: 10.5694/j.1326-5377.2009.tb02476.x. [DOI] [PubMed] [Google Scholar]
- 77.Laatikainen T, Dunbar JA, Chapman A, Kilkkinen A, Vartiainen E, Heistaro S, et al. Prevention of type 2 diabetes by lifestyle intervention in an Australian primary health care setting: Greater Green Triangle (GGT) Diabetes Prevention Project. BMC Public Health. 2007;7:249. doi: 10.1186/1471-2458-7-249. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Li G, Zhang P, Wang J, Gregg EW, Yang W, Gong Q, et al. The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study: a 20-year follow-up study. Lancet. 2008;371(9626):1783–1789. doi: 10.1016/S0140-6736(08)60766-7. [DOI] [PubMed] [Google Scholar]
- 79.Lindstrom J, Louheranta A, Mannelin M, Rastas M, Salminen V, Eriksson J, et al. The Finnish Diabetes Prevention Study (DPS): Lifestyle intervention and 3-year results on diet and physical activity. Diabetes Care. 2003;26(12):3230–3236. doi: 10.2337/diacare.26.12.3230. [DOI] [PubMed] [Google Scholar]
- 80.Lindstrom J, Eriksson JG, Valle TT, Aunola S, Cepaitis Z, Hakumaki M, et al. Prevention of diabetes mellitus in subjects with impaired glucose tolerance in the Finnish Diabetes Prevention Study: results from a randomized clinical trial. J Am Soc Nephrol. 2003;14(7 Suppl 2):S108–S113. doi: 10.1097/01.asn.0000070157.96264.13. [DOI] [PubMed] [Google Scholar]
- 81.Lindstrom J, Peltonen M, Eriksson JG, Aunola S, Hamalainen H, Ilanne-Parikka P, et al. Determinants for the effectiveness of lifestyle intervention in the Finnish Diabetes Prevention Study. Diabetes Care. 2008;31(5):857–862. doi: 10.2337/dc07-2162. [DOI] [PubMed] [Google Scholar]
- 82.Lindstrom J, Peltonen M, Eriksson JG, Ilanne-Parikka P, Aunola S, Keinanen-Kiukaanniemi S, et al. Improved lifestyle and decreased diabetes risk over 13 years: long-term follow-up of the randomised Finnish Diabetes Prevention Study (DPS) Diabetologia. 2013;56(2):284–293. doi: 10.1007/s00125-012-2752-5. [DOI] [PubMed] [Google Scholar]
- 83.Makrilakis K, Liatis S, Grammatikou S, Perrea D, Katsilambros N. Implementation and effectiveness of the first community lifestyle intervention programme to prevent Type 2 diabetes in Greece. The DE-PLAN study. Diabet Med. 2010;27(4):459–465. doi: 10.1111/j.1464-5491.2010.02918.x. [DOI] [PubMed] [Google Scholar]
- 84.Makrilakis K, Grammatikou S, Liatis S, Kontogianni M, Perrea D, Dimosthenopoulos C, et al. The effect of a non-intensive community-based lifestyle intervention on the prevalence of metabolic syndrome. The DEPLAN study in Greece. Hormones (Athens) 2012;11(3):316–324. doi: 10.14310/horm.2002.1360. [DOI] [PubMed] [Google Scholar]
- 85.Merriam PA, Tellez TL, Rosal MC, Olendzki BC, Ma Y, Pagoto SL, et al. Methodology of a diabetes prevention translational research project utilizing a community-academic partnership for implementation in an underserved Latino community. BMC Med Res Methodol. 2009;9:20. doi: 10.1186/1471-2288-9-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Oldroyd JC, Unwin NC, White M, Imrie K, Mathers JC, Alberti KG. Randomised controlled trial evaluating the effectiveness of behavioural interventions to modify cardiovascular risk factors in men and women with impaired glucose tolerance: outcomes at 6 months. Diabetes Res Clin Pract. 2001;52(1):29–43. doi: 10.1016/s0168-8227(00)00244-8. [DOI] [PubMed] [Google Scholar]
- 87.Orchard TJ, Temprosa M, Barrett-Connor E, Fowler SE, Goldberg RB, Mather KJ, et al. Long-term effects of the Diabetes Prevention Program interventions on cardiovascular risk factors: a report from the DPP Outcomes Study. Diabet Med. 2013;30(1):46–55. doi: 10.1111/j.1464-5491.2012.03750.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Patrick K, Norman GJ, Davila EP, Calfas KJ, Raab F, Gottschalk M, et al. Outcomes of a 12-month technology-based intervention to promote weight loss in adolescents at risk for type 2 diabetes. J Diabetes Sci Technol. 2013;7(3):759–770. doi: 10.1177/193229681300700322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Penn L, White M, Lindstrom J, den Boer AT, Blaak E, Eriksson JG, et al. Importance of weight loss maintenance and risk prediction in the prevention of type 2 diabetes: analysis of European Diabetes Prevention Study RCT. PLoS ONE. 2013;8(2):e57143. doi: 10.1371/journal.pone.0057143. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Perreault L, Ma Y, Dagogo-Jack S, Horton E, Marrero D, Crandall J, et al. Sex differences in diabetes risk and the effect of intensive lifestyle modification in the Diabetes Prevention Program. Diabetes Care. 2008;31(7):1416–1421. doi: 10.2337/dc07-2390. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Perreault L, Kahn SE, Christophi CA, Knowler WC, Hamman RF, Diabetes Prevention Program Research Group Regression from pre-diabetes to normal glucose regulation in the diabetes prevention program. Diabetes Care. 2009;32(9):1583–1588. doi: 10.2337/dc09-0523. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Perreault L, Pan Q, Mather KJ, Watson KE, Hamman RF, Kahn SE. Effect of regression from prediabetes to normal glucose regulation on long-term reduction in diabetes risk: results from the Diabetes Prevention Program Outcomes Study. Lancet. 2012;379(9833):2243–2251. doi: 10.1016/S0140-6736(12)60525-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Ramachandran A, Snehalatha C, Mary S, Selvam S, Kumar CK, Seeli AC, et al. Pioglitazone does not enhance the effectiveness of lifestyle modification in preventing conversion of impaired glucose tolerance to diabetes in Asian Indians: results of the Indian Diabetes Prevention Programme-2 (IDPP-2) Diabetologia. 2009;52(6):1019–1026. doi: 10.1007/s00125-009-1315-x. [DOI] [PubMed] [Google Scholar]
- 94.Ramachandran A, Arun N, Shetty AS, Snehalatha C. Efficacy of primary prevention interventions when fasting and postglucose dysglycemia coexist: analysis of the Indian Diabetes Prevention Programmes (IDPP-1 and IDPP-2) Diabetes Care. 2010;33(10):2164–2168. doi: 10.2337/dc09-1150. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 95.Ratner R, Goldberg R, Haffner S, Marcovina S, Orchard T, Fowler S, et al. Impact of intensive lifestyle and metformin therapy on cardiovascular disease risk factors in the diabetes prevention program. Diabetes Care. 2005;28(4):888–894. doi: 10.2337/diacare.28.4.888. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 96.Rautio N, Jokelainen J, Oksa H, Saaristo T, Peltonen M, Niskanen L, et al. Socioeconomic position and effectiveness of lifestyle intervention in prevention of type 2 diabetes: one-year follow-up of the FIN-D2D project. Scand J Public Health. 2011;39(6):561–570. doi: 10.1177/1403494811408482. [DOI] [PubMed] [Google Scholar]
- 97.Rautio N, Jokelainen J, Oksa H, Saaristo T, Peltonen M, Niskanen L, et al. Participation, socioeconomic status and group or individual counselling intervention in individuals at high risk for type 2 diabetes: one-year follow-up study of the FIN-D2D-project. Prim Care Diabetes. 2012;6(4):277–283. doi: 10.1016/j.pcd.2012.07.002. [DOI] [PubMed] [Google Scholar]
- 98.Rautio N, Jokelainen J, Oksa H, Saaristo T, Peltonen M, Puolijoki H, et al. Family history of diabetes and effectiveness of lifestyle counselling on the cardio-metabolic risk profile in individuals at high risk of Type 2 diabetes: 1-year follow-up of the FIN-D2D project. Diabet Med. 2012;29(2):207–211. doi: 10.1111/j.1464-5491.2011.03388.x. [DOI] [PubMed] [Google Scholar]
- 99.Rautio N, Jokelainen J, Saaristo T, Oksa H, Keinanen-Kiukaanniemi S, Peltonen M, et al. Predictors of success of a lifestyle intervention in relation to weight loss and improvement in glucose tolerance among individuals at high risk for type 2 diabetes: the FIN-D2D project. J Prim Care Community Health. 2013;4(1):59–66. doi: 10.1177/2150131912444130. [DOI] [PubMed] [Google Scholar]
- 100.Roumen C, Feskens EJ, Corpeleijn E, Mensink M, Saris WH, Blaak EE. Predictors of lifestyle intervention outcome and dropout: the SLIM study. Eur J Clin Nutr. 2011;65(10):1141–1147. doi: 10.1038/ejcn.2011.74. [DOI] [PubMed] [Google Scholar]
- 101.Saaristo T, Moilanen L, Korpi-Hyovalti E, Vanhala M, Saltevo J, Niskanen L, et al. Lifestyle intervention for prevention of type 2 diabetes in primary health care: one-year follow-up of the Finnish National Diabetes Prevention Program (FIN-D2D) Diabetes Care. 2010;33(10):2146–2151. doi: 10.2337/dc10-0410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Savoye M, Caprio S, Dziura J, Camp A, Germain G, Summers C, et al. Reversal of early abnormalities in glucose metabolism in obese youth: results of an intensive lifestyle randomized controlled trial. Diabetes Care. 2014;37(2):317–324. doi: 10.2337/dc13-1571. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 103.Snehalatha C, Mary S, Selvam S, Sathish Kumar CK, Shetty SB, Nanditha A, et al. Changes in insulin secretion and insulin sensitivity in relation to the glycemic outcomes in subjects with impaired glucose tolerance in the Indian Diabetes Prevention Programme-1 (IDPP-1) Diabetes Care. 2009;32(10):1796–1801. doi: 10.2337/dc09-0676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 104.Swanson CM, Bersoux S, Larson MH, Aponte-Furlow RT, Flatten SS, Olsen CL, et al. An outpatient-based clinical program for diabetes prevention: an update. Endocr Pract. 2012;18(2):200–208. doi: 10.4158/EP11226.OR. [DOI] [PubMed] [Google Scholar]
- 105.Uusitupa M, Peltonen M, Lindstrom J, Aunola S, Ilanne-Parikka P, Keinanen-Kiukaanniemi S, et al. Ten-year mortality and cardiovascular morbidity in the Finnish Diabetes Prevention Study–secondary analysis of the randomized trial. PLoS ONE. 2009;4(5):e5656. doi: 10.1371/journal.pone.0005656. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Uusitupa MI, Stancakova A, Peltonen M, Eriksson JG, Lindstrom J, Aunola S, et al. Impact of positive family history and genetic risk variants on the incidence of diabetes: the Finnish Diabetes Prevention Study. Diabetes Care. 2011;34(2):418–423. doi: 10.2337/dc10-1013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 107.Vanderwood KK, Hall TO, Harwell TS, Butcher MK, Helgerson SD, Montana Cardiovascular Disease and Diabetes Prevention Program Workgroup Implementing a state-based cardiovascular disease and diabetes prevention program. Diabetes Care. 2010;33(12):2543–2545. doi: 10.2337/dc10-0862. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 108.Vermunt PW, Milder IE, Wielaard F, de Vries JH, Baan CA, van Oers JA, et al. A lifestyle intervention to reduce Type 2 diabetes risk in Dutch primary care: 2.5-year results of a randomized controlled trial. Diabet Med. 2012;29(8):e223–e231. doi: 10.1111/j.1464-5491.2012.03648.x. [DOI] [PubMed] [Google Scholar]
- 109.Vlaar EM, van Valkengoed IG, Nierkens V, Nicolaou M, Middelkoop BJ, Stronks K. Feasibility and effectiveness of a targeted diabetes prevention program for 18 to 60-year-old South Asian migrants: design and methods of the DH!AAN study. BMC Public Health. 2012;12:371. doi: 10.1186/1471-2458-12-371. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Vojta D, Koehler TB, Longjohn M, Lever JA, Caputo NF. A coordinated national model for diabetes prevention: linking health systems to an evidence-based community program. Am J Prev Med. 2013;44(4 Suppl 4):S301–S306. doi: 10.1016/j.amepre.2012.12.018. [DOI] [PubMed] [Google Scholar]
- 111.West DS, Elaine PT, Bursac Z, Felix HC. Weight loss of black, white, and Hispanic men and women in the Diabetes Prevention Program. Obesity (Silver Spring) 2008;16(6):1413–1420. doi: 10.1038/oby.2008.224. [DOI] [PubMed] [Google Scholar]
- 112.Wikstrom K, Peltonen M, Eriksson JG, Aunola S, Ilanne-Parikka P, Keinanen-Kiukaanniemi S, et al. Educational attainment and effectiveness of lifestyle intervention in the Finnish Diabetes Prevention Study. Diabetes Res Clin Pract. 2009;86(1):e1–e5. doi: 10.1016/j.diabres.2009.06.014. [DOI] [PubMed] [Google Scholar]
- 113.Wing RR, Hamman RF, Bray GA, Delahanty L, Edelstein SL, Hill JO, et al. Achieving weight and activity goals among diabetes prevention program lifestyle participants. Obes Res. 2004;12(9):1426–1434. doi: 10.1038/oby.2004.179. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Xiao L, Yank V, Wilson SR, Lavori PW, Ma J. Two-year weight-loss maintenance in primary care-based Diabetes Prevention Program lifestyle interventions. Nutr Diabetes. 2013;3:e76. doi: 10.1038/nutd.2013.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.Trief PM, Cibula D, Delahanty LM, Weinstock RS. Depression, stress, and weight loss in individuals with metabolic syndrome in SHINE, a DPP translation study. Obesity (Silver Spring) 2014;22(12):2532–8. doi: 10.1002/oby.20916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 116.Diabetes Prevention Program Research Group. HbA1c as a predictor of diabetes and as an outcome in the diabetes prevention program: a randomized clinical trial. Diabetes Care. 2015;38(1):51–8. doi: 10.2337/dc14-0886. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 117.Rautio N, Jokelainen J, Oksa H, Saaristo T, Moilanen L, Vanhala M, et al. Do depressive symptoms have an impact on the effectiveness of lifestyle counseling in prevention of type 2 diabetes? One-year follow-up of FIN-D2D. Prim Care Diabetes. 2014;8(1):43–7. doi: 10.1016/j.pcd.2013.10.005. [DOI] [PubMed] [Google Scholar]
- 118.den Boer AT, Herraets IJ, Stegen J, Roumen C, Corpeleijn E, Schaper NC, et al. Prevention of the metabolic syndrome in IGT subjects in a lifestyle intervention: results from the SLIM study. Nutr Metab Cardiovasc Dis. 2013;23(11):1147–53. doi: 10.1016/j.numecd.2012.12.005. [DOI] [PubMed] [Google Scholar]
- 119.Azar KM, Xiao L, Ma J. Baseline obesity status modifies effectiveness of adapted diabetes prevention program lifestyle interventions for weight management in primary care. Biomed Res Int. 2013;2013:191209. doi: 10.1155/2013/191209. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 120.Alibasic E, Ramic E, Alic A. Prevention of diabetes in family medicine. Mater Sociomed. 2013;25(2):80–82. doi: 10.5455/msm.2013.25.80-82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 121.Gillett M, Royle P, Snaith A, Scotland G, Poobalan A, Imamura M, et al. Non-pharmacological interventions to reduce the risk of diabetes in people with impaired glucose regulation: a systematic review and economic evaluation. Health Technol Assess. 2012;16(33):1–236. doi: 10.3310/hta16330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 122.Schellenberg ES, Dryden DM, Vandermeer B, Ha C, Korownyk C. Lifestyle interventions for patients with and at risk for type 2 diabetes: a systematic review and meta-analysis. Ann Intern Med. 2013;159(8):543–551. doi: 10.7326/0003-4819-159-8-201310150-00007. [DOI] [PubMed] [Google Scholar]
- 123.Dunkley AJ, Bodicoat DH, Greaves CJ, Russell C, Yates T, Davies MJ, et al. Diabetes prevention in the real world: effectiveness of pragmatic lifestyle interventions for the prevention of type 2 diabetes and of the impact of adherence to guideline recommendations: a systematic review and meta-analysis. Diabetes Care. 2014;37(4):922–33. doi: 10.2337/dc13-2195. [DOI] [PubMed] [Google Scholar]
- 124.Aguiar EJ, Morgan PJ, Collins CE, Plotnikoff RC, Callister R. Efficacy of interventions that include diet, aerobic and resistance training components for type 2 diabetes prevention: a systematic review with meta-analysis. Int J Behav Nutr Phys Act. 2014;11:2. doi: 10.1186/1479-5868-11-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental Figure 1. Literature flow.
*Not already screened.
†Not a population of interest (n=71), diet or physical activity alone (n=58), protocol or baseline data only (n=26), no outcome of interest reported (n=25), not intervention of interest (n=20), cost-effectiveness analysis only (n=17), not a primary study (n=12), >10% of participants do not meet eligibility criteria (n=12), miscellaneous (n=7: prediction model, retrospective study, duplicate article).
‡plus 1 not analyzed due to limited quality of execution.
Supplemental Figure 2. Forest plot of RR of incident diabetes in at-risk participants in more vs. less intensive combined diet and physical activity promotion programs.
CI = confidence interval, RD = risk difference, RR = risk ratio.
Supplemental Figure 3. Forest plot of RR of reversion to normoglycemia in at-risk participants in more vs. less intensive combined diet and physical activity promotion programs.
CI = confidence interval, RD = risk difference, RR = risk ratio.
Supplemental Figure 4. Forest plot of net percent change in weight (from baseline) in at-risk participants in more vs. less intensive combined diet and physical activity promotion programs. CI = confidence interval, N = number of participants.
Supplemental Table 1. Search strategy.
Supplemental Table 2. Quality assessment of studies.
Supplemental Table 3. Study characteristics.
Supplemental Table 4. Intervention characteristics.
Supplemental Table 5. Studies using trainers or dietitians.
Supplemental Table 6. Participant characteristics.
Supplemental Table 7. Meta-analyses of glycemia measures, combined diet and physical activity promotion programs vs. usual care.
Supplemental Table 8. Meta-analyses of glycemia measures, more vs. less intensive combined diet and physical activity promotion programs.
Supplemental Table 9. Meta-analyses of blood pressure, combined diet and physical activity promotion programs vs. usual care.
Supplemental Table 10. Meta-analyses of lipids, combined diet and physical activity promotion programs vs. usual care.