

Abstract
Aims:
Comparative evaluation of EQUIA with a resin-modified glass ionomer cement (RMGIC; GC Gold Label glass ionomer light cured universal restorative cement) and a nanohybrid composite (Tetric N-Ceram) in noncarious cervical lesions (NCCLs).
Background:
To establish the most suitable material for the restoration of NCCLs.
Settings and Design:
In vivo study.
Materials and Methods:
Eighty-seven NCCLs were randomly restored with EQUIA, a RMGIC, and a nanohybrid composite. Clinical evaluation of the restorations was done following the Unites States Public Health criteria by a single-blinded investigator. Data were formulated, and statistical analysis was done by Chi-square test.
Statistical Analysis Used:
Chi-square test.
Results:
No significant difference was found between EQUIA, RMGIC, and nanohybrid composite at 1-month, at 6 months, and at 1-year (P > 0.05).
Conclusions:
EQUIA, resin-modified glass ionomer, and nanohybrid composite performed equally at 1-month, 6 months, and 1-year follow-up periods.
Keywords: EQUIA, nanohybrid composite, noncarious cervical lesions, resin-modified glass ionomer, Unites States Public Health Criteria
INTRODUCTION
Noncarious cervical lesions (NCCLs) are defined as loss of dental hard tissue in the cervical part of the tooth, with multicausal and insufficiently clarified etiology, but not caused by caries. Common problems associated with NCCLs are cosmetic problems, unpleasant hypersensitivity, plaque retention, caries incidence, painful sensations, pathological changes in the pulp, and eventually tooth loss.[1,2,3,4,5]
Special characteristics of these lesions include the presence of dentin or cementum in the gingival margins, microleakage and postoperative sensitivity, difficulty in moisture control and isolation, and lack of mechanical retention.[1,5] Higher failure rates of restorations in these lesions can be attributed to the role of mechanical stresses due to occlusal loading at the cervical margin leading to cuspal flexure.[6,7] Hence, a critical factor for the restorative success of cervical lesions is the selection of the restorative materials.[6] Currently, the materials of choice include conventional glass ionomer cements (GICs), composite resins, and their combinations.[8]
Resin-modified GIC (RMGIC) has resin monomers, like HEMA or Bis-GMA incorporated in its composition, making it a dual-cured cement having higher flexural, compressive, and tensile strengths than conventional GICs.[8]
EQUIA (GC, America) is a new glass ionomer restorative system. It is a combination of a self-adhesive, chemically cured, highly filled GIC (Fuji IX GP Extra, GC) and a self-adhesive, light cured, filled resin surface sealant (G-Coat Plus, GC). The manufacturers of EQUIA claim that the material has increased fracture toughness, flexural strength, and flexural fatigue resistance which are required in Class V restorations.[9,10]
Nanohybrid composites contain nanofillers and have a significant increase in the filler content leading to considerable improvement in the material's physical properties.[11,12,13,14,15]
As limited literature is available comparing the clinical evaluation of EQUIA with other commonly used restorative materials in NCCLs, the purpose of this study was to compare and evaluate EQUIA with RMGIC and a nanohybrid composite and also to determine which material is best suited to restore NCCLs. The null hypothesis is that there is no difference in the clinical performance of EQUIA, RMGIC, and nanohybrid composite at 1-year.
MATERIALS AND METHODS
This study was conducted from February 2013 to August 2014 after obtaining ethical clearance. A total of 87 lesions in 29 patients aged from 20 to 60 years, in vital teeth with normal occlusion and interproximal contact, with a minimum of three NCCLs in the same quadrant, with a depth of 1-3 mm were restored after obtaining signed informed consent from all patients. Teeth with parafunctional tooth wear, caries, poor oral hygiene, discolorations, periodontitis, and subgingival lesions were excluded from the study. The minimum sample size required for the study was 72 (24 per group) with 95% confidence interval and 80% power. However, as the study required follow ups by the subjects, a higher sample size of 87 was considered. Preoperative sensitivity was recorded by taking history and by clinical examination. Oral prophylaxis was carried out in all the subjects 2 weeks before the placement of the restoration. The selected lesions were assigned to Group A - RMGIC, Group B - EQUIA, and Group C - Nanohybrid composite by computer randomization.
The lesions were cleaned with prophylaxis paste and rubber cup to remove deposits at the time of the restoration. Other than this, no mechanical preparation or abrasion of the tooth surface was done. Shade selection was carried out using Vitapan classic shade guide (Zanfabrik H. Ranter Gmbh & Co., KG Germany). Isolation was achieved using cotton rolls and saliva ejector. Gingival retraction cord (Ultradent, UT, USA) was used where equigingival margins were present. Restorations were done using GC Gold Label Glass ionomer light cured universal restorative (GC Corporation, Tokyo, Japan) and dentin conditioner in Group A (GC Corporation, Tokyo, Japan). In Group B, GC Fuji IX GP Extra (EQUIA) (GC Corporation, Tokyo, Japan), GC G-Coat Plus (EQUIA) (GC Corporation, Tokyo, Japan) and dentin conditioner were used and in Group C, Tetric-N-Ceram starter kit (Ivoclar, Vivadent) was used. Placement of restorations was done according to manufacturer's instructions by a single operator. All restorations were contoured with transparent cervical matrices (KerrHawe, CA, USA) before curing.
All the restorations were finished under water cooling using fine and superfine diamond points (S.S. White, NY, USA). Polishing was carried out with polishing discs (SuperSnap, Shofu Co., Kyoto, Japan). Subjects were instructed to use a soft brush with a toothpaste and were taught the correct brushing technique.
The subjects were recalled at the end of 1-month, 6 months, and 1-year for evaluation of retention, staining, marginal staining, marginal adaptation, surface roughness, and postoperative sensitivity of the restorations according to Unites States Public Health (USPHS) criterion. The evaluation was carried out by a single-blinded investigator using a mirror and explorer under a good operating light. The operator was not involved in the evaluation of the restorations. The data were entered into spreadsheets, and Chi-square test was applied using software SPSS version 18 by IBM SPSS Statistics (P = 0.05).
RESULTS
In the present study, 3 patients out of a total 29 patients did not return for any of the follow-up periods. Out of the remaining 26 patients, 1 patient did not return for follow-up at 6 months and 1-year. Thus, the dropout percentage was 13.05%. Hence, in the present study, after making allowance for the drop outs, a total of 78 restorations in 26 patients were considered. Of the 26 patients treated, 18 were male and 8 were female. The ages of 4 patients were between 40 and 50 years, while the ages of rest 20 patients were between 50 and 60 years. Of all 78 restorations, 42 were present in maxillary teeth, and 36 were in mandibular teeth, and preoperative sensitivity was seen in 46 lesions. Tables 1 and 2 show the comparative clinical data at the three follow-up periods for retention and staining.
Table 1.
Comparison of EQUIA, RMGIC, and nanohybrid composite for retention at different time intervals
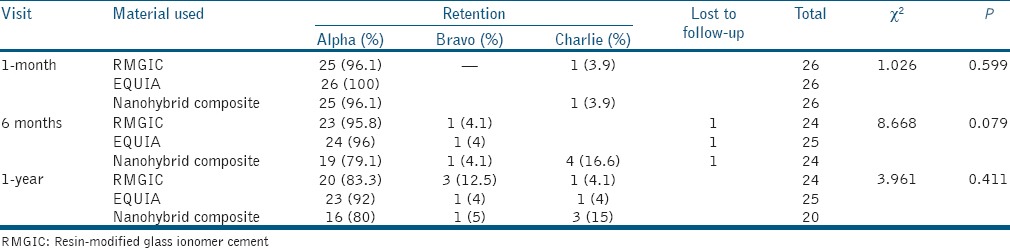
Table 2.
Comparison of EQUIA, RMGIC, and nanohybrid composite for staining at different time intervals
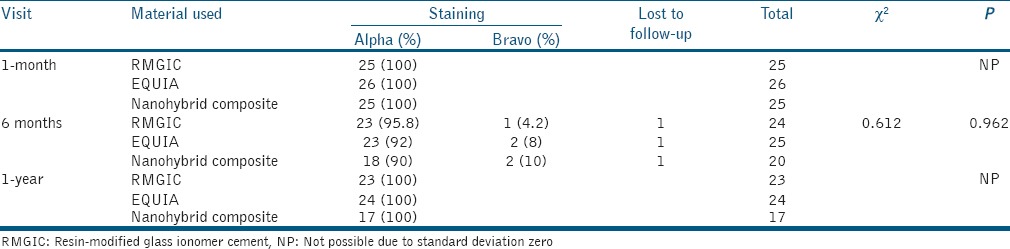
The statistical analysis showed no significant difference in the clinical performance of EQUIA, RMGIC, and nanohybrid composite for retention, staining, marginal staining, marginal adaptation, surface roughness, and postoperative sensitivity in NCCLs at 1-month, 6 months, and 1-year (P > 0.05).
DISCUSSION
The present study used the USPHS criteria for clinical evaluation of the restorations. This system was developed by Cvar and Ryge in 1971[26] and has been used extensively for clinical evaluation of restorations.[5,16]
Retention of the restorations is a function of bond strength.[17,18] Adhesion of EQUIA which uses Fuji IX GP Extra, a highly filled GIC, to dentin occurs by a micromechanical interlocking and a chemical bonding with the hydroxyapatite in enamel and dentin. Adhesion of RMGIC has been proposed by two mechanisms. First, bonding with the formation of an ion-exchange layer as seen with conventional GICs and second, bonding with the formation of a modified hybrid zone with the tooth structure. For composite resins, bonding to dentin is via the formation of the hybrid layer. A micromechanical interlocking occurs by the diffusion of resins around dentinal collagen fibrils that have been exposed by demineralization. The bond strength of GIC to dentin ranges from 3 to 10 Mpa, bond strength of RMGIC to dentin ranges from 13.56 to 19.67 MPa, while that of composite is higher and ranges from 16.84 to 23.34 MPa. In the present study, there was no significant difference found in the retention rates between the three materials at any follow-up periods. However, higher restorations were lost in the nanohybrid composite group at 1-year, in spite of it having higher bond strengths as compared to RMGIC and EQUIA. Similar results have been found by Brackett et al. and Santiago et al. In another study, Brackett et al. found RMGIC to have better retention rates than composite, although not significant.[19,20,21,22]
The failure of the restorative materials in NCCLs has been reported to be multifactorial. Some of the contributing factors are the sclerosed dentin, location of the lesion, shape of lesion, occlusal factors, absence of bevel, absence of etching, and application of adhesive for RMGIC and EQUIA, elasticity of the restorative material, and type of dentin used for bonding. A significant factor for failure in NCCL is the elasticity of the restorative material. A more rigid material, like composite, will not withstand the stress acting at the adhesive interface when the tooth is undergoing flexion during occlusal loading, which could result in debonding. This could have resulted in higher failure rates of composite restorations. Another factor is the type of dentin used for bonding. It is known that as the dentin ages, a higher amount of calcification is seen, which could negatively affect adhesion of the material. In the present study, the majority of the subjects were aged between 50 and 60 years, thus having a more calcified tooth structure, which could have contributed to less retention of composite restorations.[20,21,22,23,24,25]
Contradictory to the results of the present study, Folwaczny et al. found better retention rate of composite as compared to RMGIC. In their study, they had used bevels for composite restorations, which probably resulted in better retention of restorations.[25]
Staining depends partly on the surface texture and roughness. A smooth surface will take up fewer stains as compared to a rough surface and requires the use of finishing and polishing systems. The finished or polished surface is filler/glass rich and more characteristic of the particles in the bulk material. The size of the large fluoroamino silicate particles of the GIC cements range from 4 to 8 μm, while the mean particle size of the nanohybrid composites is <1 μm. In the present study, all restorations were scored alpha at 1-year follow-up. Similar results were found by Smales et al. and Folwaczny et al. However, Brackett et al. found resin composites to have a better color match as compared to RMGIC at the end of 2 years.[22,23,24,25] This discrepancy in the results could have been because of the longer periods of follow-up (2-5 years) in these studies as compared to the 1-year follow-up in our study.[15]
Thus, within the limitations of this study, it can be concluded that:
There was no statistically significant difference seen between clinical performance of EQUIA, RMGIC, and nanohybrid composite
Higher rates of restoration loss were associated with nanohybrid composite, but the results were not statistically significant
In all other criteria, the three restorative materials showed similar results
Clinically, EQUIA showed an overall better performance than the other two materials. However, more studies conducted over a longer period and with a higher number of samples are required to conclusively compare the three materials.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Francisconi LF, Scaffa PM, de Barros VR, Coutinho M, Francisconi PA. Glass ionomer cements and their role in the restoration of non-carious cervical lesions. J Appl Oral Sci. 2009;17:364–9. doi: 10.1590/S1678-77572009000500003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Perez Cdos R, Gonzalez MR, Prado NA, de Miranda MS, Macêdo Mde A, Fernandes BM. Restoration of noncarious cervical lesions: When, why, and how. Int J Dent 2012. 2012 doi: 10.1155/2012/687058. 687058. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Qin W, Song Z, Ye YY, Lin ZM. Two-year clinical evaluation of composite resins in non-carious cervical lesions. Clin Oral Investig. 2013;17:799–804. doi: 10.1007/s00784-012-0780-7. [DOI] [PubMed] [Google Scholar]
- 4.Jakupovic S, Vukovic A, Korac S, Tahmiscija I, Bajsman A. The prevalence, distribution and expression of noncarious cervical lesions (NCCL) in permanent dentition. Mater Sociomed. 2010;22:200–4. [Google Scholar]
- 5.Jyothi K, Annapurna S, Kumar AS, Venugopal P, Jayashankara C. Clinical evaluation of giomer- and resin-modified glass ionomer cement in class V noncarious cervical lesions: An in vivo study. J Conserv Dent. 2011;14:409–13. doi: 10.4103/0972-0707.87214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ichim IP, Schmidlin PR, Li Q, Kieser JA, Swain MV. Restoration of non-carious cervical lesions part II. Restorative material selection to minimise fracture. Dent Mater. 2007;23:1562–9. doi: 10.1016/j.dental.2007.02.002. [DOI] [PubMed] [Google Scholar]
- 7.Vasudeva G, Bogra P, Nikhil V, Singh V. Effect of occlusal restoration on stresses around class V restoration interface: A finite-element study. Indian J Dent Res. 2011;22:295–302. doi: 10.4103/0970-9290.84308. [DOI] [PubMed] [Google Scholar]
- 8.Burrow MF, Tyas MJ. Clinical evaluation of three adhesive systems for the restoration of non-carious cervical lesions. Oper Dent. 2007;32:11–5. doi: 10.2341/06-50. [DOI] [PubMed] [Google Scholar]
- 9.Zoergiebel J, Ilie N. Evaluation of a conventional glass ionomer cement with new zinc formulation: Effect of coating, aging and storage agents. Clin Oral Investig. 2013;17:619–26. doi: 10.1007/s00784-012-0733-1. [DOI] [PubMed] [Google Scholar]
- 10.Cohen C. New Glass Ionomer System and Application in Children. [Last accessed on 2015 Sep 20]. Available from: http://www.oralhealthgroup.com/news/new-glass-ionomer-systemand-application-in-children/1000536399/
- 11.Umer F, Naz F, Khan FR. An in vitro evaluation of microleakage in class V preparations restored with hybrid versus silorane composites. J Conserv Dent. 2011;14:103–7. doi: 10.4103/0972-0707.82600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Giacomelli L, Derchi G, Frustaci A, Orlando B, Covani U, Barone A, et al. Surface roughness of commercial composites after different polishing protocols: An analysis with atomic force microscopy. Open Dent J. 2010;4:191–4. doi: 10.2174/1874210601004010191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Eliguzeloglu Dalkilic E, Omurlu H. Two-year clinical evaluation of three adhesive systems in non-carious cervical lesions. J Appl Oral Sci. 2012;20:192–9. doi: 10.1590/S1678-77572012000200012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Karan K, Yao X, Xu C, Wang Y. Chemical profile of the dentin substrate in non-carious cervical lesions. Dent Mater. 2009;25:1205–12. doi: 10.1016/j.dental.2009.04.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Palaniappan S, Elsen L, Lijnen I, Peumans M, Van Meerbeek B, Lambrechts P. Three-year randomised clinical trial to evaluate the clinical performance, quantitative and qualitative wear patterns of hybrid composite restorations. Clin Oral Investig. 2010;14:441–58. doi: 10.1007/s00784-009-0313-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bayne SC, Schmalz G. Reprinting the classic article on USPHS evaluation methods for measuring the clinical research performance of restorative materials. Clin Oral Investig. 2005;9:209–14. doi: 10.1007/s00784-005-0017-0. [DOI] [PubMed] [Google Scholar]
- 17.Tyas MJ, Burrow MF. Adhesive restorative materials: A review. Aust Dent J. 2004;49:112–21. doi: 10.1111/j.1834-7819.2004.tb00059.x. [DOI] [PubMed] [Google Scholar]
- 18.Poggio C, Beltrami R, Scribante A, Colombo M, Lombardini M. Effects of dentin surface treatments on shear bond strength of glass-ionomer cements. Ann Stomatol (Roma) 2014;5:15–22. [PMC free article] [PubMed] [Google Scholar]
- 19.Santiago SL, Passos VF, Vieira AH, Navarro MF, Lauris JR, Franco EB. Two-year clinical evaluation of resinous restorative systems in non-carious cervical lesions. Braz Dent J. 2010;21:229–34. doi: 10.1590/s0103-64402010000300010. [DOI] [PubMed] [Google Scholar]
- 20.Santiago SL, Franco EB, Mendonça JS, Lauris JR, Navarro MF. One-year clinical evaluation of tooth-colored materials in non-carious cervical lesions. J Appl Oral Sci. 2003;11:175–80. doi: 10.1590/s1678-77572003000300004. [DOI] [PubMed] [Google Scholar]
- 21.Brackett MG, Dib A, Brackett WW, Estrada BE, Reyes AA. One-year clinical performance of a resin-modified glass ionomer and a resin composite restorative material in unprepared class V restorations. Oper Dent. 2002;27:112–6. [PubMed] [Google Scholar]
- 22.Brackett WW, Dib A, Brackett MG, Reyes AA, Estrada BE. Two-year clinical performance of class V resin-modified glass-lonomer and resin composite restorations. Oper Dent. 2003;28:477–81. [PubMed] [Google Scholar]
- 23.Hur B, Kim HC, Park JK, Versluis A. Characteristics of non-carious cervical lesions — An ex vivo study using micro computed tomography. J Oral Rehabil. 2011;38:469–74. doi: 10.1111/j.1365-2842.2010.02172.x. [DOI] [PubMed] [Google Scholar]
- 24.Smales RJ, Ng KK. Longevity of a resin-modified glass ionomer cement and a polyacid-modified resin composite restoring non-carious cervical lesions in a general dental practice. Aust Dent J. 2004;49:196–200. doi: 10.1111/j.1834-7819.2004.tb00073.x. [DOI] [PubMed] [Google Scholar]
- 25.Folwaczny M, Loher C, Mehl A, Kunzelmann KH, Hinkel R. Tooth-colored filling materials for the restoration of cervical lesions: A 24-month follow-up study. Oper Dent. 2000;25:251–8. [PubMed] [Google Scholar]
- 26.Cvar JF, Ryge G. Reprint of criteria for the clinical evaluation of dental restorative materials. 1971. Clin Oral Investig. 2005;9:215–32. doi: 10.1007/s00784-005-0018-z. [DOI] [PubMed] [Google Scholar]