

Abstract
Background: Radiotherapy and laser resection are established treatment modalities for early glottic carcinoma. To date, there is no confirmed conclusion which treatment is better for early glottic cancer. The objective of this study was to conduct a meta-analysis to compare the voice outcomes after laser resection (LS) and radiotherapy (RT) of Tis-T1N0M0 glottic carcinoma. Methods: we searched the relevant electronic studies and performed a meta-analysis based on 13 published studies. The Chi-square based I2-statistic test was performed to evaluate possible heterogeneity across the studies. Additionally, random-effects models were used to calculate mean differences with 95% confidence intervals (CIs). Results: Overall, a total of 13 published studies were included in our study, with 368 patients in the RT group and 440 patients in the LS group, respectively. No significant differences in Voice Handicap Index (VHI), jitter and shimmer were found between RT and endoscopic LS among patients with Tis-T1N0M0 glottic carcinoma and T1aN0M0 laryngeal cancer. However, the acoustic voice analysis parameters of Fo values were significantly lower in RT group than that in LS group. Conclusion: The results from this meta-analysis support that the LS has more advantages than RT in terms of voice quality. However, more studies on voice outcome need to validate our findings.
Keywords: Voice outcome, laser resection, radiotherapy, early glottis carcinoma, meta-analysis
Introduction
Laryngeal cancer is one of the most common squamous cell carcinoma of head and neck and has four subtypes: glottic cancer, supraglottic cancer, subglottic cancer and transglottic cancer, among which the glottic cancer is most common. How to better treat the early glottic carcinoma has attracted many clinici-ans and surgeons to focus on this disease. Currently, early glottic cancer can be treated with laser surgery (LS), radiotherapy (RT), and conventional surgery. Evidences have revealed that the average of 5-year survival rate in early glottic cancer is over 90% [1]. Local control rates range from 71-100% for LS and from 73-95% for RT in T1 carcinomas without involvement of the anterior commissure [2]. To improve quality of life and functional preservation after treatment of such patients, the clinicians need to evaluate the voice outcomes, costs and the average treatment time. The acoustic analysis is an objective method to evaluate laryngeal pronunciation function, because it is noninvasive and has the potential to provide quantitative data which may be highly descriptive of vocal fold vibrations and favorable for clinicians [1,3].
The Voice Handicap Index (VHI) is a self-administered questionnaire for measuring the impact of voice disorder on a person’s vocal functions, vocal physical ability, and emotion [4]. Because VHI has the characteristics of subjective evaluation and can be used to fully and effectively evaluate the characteristics of voice, it has been adopted as a valid instrument worldwide [4-7]. Several studies have compared the voice outcome between the treatment of LS and RT, but the findings are not consistent. Additionally, each of these studies included a limited number of study patients. Therefore, in the current meta-analysis, we gave a more comprehensive overview of evaluation of voice assessment after LS and RT in patients with early glottic carcinoma, including journal articles published up to May 30, 2015.
Methods
Search strategy
We conducted a literature search through May 30, 2015 using the key words search in the PubMed, Web of Knowledge, MEDLINE, Embase, and Google Scholar electronic databases and search engines. The language of publication was restricted to English. The following search terms were used: laryngeal carcinoma or surgical or radiotherapy.
Inclusion criteria
All relevant studies reporting the association of voice results after laser resection or RT of early glottic carcinoma were considered for inclusion. The inclusion criteria were as follows: 1) Study patients with clinically pathologically confirmed squamous cell carcinoma of glottis, according to Union for International Cancer Control (UICC) or American Joint Committee On Cancer (AJCC) and with clinical stage of Tis-T1N0M0 glottis type of laryngeal cancer or T1aN0M0 laryngeal cancer; 2) All study patients were the first time for endoscopic LS or RT; 3) The studies included the comparison information between the patients with LS and RT treatment; and 4) The research outcome measure included voice handicap index (VHI) and acoustic voice analysis parameters [8]. The questionnaire of VHI consists of 30 statements on voice-related aspects on daily life (5-point rating scale) with a total score for the 30 questions from 0 to 120 [8].
Exclusion criteria
The exclusion criteria were as follows: 1) unable to get the full text of the literature; 2) duplicate reports; 3) information and data is incomplete; 4) lost of follow-up or death; and 5) data provided in obvious errors.
Data extraction
Three investigators reviewed and extracted information independently from selected publications in accordance with the above mentioned inclusion and exclusion criteria. Any conflicts over study/data inclusion were settled by a discussion between the investigators. These investigators independently extracted the following information: name of the first author, publication year, sample size, the objects of study, period of treatment, outcome indicators. Quality evaluation was performed by the three investigators independently according to the Cochran’s system manual (version 5.1.0) quality evaluation standard.
Statistical analysis
This analysis adopts the Cochrance registries that provide Revman 5.3 meta-analysis software. Firstly, we used the fixed effects model to incorporate data from each study, then performed the heterogeneity test for P values and I2 index to estimate the degree of heterogeneity in literature. If P > 0.05 and I2 < 50%, we considered that the analysis had the homogeneity. If P < 0.05, and I2 > 50%, we considered that the analysis had heterogeneity; then the sensitivity analysis was needed to assess potential sources of the heterogeneity. Sensitivity analyses were conducted to assess the strength of our findings by excluding one study at a time. Begg’s funnel plot and Egger’s regression test were used to evaluate publication bias. In Egger’s test, when P value < 0.10, it was considered statistically significant publication bias. All analyses were conducted using Stata v.12 (StataCorp LP, TX) statistical software. If heterogeneity was too large or clinical data provided was not sufficient, random-effect model should be used.
Results
Characteristics of included studies
Our keyword search identified from the literature a total of 13 articles which were included in our study [1,9-19,21], of which 368 patients with RT and 440 patients with LS, respectively as shown in Table 1. Among them, 7 studies contained the data on VHI; and 8 had the data on acoustic voice analyses. None of them was completely randomized studies in study design; 3 studies were prospective [1,16,17]; and the rest of them were retrospective.
Table 1.
Characteristics of included studies
| Studies | Sample | Follow-up time (month) | Radiation dose (Gy) | ||
|---|---|---|---|---|---|
|
|
|||||
| RT | LS | RT | LS | ||
| Jotic 2012 [16] | 15 | 19 | 12 | 12 | 60 |
| Christine 2012 [17] | 39 | 67 | 24 | 24 | 57.5-60 |
| Sjogren 2008 [11] | 15 | 18 | 60 | 45 | N |
| Tamura 2003 [18] | 6 | 14 | 21.3 | 26.3 | 60-66 |
| Batalla 2008 [12] | 18 | 19 | 43 | 30 | 65.3 |
| Wedman 2002 [19] | 9 | 15 | ≥ 24 | ≥ 24 | 66 |
| Milovanovic 2013 [1] | 74 | 72 | ≥ 38 | ≥ 38 | 60-64 |
| Policarpo 2004 [21] | 20 | 20 | 64.9 | 64.9 | 66-70 |
| Peeters 2004 [9] | 40 | 52 | ≥ 12 | ≥ 12 | 50-70 |
| Remmelts 20013 [10] | 45 | 57 | ≥ 12 | ≥ 12 | 52-70 |
| Goor 2007 [13] | 20 | 36 | 24 | 24 | 60 |
| Loughran 2005 [14] | 18 | 18 | 27.6 | 31.4 | 55 |
| Dinapoli 2010 [15] | 49 | 33 | 60 | 60 | 69.6-70.2 |
VHI analyses
Seven studies contained data on VHI, with 206 patients in the RT group and 233 patients in the LS group, respectively [9-15]. The result from the merged analysis showed a significant heterogeneity (chi2 = 17.2, P = 0 .009, I2 = 65%), so a random effect model was used to calculate the pooled effect. Our current meta-analysis did not find a significant difference between patients with RT and LS (mean difference: -5.12; 95% CI, -11.1-0.82, P = 0.09) as shown in Figure 1. Due to the obvious heterogeneity, we removed the proportion of the largest groups, and we repeated the analysis which indicated that there were still no statistically significant differences. As shown in Figures 1, 4 studies [9,11,13,14] found no differences in voice outcome after LS and RT when using VHI in patients with glottic Tis-T1N0M0 laryngeal carcinoma. Three other studies [10,12,15] showed that the quality of voice, when analyzing VHI in patients withTis-T1N0M0 glottic carcinoma, is significantly better for patients with RT than those with LS. When patients with T1aN0M0 laryngeal cancer was also included in our study, 5 studies contained data on VHI, with 125 patients in the RT group and 160 patients in the LS group, respectively [9-11,13,14]. Analysis results meet the homogeneity (chi2 = 3.94, P =0.41, I2 = 0%), thus we choose the fixed model for data integration, and no obvious difference was found between experimental group and control group (mean difference, -2.19, 95% CI, -5.75-1.37, P = 0.023) as shown in Figure 2.
Figure 1.
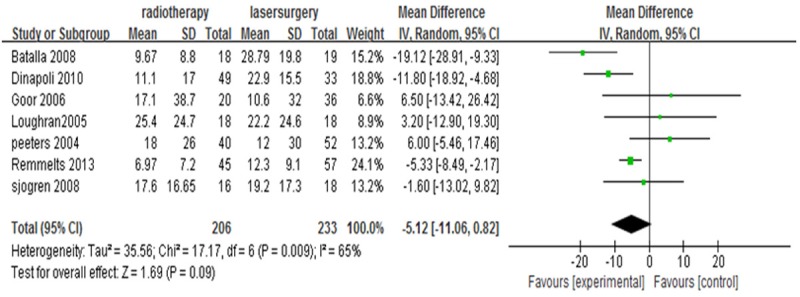
VHI (RT VS. LS of Tis-T1N0M0).
Figure 4.
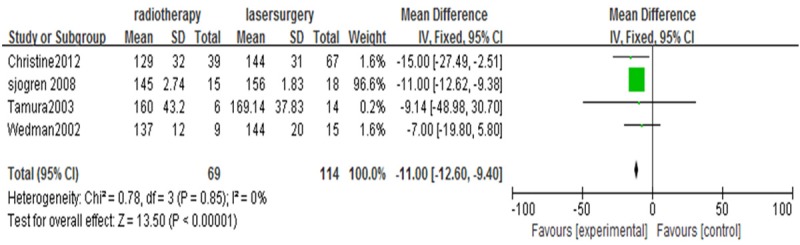
Fo (RT VS. LS of T1aN0M0).
Figure 2.
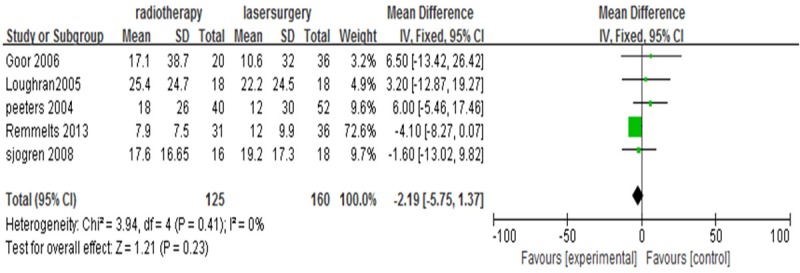
VHI (RT VS. LS of T1aN0M0).
Acoustic voice analyses
We analyzed acoustic voice from three aspects: fundamental frequency (F0, Hz), jitter (%), and shimmer (%). Among the studies, there of 8 studies [11,12,16-21] provided detailed data on F0 among 196 patients in the RT group and 244 patients in the LS group. Analysis results met the homogeneity (chi2 = 18.32, P = 0.01, I2 = 62%), we thus chose the random effect model for data integration. We found that the Values of Fo were strongly significantly lower in RT group (mean difference, -6.55, 95% CI, -12.2-0, 94, P = 0.02) (Figure 3). Among four studies contained data on Fo among patients with T1aN0M0 laryngeal cancer, there were 69 patients in the RT group and 114 patients in the LS group, respectively [11,17-19]. The analysis of heterogeneity showed that there were no heterogeneities among the studies (chi2 = 0.78, P = 0.85, I2 = 0%), thus, a fixed model was used for the meta-analysis. Values of F0 were also strongly significantly lower in RT group (mean difference, -11.0, 95% CI, -12.6-9.4], P < 0.00001 (Figure 4).
Figure 3.
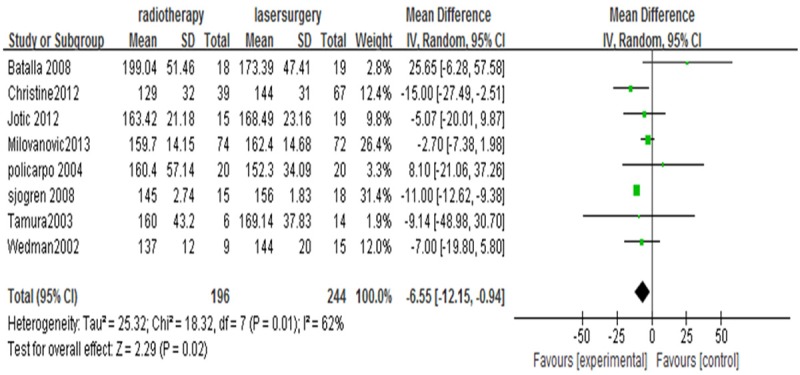
Fo (RT VS. LS of Tis-T1N0M0).
The Shimmer was reported in 6 trials [1,12,17-19,21], with 166 patients in the RT group and 171 patients in the LS group, respectively. The heterogeneity was identified between the studies (chi2 = 13.9, P = 0 .02, I2 = 64%), thus a random effect model was used for data integration. The results showed that the difference between experimental group and control group with respect to the shimmer was not significant (mean difference, -0.37, 95% CI, -1.24-0.50, P = 0.4) (Figure 5). The shimmer of T1aN0M0 glottic carcinoma was assessed in 3 studies [17-19] and no significant heterogeneity among the studies was found (chi2 = 2.38, P = 0.30, I2 = 16%), and thus a fixed model for the meta-analysis showed that there is no significant difference between T1aN0M0 glottic carcinoma patients with RT and LS in shimmer (mean difference, 0.19, 95% CI, -0.04-0.43, P = 0.100) (Figure 6).
Figure 5.
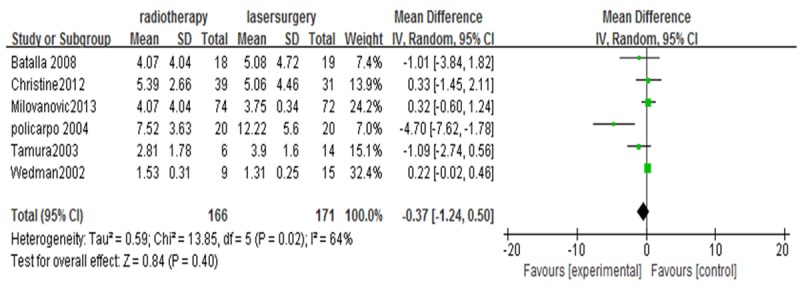
Shimmer (RT VS. LS of Tis-T1N0M0).
Figure 6.
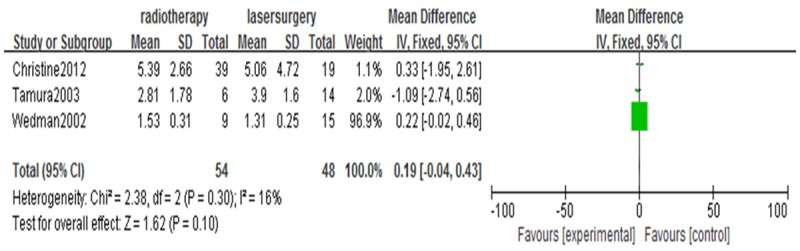
Shimmer (RT VS. LS of T1aN0M0).
The jitter was also reported in 6 studies [1,12,17-19,21]. The Heterogeneity was also identified (chi2 = 13.1, P = 0.02, I2 = 62%). No significant difference in jitter was found after incorporated data from each study (mean difference, -0.08, 95% CI, -0.36-0.20, P = 0.57) (Figure 7). The jitter of T1aN0M0 glottic cancer was assessed in 3 studies [17-19]. There was no heterogeneity among these studies (chi2 = 0.44, P = 0.8, I2 = 0%), and a fixed model was thus used for the meta-analysis. No a significant difference was found between the two groups when comparing the scores of the jitter parameter in patients with T1aN0M0 glottic cancer (mean difference, -0.03, 95% CI, -0.30-0.23, P = 0.8) (Figure 8).
Figure 7.
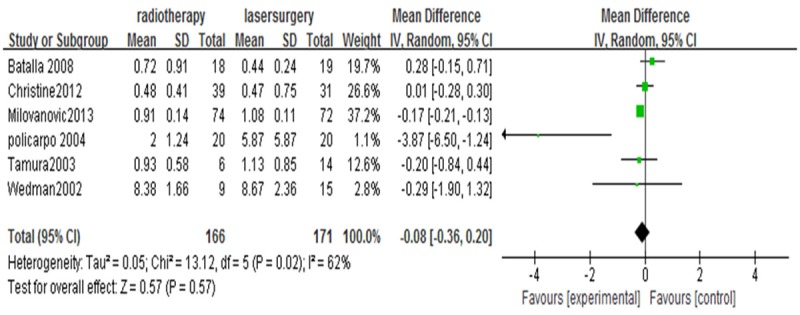
Jitter (RT VS. LS of T1s-T1N0M0).
Figure 8.
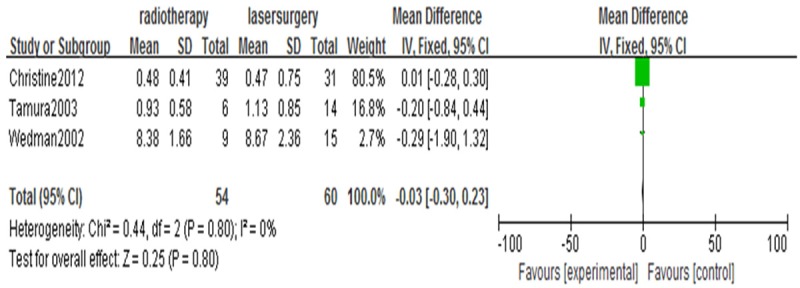
Jitter (RT VS. LS of TiaN0M0).
Publication bias
Begg’s funnel plot and Egger’s test were performed to assess the publication bias of our meta-analysis. As shown in Figure 9, the shapes of the funnel plots did not reveal any evidence of obvious asymmetry. Furthermore, the Egger’s test did not show any statistical evidence of publication bias (P = 0.623).
Figure 9.
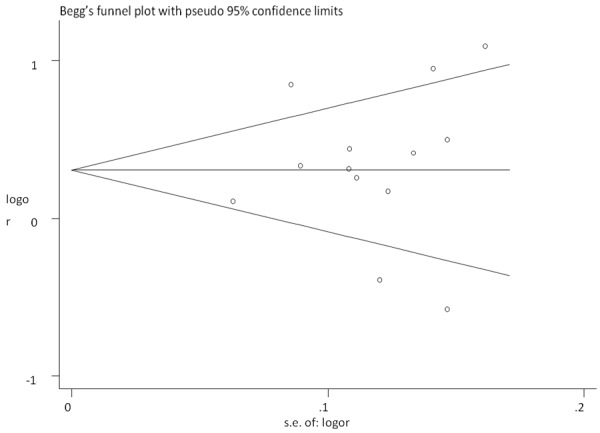
Begg’s funnel plot for publication bias test. Each point represents a separate study for the indicated association.
Discussion
RT and endoscopic LS are established treatment modalities for early glottic carcinoma. For each modality, it has its own advantages. The treatment of endoscopic LS is quicker and repeatable, has many salvage options, and do not develop mucositis [14]. RT has proven to have high efficacy, and possibly gives a better voice outcome [14]. However, to date, it is still unclear which treatment modalities patients with early glottic cancer should be used properly. It was reported that for early glottic carcinomas either transoral LS or primary high-dose RT is applied. RT is recommended for patients with tumors not suitable for LS because of anatomic reasons [22]. It is likely that the difference in outcome between two groups may be subtle and thus the assessment of possible outcome measures is essential [14].
In our meta-analysis, no significant differences in VHI, jitter and shimmer were found between RT and endoscopic LS in Tis-T1N0M0 glottic carcinoma or T1aN0M0 glottic carcinoma. However, in the current study, the values of F0 were significantly lower in RT group than that in LS group. Therefore, based on our above analysis, we suggest that the LS treatment may have some advantages in terms of voice quality than RT. However, we still have some limitations for such a research: (1) the sample sizes for the analysis is relatively small, selection bias could be excluded; (2) the study design for studies included for current analysis are not completely randomized controlled; and the proportion of the prospective study is relatively small. Most of them are retrospective studies, which may undoubtedly increase the heterogeneity of our analysis; and (3) the studies included from literature lack information on the radiation dose for RT and different choices of the laser equipment for LS, and such information may also cause additional heterogeneity among the studies. In addition, the choice of patient treatment generally depends on the clinician’s preferences, or the patient’s wishes. All the measurements of above factors lack the unified standards; and thus may have certain impact on the results. In conclusion, this meta-analysis demonstrates that the LS has more advantages than RT in terms of voice quality. To confirm our findings, more and well-designed large-scale studies are warranted.
Acknowledgements
This work was supported in part by a grant-in-aid from National clinical key discipline construction project (No. 2012-649), and the Chongqing medical research key project (No. 2013-1-004 to JZ).
Disclosure of conflict of interest
None.
Abbreviations
- LS
laser surgery
- RT
radiotherapy
- VHI
Voice Handicap Index
References
- 1.Jotic A, Stankovic P, Jesic S, Milovanovic J, Stojanovic M, Djukic V. Voice quality after treatment of early glottic carcinoma. J Voice. 2012;26:381–389. doi: 10.1016/j.jvoice.2011.04.004. [DOI] [PubMed] [Google Scholar]
- 2.Remmelts AJ, Hoebers FJ, Klop WMC. Evaluation of lasersurgery and radiotherapy as treatment modalities in early stage laryngeal carcinoma: tumour outcome and quality of voice. Eur Arch Otorhinolaryngol. 2013;270:2079–2087. doi: 10.1007/s00405-013-2460-x. [DOI] [PubMed] [Google Scholar]
- 3.Eadie TL, Doyle PC. Classification of dysphonic voice: acoustic and auditory-perceptual measures. J Voice. 2005;19:1–14. doi: 10.1016/j.jvoice.2004.02.002. [DOI] [PubMed] [Google Scholar]
- 4.Lam PK, Chan KM, Ho WK, Kwong E, Yiu EM, Wei WI. Cross-cultural adaptation and validation of the Chinese Voice Handicap Index-10. Laryngoscope. 2006;116:1192–1198. doi: 10.1097/01.mlg.0000224539.41003.93. [DOI] [PubMed] [Google Scholar]
- 5.Pruszewicz A, Obrebowski A, Wiskirska-Woznica B, Wojnowski W. Complex voice assessment: Polish version of the Voice Handicap Index (VHI) Otolaryngol Pol. 2004;58:547–549. [PubMed] [Google Scholar]
- 6.Guimaraes I, Abberton E. An investigation of the Voice Handicap Indix with speakers Portuguese: preliminary data. J Voice. 2004;18:71–82. doi: 10.1016/j.jvoice.2003.07.002. [DOI] [PubMed] [Google Scholar]
- 7.Husiung MW, LU P, Kang BH, Wang HW. Measurement and validation of the voice handicap index in voice disordered patients in Taiwan. J Laryngol Otol. 2003;117:478–481. doi: 10.1258/002221503321892334. [DOI] [PubMed] [Google Scholar]
- 8.van Gogh CD, Verdonck-de Leeuw IM, Boon-Kamma BA. The efficacy of voice therapy in patients after treatment for early glottic carcinoma. Cancer. 2006;106:95–105. doi: 10.1002/cncr.21578. [DOI] [PubMed] [Google Scholar]
- 9.Peeters AJ, van Gogh CD, Goor KM. Health status and voice outcome after treatment for T1a glottic carcinoma. Eur Arch Otorhinolaryngol. 2004;261:534–540. doi: 10.1007/s00405-003-0697-5. [DOI] [PubMed] [Google Scholar]
- 10.Remmelts AJ, Hoebers FJ, Klop WM. Evaluation of lasersurgery and radiotherapy as treatment modalities in early stage laryngeal carcinoma: tumour outcome and quality of voice. Eur Arch Otorhinolaryngol. 2013;270:2079–2087. doi: 10.1007/s00405-013-2460-x. [DOI] [PubMed] [Google Scholar]
- 11.Sjögren EV, van Rossum MA, Langeveld TP. Voice outcome in T1a midcord glottic carcinoma: laser surgery vs radiotherapy. Arch Otolaryngol Head Neck Surg. 2008;134:965–972. doi: 10.1001/archotol.134.9.965. [DOI] [PubMed] [Google Scholar]
- 12.Núñez Batalla F, Caminero Cueva MJ, Señaris González B. Voice quality after endoscopic laser surgery and radiotherapy for early glottic cancer: objective measurements emphasizing the Voice Handicap Index. Eur Arch Otorhinolaryngol. 2008;265:543–548. doi: 10.1007/s00405-007-0512-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Goor KM, Peeters AJ, Mahieu HF. Cordectomy by CO2 laser or radiotherapy for small T1a glottic carcinomas: costs, local control, survival, quality of life, and voice quality. Head Neck. 2007;29:128–136. doi: 10.1002/hed.20500. [DOI] [PubMed] [Google Scholar]
- 14.Loughran S, Calder N, MacGregor FB, Carding P, MacKenzie K. Quality of life and voice following endoscopic resection or radiotherapy for early glottic cancer. Clin Otolaryngol. 2005;30:42–47. doi: 10.1111/j.1365-2273.2004.00919.x. [DOI] [PubMed] [Google Scholar]
- 15.Dinapoli N, Parrilla C, Gallil J. Multidisciplinary approach in the treatment of T1 glottic cancer. Strahlenther Onkol. 2010;4:607–613. doi: 10.1007/s00066-010-2142-1. [DOI] [PubMed] [Google Scholar]
- 16.Jotic A, Stankovic P, Jesic S. Voice quality after treatment of early glottic carcinoma. J Voice. 2012;26:381–389. doi: 10.1016/j.jvoice.2011.04.004. [DOI] [PubMed] [Google Scholar]
- 17.van Gogh CD, Verdonck-de Leeuw IM, Wedler-Peeters J, Langendijk JA, Mahieu HF. Prospective evaluation of voice outcome during the first two years in male patients treated by radiotherapy or laser surgery for T1a glottic carcinoma. Eur Arch Otorhinolaryngol. 2012;269:1647–1652. doi: 10.1007/s00405-012-1947-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Tamura E, Kitahara S, Ogura M, Kohno N. Voice quality after laser surgery or radiotherapy for T1a glottic carcinoma. Laryngoscope. 2003;113:910–914. doi: 10.1097/00005537-200305000-00025. [DOI] [PubMed] [Google Scholar]
- 19.Wedman J, Heimdal JH, Elstad I, Olofsson J. Voice results in patients with T1a glottic cancer treated by radiotherapy or endoscopic measures. Eur Arch Otorhinolaryngol. 2002;259:547–550. doi: 10.1007/s00405-002-0478-6. [DOI] [PubMed] [Google Scholar]
- 20.Milovanovic J, Djukic V, Milovanovic A. Clinical outcome of early glottic carcinoma in Serbia. Auris Nasus Larynx. 2013;40:394–399. doi: 10.1016/j.anl.2012.11.013. [DOI] [PubMed] [Google Scholar]
- 21.Policarpo M, Aluffi P, Brovelli F, Borello G, Pia F. Oncological and functional results of CO2 laser cordectomy. Acta Otorhinolaryngol Ital. 2004;24:267–274. [PubMed] [Google Scholar]
- 22.Stoeckli SJ, Schnieper I, Huguenin P, Schmid S. Early glottic carcinoma: treatment according patient’s preference? Head Neck. 2003;25:1051–1056. doi: 10.1002/hed.10323. [DOI] [PubMed] [Google Scholar]