

Abstract
Objective: This study is to investigate anemia management trends in patients on peritoneal dialysis in Huashan Hospital in the past 10 years. Methods: A total of 463 cases of patients receiving peritoneal dialysis from July 2004 to March 2014 were analyzed retrospectively. The patients enrolled in this study all were elder than 18 years old, those who had been followed up for at least 1 quarter. Clinical data of anemia including hemoglobin, serum iron, iron saturation, dosage of erythropoietin (EPO) and iron supplements were collected quarterly and then analyzed those data. Results: In the first period of 25 quarters, in a certain range, increased dose of erythropoietin and iron content, can make the patient’s hemoglobin gradually increased to the ideal level, which helps to treat the symptoms of anemia patients. Results of comparation before and after the education program showed that with the enhance the EPO injection compliance and treat anemia with the proper dose of EPO, the PD patients have stable level of Hemoglobin, accompanying with the decreased dose of oral Iron and intravenous iron. Conclusion: It was shown that hemoglobin value was constantly stable. Treat anemia with proper dose of EPO individually could cure anemia effectively with the reducing of iron supplement improvement peritoneal dialysis patients’ anemia related knowledge, and the good compliance of injection of EPO, serum iron and iron saturation could still keep stable, although declined intake of iron supplements. Therefore, optimizing anemia management in peritoneal dialysis patients is helpful to improve their quality of life.
Keywords: Anemia, peritoneal dialysis, hemoglobin, erythropoietin, iron
Introduction
According to a report about 11041 cases of patients for more than six months from 309 dialysis centers within 12 countries in 2004, hemoglobin < 110 g/L is found in 23%-77% of the patients [1]. In the year of 2011, a report for 12 hospitals of Shanghai city shows that hemoglobin in 86.01% of the patients is less than 110 g/L. Among the patients, 1166 cases are in hemodialysis group and 230 cases are in peritoneal dialysis group [2].
Management of anemia in patients on peritoneal dialysis is gradually becoming a hot topic in the field of dialysis. By previous Meta analysis, it is shown that excessive erythropoietin (EPO) will increase mortality in dialysis patients [1,2]. It is suggested that when a patient’s hemoglobin value is below 100 g/L, EPO treatment should be performed, and when the patient’s hemoglobin value is higher than 110 g/L, EPO application should be stopped or the dosage be reduced [3]. Additionally, combined application of the iron and EPO can improve the anemia symptoms in patients of end-stage renal diseases.
In this study, patients received peritoneal dialyses in a teaching hospital, shanghai, China in the past 10 years were reviewed and the symptoms of anemia status and the treatment the patients accepted were analyzed. The causes and existing problems of dialysis were studied according to the result describing the trend and status of anemia in dialysis patients.
Material and methods
Patients’ data
A total of 463 cases of patients receiving peritoneal dialysis from July 2004 to March 2014 in our hospital were analyzed retrospectively. The patients all were elder than 18 years old, those who had been followed up for at least 1 quarter. Meanwhile, their clinical data were completely preserved in the database of our peritoneal dialysis center. Baseline data of the patients including age and gender were compared with the data of Shanghai City Dialysis Registration Center in order to detect whether the study population was good enough to represent those peritoneal dialysis patients in Shanghai. Prior written and informed consent were obtained from every patient and the study was approved by the ethics review board of Huashan Hospital.
Anemia management measures
Anemia management was based upon collection of clinical data of anemia including hemoglobin, serum iron, iron saturation, dosage of EPO and iron supplements each quarter. The data were analyzed so as to understand the general condition in patients receiving treatment for anemia.
Statistical analysis
All the statistical analyses were performed using SPSS version 21.0 (SPSS Inc, Chicago, IL, USA) for Windows and P value less than 0.05 was considered as statistically significant. The baseline was expressed as mean ± standard deviation and frequency (%). The chi square test was used to study the correlation between the subject and the overall subjects so as to identify its representativeness. EPO, oral iron, intravenous iron and HB were described by mean number. The level of hemoglobin erythropoietin, and intake of iron before and after the regular treatment of anemia in PD patients’ comparisons were performed using t test to examine the relation. Pearson correlation was used to test the correlation between different treatment and anemia condition.
Results
Baseline characteristics of the samples
To identify the representativeness of the patients enrolled in this study, baseline analysis was performed. Baseline data of the patients were shown in Table 1. Average age of the patients was 64.3 ± 17.9 years, with 87 cases in the youth group (18-45 years old, accounted for 18.8%), 170 case in the middle-aged group (46-64 years old, accounted for 36.8%) and 206 cases in the elderly group (65 years and over, accounting for 44.4%). There were no differences in age structure between this study and the data of the entire city of Shanghai (P > 0.05). There were 225 cases of females (accounted for 48.6%), with no significant difference with Shanghai city (49%) (P > 0.05). Therefore, the samples of this study had certain representativeness.
Table 1.
Baseline analysis of patients from our center in this study and Shanghai City Peritoneal Dialysis center
| Samples in this study | Samples of Shanghai City Peritoneal Dialysis Center1 | |||
|---|---|---|---|---|
|
|
||||
| N = 463 | N = 2799 | |||
|
|
||||
| Baseline | Cases | % | Cases | % |
| Age, medium (SD) years | 64.3 (17.9) | NA2 | NA2 | |
| Age group, years3 | ||||
| 18-45 | 87 | 18.8 | 521 | 18.6 |
| 46-64 | 170 | 36.8 | 1126 | 40.2 |
| ≥ 65 | 206 | 44.4 | 1152 | 41.2 |
| Gender3 | ||||
| Female | 225 | 48.6 | 1372 | 49.0 |
| Male | 238 | 51.4 | 1427 | 51.0 |
Data of Shanghai City Dialysis Registration Center in 2012;
Not Available;
chi square test, P > 0.05.
Anemia treatment
To understand anemia treatment condition in patients receiving peritoneal dialysis in the past 10 years, the medications were analyzed. According to ‘Clinical practice guidelines for the treatment of anemia in chronic kidney disease, NKF-K/DOQI’, we did some education material to persuade PD patients to visit doctors or nurses regularly in hospital, which helped to enhance the EPO injection compliance of PD patients. So, we decided the end of the education program as the turning point to divide it into two periods, one is “the first 25 quarters” and another is “the posterior 14 quarters”. From the third quarter of 2004 to the third quarter of 2010, hereinafter referred to as the first 25 quarters, the application dose of EPO in patients increased from 2000 IU/w to 7068.49 IU/w, with an average dose of 4673 u/week, meanwhile, intravenous and oral iron supplementation dose increased at different degrees. From the fourth quarter of 2010 to the first quarter of 2014, hereinafter referred to as the posterior 14 quarter, EPO dose maintained between 5917.59 IU/w to 5173.35 IU/w, with an average dose of 5460 u/week, at the same time, intravenous and oral iron supplementation dose decreased (Figures 1, 2 and 3). Together, the result showed that EPO and iron intake increased in the first 25 quarters but increased no longer in the posterior 14 quarter.
Figure 1.
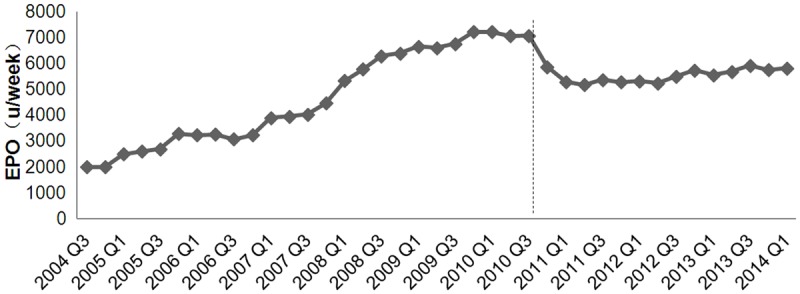
Patients receiving peritoneal dialysis from July 2004 to March 2014 in our hospital were analyzed retrospectively. Their clinical data were completely preserved in the database of our peritoneal dialysis center. EPO application dose was obtained by reviewing the database. The X axis presents the weekly dose of EPO used in each quarter and the Y axis stands for the time. Dotted line represents the third quarter of 2010.
Figure 2.
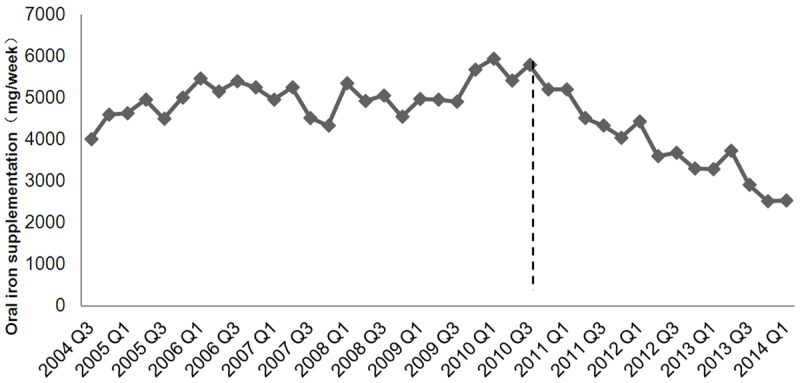
Patients receiving peritoneal dialysis from July 2004 to March 2014 in our hospital were analyzed retrospectively. Their clinical data were completely preserved in the database of our peritoneal dialysis center. Oral iron supplementation dose was obtained by reviewing the database. The X axis presents the weekly dose of oral iron used in each quarter and the Y axis stands for the time. Dotted line represents the third quarter of 2010.
Figure 3.
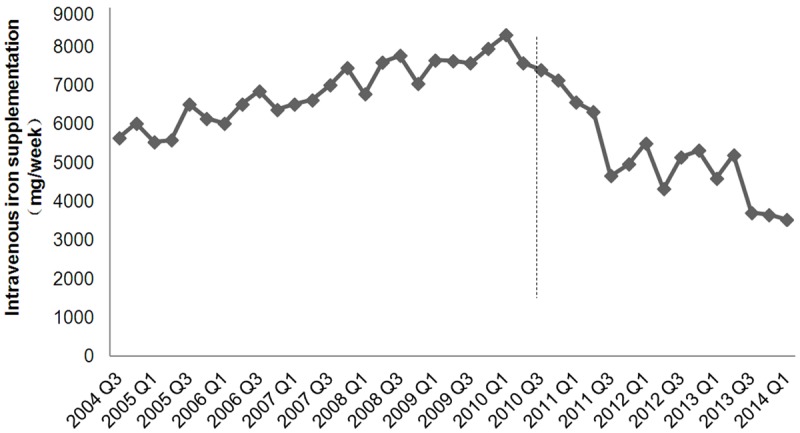
Patients receiving peritoneal dialysis from July 2004 to March 2014 in our hospital were analyzed retrospectively. Their clinical data were completely preserved in the database of our peritoneal dialysis center. Intravenous iron supplementation dose was obtained by reviewing the database. The X axis presents the weekly dose of intravenous iron used in each quarter and the Y axis stands for the time. Dotted line represents the third quarter of 2010.
To identify the curative effects of treatment methods, the compration between treatment and anemia status before and after education program was investigated. As Table 2 showed that intake dose of oral iron dropped from average dose of 5019 mg/week during first period of 25 quarters to 3802 mg/week later. While, Intake dose of oral iron dropped from average dose of 5019 mg/week during first period of 25 quarters to 3802 mg/week later. To sum up, hemoglobin level in peritoneal dialysis patients is closely related to the amount of erythropoietin injection and the amount of supplement iron, meanwhile, erythropoietin injection can obviously improve the symptoms of anemia.
Table 2.
Comparation of EPO, Hemoglobin, Oral Iron, and Intravenous Iron before and after the education program
| EPO | Hemoglobin | Oral Iron | Intravenous Iron | |
|---|---|---|---|---|
| The first period of 25 quarters | 4673 ± 197 | 103.3 ± 12.5 | 5019 ± 325 | 6886 ± 356 |
| The posterior period of 14 quarters | 5460 ± 240 | 107.1 ± 15.2 | 3802 ± 246 | 5048 ± 302 |
| T value | 2.011 | 0.561 | -3.737 | 4.671 |
| P value | 0.035 | 0.455 | 0.011 | P < 0.001 |
Note: EPO, Erythropoietin.
Median hemoglobin value
To figure out anemia in patients with peritoneal dialysis, hemoglobin value was studied. As shown in Figure 4, median hemoglobin value of the first 25 quarters increased from 89.86 g/L to 110.66 g/L, with an average of 103 g/l, and then fluctuated between 104.54 g/L to 109.54 g/L, with an average of 107 g/l. As only 14.6% of the patients used oral iron supplementation and 18.3% of the patients had taken intra venous iron supplementation, further statistics of the corresponding hemoglobin value was performed. The result indicated that the anemia status of peritoneal dialysis patients gradually improved and HB maintained at a good level after 25 quarters.
Figure 4.
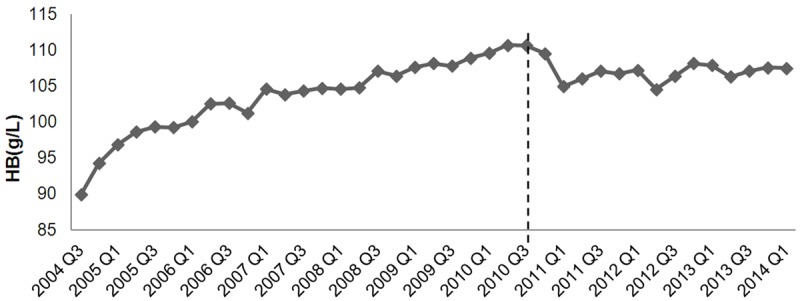
Patients receiving peritoneal dialysis from July 2004 to March 2014 in our hospital were analyzed retrospectively. Their clinical data were completely preserved in the database of our peritoneal dialysis center. HB dose was obtained by reviewing the database. The X axis presents the weekly dose of HB used in each quarter and the Y axis stands for the time. Dotted line represents the third quarter of 2010.
Relationship between treatment and anemia
To identify the curative effects of different treatment methods, the relationship between treatment and anemia was investigated. During the whole follow up time, treatment of the first 25 quarter was different from that of the posterior 14 quarter. The relationship of hemoglobin value, serum iron and iron saturation with treatment methods the patients received were tested by Pearson correlation test according to time, respectively. As shown in Tables 3 and 4, in addition to oral iron supplementation in the posterior 14 quarter had no significant correlation with the three biochemical indexes (P > 0.05), other data showed a good correlation (P < 0.01). To sum up, hemoglobin level in peritoneal dialysis patients is closely related to the amount of erythropoietin injection and the amount of supplement iron, meanwhile, erythropoietin injection can obviously improve the symptoms of anemia.
Table 3.
Relationship between different treatment schemes and patients’ anemia (the first period of 25 quarters)
| Hemoglobin | Serum iron | Iron saturation | ||||
|---|---|---|---|---|---|---|
|
| ||||||
| Paterson correlation | P value | Pearson correlation | P value | Pearson correlation | P value | |
| EPO (the first period of 25 quarters) | 0.731 | 0.000 | - | - | - | - |
| Oral iron (the first period of 25 quarters) | 0.549 | 0.004 | 0.604 | 0.001 | 0.611 | 0.001 |
| Intravenous iron (the first period of 25 quarters) | 0.793 | 0.000 | 0.584 | 0.000 | 0.530 | 0.000 |
Note: EPO, Erythropoietin.
Table 4.
Relationship between different treatment schemes and patients’ anemia (the posterior period of 14 quarters)
| Hemoglobin | Serum iron | Iron saturation | ||||
|---|---|---|---|---|---|---|
|
| ||||||
| Paterson correlation | P value | Pearson correlation | P value | Pearson correlation | P value | |
| EPO (the posterior period of 14 quarters) | 0.782 | 0.000 | - | - | - | - |
| Oral iron (the posterior period of 14 quarters) | -0.308 | 0.284 | -0.452 | 0.105 | -0.377 | 0.184 |
| Intravenous iron (the posterior period of 14 quarters) | 0.082 | 0.003 | 0.270 | 0.004 | 0.743 | 0.000 |
Note: EPO, Erythropoietin.
Discussion
Anemia is a common complication in patients with end-stage renal diseases, and it is also an important factor affecting the quality of life and the prognosis of the patients [2]. Following early indications, although the majority of patients have taken EPO treatment, there are still 23%-77% patients with hemoglobin < 110 g/L [1]. Moreover, a study showed that hemoglobin < 110 g/L is found in 86.01% of the patients and EPO treatment rate is 97.42%, of which, the treatment rate in hemodialysis group and peritoneal dialysis group are 98.32% and 94.78% respectively [2]. In this study, we found that incidence of anemia was 84.7%, which, was close to previous report [2]. A large number of studies have shown that anemia is correlated with high mortality in patients with chronic kidney diseases [4-6]. The reason may be that severe chronic anemia can cause effects on heart function, thereby lead to blood vessel relaxation and dilatation of the heart, and at last, increase cardiac output and induce left ventricular dilatation and hypertrophy. Once hemoglobin is adjusted above 100 g/L, complications such as cardiovascular disease and infection are greatly reduced and the quality of life and survival of patients will be improved at the same time.
Injection of EPO can effectively cut off renal anemia approach, in addition, it also can correct amino acid metabolism and improve oxygen supply of muscle, liver and brain tissues [7]. In this study, it was shown that anemia status was closely related to EPO application dose in patients on peritoneal dialysis (as shown in Tables 3 and 4, the correlation coefficients of the first 25 quarter and posterior 14 quarter were 0.731 and 0.782, P < 0.01). EPO application dose in this study increased gradually in the first 25 quarter with the highest value of 7207.9 IU/w at the fourth quarter of 2009, which was close to the data of other dialysis center. EPO application was not good because of the poor compliance of PD patients [2]. From 2010, and the hemoglobin value fluctuated around 100 g/L, in the meanwhile EPO application dose gradually decreased and fluctuated between 5917.59 IU/w and 5173.35 IU/w. Excessive EPO can increase mortality in dialysis patients [3]. According to British Dialysis Registry Center [8], EPO application dose of peritoneal dialysis patients was 6212 IU/w, which was about 1/3 less than that of hemodialysis patients (9507 IU/w), and this conclusion was consistent to our result (5917.59 IU/w). However, this study has not carried on mortality statistics, and further study is needed to figure out the relation between dose of EPO and the complication, even mortality.
It is unnecessary for peritoneal dialysis patients to go to dialysis center for treatment as often as hemodialysis patients, who mostly visit the hemodialysis center two or three times every week. Many elderly patients only go to dialysis center while they are asked for collecting biochemical index information instead of regularly visit doctors and nurses. Some of patients have learned how to inject EPO themselves at home, hence EPO injection compliance of the patients is lower than of hemodialysis patients [9]. For the patients who are beginning to take peritoneal dialysis, proper EPO injection way and related announcements should be guided. During each follow-up, the patient’s treatment compliance should be learned and corresponding education should be taken. Medical staff should tell the patients the dangers of anemia and the significance of each result so as to improve the therapeutic effect.
For dialysis patients, in addition to EPO application, iron supplement treatment can be taken in order to better cure renal anemia, and it can maintain sufficient body iron reserves and improve erythropoiesis [10]. In this study, except the oral iron supplementation of posterior 14 quarter after 2010, intravenous or oral iron supplementation dose in the past 10 years were closely related to hemoglobin value, serum iron and iron saturation. It is visible that iron supplementation is very important in the use of EPO for correction of renal anemia, and the effect of EPO will be worse when iron deficiency is obvious [11]. According to Singh et al., in the situation of hemoglobin is between 95 g/L and 115 g/L, transferin saturation is less or equal to 25% and serum iron is less or equal to 100 ng/ml, combined use of iron sucrose with EPO has batter effects than single EPO application [(1.3 ± 1.1) g/L vs (0.7 ± 1.1) g/L, P < 0.01]. Meanwhile, overall application dosage of EPO in combined use decreases [12]. In this study, we found with the proper dose of IPO, oral iron dose decreased in the posterior 14 quarter while the laboratory indexes in patients were relatively stable showed the anemia treatment was effective. The main reason might be that health education for patients in Shanghai area had been strengthened, the diet structure had become more reasonable and had made up for oral medicine, namely the total iron intake of the patients had no obvious change. With the good education and especially the dose of stable EPO, even if the amount of iron is reduced, caused little influence of hemoglobin level in peritoneal dialysis patients.
Diet education is an important nursing measure for peritoneal dialysis patients with iron deficiency anemia. Medical workers should explain the significance of high iron diet and introduce iron rich food and the food which can help the absorption of iron to the patients in health education. However, for patients with end-stage renal diseases it is common that they are in high phosphorus and high blood lipid status, or accompanied by diabetes, hypertension and other complications, therefore, diet choice should be based on the specific condition of each patient. Selecting suitable food according to the condition of the patients so as to prevent causing side effects on other diseases is rather important, thus, the dialysis center should be aimed at making individualized diet plan for each patient. So, if nurses educate patients pay more attention to diet, exercise and other noninvasive therapies may improve their quality of life.
In addition, long-term intravenous iron supplementation can sometimes lead to excessive iron reserves and persistent iron excess may cause cardiovascular disease, infection and increased tumor rate. As a result, medical personnel should pay more attention to condition changes in patients with long-term intravenous iron supplements. For patients taking iron sucrose for the first time, allergy test should be applied at first and once dyspnea, tachycardia, erubescence, urticaria and other allergic symptoms appeared, drug application should be stopped immediately and intravenous injection of dexamethasone or epinephrine should be performed.
Compared with other chronic kidney diseases, complicated anemia symptoms of peritoneal dialysis patients are more complex. Because of the lack of large sample size of this population, there is no “gold standard” for the treatment of peritoneal dialysis patients with anemia. As a result, the treatment reference data are from patients who are with chronic kidney diseases but without receiving dialysis treatment or who are undergoing hemodialysis. In addition, compared with patients taking hemodialysis, willingness to dialysis center of peritoneal dialysis patients is much lower. Therefore, it is still a challenging job to study on the exact data of peritoneal dialysis patients and design a nursing plan in the future.
Acknowledgements
This work was supported by Fudan University Nursing Research Foundation (FNF201430) and Shanghai Municipal Commission of Health and Family Planning Research Foundation (201540085).
Disclosure of conflict of interest
None.
References
- 1.Pisoni RL, Bragg-Gresham JL, Young EW, Akizawa T, Asano Y, Locatelli F, Bommer J, Cruz JM, Kerr PG, Mendelssohn DC, Held PJ, Port FK. Anemia management and outcomes from 12 countries in the Dialysis Outcomes and Practice Patterns Study (DOPPS) Am J Kidney Dis. 2004;44:94–111. doi: 10.1053/j.ajkd.2004.03.023. [DOI] [PubMed] [Google Scholar]
- 2.Lin P, Liu Z, Zou J, Jing X, Zhang J, Wang N, He L, Bao X, Xu S, Yan H, Jiang G, Zhang J, Yang H, ZHu K, Zhang W. A multicenter cross-sectional survey of anemia in patients with dialysis: a survey in Shangha. Chinese Journal of Nephrology, Dialysis & Transplantation. 2011;20:332–337. [Google Scholar]
- 3.Locatelli F, Aljama P, Canaud B, Covic A, De Francisco A, Macdougall IC, Wiecek A, Vanholder R Anaemia Working Group of European Renal Best Practice (ERBP) Target haemoglobin to aim for with erythropoiesis-stimulating agents: a position statement by ERBP following publication of the Trial to reduce cardiovascular events with Aranesp therapy (TREAT) study. Nephrol Dial Transplant. 2010;25:2846–50. doi: 10.1093/ndt/gfq336. [DOI] [PubMed] [Google Scholar]
- 4.Locatelli F, Pisoni RL, Combe C, Bommer J, Andreucci VE, Piera L, Greenwood R, Feldman HI, Port FK, Held PJ. Anaemia in haemodialysis patients of five European countries: association with morbidity and mortality in the Dialysis Outcomes and Practice Patterns Study (DOPPS) Nephrol Dial Transplant. 2004;19:121–132. doi: 10.1093/ndt/gfg458. [DOI] [PubMed] [Google Scholar]
- 5.Volkova N, Arab L. Evidence-based systematic literature review of hemoglobin/hematocrit and all-cause mortality in dialysis patients. Am J Kidney Dis. 2006;47:24–36. doi: 10.1053/j.ajkd.2005.09.007. [DOI] [PubMed] [Google Scholar]
- 6.Collins AJ, Li S, PETER WS, Ebben J, Roberts T, Ma JZ, Manning W. Death, hospitalization, and economic associations among incident hemodialysis patients with hematocrit values of 36 to 39% J Am Soc Nephrol. 2001;12:2465–2473. doi: 10.1681/ASN.V12112465. [DOI] [PubMed] [Google Scholar]
- 7.Liu H, Wang L, Zhang J, Guo F, Ran L, Li H. Analysis of nutritional condition of patients undergoing continuous ambulatory peritoneal dialysis and nursing. Chinese Journal of Practical Nursing. 2013;29:13–16. [Google Scholar]
- 8.Gilg J, Webb L, Feest T, Fogarty D. UK Renal Registry 13th Annual Report (December 2010): Chapter 9: haemoglobin, ferritin and erythropoietin amongst UK adult dialysis patients in 2009: national and centre-specific analyses. Nephron Clin Pract. 2011;119(Suppl 2):c149–177. doi: 10.1159/000331759. [DOI] [PubMed] [Google Scholar]
- 9.Del Vecchio L, Cavalli A, Locatelli F. Anemia management in patients on peritoneal dialysis. Contrib Nephrol. 2012;178:89–94. doi: 10.1159/000337818. [DOI] [PubMed] [Google Scholar]
- 10.Peng Y, Kuang P, Huang H. Study on the related nursing and treatment for patients anemia due to kidney disease treated by continously hemodialysis for iron supply. Journal of Nurses Training. 2007;22:435–436. [Google Scholar]
- 11.Wang H, Wang T, Lai X. Nursing of intravenous total dose iron infusion to treat anemia in peritoneal dialysis patients. Chinese Journal of Practical Nursing. 2010;26:21–22. [Google Scholar]
- 12.Singh H, Reed J, Noble S, Cangiano JL, Van Wyck DB United States Iron Sucrose (Venofer) Clinical Trials Group. Effect of intravenous iron sucrose in peritoneal dialysis patients who receive erythropoiesis-stimulating agents for anemia: a randomized, controlled trial. Clin J Am Soc Nephrol. 2006;1:475–482. doi: 10.2215/CJN.01541005. [DOI] [PubMed] [Google Scholar]