

Abstract
AIM: To study the anti-hepatofibrosis mechanism of Bie Jia Jian oral liquid (BOL).
METHODS: The model was induced by subcutaneous injection of CCl4. BOL was administered and the change of serum hyaluronic acid (HA) and laminin (LN) was observed and the degeneration of liver cells and the degree of fibre hyperplasia analyzed. Changes of ultra micro-structure in liver cells were observed in some samples.
RESULTS: HA was reduced in both the groups with low and high dosage of BOL, which showed a remarkable difference as compared with that of the model group (low dosage group: 376.15 μg/L ± 35.48 μg/L vs 806.07 μg/L ± 98.49 μg/L, P < 0.05; high dosage group: 340.14 μg/L ± 30.18 μg/L vs 806.07 μg/L ± 98.49 μg/L, P < 0.05). The LN content of low and high dosage group of BOL was lower than that of model group (low dosage group: 71.99 μg/L ± 8.15 μg/L vs 133.94 μg/L ± 14.45 μg/L, P < 0.01; high dosage group: 71.68 μg/L ± 11.62 μg/L vs 133.94 μg/L ± 14.45 μg/L, P < 0.01) and colchicine group (low dosage group: 71.99 μg/L ± 8.15 μg/L vs 118.28 μg/L ± 16.13 μg/L, P < 0.05; high dosage group: 71.68 μg/L ± 11.62 μg/L vs 118.28 μg/L ± 16.13 μg/L, P < 0.05). Examined by Ridit, BOL could reduce the degeneration and necrosis of liver cells (χ² = 11. 99 P < 0.05), the degree of fibre hyperplasia (χ² = 13.24 P < 0.05) and the pathological change of ultra micro-structure as well.
CONCLUSION: The BOL has certain therapeutic effect on the experiment hepatofibrosis. Its mechanisms might include: protecting the function of liver cells, inhibiting excessive synthesis and secretion of extracelluar matrix from hepatic stellate cells, relieving the capillarization of hepatic sinusoid, improving liver micro-circulation, and regulating immune function.
Keywords: BIEJIA JIAN PILL/administration dosage; BIEJIA JIAN PILL/pharmacology; peroral liquids; liver cirrhosis, experiment al/TCD therapy; laminin/analysis; hyaluronic acid/analysis
INTRODUCTION
Since 1994, our research group has studied on anti-hepatofibrotic effect of the Biejiajian pill and Biejiajian oral liquid (BOL) in rats. It verified that both of them had fair effect on anti-hepatofibrosis[1-3]. Supported by the Natural Scientce Foundation of Zhejiang Province in 1999, we studied the anti-hepatofibrotic mechanism of BOL in rats again. Now we report the results below.
MATERIALS AND METHODS
Materials
Eighty SD rats, weighing (180 ± 20)g, offered by Animal Centre of the Academy of Medical Sciences of Zhejiang Province. Fodder: maize powder (produced by Hangzhou Sijiqing Feed Factory); Lard (commercially supplied); Cholesterol (produced by Chemical Branch of Guangzhou Medicinal Company, batch number: 980503). Ethanol (A.R) (produced by Changyuan Chemical Plant of Changshu City, batch number: 980630). Medicines: All of the 23 ingredients of BOL are purchased from the Out patient Department of Zhejiang College of TCM, such as Biejia, Danpi, etc. appraised by the Department of Pharmacy. Colchicine (produced by Kunming Pharmacy Company, Limited. batch number: 980536). Reagents: CCl4 (A.R) (produced by Fenshui Synthesis Chemical Plant of Yixing City, batch number: 1995122). Liquid paraffin (C.P) (produced by Hangzhou Chemical Reagents Factory, batch number: 971020). HA and LN radioimmunoassay kits (afforded from Shanghai Navy Institute of Medical Science); main instruments: SN-688γ -counter (Shanghai Atomic Energy Institute); UV-754 ultraviolet-visible spectrophotometer (Shanghai 3rd Analytic Instrument Factory); MR4100 enzyme marker (American Dynatach Company); H-500 transmission electricmicroscope (Japanese Hitachi, Co).
METHODS
Animal model
All groups but the normal group received sc CCl4 (A.R) 5 mL•kg¯¹ in the first day of experiment, afterwards sc 400 mL•L¯¹CCl4-liquid paraffin mixture 3 mL•kg¯¹ every 3 d; the normal group sc equal amount of 9 g•L¯¹ NaCl (NS), lasted 6 wk. Except the normal group, every group was fed with mixed fodder (maize powder with 5 g•L¯¹ cholesterol and 200 g•L¯¹ lard) and drank 200 g•L¯¹ ethanol only. The normal group was fed with general fodder and water. The time required to complete the induction of model is 6 wk.
Grouping
Thirty-seven established rat models were grouped into II-V groups randomly i.e. group II model control (n = 10), group IIIcolchicine (n = 9), group IV low dosage of BOL (n = 9) and group V high dosage of BOL (n = 9). Another 11 normal rats served as normal control in group I.
Therapy
The BOL afforded by Zhejiang College of TCM, according to the ingredient of Jingui Biejiajian pill, which is recorded in an ancient medical book of TCM (Jinkui Yaolue). It contains crude Chinese medicine 0.92 g per millilitre (that is 20 times the dosage used in adults). I, II group ig NS 10 mL/kg, III group ig 0.001% colchicine in distilled water of the dosage of 0.1 mg•kg¯¹, IV group ig BOL 4.6 g•kg¯¹ and V group ig BOL 9.2 g•kg¯¹. All groups had been treated once a day for 5 wk and took water and fodder ad lib. For maintaining pathological attack, 400 mL•L¯¹ CCl4-liquid paraffin mixture 3 mL•kg¯¹ once a week until the end of treatment was injected subcutaneously to the models of II-V groups. After the treatment, venous blood was collected from retrobulbar vein, serum was separated and preserved under -70 °C for test. HA and LN were examined by radioimmunoassay. The left liver lobe was dessected and fixated by 100 mL•L¯¹ formalin and embedded in paraffin, serially sectionalized and then stained with HE observed under optical microscope. In case of observing the collagenous fiber hyperplasia Masson staining was employed. The standards for interpreting the degree of hyperplasia under microscope are in accordance to the criteria of the 5th National Academic Conference of Infection and parasitosis[4], and the degree of degeneration refers to the standard of reference [5].
Statistical analysis
Data described as mean ± SD and analysed by F test, and q test was used to compare the data between 2 groups of multiple groups. The semiquantitative data was analysed by Ridit test. P < 0.05 regarded as significant.
RESULTS
During the period of treatment, in gruop II 2 rats died, 1 rat each died in group I, IV and V, and in group III no rat died.
Influence of BOL on serum HA and LN
Compared with model group, the serum HA of each treated group was lowered significantly (P < 0.05). There was no significant difference between each treated group (P > 0.05). This is in accordance with the results of other article[6]. Results of the serum LN: the difference between the colchicine group and the model group was not significant (P > 0.05). Compared with the normal group, the LN of each treated group was raised significantly (P < 0.01). The LN in both low-and high-dose BOL groups were higher significantly than that of normal group (P < 0.01) and colchicine group (P < 0.05, Table 1). The difference between high-and low-dose BOL groups was not significant.
Table 1.
Serum HA and LN in BOL treated SD rats (mean ± SD, μg•L¯¹)
| Groups | n | HA | LN |
| Normal | 10 | 197.77 ± 26.02 | 42.78 ± 10.05 |
| Model | 8 | 806.07 ± 98.49b | 133.94 ± 14.45b |
| Colchicine | 9 | 402.53 ± 50.78a | 118.28 ± 16.13b |
| Low-dose BOL | 8 | 376.15 ± 35.48a | 71.99 ± 8.15bdc |
| High-dose BOL | 8 | 340.14 ± 30.18a | 71.68 ± 11.62bdc |
P < 0.01 vs normal group;
P < 0.05 vs model group,
P < 0.01 vs model group;
P < 0.05 vs colchicine.
Influence of BOL on liver hyperplasia and degeneration
Being analysed by Ridit (χ² = 13.24, P < 0.05, Table 2), we found that the treatment was relevant with the extent of liver hyperplasia. According to the average Ridit, the high-dose BOL group did the best in improving liver hyperplasia.
Table 2.
Extent of liver hyperplasia in each treated group
| Groups | n |
Degree of liver fibrosis |
Average of Ridit | ||||
| - | + | ++ | +++ | ++++ | |||
| Model | 8 | 0 | 0 | 1 | 4 | 3 | 0.7247 |
| Colchicine | 9 | 0 | 1 | 2 | 4 | 2 | 0.5894 |
| Low-dose BOL | 8 | 0 | 2 | 1 | 4 | 1 | 0.5176 |
| High-dose BOL | 8 | 0 | 5 | 2 | 1 | 0 | 0.2364 |
χ² = 13.24, χ² (4) = 9.49.
According to the results of statistical analysis (χ² = 11.99, P < 0.05, Table 3), we considered that the extent of liver cell degeneration was related to the treatment. Referring to the average Ridit, the effectiveness of improving the degeneration in high dosed BOL group was best, and model group had the worst result.
Table 3.
Liver cell degeneration in each treated group
| Groups | n |
Extent of hyperplasia |
Average of Ridit | ||||
| - | + | ++ | +++ | ++++ | |||
| Model | 8 | 0 | 0 | 2 | 3 | 3 | 0.7408 |
| Colchicine | 9 | 0 | 1 | 4 | 3 | 1 | 0.5584 |
| Low-dose BOL | 8 | 0 | 1 | 2 | 4 | 1 | 0.5599 |
| High-dose BOL | 8 | 0 | 4 | 3 | 1 | 0 | 0.2576 |
χ² = 11.99, χ² (4) = 9.49.
Electron microscopy
The nucleuses in liver cell of normal SD rats were circular or elliptic and located in the center of cell, the mitochondria were circular or elliptic, the ridges were clear, the Ito cell could be found in Disse’s spaces, its cytoplasm contained plenty of fat droplets. How eic, the nucleoluses disappeared, rough endoplasmic reticulums expanded obviously, the mitochondria were tumid, the ridges were broken or lacked, there were a gr eat deal of fat droplets in the cytoplasm. Many collagenous fibers accumulated in Disse’s spaces. The number of stellate cells and rough endoplasmic reticulum increased and surrounded by a large number of collagenous fibers. Compared with the model group, the fat droplets in liver cell of the high-dose BOL group decreased, the structure of nucleus was clear and the mitochondria were tumid lightly. Being observed under the electronic microscope the results of low dosed BOL group were similar to those of colchicine group. Their damage as lighter and more serious than that in model group and high-dose BOL group respectively (Figure 1, Figure 2, Figure 3, Figure 4, Figure 5).
Figure 1.
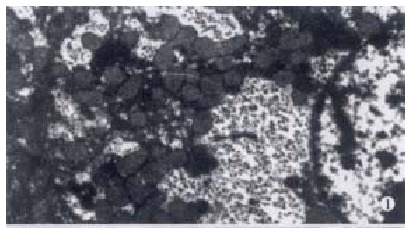
Normal group Showing clear liver cell structure with plenty of mitochondria and clear ridges, no fat droplets in cytoplasm. EM × 6000
Figure 2.
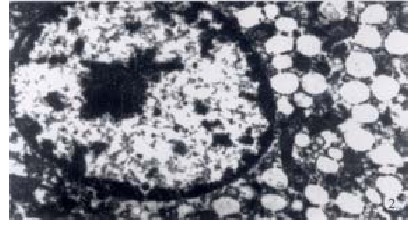
Model group Showing few mitochondria without nucleolus, cell structure is not clear, a lot of fat droplets in cytoplasm. EM × 4000
Figure 3.
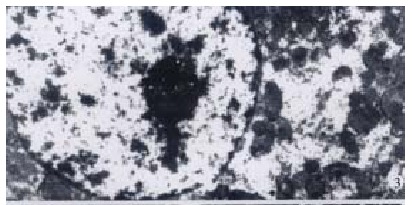
High dosed BOL group Showing clear nucleus structure, lightly tumid mitochondria and few fat droplets in cytoplasm. EM × 4000
Figure 4.
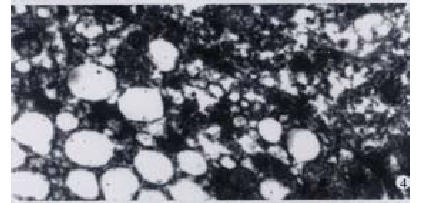
Model group Showing many deposited fibers. EM × 8000
Figure 5.
High dosed BOL group Showing few deposited fibers. EM × 5000
DISCUSSION
Recently, studies on the prevention and treatment of liver fibrosis are very popular in China. Besides western medicine[7-11], single Chinese drug and its effective ingredients[12-19], anti- hepatofibrotic effect of Chinese complex formula[20-27] are also the main project in researches. These studies illustrate the mechanism and clinical effectiviness[28-32] in anti-hepatofibrosis from different point of view. Now, we will especially discuss the anti-hepatofibrotic mechanism of BOL.
The knowledge of liver fibrosis in TCM
Though the term, liver fibrosis, is not mentioned in the ancient medical documents of TCM, the corresponding clinical symptoms of this disease in TCM terms such as abdominal mass, costal pain, flatulence, jaundice, blood stasis, etc. are commonly noted. The clinical symptom of liver fibrosis is intricate. According to the theory of TCM, its basic pathogenesis is that: the condition is manifested as body resistance weakened while pathogenic factors prevailed, damp-heat and blood stasis coexisted, liver depressed and deficiency of qi and blood in spleen and kidney. Liver depression and qi stagnation can result in blood stasis, blood fails to nourish liver, and the key pathogenetic mechanism is blood stasis[33]. At the beginning, the pathogenetic mechanism is qi stagnation and blood stasis. If being treated unproperly, the disease will evolve into blood stasis mainly, then into a condition which manifests as blood stasis, body resistance weakened and excess in superficiality. The therapy is promoting the circulation and relieving the stasis, s trengthening the body resistance to eliminate pathogenic factors, resolving and softening hard mass.
BOL is an improved preparation from Biejiajian Pill which is recorded in an ancient medical book (Jinkui Yaolue). Its ingredients include twenty-three herbs, such as biejia, taoren, danpi, shaoyao, dahuang, caihu, guizhi, banxia, houpu, renshen, e-jiao, huangqin etc. The combination of ingredients has the effect on promoting circulation and relieving stasis, strengthening body resistance and eliminating pathogenic factors simultaneously, resolving and softening the hard mass, which is conformable with the principle of treating liver fibrosis. The therapy of promoting blood circulation and cleminishing stasis has been adopted in clinic[34].
Inquiring into the anti-hepatofibrotic mechanism of BOL
At present, the mechanism of liver fibrosis is inferred that the pathogenic factors injure the liver cell and activate Kupffer’s cells to secrete certain kinds of cytokines, which act jointly with other cytokines secreted by the platelets, hepatic sinusoid endotheliocytes, hepatocytes and some chemical intermediates to activate stellate cells, converting them into myofibroblasts, secreting a great deal of extracellular matrix (ECM). The increase of secretion and decrease of degradation result in accumulation of ECM in liver, forming liver fibrosis gradually[35-39]. According to this experimental result, we suggest the main effect of BOL on treating liver fibrosis in four aspects as follows. ①Preventing the hepatocyte from degeneration and necrosis. The degeneration and necrosis of liver cell are the factors inducing excessive deposition of ECM, which takes an important role in the progression of liver fibrosis[40,41]. So, preventing the degeneration and necrosis of liver cell after being hurt can eliminate the promoting factor of liver fibrosis, preventing Kupffer’s cells and stellate cells from being activated, inhibiting the progression of liver fibrosis. This experimental result shows that BOL can protect the liver cells from being harmed, reduce their degeneration and necrosis, clean or partly clean the inflammatory reaction (also a promoting factor of liver fibrosis), all these demonstrate the good effect on treating liver fibrosis. ② Inhibiting the liver stellate cells to synthesize and secrete ECM. It is well known that liver stellate cells are the interstitial cells served as the main source of ECM. As the liver cells are injured, they will be activated, and increased, and then convert into the transitive type and myofibroblast which synthesize and secrete the ECM excessivly[40,42-44]. The collagens are the main elements of ECM. They are formed in rough endoplasmic reticulums of fibroblasts and are secreted as collagenous fibrils[45]. Both the number of stellate cells and rough endoplasmic reticulums of high dosed BOL group are less than those of model group, which indicates that inhibiting the activation and hyperplasia of the liver stellate cells maybe one of the effects of BOL to prevent and treat liver fibrosis. ③Relieving the capillarization of hepatic sinusoid, improving the microcirculation of liver. The fenestrate on the hepatic sinusoid endotheliocyte is the site for exchanging materials between the liver cells and plasma. When liver fibrosis developed, ECM synthesized profoundly, deposited in Disse’s spaces, forming the membranous spiral lamina under the hepatic sinusoid endothelium, fenestrate of hepatic sinusoid decreased or vanished and then forming capillarization, resulting in impairment of microcirculation, subsequently, affecting the exchange of the oxygen and substance of the liver cell seriously, thus bringing out or aggravating the damage of liver cell[45-48]. LN is the main glycoprotein of the membranous spiral lamina and distributes together with the IV type collagen in the liver. So its serum content is considered as a renewal index of membranous spiral lamina[49-51]. This experimental result indicated that: BOL can decrease the LN content in liver fibrosis, thus relieving the capillarization of hepatic sinusoid, improve the microcirculation of liver, reducing the damage of liver cell and accelerating the repairment of liver. This may be an important effect of BOL on promo ting the circulation and transforming stasis. ④ Regulating the immune function, reducing the immuno-damage of liver cell. Some researchers[52] complain that the liver cirrhosis is the result of the immune function disturbance. According to our previous report[2], we suggest that BOL can adjust humoral immunity, reduce the immuno-damage of liver cell, improve the substance metabolism and protect the liver tissue from being injured.
Footnotes
Edited by You DY
Supported by the Natural Science Foundation of Zhejiang Province, No.398402.
References
- 1.Yao ZM, Lu GY, Zhao ZY. Experimental study on anti-hepatofibrosis effect of Biejiajian Pill. Zhejiang Zhongyi Xueyuan Xuebao. 1997;21:45–46. [Google Scholar]
- 2.Yao ZM, Xiong YK, Li JP. Experimental study on anti-hepatofibrosis effect of Biejiajian Oral Liquid (BOL) Zhejiang Zhongyi Xueyuan Xuebao. 2000;24:58–61. [Google Scholar]
- 3.Zhao ZY, Yao ZM, Zhong QP, Zhu FY, Wu CZ, Lu GY, Wang GY. Clinical study on Chinese herb Biejiajian pill for treating hepatic fibrosis. Zhongxiyi Jiehe Ganbing Zazhi. 2001;11:136–138. [Google Scholar]
- 4.The scheme of preventing and treating the viral hepatitis (try out) (Revised by the 5th national academic conference of infection & parasitosis in Beijing, May of 1995) Zhonghua Neike Zazhi. 1995;34:788. [Google Scholar]
- 5.Chen ML, Liu SD. The basic research and clinical treatment of hepatofibrosis. In: 1st edition, Beijing: Renmin Weisheng Chubanshe; 1996. p. 229. [Google Scholar]
- 6.He QL, Xie CL, Gan DC, Gu SL, Lai SP, Chen Y. Research on the correlativity between TGF-β and HA in human liver fibrosis. Shijie Huaren Xiaohua Zazhi. 2000;8(Suppl 8):80. [Google Scholar]
- 7.Lin WL, Zhou HG. Treatment of liver fibrosis. Huaren Xiaohua Zazhi. 1998;6(Suppl 7):106–107. [Google Scholar]
- 8.Cai WM, Weng HL. Animal experiment and clinical study on anti-hepatofibrosis of IFN-γ. Shijie Huaren Xiaohua Zazhi. 2000;8(Suppl 8):13. [Google Scholar]
- 9.Weng HL, Cai WM, Liu RH. Animal experiment and clinical study of effect of gamma-interferon on hepatic fibrosis. World J Gastroenterol. 2001;7:42–48. doi: 10.3748/wjg.v7.i1.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Liu YL, Li DG, Lu HM, Jiang ZM, Xu QF. The subcellular study of calcium antagonists in treatment of hepatofibrosis. Xin Xiaohuabingxue Zazhi. 1996;4:3–5. [Google Scholar]
- 11.Jiang XL, Quan QZ, Shun ZQ, Wang YJ. Progress on calcium antagonists treating hepatofibrosis. Xin Xiaohuabingxue Zazhi. 1995;3:161–162. [Google Scholar]
- 12.Shen LY, Li DG, Lu HM. A review of Chinese medicinal herbs for treatment of liver fibrosis. Xin Xiaohuabingxue Zazhi. 1997;5:121–122. [Google Scholar]
- 13.Wang YJ, Sun ZQ, Quan QZ, Zhang ZJ. Controlled study of Cordyceps sine nsis and colchicine on the antifibrosis effect of liver. Xin Xiaohuabingxue Zazhi. 1994;2:208–209. [Google Scholar]
- 14.Zheng G, Hao J, Jia GR, Zhong HM. Effects of algin in prevention of liver fibrosis in mice. Xin Xiaohuabingxue Zazhi. 1997;5:353–354. [Google Scholar]
- 15.Li DG, Lu HM, Chen YW. Progress in studies of tetrandrine against hepatofibrosis. World J Gastroenterol. 1998;4:377–379. doi: 10.3748/wjg.v4.i5.377. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Sun ZQ, Wang YJ, Quan QZ, Liu XF, Pan X, Jiang XL. Prevention and trea tment action of tetrandrine on experimental liver fibrosis in rats. Xin Xiaohuabingxue Zazhi. 1994;2:19–20. [Google Scholar]
- 17.Wang YJ, Sun ZQ, Quan QZ, Zhang ZJ, Liu XF, Jiang XL, Pan X. Study on type IV collagen and fat-storing cells in fibrotic rat liver treated by tetrand rine. Xin Xiaohuabingxue Zazhi. 1994;2:78–79. [Google Scholar]
- 18.Ma X, Qiu DK, Xu J, Zeng MD. Effects of Cordyceps polysaccharides in patients with chronic hepatitis C. Huaren Xiaohua Zazhi. 1998;6:582–584. [Google Scholar]
- 19.Xu LM, Liu C, Liu P. Effect of amygdalin of proliferation of rat hepat ic fat-storing cells and collagen production in vitro. Xin Xiaohuabingxue Zazhi. 1997;5:84–85. doi: 10.3748/wjg.v3.i2.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Hu YY, Liu C, Liu P, Gu HT, Ji G, Wang XL. Anti-fibrosis and anti-pe roxidation of lipid effects of Fuzhenghuayu decoction on rat liver induced by CC l4. Xin Xiaohuabingxue Zazhi. 1997;5:485–486. [Google Scholar]
- 21.Du LJ, Tang WX, Dan ZL, Zhang WY, Li SB. Protective effect of Ganyanyp ing on CCl4 induced liver fibrosis in rats. Huaren Xiaohua Zazhi. 1998;6:21–22. [Google Scholar]
- 22.Li BS, Wang J, Zhen YJ, Wang XG, Sun YH, Wang SQ, Wu ZQ. Blocking effe ct of Chinese herbs Yiganxian and PHGF on immuno-damaged hepatic fibrosis in rats. Huaren Xiaohua Zazhi. 1998;6:786–788. [Google Scholar]
- 23.Shen BS, Wong XG, Qiao HC, Lu ZH, Han Q, Wang W, Guan HL. Preventive effect of Sanjia Yigan granule in hepatofibrosis in rats. Huaren Xiaohua Zazhi. 1998;6:386–388. [Google Scholar]
- 24.Wang QC, Shen DL, Zhang CD, Xu LZ, Nie QH, Xie YM, Zhou YX. Effect of Rangansuopiwan in expression of tissue inhibitor of metalloproteinase-1/2 in rat liver fibrosis. Shijie Huaren Xiaohua Zazhi. 2001;9:379–382. [Google Scholar]
- 25.Liu C, Liu P, Liu CH, Zhu XQ, Ji G. Effects of Fuzhenghuayu decoction on collagen synthesis of cultured hepatic stellate cells, hepatocytes and fibroblasts in rats. World J Gastroenterol. 1998;4:548–549. doi: 10.3748/wjg.v4.i6.548. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Wang Z, Zhang ZY, Ruan JG, Si C. Clinical and experimental research on Keganlin treating chronic liver diseases and hepatofibrosis. Shijie Huaren Xiaohua Zazhi. 2000;8(Suppl 8):28. [Google Scholar]
- 27.Wang XL, Li ZZ, Li JM, Wang TG. Therapeutic influence of Xuelong Chong ji on blood test, liver function test, liver fibrosis and virus immunology indic ator of chronic hepatitis and liver cirrhosis. Shijie Huaren Xiaohua Zazhi. 2000;8(Suppl 8):55. [Google Scholar]
- 28.Liu P, Liu C, Xu LM, Hu YY, Xue HM, Liu CH, Zhang ZQ. Effects of Fuzheng Huayu 319 recipe on liver fibrosis in chronic hepatitis B. World J Gastroenterol. 1998;4:348–353. doi: 10.3748/wjg.v4.i4.348. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Cheng ML, Wu YY, Huang KF, Luo TY, Ding YS, Lu YY, Liu RC, Wu J. Clinical study on the treatment of liver fibrosis due to hepatitis B by IFN-alpha (1) and traditional medicine preparation. World J Gastroenterol. 1999;5:267–269. doi: 10.3748/wjg.v5.i3.267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Wu JG, Li FJ. Effects of kanggianfang and the relationship between ser um hyaluronic acid and TCM bianzheng in patients with cirrhosis. Xin Xiaohuabingxue Zazhi. 1995;3(Suppl 4):19. [Google Scholar]
- 31.Wu JG, Li XY. Clinical studies of Kangxianfang in treating liver cirrhosis. Xin Xiaohuabingxue Zazhi. 1997;5:303–304. [Google Scholar]
- 32.Jiao WJ, Zhang F, Dai W, Li MR, Wang XY. Clinical effect of Huangqi co mplex decoction on treating hepatofibrosis. Huaren Xiaohua Zazhi. 1998;6(Suppl 7):354. [Google Scholar]
- 33.Gu HT, Hu YY, Xu LM, Liu P, Liu C. The histological observation of the effect of supporting the condition and transforming stasis formula on preven ting experimental hepatofibrosis. Zhongxiyi Jiehe Ganbing Zazhi. 1997;7:224. [Google Scholar]
- 34.Shun YF, Yao XX, Jiang SL. Traditional Chinese Drug therapy for hepato fibrosis. Shijie Huaren Xiaohua Zazhi. 2000;8:686–687. [Google Scholar]
- 35.Friedman SL. Seminars in medicine of the Beth Israel Hospital, Boston. The cellular basis of hepatic fibrosis. Mechanisms and treatment strategies. N Engl J Med. 1993;328:1828–1835. doi: 10.1056/NEJM199306243282508. [DOI] [PubMed] [Google Scholar]
- 36.Wang YJ, Sun ZQ, Quan QZ, Yu JJ. Fat-storing cells and liver fibrosis. China Natl J New Gastroenterol. 1996;2:58–60. [Google Scholar]
- 37.Yan JP, Liu JC, Ma XH, Jia JB, Zhao YC, Xu RL, Li CM, Han DW. Immunoh istochemical study on basic fibroblast growth factor in experimental liver fibro sis. Xin Xiaohuabingxue Zazhi. 1997;5:642–644. [Google Scholar]
- 38.Bai WY, Yao XX, Feng LY. Current situation in studies of liver fibrosi s. Shijie Huaren Xiaohua Zazhi. 2000;8:1267–1268. [Google Scholar]
- 39.Jiang HQ, Zhang XL. Pathogenesis of hepatofibrosis. Shijie Huaren Xiaohua Zazhi. 2000;8:687–689. [Google Scholar]
- 40.Liu SR, Gu HD, Li DG, Lu HM. A comparative study of fat storing cells and hepatocytes in collagen synthesis and collagen gene expression. Xin Xiaohuabingxue Zazhi. 1997;5:761–762. [Google Scholar]
- 41.Yan JC, Chen WB, Ma Y, Xu CJ. Immunohistochemical study on hepatic vascular forming factors in liver fibrosis incuced by CCl4 in rats. Shijie Huaren Xiaohua Zazhi. 2000;8:1238–1241. [Google Scholar]
- 42.Huang ZG, Zhai WR, Zhang YE, Zhang XR. Study of heteroserum-induced rat liver fibrosis model and its mechanism. World J Gastroenterol. 1998;4:206–209. doi: 10.3748/wjg.v4.i3.206. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Wang YD, Jia LW, Li CM. Hepatic content of collagens and laminin in rat model of experimental liver fibrosis. World J Gastroenterol. 2000;6(Suppl 3):73. [Google Scholar]
- 44.Wang BE. Synthesis and degradation of extracelluar matrix of hepatofib rosis. Zhonghua Ganbing Zazhi. 1997;5:65. [Google Scholar]
- 45.Han JH, Han ZY. Is the liver cirrhosis irreversible. Zhongxiyi Jiehe Ganbing Zazhi. 1999;9:1. [Google Scholar]
- 46.Lu X, Xu GF, Chen WH, Liu CH, Liu P. Dynamic change of hepatic sinuso id capillarization in hepatofibrosis of rats. Shijie Huaren Xiaohua Zazhi. 2000;8:1415–1416. [Google Scholar]
- 47.Wang YJ, Sun ZQ. Advancement of hepatofibrosis on cytology and molecul ar biology. Xin Xiaohuabingxue Zazhi. 1994;2:244–246. [Google Scholar]
- 48.Yao D, Li DG. Advancement of hepatofibrosis mechanism. Xin Xiaohuabingxue Zazhi. 1995;3(Suppl 4):59. [Google Scholar]
- 49.Kong XT. The diagnosis indicator and evaluation of hepatofibrosis: the evaluation of serum diagnosis indicator of hepatofibrosis. Zhonghua Ganbing Zazhi. 1998;6:244. [Google Scholar]
- 50.Lu X, Liu CH, Xu GF, Chen WH, Liu P. Successive observation of lamin in and collagen on hepatic sinusoid during the formation of the liver fibrosis in rats. Shijie Huaren Xiaohua Zazhi. 2001;9:260–262. [Google Scholar]
- 51.Gong AY, Ma XH, Xu RL, Yin L, Chen XM, Zhao YC, Han DW. Changes of laminin in the liver of rats with experimental cirrhosis. Xin Xiaohuabingxue Zazhi. 1997;5:3–5. [Google Scholar]
- 52.Miskulin M, Dalgleish R, Kluve-Beckerman B, Rennard SI, Tolstoshev P, Brantly M, Crystal RG. Human type III collagen gene expression is coordinately modulated with the type I collagen genes during fibroblast growth. Biochemistry. 1986;25:1408–1413. doi: 10.1021/bi00354a033. [DOI] [PubMed] [Google Scholar]