

Abstract
The main aim of this study was to evaluate the perceived level of difficulty and fear of movement among patients with chronic low back pain (CLBP) compared with asymptomatic subjects when they visualized motor control therapeutic exercises (MCTEs) commonly used in physiotherapy. Our secondary objective was to analyse the correlation between fear of MCTEs and other psychological and disability variables. Thirty patients with CLBP comprised the treatment group, and 30 asymptomatic subjects comprised the control group. The procedure consisted of showing photographs and videos of seven MCTEs and having the participants rate their perceived difficulty and fear. Participants then answered a series of psychological self-report measures. Differences were found between groups in perceived difficulty of the MCTEs shown in videos (F=21.06, P<0.001) and photographs (F=15.86, P<0.001), as well as for perceived fear (F=9.71, P<0.001; F=8.61, P<0.001, respectively). Regression analysis indicated that in the CLBP group the predictor variable for perceived difficulty and fear was the lumbar disability (explaining 44% and 28% of the variance, respectively), however in the control group the predictor variables were catastrophizing and self-efficacy (38% and 34% of the variance, respectively). In conclusion, patients with CLBP experience greater perceived level of difficulty and fear of movement when visualizing MCTEs than asymptomatic subjects. Psychological factors and disability were correlated with perceived difficulty and fear when videos and photographs of exercises were shown.
Keywords: Recurrent low back pain, Fear-avoidance beliefs, Self-efficacy, Exercise
INTRODUCTION
Chronic low back pain (CLBP) has a great impact on Western society, through either absenteeism or disability in daily life, especially in developed countries (Loney and Stratford, 1999). According to de la Cruz-Sánchez et al. (2012), 24% of the Spanish population has suffered some kind of back pain during the last year, and CLBP is more frequent in women (30.2%–17.5%). The pain is considered as a chronic condition when it persists for at least 12 weeks (Airaksinen et al., 2006). Most of the patients that suffer an acute episode of low back pain recover relatively quickly, but a small percentage of those patients become chronic (George et al., 2004).
Chronic back pain is related to a low or moderate physical activity intensity pattern, and it produces a significant functional disability (Thomas et al., 2010). In the Fear-Avoidance Model of Pain described by Vlaeyen et al. (1995), CLBP could lead to catastrophizing, fear of movement (kinesiophobia), and avoidance belief attitudes, which together could perpetuate pain. Psychosocial, physical, and behavioural components play important roles in the chronicity of low back pain (Thomas et al., 2010; Vlaeyen et al., 1995). The main goals of clinical research are focused on pain treatment, functional recovery, and minimization of avoidance behaviours (Barzilay et al., 2015; Lawford et al., 2015; Wälti et al., 2015). Specific muscle training is one of the key options for management of low back pain (Yue et al., 2014). However, current treatment could be improved by adding an appropriate approach based on psychosocial factors in order to focus on reducing pain, improving function, and minimizing avoidance behaviours (Thomas et al., 2010).
The clinical interaction between physical function and psychosocial characteristics is one of the areas of interest in recent literature (Karayannis et al., 2013). The potential therapeutic role of this interaction in the management of persisting pain and the functional impact of chronicity must be addressed properly. This interaction between the physical function and psychological part has been demonstrated in research showing that kinesiophobia is associated with rigidity of the trunk (Karayannis et al., 2013).
According to Leeuw et al. (2007), kinesiophobia contributes to the development and maintenance of CLBP. It has been postulated that fear of movement could lead to subsequent avoidance of physical activity and contributes to the development of chronic pain syndrome (Barke et al., 2012). There is some evidence that exercise programs can lead to a reduction in the level of kinesiophobia in such patients (Klaber Moffett et al., 2004). Kinesiophobia has the broadest relationship with the mechanical properties of the spine, such as muscle activation and movement patterns of the trunk. However, other factors, such as catastrophism, depression, or fear-avoidance factors, are also related to the mechanical properties of the spine (Karayannis et al., 2013). Due to this interaction, it is suggested that the evaluation of kinesiophobia during treatment planning could lead to a more appropriate therapeutic approach.
In addition, previous studies have investigated the perception of harm or fear to movement when showing patients photographs of activities of daily living or after performing a specific lumbar region test (Demoulin et al., 2013; George et al., 2009; Houben et al., 2005; Trost et al., 2009). However, to our knowledge, there are no studies evaluating the perception of difficulty and fear from motor control therapeutic exercises (MCTEs).
For all this, the main objective is to evaluate the perceived level of difficulty and fear of movement by patients with CLBP compared with asymptomatic subjects when visualizing MCTEs commonly used in physiotherapy. The secondary objective is to analyse the correlation between fear of MCTEs with kinesiophobia, catastrophizing, and self-efficacy.
MATERIALS AND METHODS
Study design
This research was a cross-sectional design with a nonprobabilistic sample. The sample was composed of two groups, the first group comprised patients with CLBP and the second group consisted of asymptomatic subjects as a control group (CG). All of the procedures used in this study were planned under the ethical norms of the Helsinki Declaration and were approved by the Local Ethics Committee of the Center for Advanced Studies of University La Salle, Madrid, Spain. This study follows the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) statement (von Elm et al., 2008). After receiving detailed information about the study, the volunteers provided written informed consent.
Recruitment of participants
A consecutive nonprobabilistic convenience sample of 30 patients with CLBP and 30 healthy subjects for the CG were recruited between February 2014 and June 2014. The sample was recruited from outpatients of a primary health care centre in Madrid, Spain. Patients in the CLBP group were selected if they met all of the following inclusion criteria: (a) low back pain in at least the prior six months; (b) low back pain of nonspecific nature; and (c) men and women aged 18 to 65 yr old. And as exclusion criteria: (a) the presence of neurological signs (such as weakness perceived in the lower limbs); (b) specific spinal pathology (e.g., malignancy, inflammatory joint or bone diseases); (c) having undergone back surgery.
The CG was recruited from our university campus and the local community through flyers, posters, and social media. Healthy participants were examined and included in the study if they met the following criteria: (a) subjects who have not had low back pain in the last 6 months; (b) men and women aged 18 to 65 yr old.
These general exclusion criteria are common to both groups: (a) any cognitive disability that hinders viewing of the audio-visual material; (b) illiteracy; (c) understanding or communication difficulties; and (d) insufficient Spanish language comprehension to follow measurement instructions.
Outcomes
Fear and difficulty
As primary outcomes the perceived fear and difficulty were measured with the Visual Analogue Scale (VAS) as: Fear VAS (FVAS); difficulty VAS (DVAS). The VAS consists of a 100-mm line, the left side of which represents “no fear” or “no difficulty”, whereas the right side represents “maximal fear” or “maximal difficulty”. The participants placed a mark where they felt represented their perception of fear or difficulty. The perceived fear and difficulty for each photography and video of the MCTEs were quantified in mm. The total sum of mm was calculated separately for pictures and for videos for each variable.
Disability and function
The Roland Morris Disability Questionnaire (RMDQ) was used to assess the physical disability in activities of daily living due to low back pain. This self-administered questionnaire consists of 24 items that refer to the limitations of daily activities as a result of low back pain (Roland and Morris, 1983). The total score ranges from 0 to 24 (higher scores indicate a more severe disability level). The Spanish version of RMDQ has been demonstrated as having acceptable psychometric properties (Kovacs et al., 2002).
Pain catastrophizing
The Spanish version of the Pain Catastrophizing Scale (PCS) assesses the degree of pain catastrophizing (García Campayo et al., 2008; Sullivan et al., 1995). The PCS has 13 items and a three-factor structure: rumination, magnification, and helplessness. Each item is rated on a 5-point scale from 0 (not at all) to 4 (all the time). The theoretical range is between 0 and 52, with lower scores indicating less catastrophizing. The PCS has been demonstrated as having acceptable psychometric properties (García Campayo et al., 2008).
Pain-related fear
The Spanish version of the Tampa Scale for Kinesiophobia (TSK-11) is a self-reported questionnaire that assesses fear of reinjury due to movement (Gómez-Pérez et al., 2011). The TSK-11 is an 11-item questionnaire that eliminates psychometrically poor items from the original version of the TSK (Kori et al., 1990) to create a shorter questionnaire with comparable internal consistency. Total TSK-11 scores range from 11 to 44 points, and each item is scored on a 4-point Likert scale (1, strongly disagree; 4, strongly agree). Higher scores indicate greater fear of pain, movement, and injury. The TSK-11 has a two-factor structure covering activity avoidance and harm, and it has been demonstrated as having acceptable psychometric properties (Gómez-Pérez et al., 2011).
Self-efficacy
Self-efficacy was assessed through the Spanish version of the Chronic Pain Self-Efficacy Scale (CPSS) (Anderson et al., 1995). The scale was developed to measure the perceived self-efficacy and ability to cope with the consequences of pain in chronic pain patients. The Spanish version of this scale consists of 19 items and three domains that assess self-efficacy for pain management, physical functioning, and coping with symptoms. CPSS total scores are obtained by adding patient responses to each item, with higher scores indicating greater self-efficacy for managing pain. The Spanish version of the CPSS has been demonstrated as having acceptable psychometric properties (Anderson et al., 1995).
Procedure
After consenting to participation, all the recruited patients received a sociodemographic questionnaire to complete on the day of the measurement, which collected gender, date of birth, marital status, living arrangements, education level, and work status. When subjects completed the sociodemographic questionnaire, they were shown audio-visual material consisting of seven different MCTEs performed by a male subject (Fig. 1), which were first shown through photographs and then with videos. The videos and photographs used in this study featured very common exercises used in the treatment of CLBP, which have also been investigated in many scientific studies. Each time that the subjects watched a video or photography, they proceeded to assess the perceived difficulty and fear related to the MCTEs using a VAS. This procedure was the same for both groups.
Fig. 1.
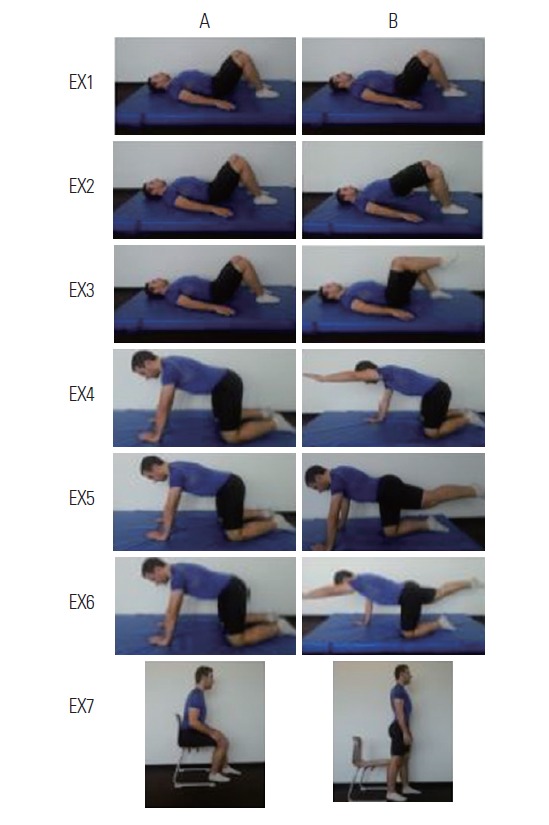
Representative photographs of exercises used to assess the perceived fear and difficulty. A, initial position; B, final position; EX, exercise; EX1, breathing lying up; EX2, pelvic bridging exercise; EX3, leg flexion; EX4, arm flexion; EX5, leg extension; EX6, arm flexion and leg extension; EX7, stand up from a chair.
Finally, each participant had to complete a battery of self-report measures (RMDQ, PCS, TSK-11, and CPSS) with an invariable order across the participants to assess psychological and disability aspects.
Sample size calculation
A power calculation was considered for the sample size calculation to detect between-group differences in the primary outcome measures (perception of fear or difficulty). To obtain 80% statistical power (1-β error probability) with an α error level probability of 0.05, we considered two groups and seven measurements for primary outcomes using analysis of variance (ANOVA) within-between interaction and a small effect size of 0.20. This generated a total sample size of 54 participants (27 participants per group). The sample size was estimated with G*Power ver. 3.1.7 (University of Dusseldorf, Dusseldorf, Germany) (Faul et al., 2007).
Statistical analysis
Descriptive statistics that were used to summarize data for continuous variables are presented as mean±standard deviation and the 95% confidence interval, while categorical variables are presented as an absolute number or relative frequency percentage. The central limit theorem justifies the use of parametric tests (Mouri, 2013; Nixon et al., 2010).
A chi-square test with residual analysis was used to compare categorical variables. A Student t-test was used to compare variables (sociodemographic questionnaire and self-report measures). For outcome variables, we used two-way repeated-measures models in ANOVA, including within-between interaction factors. The factors analysed were group (CG and CLBP group) and test (perception of fear or difficulty of each MCTEs). Test x group interaction was also analysed. The hypothesis of interest was the test x group interaction. Post hoc analysis with Bonferroni corrections was performed in the case of significant ANOVA findings for multiple comparisons between variables. Effect sizes (Cohen d) were calculated for outcome variables.
According to Cohen method, the magnitude of the effect was classified as small (0.20 to 0.49), medium (0.50 to 0.79), or large (0.8) (Cohen, 1988). The relationship between total information of the perceived difficulty and fear and psychological and disability variables was examined using Pearson correlation coefficients.
Multiple linear regression analysis was performed to estimate the strength of the associations between the results of mean of difficulty perceived to photographs and videos (DIFMEAN) (model 1) and mean of fear perceived to photographs and videos (FEARMEAN) (model 2) (criterion variables). PCS, TSK-11, CPSS, and RMDQ were used as predictor variables. Variance inflation factors were calculated to determine whether there were any multicollinearity issues in either of the two models.
The strength of association was examined using regression coefficients (β), P-values, and adjusted R2. Standardized beta coefficients were reported for each predictor variable included in the final reduced models to allow for direct comparison between the predictor variables in the regression model and the criterion variable being studied. Another general guideline provided for regression analyses is to have between 5 and 10 subjects per predictor variable (Hair et al., 1998). The IBM SPSS Statistics ver. 21.0 (IBM Co., Armonk, NY, USA) was used for statistical analysis. The significance level for all tests was set to P<0.05.
RESULTS
The baseline characteristics of sociodemographic, psychological, and pain-related variables of the sample are summarized in Table 1. The total study sample consisted of 60 participants (29 females and 31 males). Table 1 shows no statistically significant differences between groups in relation to sociodemographic variables except for three psychological variables: RMDQ, TSK-11, and PCS. There were no statistically significant differences for age, gender, height, weight, marital status, educational level, and self-efficacy between groups.
Table 1.
Descriptive statistics for demographic and clinical status variables (n=60)
| Variable | CLBP (n=30) | CG (n=30) | P-value |
|---|---|---|---|
| Age (yr) | 47.03±15.54 | 42.90±14.72 | 0.30* |
|
| |||
| Gender | 0.43† | ||
| Female | 16 (53.3) | 14 (46.7) | |
| Male | 13 (43.3) | 17 (56.7) | |
|
| |||
| Height (cm) | 165.4±7.88 | 168.5±7.46 | 0.12* |
|
| |||
| Weight (kg) | 69.13±10.74 | 74.10±12.95 | 0.11* |
|
| |||
| Marital status | |||
| Single | 8 (26.7) | 10 (33.3) | 0.95† |
| Widow | 1 (3.3) | 1 (3.3) | |
| Married | 20 (66.7) | 18 (60) | |
| Divorced | 1 (3.3) | 1 (3.3) | |
|
| |||
| Educational level | 0.06† | ||
| No studies | 6 (20.0) | 0 (0) | |
| Primary education | 7 (23.3) | 6 (20) | |
| Secondary education | 12 (40.0) | 16 (53.3) | |
| College education | 5 (16.7) | 8 (26.7) | |
|
| |||
| RMDQ | 7.23±4.08 | 0.93±1.34 | <0.01* |
|
| |||
| PCS | 21.13±11.04 | 10.43±8.16 | <0.01* |
|
| |||
| TSK-11 | 29.27±8.06 | 24.83±7.11 | 0.03* |
|
| |||
| CPSS | 250.97±32.56 | 254.87±25.14 | 0.61* |
Values are presented as mean±standard deviation or number (%).
CLBP, chronic low back pain; CG, control group; RMDQ, Roland-Morris Disability Questionnaire; PCS, Pain Catastrophizing Scale; TSK-11, Tampa Scale of Kinesiophobia-11; CPSS, Chronic Pain Self-Efficacy Scale.
Independent-samples t-test.
Chi-square tests.
Perceived fear toward photographs and videos
The ANOVA revealed significant differences between the type of the exercises (F=8.61, P<0.001), for the group factor vs. exercises (F=2.07, P<0.05), related to the interaction for exercise vs. group (F=34.82, P<0.001), and also regarding the perceived fear toward the photographs. The data for fear and difficulty perceived to the exercise photographs can be seen in Table 2. Post hoc analysis revealed higher values on the perceived fear for the CLBP group compared to the CG. Statistically significant differences between the patients and the CG were observed in relation to fear in response to 4 photographs (Table 2).
Table 2.
Descriptive data of results and multiple comparisons of fear and difficulty perceived to the exercise photographs
| Fear and difficulty | CLBP | CG | Mean difference (95% CI) | Effect size (d) |
|---|---|---|---|---|
| Fear perceived to photographs | ||||
| Exercise 1 | 3.70±7.82 | 1.23±5.67 | 2.47 (−1.06–5.99) | 0.36 |
| Exercise 2 | 19.07±23.87 | 6.27±12.73 | 12.80 (2.91–22.69)* | 0.67 |
| Exercise 3 | 12.43±17.00 | 0.53±1.71 | 11.90 (5.66–18.15)** | 0.98 |
| Exercise 4 | 8.53±12.37 | 4.10±11.67 | 4.43 (−1.78–10.65) | 0.37 |
| Exercise 5 | 15.90±22.19 | 6.53±16.87 | 9.37 (−0.82–19.55) | 0.47 |
| Exercise 6 | 22.63±24.79 | 7.83±16.97 | 14.80 (3.82–25.78)** | 0.70 |
| Exercise 7 | 10.13±20.04 | 0.80±3.35 | 9.33 (1.91–16.76)* | 0.65 |
|
| ||||
| Difficult perceived to photographs | ||||
| Exercise 1 | 5.27±9.73 | 1.43±4.54 | 3.84 (−0.21–7.89) | 0.51 |
| Exercise 2 | 26.78±22.73 | 11.96±20.90 | 14.9 (3.39–26.41)* | 0.68 |
| Exercise 3 | 15.30±18.93 | 3.43±6.52 | 11.87 (4.32–19.43)** | 0.84 |
| Exercise 4 | 11.83±16.50 | 6.57±13.54 | 5.27 (−2.71–13.24) | 0.34 |
| Exercise 5 | 16.50±18.04 | 9.36±18.72 | 7.14 (−2.53–16.81) | 0.38 |
| Exercise 6 | 29.53±25.30 | 17.21±24.04 | 12.32 (−0.68–25.32) | 0.49 |
| Exercise 7 | 12.07±19.38 | 2.71±5.46 | 9.35 (1.74–16.96)* | 0.66 |
Values are presented as mean±standard deviation.
CLBP, chronic low back pain; CG, control group; CI, confidence interval.
P<0.05.
P<0.01.
For perceived fear toward the videos, the ANOVA showed differences between exercises (F=34.98, P<0.001). There was also a significant effect between groups (F=9.71, P<0.001) and an interaction for group vs. exercises (F=2.01, P=0.046). The data for perceived fear toward the videos can be seen in Table 3. Fear values were higher for the low back pain group than for the CG. The post hoc analysis shows differences between groups (Table 3). Statistically significant differences between the patients and the CG were observed in relation to fear in response to three videos.
Table 3.
Descriptive data of results and multiple comparisons of fear and difficulty perceived to the exercise videos
| Fear and difficulty | CLBP | CG | Mean difference (95% CI) | Effect size (d) |
|---|---|---|---|---|
| Fear perceived to videos | ||||
| Exercise 1 | 2.43±5.81 | 1.37±6.39 | 1.07 (−2.09–4.22) | 0.17 |
| Exercise 2 | 20.43±26.41 | 10.03±20.92 | 10.40 (−1.91–22.71) | 0.43 |
| Exercise 3 | 11.03±13.53 | 0.57±1.94 | 10.47 (5.47–15.46)** | 1.08 |
| Exercise 4 | 7.23±8.41 | 5.50±14.11 | 1.73 (−4.27–7.74) | 0.15 |
| Exercise 5 | 14.50±20.69 | 6.17±18.99 | 8.33 (−1.93–18.6) | 0.42 |
| Exercise 6 | 23.17±27.66 | 9.20±16.60 | 13.97 (2.18–25.76)* | 0.61 |
| Exercise 7 | 11.37±20.78 | 2.13±5.36 | 9.23 (1.39–17.08)* | 0.61 |
|
| ||||
| Difficult perceived to videos | ||||
| Exercise 1 | 3.83±8.87 | 1.89±6.09 | 1.94 (−2.09–5.97) | 0.25 |
| Exercise 2 | 30.70±21.82 | 13.86±19.89 | 16.84 (5.84–27.85)** | 0.81 |
| Exercise 3 | 12.70±12.75 | 3.79±6.53 | 8.91 (3.53–14.30)** | 0.88 |
| Exercise 4 | 12.03±17.56 | 6.71±14.18 | 5.32 (−3.11–13.75) | 0.33 |
| Exercise 5 | 18.83±21.08 | 10.50±18.53 | 8.33 (−2.14–18.80) | 0.41 |
| Exercise 6 | 30.73±23.43 | 19.54±26.14 | 11.20 (−1.84–24.24) | 0.45 |
| Exercise 7 | 17.17±22.16 | 3.64±7.62 | 13.52 (4.68–22.37)** | 0.82 |
Values are presented as mean±standard deviation.
CLBP, chronic low back pain; CG, control group; CI, confidence interval.
P<0.05.
P<0.01.
Perceived difficulty to photograph and video
Regarding the perceived difficulty from photographs, the ANOVA revealed a significant difference for group vs. exercises (F=1.31, P=0.251) and for the group factor (F=15.86, P<0.001). There were also differences between exercises (F=57.07, P<0.001). The post hoc analysis showed an augmented perception of difficulty from the photographs in the CLBP group (Table 2). Regarding perceived difficulty, there were statistically significant differences for three photographs between groups.
For the perceived difficulty from the videos, the ANOVA showed statistically significant differences between exercises (F=64.95, P<0.001). There was also a difference in the interaction for group vs. exercises (F=2.06, P<0.05) and a significant difference between groups (F=21.06, P≤0.001). The post hoc analysis showed an increased level of perceived difficulty in the CLBP group, and there were statistically significant differences for three videos between groups.
Correlations analysis
Table 4 shows the results of the correlation analysis examining the bivariate relationships among psychological measures, as well as perceived difficulty and perceived fear measured just after showing the photographs and videos to the subjects. The strongest correlations were found in the analysis for the CLBP group with perceived disability measured with the RMDQ and mean of perceived difficulty to photographs and with RMDQ and mean of perceived difficulty to videos. The perceived difficulty between photographs and videos was equal (r=0.68, P<0.001). For the CG, the greatest correlation was between self-efficacy measured with the CPSS and the difficulty perceived in the photographs, which had a negative association (r=−0.68; P<0.001). Table 4 shows the results of bivariate correlations for the CG and the CLBP group.
Table 4.
Pearson correlation coefficient between variables analyzed in the study
| Variable | DPPMEAN | DPVMEAN | DIFMEAN | FPPMEAN | FPVMEAN | FEARMEAN |
|---|---|---|---|---|---|---|
| RMDQ | ||||||
| CLBP | 0.67** | 0.67** | 0.68** | 0.58** | 0.51** | 0.55** |
| CG | 0.11 | 0.12 | 0.12 | 0.30 | 0.30 | 0.30 |
|
| ||||||
| PCS | ||||||
| CLBP | 0.34 | 0.40* | 0.38* | 0.09 | −0.01 | 0.05 |
| CG | 0.51** | 0.49** | 0.51** | 0.38* | 0.37* | 0.38* |
|
| ||||||
| TSK-11 | ||||||
| CLBP | 0.36 | 0.28 | 0.33 | 0.28 | 0.28 | 0.29 |
| CG | 0.45* | 0.50** | 0.48* | 0.42* | 0.37* | 0.40 |
|
| ||||||
| CPSS | ||||||
| CLBP | 0.17 | 0.20 | 0.19 | −0.05 | −0.04 | −0.04 |
| CG | −0.68** | −0.58** | −0.63** | −0.51** | −0.43* | −0.47** |
DPPMEAN, mean of perceived difficulty to photographs; DPVMEAN, mean of perceived difficulty to videos; DIFMEAN, mean of perceived difficulty to photographs and videos; FPPMEAN, mean of perceived fear to photographs; FPVMEAN, mean of perceived fear to videos; FEARMEAN, mean of perceived fear to photographs and videos; CLBP, chronic low back pain; CG, control group; RMDQ, Roland-Morris Disability Questionnaire; PCS, Pain Catastrophizing Scale; TSK-11, Tampa Scale of Kinesiophobia-11; CPSS, Chronic Pain Self-Efficacy Scale.
P<0.05.
P<0.01.
Multiple linear regression analysis
A linear regression analysis was performed to evaluate contributors to DIFMEAN revealing equal perceived difficulty between the photographs and videos, and FEARMEAN revealing equal perceived fear between photographs and videos. The results are presented in the Tables 5 and 6. In the first model, as shown in Table 5, the criterion variable DIFMEAN was predicted by disability measured with the RMDQ (for the CLBP group), explaining 44% of the variance. The variables PCS (β=0.15, P=0.32), TSK (β= −0.03, P=0.88), and CPSS (β=0.16, P=0.24) were not significant predictors. In the CG, the variables CPSS (β= −0.58, P<0.01) and PCS (β=0.43, P=0.003) explained 38% of the variance in predicting the criterion variable DIFMEAN. The RMDQ (β=0.94, P=0.49) and the TSK-11 (β=0.25, P=0.08) were not significant predictors.
Table 5.
Multiple linear regression analysis for mean of perceived difficulty to photographs and videos in each group
| Group | Regression coefficient (B) | Standardized coefficient (β) | P-value | VIF | Overall model | ||
|---|---|---|---|---|---|---|---|
|
| |||||||
| R2 | Adjusted R2 | F | |||||
| CLBP | 0.46 | 0.44 | 24.19 | ||||
| Predictor variable | |||||||
| RMDQ | 30.24 | 0.68 | 0.63 | 1.00 | |||
| Excluded variable | |||||||
| PCS | - | 0.15 | 0.32 | 1.15 | |||
| TSK-11 | - | −0.03 | 0.88 | 1.13 | |||
| CPSS | - | 0.16 | 0.24 | 1.00 | |||
|
| |||||||
| CG | 0.40 | 0.38 | 17.59 | ||||
| Predictor variable | |||||||
| CPSS | −3.83 | −0.58 | <0.01 | 1.02 | |||
| PCS | 8.27 | 0.43 | 0.003 | 1.02 | |||
| Excluded variable | |||||||
| RMDQ | - | 0.94 | 0.49 | 1.04 | |||
| TSK-11 | - | 0.25 | 0.08 | 1.24 | |||
VIF, variance inflation factor; CLBP, chronic low back pain; CG, control group; RMDQ, Roland-Morris Disability Questionnaire; PCS, Pain Catastrophizing Scale; TSK-11, Tampa Scale of Kinesiophobia-11; CPSS, Chronic Pain Self-Efficacy Scale.
Table 6.
Multiple linear regression analysis for mean of perceived fear to photographs and videos in each group
| Group | Regression coefficient (B) | Standardized coefficient (β) | P-value | VIF | Overall model | ||
|---|---|---|---|---|---|---|---|
|
| |||||||
| R2 | Adjusted R2 | F | |||||
| CLBP | 0.31 | 0.28 | 12.36 | ||||
| Predictor variable | |||||||
| RMDQ | 25.74 | 0.55 | 0.02 | 1.00 | |||
| Excluded variable | |||||||
| PCS | - | -0.18 | 0.31 | 1.15 | |||
| TSK-11 | - | 0.01 | 0.97 | 1.13 | |||
| CPSS | - | −0.07 | 0.69 | 1.00 | |||
|
| |||||||
| CG | 0.59 | 0.34 | 7.09 | ||||
| Predictor variable | |||||||
| CPSS | −2.14 | −0.45 | 0.01 | 1.00 | |||
| PCS | 5.11 | 0.35 | 0.03 | 1.00 | |||
| Excluded variable | |||||||
| RMDQ | - | 0.25 | 0.11 | 1.03 | |||
| TSK-11 | - | 0.21 | 0.22 | 1.24 | |||
VIF, variance inflation factor; CLBP, chronic low back pain; CG, control group; RMDQ, Roland-Morris Disability Questionnaire; PCS, Pain Catastrophizing Scale; TSK-11, Tampa Scale of Kinesiophobia-11; CPSS, Chronic Pain Self-Efficacy Scale.
In the second model, as presented in Table 6, the FEARMEAN was predicted by RMDQ for the CLBP group, explaining 28% of the variance. The PCS (β= −0.18, P=0.31), TSK (β=0.01, P=0.97), and CPSS (β= −0.07, P=0.69) were not significant predictors. For the CG, the CPSS (β= −0.45, P=0.01), and the PCS (β=0.35, P=0.03) were significant predictors, explaining 34% of the variance, but the variables RMDQ (β=0.25, P=0.22) and TSK (β=0.21, P=0.22) were not significant predictors.
DISCUSSION
The main objective of this research was to identify if there were any differences in the perceived level of difficulty or fear between healthy control subjects and patients with CLBP when showing them photographs and videos of MCTEs that are widely used in physiotherapy practice. To our knowledge, this is the first study evaluating the perception of difficulty and fear from therapeutic exercise. We believe that the findings of this research have clinical importance, since therapeutic exercise is one of the most widely used treatments for patients with CLBP.
Our results show high levels of perceived fear and difficulty from most MCTEs videos and photographs displayed to patients with CLBP. A similar result to ours was described by Basler et al. (2008), who found that CLBP patients had higher fear-avoidance belief levels related to photographs of daily life activities compared to asymptomatic subjects.
Disability and perception of difficulty and fear
An important discovery related to the CLBP group is that disability was a predictor for both mean of perception of fear and difficulty of the exercises. This result is widely supported by previous research in which relations between disability and fear avoidance beliefs were observed (Basler et al., 2008; Chung et al., 2013; Thomas et al., 2010; Verbunt et al., 2003). Unexpectedly, the kinesiophobia measured with the TSK-11 was not identified as a predictor or a variable correlated with the overall perception of fear toward the displayed exercises, despite being constructs that apparently assess similar aspects. In connection to this, Demoulin et al. (2013) did not find statistically significant correlations between several pain-related fear variables measured with the VAS, the TSK-11, and the Photograph Series of Daily Activities.
Regarding the overall perceived difficulty, it is hard to explain our results since there have been no similar studies where these variables were measured. We suggest that the level of disability to perform daily life activities can generate an altered cognitive response in evaluating the displayed exercises by categorizing them with larger difficulty than they may actually have. Another aspect is that current evidence for patients with CLBP describes that patients’ physical performance is related to the perception of disability (Pfingsten et al., 2014), and it has been shown that the perception of fear is related to functionally limitations (de Jong et al., 2011).
Self-efficacy, catastrophizing, and difficulty and fear perceived
The result of the multiple regression analysis for the group of asymptomatic subjects showed that self-efficacy and pain catastrophizing are predictors of mean of perceived fear and difficulty when we showed the exercises. Although this group did not have subjects with CLBP or other musculoskeletal pain, it is interesting to see how these constructs relate with perceptions of difficulty and fear in asymptomatic subjects. It is important to remark that self-efficacy was negatively correlated, while association with pain catastrophizing was positive. Similar results have been observed in patients with CLBP. De Moraes Vieira et al. (2014) found reduced self-efficacy levels and an increase in fear-avoidance factors. Recent studies highlight the importance of self-efficacy over disability (Costa Lda et al., 2011; Morone et al., 2009). In relation to pain catastrophizing, an association was observed with beliefs about physical activity within the framework of the fear avoidance model (George et al., 2011). We could partially relate this data to our study when applying it only to asymptomatic subjects.
Limitations
This study presents some limitations that must be considered. The physical activity levels were not previously assessed among the subjects of this study, so it is possible that this factor may influence the subjects’ perceived difficulty and fear. It would be interesting for future studies to identify whether this factor influences the results.
An important limitation is that the instrument used to measure the perception of fear has not been validated, and its reliability is unknown, although it has been used in different studies (Demoulin et al., 2013; George et al., 2009). Furthermore, it was the first time that the instrument for measuring perceived difficulty was used, and we have no reliability data for this tool. We only used self-report measures to relate them to the perceived difficulty and fear. It would have been interesting to introduce physiological and functional capacity variables to check if they were directly related to the primary variables.
Although this research has a balanced sample of men and women, no statistical analyses were performed to see if the behaviour of the secondary variables was influenced by the gender factor. Another limitation may be the choice of a few psychological variables for assessment without taking into account other aspects such as motivation (Jensen et al., 2003) or acceptance (Hayes et al., 2006), which are important factors that can interfere with fear or difficulty of the subject. Also, as suggested in different motivational models (Jensen et al., 2003; Viane et al., 2003), having a specific goal and belief by the patients in their own ability (self-efficacy) to reach a goal will directly influence the results. Finally, a potential bias of the results could be the nonprobabilistic convenience of the sample.
Clinical and scientific implications
Therapeutic exercise should continue to be one of the treatment strategies of the physiotherapists, because there is evidence enough supporting it is useful for treating CLBP (Baena-Beato et al., 2014; Daenen et al., 2015; Hidalgo et al., 2014; Wells et al., 2014). However, in view of our findings, we believe that it should be considered from therapeutic and diagnostic perspectives that fear-avoidance factors could be directly involved in perception and personal evaluation of MCTEs that a patient can learn. Future studies should explore the possible involvement of perceived difficulty and fear about exercise and how they affect proper motor action. Related to this, a recent study found that fear of movement is associated with trunk stiffness (Karayannis et al., 2013).
We consider that when fear-avoidance factors involved in pain or movement of the patient are identified, they should be incorporated into more specific treatment strategies that reduce such maladaptive beliefs. Therapeutic strategies that incorporate the model of fear avoidance have been reported, including graded activity (George et al., 2003; Lindström et al., 1992; van der Giessen et al., 2012), graduated exposure (de Jong et al., 2011; Leeuw et al., 2008), and therapeutic education (Burton et al., 1999; Coudeyre et al., 2007; de Jong et al., 2011). These methods have also been effective in reducing fear of movement and catastrophizing (de Jong et al., 2011). Inclusion of strategies to reduce fear avoidance is the key to the success of treatment (Wertli et al., 2014). We consider it necessary to include such strategies before starting the therapeutic exercise prescription in patients with CLBP. It seems necessary to consider a biopsychosocial model when diagnosing and planning treatment for patients with CLBP.
In conclusion, the results of this study shows that difficulty and fear of movement perceived in assessing typical exercises in physiotherapy protocols are different between asymptomatic subjects and patients that suffer from CLBP. Disability and psychological factors were correlated with perceived difficulty and fear by patients and asymptomatic subjects when the subjects watched videos and photographs of the exercises. New information has been provided about possible factors that can alter the prescription of MCTEs for the lumbar region.
Footnotes
CONFLICT OF INTEREST
No potential conflict of interest relevant to this article was reported.
REFERENCES
- Airaksinen O, Brox JI, Cedraschi C, Hildebrandt J, Klaber-Moffett J, Kovacs F, Mannion AF, Reis S, Staal JB, Ursin H, Zanoli G COST B13 Working Group on Guidelines for Chronic Low Back Pain. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur Spine J. 2006;15(Suppl 2):S192–300. doi: 10.1007/s00586-006-1072-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Anderson KO, Dowds BN, Pelletz RE, Edwards WT, Peeters-Asdourian C. Development and initial validation of a scale to measure self-efficacy beliefs in patients with chronic pain. Pain. 1995;63:77–84. doi: 10.1016/0304-3959(95)00021-J. [DOI] [PubMed] [Google Scholar]
- Baena-Beato PÁ, Delgado-Fernández M, Artero EG, Robles-Fuentes A, Gatto-Cardia MC, Arroyo-Morales M. Disability predictors in chronic low back pain after aquatic exercise. Am J Phys Med Rehabil. 2014;93:615–623. doi: 10.1097/PHM.0000000000000123. [DOI] [PubMed] [Google Scholar]
- Barke A, Baudewig J, Schmidt-Samoa C, Dechent P, Kröner-Herwig B. Neural correlates of fear of movement in high and low fear-avoidant chronic low back pain patients: an event-related fMRI study. Pain. 2012;153:540–552. doi: 10.1016/j.pain.2011.11.012. [DOI] [PubMed] [Google Scholar]
- Barzilay Y, Segal G, Lotan R, Regev G, Beer Y, Lonner BS, Mor A, Elbaz A. Patients with chronic non-specific low back pain who reported reduction in pain and improvement in function also demonstrated an improvement in gait pattern. Eur Spine J. 2015 May 16; doi: 10.1007/s00586-015-4004-0. [Epub]. http://dx.doi.org/10.1007/s00586-015-4004-0. [DOI] [PubMed]
- Basler HD, Luckmann J, Wolf U, Quint S. Fear-avoidance beliefs, physical activity, and disability in elderly individuals with chronic low back pain and healthy controls. Clin J Pain. 2008;24:604–610. doi: 10.1097/AJP.0b013e31816b54f6. [DOI] [PubMed] [Google Scholar]
- Burton AK, Waddell G, Tillotson KM, Summerton N. Information and advice to patients with back pain can have a positive effect. A randomized controlled trial of a novel educational booklet in primary care. Spine (Phila Pa 1976) 1999;24:2484–2491. doi: 10.1097/00007632-199912010-00010. [DOI] [PubMed] [Google Scholar]
- Chung EJ, Hur YG, Lee BH. A study of the relationship among fear-avoidance beliefs, pain and disability index in patients with low back pain. J Exerc Rehabil. 2013;9:532–535. doi: 10.12965/jer.130079. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Hillsdale (NJ): Lawrence Erlbaum Associates; 1988. [Google Scholar]
- Costa Lda C, Maher CG, McAuley JH, Hancock MJ, Smeets RJ. Self-efficacy is more important than fear of movement in mediating the relationship between pain and disability in chronic low back pain. Eur J Pain. 2011;15:213–219. doi: 10.1016/j.ejpain.2010.06.014. [DOI] [PubMed] [Google Scholar]
- Coudeyre E, Tubach F, Rannou F, Baron G, Coriat F, Brin S, Revel M, Poiraudeau S. Effect of a simple information booklet on pain persistence after an acute episode of low back pain: a non-randomized trial in a primary care setting. PLoS One. 2007;2:e706. doi: 10.1371/journal.pone.0000706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Daenen L, Varkey E, Kellmann M, Nijs J. Exercise, not to exercise, or how to exercise in patients with chronic pain? Applying science to practice. Clin J Pain. 2015;31:108–114. doi: 10.1097/AJP.0000000000000099. [DOI] [PubMed] [Google Scholar]
- de Jong JR, Vlaeyen JW, de Gelder JM, Patijn J. Pain-related fear, perceived harmfulness of activities, and functional limitations in complex regional pain syndrome type I. J Pain. 2011;12:1209–1218. doi: 10.1016/j.jpain.2011.06.010. [DOI] [PubMed] [Google Scholar]
- de la Cruz-Sánchez E, Torres-Bonete MD, García-Pallarés J, Gascón-Cánovas JJ, Valero-Valenzuela A, Pereñíguez-Barranco JE. Back pain and restricted daily physical activity in the Spanish adult population. An Sist Sanit Navar. 2012;35:241–249. doi: 10.4321/s1137-66272012000200006. [DOI] [PubMed] [Google Scholar]
- de Moraes Vieira EB, de Góes Salvetti M, Damiani LP, de Mattos Pimenta CA. Self-efficacy and fear avoidance beliefs in chronic low back pain patients: coexistence and associated factors. Pain Manag Nurs. 2014;15:593–602. doi: 10.1016/j.pmn.2013.04.004. [DOI] [PubMed] [Google Scholar]
- Demoulin C, Huijnen IP, Somville PR, Grosdent S, Salamun I, Crielaard JM, Vanderthommen M, Volders S. Relationship between different measures of pain-related fear and physical capacity of the spine in patients with chronic low back pain. Spine J. 2013;13:1039–1047. doi: 10.1016/j.spinee.2013.02.037. [DOI] [PubMed] [Google Scholar]
- Faul F, Erdfelder E, Lang AG, Buchner A. G*Power 3: a flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav Res Methods. 2007;39:175–191. doi: 10.3758/bf03193146. [DOI] [PubMed] [Google Scholar]
- García Campayo J, Rodero B, Alda M, Sobradiel N, Montero J, Moreno S. Validation of the Spanish version of the Pain Catastrophizing Scale in fibromyalgia. Med Clin (Barc) 2008;131:487–492. doi: 10.1157/13127277. [DOI] [PubMed] [Google Scholar]
- George SZ, Bialosky JE, Fritz JM. Physical therapist management of a patient with acute low back pain and elevated fear-avoidance beliefs. Phys Ther. 2004;84:538–549. [PubMed] [Google Scholar]
- George SZ, Calley D, Valencia C, Beneciuk JM. Clinical Investigation of Pain-related Fear and Pain Catastrophizing for Patients With Low Back Pain. Clin J Pain. 2011;27:108–115. doi: 10.1097/AJP.0b013e3181f21414. [DOI] [PubMed] [Google Scholar]
- George SZ, Fritz JM, Bialosky JE, Donald DA. The effect of a fear-avoidance-based physical therapy intervention for patients with acute low back pain: results of a randomized clinical trial. Spine (Phila Pa 1976) 2003;28:2551–2560. doi: 10.1097/01.BRS.0000096677.84605.A2. [DOI] [PubMed] [Google Scholar]
- George SZ, Valencia C, Zeppieri G, Jr, Robinson ME. Development of a self-report measure of fearful activities for patients with low back pain: the fear of daily activities questionnaire. Phys Ther. 2009;89:969–979. doi: 10.2522/ptj.20090032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gómez-Pérez L, López-Martínez AE, Ruiz-Párraga GT. Psychometric Properties of the Spanish Version of the Tampa Scale for Kinesiophobia (TSK) J Pain. 2011;12:425–435. doi: 10.1016/j.jpain.2010.08.004. [DOI] [PubMed] [Google Scholar]
- Hair JF, Anderson RE, Tatham RL, Black W. Multivariate data analysis. 5th ed. Englewood Cliffs: Prentice Hall; 1998. [Google Scholar]
- Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes and outcomes. Behav Res Ther. 2006;44:1–25. doi: 10.1016/j.brat.2005.06.006. [DOI] [PubMed] [Google Scholar]
- Hidalgo B, Detrembleur C, Hall T, Mahaudens P, Nielens H. The efficacy of manual therapy and exercise for different stages of non-specific low back pain: an update of systematic reviews. J Man Manip Ther. 2014;22:59–74. doi: 10.1179/2042618613Y.0000000041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Houben RM, Ostelo RW, Vlaeyen JW, Wolters PM, Peters M, Stomp-van den Berg SG. Health care providers’ orientations towards common low back pain predict perceived harmfulness of physical activities and recommendations regarding return to normal activity. Eur J Pain. 2005;9:173–183. doi: 10.1016/j.ejpain.2004.05.002. [DOI] [PubMed] [Google Scholar]
- Jensen MP, Nielson WR, Kerns RD. Toward the development of a motivational model of pain self-management. J Pain. 2003;4:477–492. doi: 10.1016/s1526-5900(03)00779-x. [DOI] [PubMed] [Google Scholar]
- Karayannis NV, Smeets RJ, van den Hoorn W, Hodges PW. Fear of movement is related to trunk stiffness in low back pain. PLoS One. 2013;8:e67779. doi: 10.1371/journal.pone.0067779. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klaber Moffett JA, Carr J, Howarth E. High fear-avoiders of physical activity benefit from an exercise program for patients with back pain. Spine (Phila Pa 1976) 2004;29:1167–1172. doi: 10.1097/00007632-200406010-00002. [DOI] [PubMed] [Google Scholar]
- Kori SH, Miller RP, Todd DD. Kinesiophobia: a new view of chronic pain behavior. Pain Manag. 1990;3:35–43. [Google Scholar]
- Kovacs FM, Llobera J, Gil Del Real MT, Abraira V, Gestoso M, Fernández C, Primaria Group KA. Validation of the spanish version of the Roland-Morris questionnaire. Spine (Phila Pa 1976) 2002;27:538–542. doi: 10.1097/00007632-200203010-00016. [DOI] [PubMed] [Google Scholar]
- Lawford BJ, Walters J, Ferrar K. Does walking improve disability status, function, or quality of life in adults with chronic low back pain? A systematic review. Clin Rehabil. 2015 Jun 18; doi: 10.1177/0269215515590487. [Epub]. http://dx.doi.org/10.1177/0269215515590487. [DOI] [PubMed]
- Leeuw M, Goossens ME, van Breukelen GJ, de Jong JR, Heuts PH, Smeets RJ, Köke AJ, Vlaeyen JW. Exposure in vivo versus operant graded activity in chronic low back pain patients: results of a randomized controlled trial. Pain. 2008;138:192–207. doi: 10.1016/j.pain.2007.12.009. [DOI] [PubMed] [Google Scholar]
- Leeuw M, Peters ML, Wiers RW, Vlaeyen JW. Measuring fear of movement/(re)injury in chronic low back pain using implicit measures. Cogn Behav Ther. 2007;36:52–64. doi: 10.1080/16506070601070400. [DOI] [PubMed] [Google Scholar]
- Lindström I, Ohlund C, Eek C, Wallin L, Peterson LE, Fordyce WE, Nachemson AL. The effect of graded activity on patients with subacute low back pain: a randomized prospective clinical study with an operant-conditioning behavioral approach. Phys Ther. 1992;72:279–290. doi: 10.1093/ptj/72.4.279. [DOI] [PubMed] [Google Scholar]
- Loney PL, Stratford PW. The prevalence of low back pain in adults: a methodological review of the literature. Phys Ther. 1999;79:384–396. [PubMed] [Google Scholar]
- Morone NE, Karp JF, Lynch CS, Bost JE, El Khoudary SR, Weiner DK. Impact of chronic musculoskeletal pathology on older adults: a study of differences between knee OA and low back pain. Pain Med. 2009;10:693–701. doi: 10.1111/j.1526-4637.2009.00565.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mouri H. Log-normal distribution from a process that is not multiplicative but is additive. Phys Rev E Stat Nonlin Soft Matter Phys. 2013;88:042124. doi: 10.1103/PhysRevE.88.042124. [DOI] [PubMed] [Google Scholar]
- Nixon RM, Wonderling D, Grieve RD. Non-parametric methods for cost-effectiveness analysis: the central limit theorem and the bootstrap compared. Health Econ. 2010;19:316–333. doi: 10.1002/hec.1477. [DOI] [PubMed] [Google Scholar]
- Pfingsten M, Lueder S, Luedtke K, Petzke F, Hildebrandt J. Significance of physical performance tests for patients with low back pain. Pain Med. 2014;15:1211–1221. doi: 10.1111/pme.12482. [DOI] [PubMed] [Google Scholar]
- Roland M, Morris R. A study of the natural history of back pain. Part I: development of a reliable and sensitive measure of disability in low-back pain. Spine (Phila Pa 1976) 1983;8:141–144. doi: 10.1097/00007632-198303000-00004. [DOI] [PubMed] [Google Scholar]
- Sullivan MJ, Bishop SR, Pivik J. The pain catastrophizing scale: development and validation. Psychol Assess. 1995;7:524–532. [Google Scholar]
- Thomas EN, Pers YM, Mercier G, Cambiere JP, Frasson N, Ster F, Hérisson C, Blotman F. The importance of fear, beliefs, catastrophizing and kinesiophobia in chronic low back pain rehabilitation. Ann Phys Rehabil Med. 2010;53:3–14. doi: 10.1016/j.rehab.2009.11.002. [DOI] [PubMed] [Google Scholar]
- Trost Z, France CR, Thomas JS. Examination of the photograph series of daily activities (PHODA) scale in chronic low back pain patients with high and low kinesiophobia. Pain. 2009;141:276–282. doi: 10.1016/j.pain.2008.11.016. [DOI] [PubMed] [Google Scholar]
- van der Giessen RN, Speksnijder CM, Helders PJ. The effectiveness of graded activity in patients with non-specific low-back pain: a systematic review. Disabil Rehabil. 2012;34:1070–1076. doi: 10.3109/09638288.2011.631682. [DOI] [PubMed] [Google Scholar]
- Verbunt JA, Seelen HA, Vlaeyen JW, van der Heijden GJ, Knottnerus JA. Fear of injury and physical deconditioning in patients with chronic low back pain. Arch Phys Med Rehabil. 2003;84:1227–1232. doi: 10.1016/s0003-9993(03)00132-1. [DOI] [PubMed] [Google Scholar]
- Viane I, Crombez G, Eccleston C, Poppe C, Devulder J, Van Houdenhove B, De Corte W. Acceptance of pain is an independent predictor of mental well-being in patients with chronic pain: empirical evidence and reappraisal. Pain. 2003;106:65–72. doi: 10.1016/s0304-3959(03)00291-4. [DOI] [PubMed] [Google Scholar]
- Vlaeyen JW, Kole-Snijders AM, Boeren RG, van Eek H. Fear of movement/(re)injury in chronic low back pain and its relation to behavioral performance. Pain. 1995;62:363–72. doi: 10.1016/0304-3959(94)00279-N. [DOI] [PubMed] [Google Scholar]
- von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61:344–349. doi: 10.1016/j.jclinepi.2007.11.008. [DOI] [PubMed] [Google Scholar]
- Wälti P, Kool J, Luomajoki H. Short-term effect on pain and function of neurophysiological education and sensorimotor retraining compared to usual physiotherapy in patients with chronic or recurrent non-specific low back pain, a pilot randomized controlled trial. BMC Musculoskelet Disord. 2015;16:83. doi: 10.1186/s12891-015-0533-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wells C, Kolt GS, Marshall P, Hill B, Bialocerkowski A. The effectiveness of Pilates exercise in people with chronic low back pain: a systematic review. PLoS One. 2014;9:e100402. doi: 10.1371/journal.pone.0100402. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wertli MM, Rasmussen-Barr E, Held U, Weiser S, Bachmann LM, Brunner F. Fear-avoidance beliefs-a moderator of treatment efficacy in patients with low back pain: a systematic review. Spine J. 2014;14:2658–2678. doi: 10.1016/j.spinee.2014.02.033. [DOI] [PubMed] [Google Scholar]
- Yue YS, Wang XD, Xie B, Li ZH, Chen BL, Wang XQ, Zhu Y. Sling exercise for chronic low back pain: a systematic review and meta-analysis. PLoS One. 2014;9:e99307. doi: 10.1371/journal.pone.0099307. [DOI] [PMC free article] [PubMed] [Google Scholar]