

Treatment of acute myeloid leukemia (AML) is generally dictated by the patient’s age and performance status and the biological, genetic, and molecular characteristics of the disease.1 Specific cytogenetic alterations divide AML classification into three risk-based categories: favorable, intermediate and unfavorable.2,3 Patients with normal karyotype belong to the intermediate-risk category, and their prognosis is further determined by specific genetic alterations, particularly Nucleophosmin-1 (NPM1) mutation and FLT-3 internal tandem duplication (ITD).4–6
NPM1 is an essential gene that encodes a nucleolar shuttling protein. It is the most frequently mutated gene in AML, accounting for more than one third of all AML cases.7,8 In patients with normal diploid karyotype, NPM1 mutation, when present alone, is associated with a lower risk of relapse, and confers a major survival advantage.9 However, the presence of both NPM1 mutation and FLT3-ITD results in a poor prognosis. Therefore, patients with unmutated NPM1 or patients with both NPM1 mutation and FLT3-ITD are generally referred for an allogeneic hematopoietic cell transplant (allo-HCT) in first complete remission (CR1). Conversely, patients with normal karyotype and NPM1 mutation without FLT3-ITD belong to the European LeukemiaNet (ELN) favorable-risk group and, accordingly, are referred to transplant only at the time of relapse. However, little is known about post-transplant outcomes in this particular setting and the predictive factors for disease-free survival. Furthermore, recent data based on the donor versus no-donor approach indicates a beneficial effect of allo-HCT on leukemia-free survival (LFS) but not overall survival (OS) for NPM1+FLT3- AML patients.10–12
To explore the prognosis of patients allografted for AML with normal diploid karyotype and mutated NPM1 without FLT3-ITD, we performed a retrospective multi-center analysis. Data were provided and approved for this study by the Acute Leukemia Working Party (ALWP) of the EBMT group registry. The latter is a voluntary working group of more than 500 transplant centers that are required to report all consecutive stem cell transplantations and follow-ups once a year. The participating centers are listed in the Online Supplementary TableS1. Audits are routinely performed to determine the accuracy of the data. Since 1990, patients have provided informed consent authorizing the use of their personal information for research purposes. Eligibility criteria for this analysis included adult patients (age >18 years) with AML, transplanted between 2006 and 2012, from an HLA-matched related (MRD) or matched unrelated (MUD) donor with bone marrow (BM) or G-CSF-mobilized peripheral blood stem cells (PBSCs).
Endpoints included LFS, cumulative incidence of relapse (CIR), NRM, OS and acute and chronic GVHD. The probabilities of OS and LFS were calculated by using the Kaplan-Meier estimator. The probabilities of acute and chronic GVHD, NRM, and relapse were calculated by using the cumulative incidence estimator to accommodate competing risks. For NRM, relapse was the competing risk, and for relapse, the competing risk was NRM. For acute and chronic GVHD, death without the event was the competing risk. For all prognostic analyses, continuous variables were categorised and the median was used as a cut-off point. Univariate comparisons were done using the log-rank test for LFS and OS, and Gray’s test was used for cumulative incidences. Chronic GVHD was analyzed as a time-dependent variable. A Cox proportional hazards model was used for multivariate regression. Factors known to influence the outcome associated with a P value less than 0.10 with any endpoint by univariate analysis were included in the model. Results are expressed as hazard ratio (HR) with 95% confidence interval (CI). All tests were two-sided. Statistical analyses were performed with SPSS 19 (SPSS Inc./IBM, Armonk, NY, USA) and R 3.0.1 (R Development Core Team, Vienna, Austria) software packages.
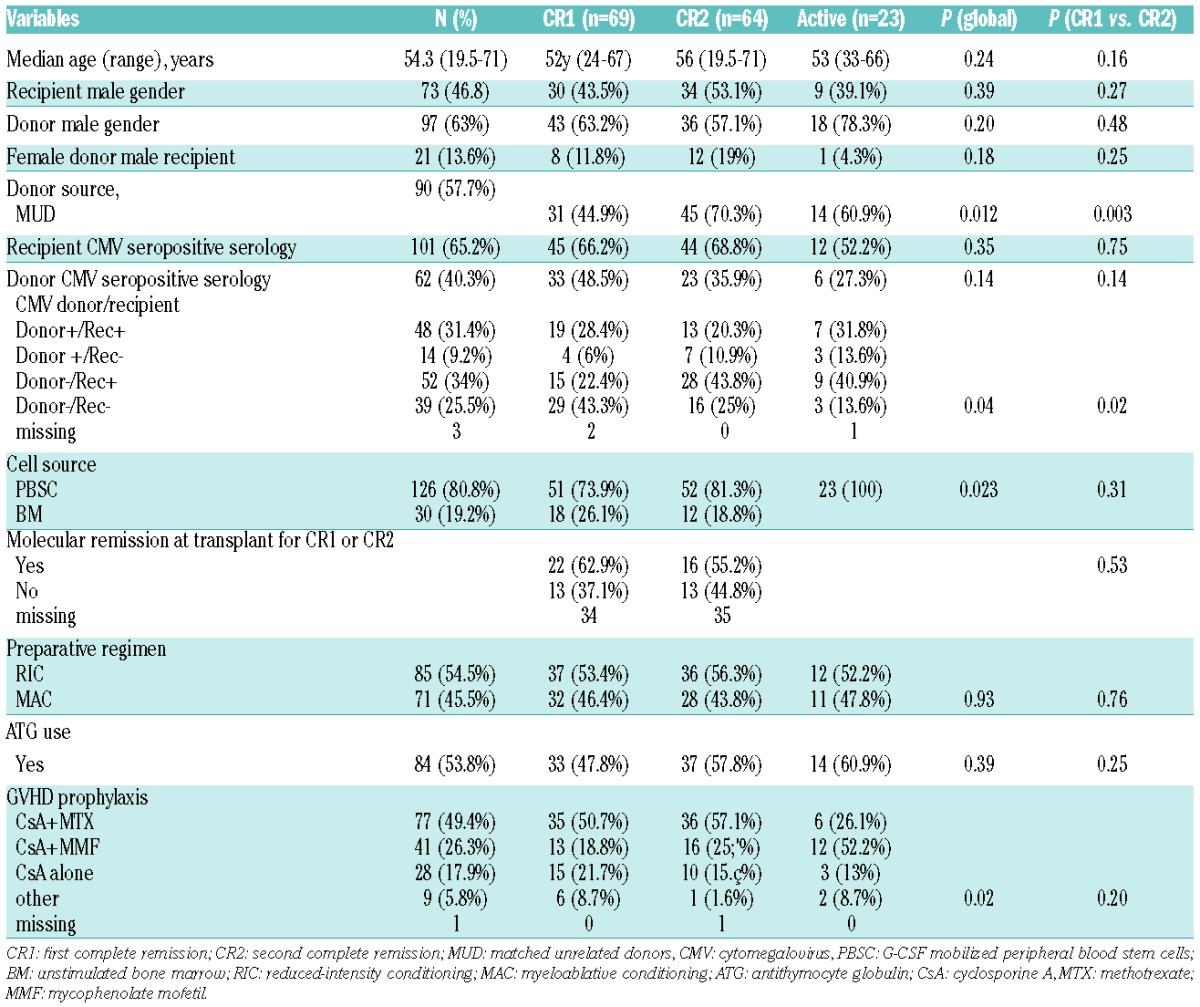
In this study, we evaluated the post-transplant outcomes of 156 patients (females=83, 53%; males=73, 47%), with a median age of 54.3 (19.5–71) years and normal diploid karyotype and mutated NPM1 without FLT3-ITD, who underwent an allo-HCT between 2006 and 2012. The median follow-up from time of allografting was 32 (2–86) months. At transplantation, 69 patients (44%) were in CR1, 64 (41%) in CR2 and 23 (15%) had advanced/active disease. The median time from initial diagnosis to transplantation was 161 (89–483) days in patients transplanted in CR1, 618 (189–1333) days in CR2 and 315 (189–896) days in advanced/active disease. The median time from diagnosis to CR1 was 39 (16–176) days in patients transplanted in CR1 and 41 (14–169) days in patients transplanted in CR2. The graft source was limited to matched related (MRD) (N=66, 42%) or matched unrelated (MUD) donors (N=90, 58%), including 21 male patients (14%) allografted from female donors. The cell source consisted of BM (N=30, 19%), G–CSF mobilized PBSC (N=125, 80%), or both (N=1). A reduced intensity conditioning (RIC) was used in 85 patients (54%), whereas 71 (46%) received a myeloablative conditioning (MAC). Patients’, donors’, and disease characteristics are summarized in Table 1.
Table 1.
Patient, disease and treatment characteristics.
Thirty patients (19%) developed acute GVHD grade II–IV. Patients allografted from MUD had a higher 100-day cumulative incidence of acute GVHD above grade II [MUD=28% (95%CI=19–39%)] than MRD [MRD=12% (95%CI=5–22%), P=0.02]. Patients older than the median age had a higher 2-year cumulative incidence of NRM [20% (95%CI=11–31%) vs. 7% [95%CI=2–14%], P=0.03]. Overall, the cumulative incidence of cGVHD at 2 years was 37%. When cGVHD was analyzed as a time-dependent variable, it had no significant effect on CIR [HR=0.78 (95%CI=0.31–1.97), P=0.59], NRM [HR=3.23 (95%CI=0.83–12.56), P=0.09], LFS [HR=1.21 (95%CI=0.58–2.55), P=0.61] or OS [HR=1.24 (95%CI=0.58–2.64), P=0.58].
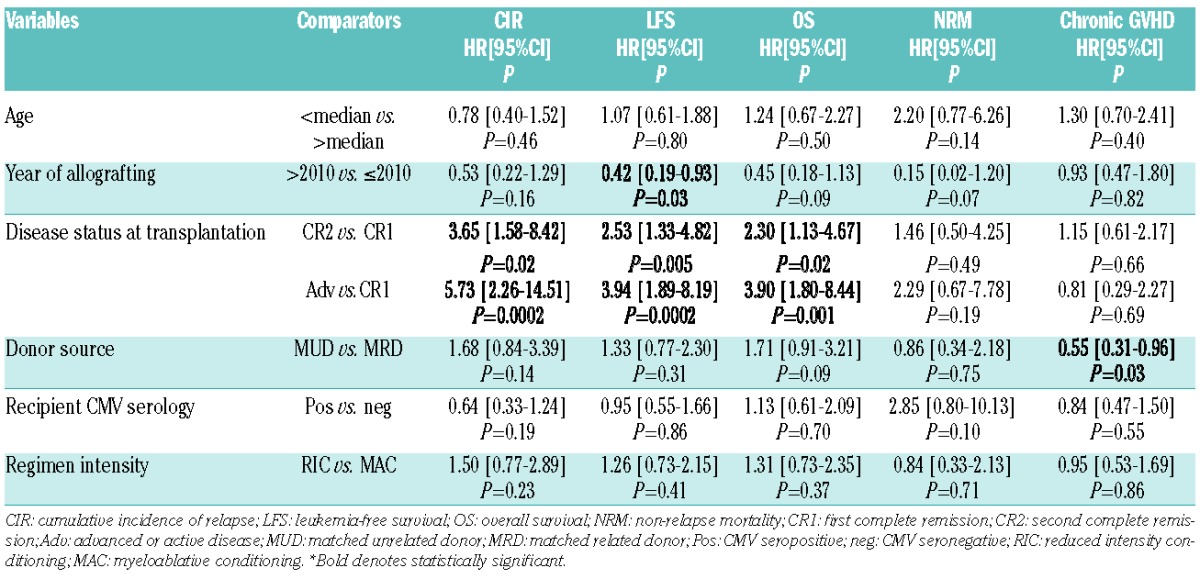
In univariate analysis, the presence of advanced/active disease at the time of allografting was associated with a higher 2-year CIR [advanced disease=48% (95%CI=26–67%), CR1=14% (95%CI=7–23%), CR2=37% (95%CI=23–51%), P=0.0009] (Figure 1A), an inferior 2-year LFS [advanced disease =30% (95%CI=11–49%), CR1=75% (95%CI=64–86%), CR2=51% (95%CI=36–65%), P<0.0001] (Figure 1B) and an inferior 2-year OS [advanced disease=39% (95%CI=19–59%), CR1=81% (95%CI=72–91%), CR2=67% (95%CI=54–80%), P<0.0001] (Figure 1C). Patients older than 54.3 years had an inferior 2-year OS [61% (95%CI=49–72%) vs. 78% (95%CI=68–88%), P=0.02]. The use of in vivo T-cell depletion has no impact on CIR, OS, LFS and NRM. In multivariable analysis, using a Cox proportional-hazards model, advanced disease or CR2 at time of transplant resulted in a higher 2-year CIR and an inferior 2-year LFS and OS (Table 2).
Figure 1.
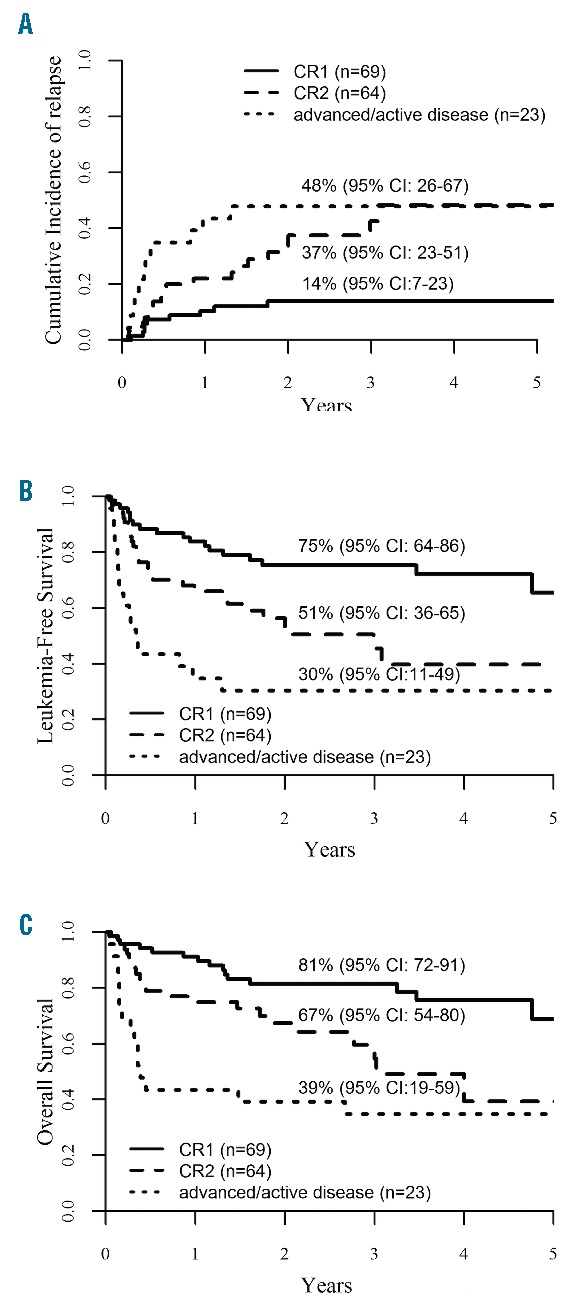
(A) Two-year cumulative incidence of relapse. (B) Two-year leukemia-free survival. (C). Two-year overall survival.
Table 2.
Multivariable analysis.
In a previous retrospective “donor” versus “no-donor” analysis of 135 AML patients with a normal karyotype and NPM1 mutation without FLT3-ITD, Schlenk et al. reported no difference in relapse-free survival between the two groups, suggesting no beneficial effect of allo-HCT in these patients.10 Conversely, using a similar strategy in a small group of FLT3- NPM1+ patients, Rollig et al. recently reported a better outcome in the donor group (N=43) in terms of 3-year relapse-free survival (83% versus 53%; P=0.004) but not in 3-year OS (81% versus 75%; P=0.3).12 Currently, AML patients with normal karyotype and NPM1 mutation without FLT3-ITD belong to the ELN favorable-risk group and, accordingly, are referred for allo-HCT upon relapse. Our results indicate a 3-year LFS close to 40% for CR2 patients, not different from that of advanced/active disease. Conversely, the 3-year LFS in CR1 patients is close to 75%, and quite similar to the 83% reported by Rollig et al.12 The good outcome of allo-HCT in CR1 in contrast to that in CR2 and the recent reduction in NRM, together with the relatively high rate of relapse with only consolidation chemotherapy in CR1, may suggest revisiting the role of allogeneic transplant in some of the young AML patients with normal karyotype and NPM1 mutation, even without FLT3-ITD, in CR1,12 for example in those patients who are slow in achieving remission or have high MRD.
One of the important limitations of our retrospective registry study is the risk of selection bias. Ideally, this question ought to be answered through a prospective randomized trial comparing allo-HCT against consolidation chemotherapy in AML patients with normal diploid karyotype, NPM1 mutation, no FLT3-ITD, and with an available matched donor. This would, however, require large international cooperation to achieve the required sample size.
In conclusion, AML disease status at allografting remains the most important predictor of post-allogeneic HCT outcomes despite expression of mutated NPM1. Survival outcomes are better when patients are transplanted in CR1 versus CR2 or advanced/active disease. Although judged to be good-risk patients and not considered for allogeneic HCT, CR1 patients with NPM1+ FLT3- are still faced with significant risk of relapse. Delaying transplant to CR2 leads to around 50% survival. The impact of other molecular abnormalities in conjunction with NPM1 is yet to be established.
Footnotes
Funding: FM was supported by educational grants from the “Association for Training, Education and Research in Hematology, Immunology and Transplantation” (ATERHIT, Nantes, France). Michal Karas is supported by Ministry of Health, Czech Republic - conceptual development of research organization (Faculty Hospital in Pilsen - FNPl, 00669806).
Information on authorship, contributions, and financial & other disclosures was provided by the authors and is available with the online version of this article at www.haematologica.org.
References
- 1.Ferrara F, Schiffer CA. Acute myeloid leukaemia in adults. Lancet. 2013;381(9865):484–495. [DOI] [PubMed] [Google Scholar]
- 2.Lowenberg B, Downing JR, Burnett A. Acute myeloid leukemia. N Engl J Med. 1999;341(14):1051–1062. [DOI] [PubMed] [Google Scholar]
- 3.Grimwade D, Hills RK, Moorman AV, et al. Refinement of cytogenetic classification in acute myeloid leukemia: determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood. 2010;116(3):354–365. [DOI] [PubMed] [Google Scholar]
- 4.Frohling S, Schlenk RF, Breitruck J, et al. Prognostic significance of activating FLT3 mutations in younger adults (16 to 60 years) with acute myeloid leukemia and normal cytogenetics: a study of the AML Study Group Ulm. Blood. 2002;100(13):4372–4380. [DOI] [PubMed] [Google Scholar]
- 5.Patel JP, Gonen M, Figueroa ME, et al. Prognostic relevance of integrated genetic profiling in acute myeloid leukemia. N Engl J Med. 2012;366(12):1079–1089. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ostronoff F, Othus M, Lazenby M, et al. Prognostic significance of NPM1 mutations in the absence of FLT3-internal tandem duplication in older patients with acute myeloid leukemia: a SWOG and UK National Cancer Research Institute/Medical Research Council report. J Clin Oncol. 2015;33(10):1157–1164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Falini B, Martelli MP, Bolli N, et al. Acute myeloid leukemia with mutated nucleophosmin (NPM1): is it a distinct entity? Blood 2011;117(4):1109–1120. [DOI] [PubMed] [Google Scholar]
- 8.Verhaak RG, Goudswaard CS, van Putten W, et al. Mutations in nucleophosmin (NPM1) in acute myeloid leukemia (AML): association with other gene abnormalities and previously established gene expression signatures and their favorable prognostic significance. Blood. 2005;106(12):3747–3754. [DOI] [PubMed] [Google Scholar]
- 9.Schnittger S, Schoch C, Kern W, et al. Nucleophosmin gene mutations are predictors of favorable prognosis in acute myelogenous leukemia with a normal karyotype. Blood. 2005;106(12):3733–3739. [DOI] [PubMed] [Google Scholar]
- 10.Schlenk RF, Dohner K, Krauter J, et al. Mutations and treatment outcome in cytogenetically normal acute myeloid leukemia. N Engl J Med. 2008;358(18):1909–1918. [DOI] [PubMed] [Google Scholar]
- 11.Kienast J, Beelen DW, Kolb HJ, et al. Allogeneic Hematopoietic Stem Cell Transplantation (Allo-SCT) Versus Conventional Postremission Therapy (PRT) for AML in First Complete Remission (CR1): A Matched Pairs Analysis Based on Data of the AML Cooperative Group (AMLCG) 1999 Trial. Blood. 2007;110(11):328 abstr. [Google Scholar]
- 12.Rollig C, Bornhauser M, Kramer M, et al. Allogeneic stem-cell transplantation in patients with NPM1-mutated acute myeloid leukemia: results from a prospective donor versus no-donor analysis of patients after upfront HLA typing within the SAL-AML 2003 trial. J Clin Oncol. 2015;33(5):403–410. [DOI] [PubMed] [Google Scholar]