

Abstract
Individuals with unilateral hearing loss of severe-profound degree face listening difficulties while localizing a sound source and while perceiving speech in the presence of noise. The objective was to compare the efficacy of the digitally programmable bone anchored hearing aid (BAHA), trimmer digital BAHA and the transcranial contralateral routing of signal (T-CROS) in improving the listening performance in adults with unilateral hearing loss. Twenty-four adults with unilateral hearing loss was assessed for sound field thresholds, speech perception performance in quiet and noise (direct and indirect conditions) and the subjective quality rating of speech in unaided and aided with either T-CROS or digitally programmable BAHA or trimmer digital BAHA attached to the headband. Results indicated that the participants performed better with both the digitally programmable and the trimmer digital BAHA than the T-CROS in both quiet and noise. However, the digitally programmable BAHA performed better when the speech arrived from the poorer ear side. The current study helps in prioritizing the hearing amplification devices for the trial and also helps in arriving at the appropriate hearing amplification device for the individuals with unilateral hearing loss.
Key words: Speech in noise, direct and indirect condition, speech perception
Introduction
Individuals with unilateral hearing loss of severe-profound degree with normal or near normal hearing sensitivity in the better ear, exhibit good listening performance in quiet environments without remarkable effort. However, difficulty arises while localizing a sound source when the signal arrives from the direction of the poorer ear1,2 and while perceiving the speech information in the presence of background noise.3 Previously, unilateral hearing loss was thought to have negligible deleterious impact on the daily listening circumstances and in consequence, required minimal or no intervention. However, currently, more and more individuals with unilateral severe to profound hearing loss are bringing in reports of faced difficulties in daily life listening situations, in turn compelling the professionals to look for a satisfactory rehabilitative approach. In fact, 86% of the individuals with unilateral hearing loss do consider the hearing loss to be a hindrance to social interaction.4,5 Adults are unable to communicate appropriately in various circumstances, such as listening at office, public places, meetings, social gatherings, etc. This affects their emotional, psychological and social aspects. Hence, this calls for a need to examine the available rehabilitation approaches for individuals with unilateral hearing loss and arrive at the best. One way of approaching the problem is by counseling the individual about the compensatory strategies to be used for better communication in adverse listening conditions. Despite the fact that this approach may not work out in all the situations, strategies such as preferential seating, utilizing speech reading cues and facing the better ear towards the signal will provide at least some benefit at times.1 Rehabilitation through hearing devices is another way of combating the difficulties faced by the individuals with unilateral hearing loss. Wearing a hearing aid in the poorer ear with usable residual hearing will certainly be beneficial enough to consider amplification in daily listening environments.6 However, for those without usable residual hearing in the poorer ear, contralateral routing of signal (CROS) hearing aid comes as a useful tool. Wireless conventional CROS has been compared with the behind the ear transcranial CROS in eight adults with unilateral hearing loss.7 The transcranial CROS (T-CROS) fitting was verified by means of the transcranial threshold (TCT) and real-ear aided response (REAR) measurement. The participants who went for the transcranial CROS had lower TCT values. The conventional CROS was compared with the bone anchored hearing aid (BAHA) in ten adults with the unilateral hearing loss.8 After one month of trial with each of the devices, localization in noise, subjective assessment, and speech recognition in quiet and noise were carried out. Localization test results revealed poorer scores in both the devices as well as the unaided condition. Participants preferred the BAHA to the conventional CROS, which was also indicated by the improved speech recognition scores with the BAHA in both quiet and noise. Further, ten adult participants having unilateral hearing loss underwent localization, speech perception performance in noise test and the subjective quality rating with the aid of three questionnaires with the conventional CROS, transcranial CROS and the BAHA.9 Chance level localization was observed in both the aided and unaided conditions, better speech perception in noise with the conventional CROS followed by BAHA; however, subjectively, only one participant chose the conventional CROS and three picked up the BAHA. The review indicates a mismatch between the subjective preference and the functional performance of the individuals with the rehabilitation devices and the studies lack uniformity in terms of the results obtained. Hence, there still exists a lack of consensus on the most appropriate device for the individuals with unilateral hearing loss. Additionally, the number of participants considered in the previously conducted research on unilateral hearing loss rehabilitation is not sufficient enough to generalize the results to the complete population of those with unilateral hearing loss. Furthermore, as the technology evolves, there are more and more new and developed devices, which will be available for the individuals with unilateral hearing loss. A thorough understanding of their usefulness to the target population and their stand among other similar technological innovations is vital for audiologists to prescribe the best device suitable for a particular individual. There is a dearth of such studies, which compare the latest hearing amplification options for the individuals with unilateral hearing loss. Hence, the present study was taken up with a null hypothesis that there would be no effect of the amplification devices on the auditory performance of the participants. The study aimed to determine whether technological advancements in digital signal processing have truly enhanced the efficacy of CROS and BAHA devices and to identify any shortcomings that may have remained.
Aim
The present study specifically aimed at comparing the efficacy of the digitally programmable BAHA, trimmer digital BAHA and the transcranial CROS in improving the listening performance in adults with unilateral hearing loss.
Materials and Methods
Participants
The participants comprised of 24 adults (17 to 56 years, mean age=34 years, 16 males and 8 females) having unilateral hearing loss with either severe mixed or sensorineural hearing loss or profound hearing loss in the poorer ear and normal or near normal hearing sensitivity (pure-tone audiometry <25 dBHL) in the better ear. All the participants were native speakers of Kannada language with adequate speech and language skills and none of them had a prior experience with hearing amplification. Audiological testing as well as the recording of the test stimulus was conducted in an acoustically treated room with noise levels within permissible limits.10 All the testing procedures in the present study were noninvasive and were approved by the institutional review board (All India Institute of Speech & Hearing). An informed consent was taken from all the participants prior to the commencement of the testing.
Optimizing the amplification devices for each participant
Transcranial contralateral routing of signal
The poorer ear of each participant was aided with air conduction digitally programmable behind-the-ear hearing aid attached to a custom-made silicone shell earmold. NAL-NL1 prescriptive formula was used for the participants. The hearing aid settings were programmed to get the maximum output and a feedback test was run if there was any trace of feedback. The acoustic head shadow effect is frequency dependent with attenuation greater at higher frequencies starting from approximately 1.5 kHz and less prominent at lower frequencies below approximately 1 kHz.11-13 As a consequence, for individuals with SSD, sounds below approximately 1.5 kHz reach the better ear without significant attenuation with a sound source placed at the side of the poorer ear. Whereas, the high frequency sounds from the same source suffer a considerable attenuation by reason of the acoustic head shadow effect. Hence, low-frequency attenuation was incorporated into the study cutting down the gain for frequencies below 0.75 kHz in the hearing aid. The directionality of the hearing aid microphone was set to omnidirectional and noise reduction was switched off to keep the features uniform across all the devices used in the study since BAHA 2 with soft band is devoid of directionality and feedback reduction. Subsequent to the programming of T-CROS, a verification process by measuring TCTs and REAR was carried out to check whether the gain was sufficient enough to cross over and be available for the better ear.
Measurement of transcranial thresholds
The participant was instructed to have his/her head steady while testing with T-CROS. The probe microphone from a real ear analyzer (Fonix 7000; Frye Electronics, Tigard, OR, USA) was equalized. The probe tube was placed in the ear canal of the poorer ear along with the custom soft earmold at a predetermined length of 5 mm from the tip of the ear canal portion of the earmold. An insert earphone (ER-3A; Etymotic Research, Grove Village, IL, USA) connected to a calibrated audiometer (Maico MA-52; Maico, Berlin, Germany) was coupled to the tubing of the soft earmold using an adapter. Pure tones were presented at 0.5, 1, 1.5, 2, 3 and 4 kHz and unmasked air conduction thresholds were obtained. At the obtained threshold level, the signal was presented continuously with the Fonix 7000 (Frye Electronics) analyzer set to calibrate probe microphone and the sound pressure level (SPL) in the ear canal was read from the monitor of the analyzer. These SPL values represent the TCTs and function as baseline for assessing if the measured REARs for input levels of 50, 70, and 80 dB SPL overreach the TCTs.7
Measurement of real ear aided response
The sound field was equalized. The TCTs were fed in as hearing threshold levels in the target screen. NAL-NL1 prescriptive formula was chosen. As a consequence, target gain was obtained at different frequencies on the real ear SPL screen. The REAR procedure was subsequently executed for input levels of 50, 70, and 80 dB SPL with Digi speech as the signal. For this, the loudspeaker was placed at a distance of one foot from the surface of the head and at ear level of the participant. The probe tube was placed in the ear canal of the poorer ear along with the custom soft earmold at a predetermined length of 5 mm from the tip of the ear canal portion of the earmold. The hearing aid was coupled to the tubing of the soft earmold.
Bone anchored hearing aid 1
The digitally programmable BAHA was programmed based on the participant’s better ear thresholds and their listening needs, according to the device’s company’s prescription for bone conduction. As mentioned previously, sounds with frequency content lower than 1.5 kHz cross over to the opposite ear without noteworthy attenuation due to the frequency specific acoustic head shadow effect. Also, BAHAs tend to induce more distortion at lower frequencies hence, low frequency attenuation of up to 1.5 kHz in the BAHA sound processor will not undermine the advantages provided by BAHA in individuals with unilateral hearing loss in presence of noise coming from the front but in turn reduces the detrimental effects of noise arriving from the BAHA side.14 This reduction in the adverse effects of noise on speech perception was seen to increase with the low-frequency cut off values. Therefore, low-frequency attenuation was implemented with cut-off frequency of 0.75 kHz. The microphone was set to omnidirectional mode, noise reduction was switched off and feedback reduction was kept to default. Position compensation feature was turned on. The BAHA was coupled to the headband and placed on the poorer ear mastoid while testing.
Bone anchored hearing aid 2
The settings on the BAHA 2 were optimized based on the identification of the Ling’s six sounds for each participant. The trimmer controls were set to attenuate frequencies below 0.75 kHz.
Assessing the usefulness of the devices
Sound field warble tone thresholds
Warble tones were presented at frequencies 0.5, 1, 2 and 4k Hz through the loudspeaker placed at 45°, towards the side of the test ear and at one meter distance from the participant. Instructions were given to the participant to indicate whenever he heard a tone, no matter how soft it was. The lowest intensity at which the participant responded positively 50% of the time was taken as the threshold. This procedure was conducted in unaided and three aided conditions. Aided conditions included testing with TCROS, with BAHA 1 and BAHA 2. The better ear of the participant was blocked by a combination of ear plug and ear muffs (noise reduction rating=39 dB approx.) both in aided and unaided conditions.15 Blocking the better ear was chosen over masking by noise since noise would adversely affect the performance of the better ear for transcranial conduction, in turn reducing the efficiency of the amplification devices. The order of aided conditions was randomized among the participants to hinder the order effect. Consequently, four sets of warble tone thresholds were acquired for each participant.
Speech identification score in quiet
The speech identification score (SIS) was obtained using PB word list consisting of 25 words in Kannada16 for adults. The loudspeaker was located at 45°, towards the side of the test ear and at one meter distance from the participant. The participation of the better ear was excluded by blocking it with the help of earplug and earmuffs. The list was presented at 40 dB HL at a distance of 6-7 inches from the microphone of the audiometer and the participant was instructed to repeat the words comprehended. The total number of correctly repeated words was noted to calculate the SIS. This was repeated for each of the aided conditions and in unaided condition.
Signal to noise ratio-50 in direct and indirect conditions
Signal to noise ratio-50 (SNR-50) is defined as the difference between the intensity of the live speech material and the intensity of the speech noise in dB when the participant repeats back at least two words in a set of three, presented along with competing speech noise. The SNR-50 was obtained in two conditions for each of the aided conditions and in unaided condition. In the direct condition, signal was presented towards the better ear and noise towards the poorer ear, whereas, in the indirect condition, signal was presented towards the poorer ear and noise towards the better ear. During the testing, the participant was asked to sit comfortably on a chair at one-meter distance from the loudspeaker. A list of 40 sets of Kannada bi-syllabic words17 was used to find out the SNR-50. The speech material was presented at a constant intensity of 40 dB HL. The speech noise was started at intensity 15 dB lower than the signal and manipulated systematically in one dB steps. The patient was asked to repeat the words understood. At each level of noise, a set of three words was presented to the participant. The level of noise was increased by one dB if the participant restated at least two out of three words correctly. If they failed to repeat at least two of the three words, then the level of noise was dropped by two dB. This procedure was carried on till the highest level of speech noise was reached in the presence of which the participant could repeat at least two out of the three words correctly. The difference between the signal and noise at this juncture was taken as the SNR-50.
Subjective quality rating
The five-point rating scale was used for the subjective evaluation of the devices.18 The scale had five parameters on which the devices were to be evaluated. They were loudness, fullness, clarity, naturalness and overall fidelity. Participants had to assign numbers towards each parameter from 1 to 5 where in 1 was worst and 5 was best. The stimulus used for the subjective quality rating was a recorded Kannada passage19 which was directed through the auxiliary input of the audiometer to the loudspeaker placed at one meter distance from the participant at the side of the test ear. The passage was presented at 65 dB SPL.
Results and Discussion
Functional measures
The mean and standard deviation values for each of the measures obtained in both the groups in each of the conditions have been calculated and tabulated in Table 1.
Table 1.
Mean and standard deviation values for the sound field thresholds, speech identification scores and signal to noise ratio-50 scores obtained in unaided and three aided conditions.
| Condition | Sound field thresholds (dB) (mean, SD) | SIS (max=25) (mean, SD) | SNR-50 (mean, SD) | ||||
|---|---|---|---|---|---|---|---|
| 500 Hz | 1000 Hz | 2000 Hz | 4000 Hz | D | ID | ||
| Unaided | 53.12 | 51.87 | 51.46 | 64.37 | 0.00 | –5.67 | 3.12 |
| (10.61) | (7.34) | (11.56) | (10.03) | (6.80) | (6.01) | ||
| BAHA 1 | 15.42 | 20.21 | 19.37 | 30.21 | 23.08 | –4.87 | 1.17 |
| (9.43) | (11.08) | (11.64) | (14.70) | (2.28) | (6.40) | (5.48) | |
| BAHA 2 | 17.29 | 17.92 | 26.25 | 49.17 | 22.46 | –6.37 | 2.33 |
| (9.89) | (12.42) | (13.53) | (16.26) | (3.20) | (5.39) | (6.25) | |
| T-CROS | 38.33 | 20.42 | 22.71 | 43.96 | 18.29 | –6.37 | 3.04 |
| (9.40) | (10.62) | (10.93) | (19.72) | (4.51) | (5.45) | (6.15) | |
SIS, speech identification scores; SNR-50, signal to noise ratio-50; SD, standard deviation; D, direct condition; ID, indirect condition; BAHA, bone anchored hearing aid; T-CROS, transcranial contralateral routing of offside signal.
The mean data for the sound field thresholds show that the aided thresholds were considerably better than the unaided. The thresholds were lowest for the BAHA 1 as compared to other devices and that the thresholds were slightly better at the lower frequencies for all the devices. The SIS in the quiet condition improved from the unaided condition to the aided and BAHA 1 obtained higher scores compared to other devices. Better performance on the SNR-50 test would yield lower SNR scores. The direct SNR-50 values were seen to be lower than indirect and the T-CROS hearing aid seemed to interfere less with the speech perception and hence had better SNR than the other devices. No observable differences were seen across the devices in terms of the indirect SNR-50 values.
The data showed vast variability indicating the group lacked homogeneity, hence non-parametric statistics were considered for the analysis. Freidman test was applied on the sound field thresholds, SIS obtained in the quiet condition and the SNR-50 values to find out whether the hearing devices were significantly different from each other. Further, Wilcoxon’s signed rank test was utilized for the pair wise comparison wherever significance was indicated by the Friedman test.
The sound field thresholds, SIS measured in quiet condition and the SNR-50 values obtained in direct and indirect conditions were analyzed using Freidman test and the results have been tabulated in Table 2, which indicates that listening conditions were significantly different (P<0.05) from each other as measured in terms of sound field thresholds, SIS obtained in quiet condition and SNR-50 indirect. However, it can be seen that the listening conditions did not differ significantly in terms of SNR-50 direct measure. This shows that the aided condition was not significantly different from the unaided condition and neither of the devices had any adverse effects on the speech perception as evident in Table 1. However, this result is in contradiction to that reported by Niparko et al.8 who measured speech perception in noise using hearing in noise test in ten adults with unilateral hearing loss. They compared the speech perception performance in the presence of noise in unaided and while the individuals were aided with the conventional CROS and the BAHA. They reported that in the direct condition, there was significant difference between the unaided and both the aided conditions and that BAHA performed better than the conventional CROS. The significance of difference seen in the SNR-50 indirect condition shows that the aided condition was significantly different from the unaided, and from the Table 1, it can be inferred that the aids were beneficial to the individuals with unilateral hearing loss. Further, Wilcoxon’s signed rank test was applied wherever significant differences were obtained across the listening conditions. The results of the Wilcoxon’s signed rank test for the sound field thresholds have been displayed in the Table 3. From the Table 3, it can be deduced that the unaided sound field thresholds are significantly different from those of aided condition for all the frequencies, aided scores being better. However, the results vary across frequencies for the aided condition. It was observed that at 500 Hz, both the BAHA devices performed better than the T-CROS device. At 1000 and 2000 Hz, all the devices performed more or less to the same extent and at 4000 Hz BAHA 1 scored better than the BAHA 2 and T-CROS. The results of the Wilcoxon’s signed rank test for the SIS obtained in the quiet condition and for the SNR-50 obtained in the indirect condition are as displayed in the Table 4.
Table 2.
Comparison of the unaided and aided conditions on the basis of sound field thresholds, speech identification scores and signal to noise ratio-50 values.
| Sample no. | Measures | X2 (df) | P |
|---|---|---|---|
| 1 | 500 Hz | 65.48(3) | 0.000 |
| 2 | 1000 Hz | 47.88(3) | 0.000 |
| 3 | 2000 Hz | 49.14(3) | 0.000 |
| 4 | 4000 Hz | 53.62(3) | 0.000 |
| 5 | SIS | 57.08(3) | 0.000 |
| 6 | SNR-50 direct | 6.28(3) | 0.090 |
| 7 | SNR-50 indirect | 10.89(3) | 0.010 |
df, degree of freedom; SIS, speech identification scores; SNR-50, signal to noise ratio-50.
Table 3.
Pairwise-comparison of the unaided and aided conditions for sound field thresholds.
| Measure | Condition | Unaided | BAHA 1 | BAHA 2 | T-CROS |
|---|---|---|---|---|---|
| 500 Hz | Unaided | - | * | * | * |
| BAHA 1 | * | - | ** | * | |
| BAHA 2 | * | ** | - | * | |
| T-CROS | * | * | * | - | |
| 1000 Hz | Unaided | - | * | * | * |
| BAHA 1 | * | - | ** | ** | |
| BAHA 2 | * | ** | - | ** | |
| T-CROS | * | ** | ** | - | |
| 2000 Hz | Unaided | - | * | * | * |
| BAHA 1 | * | - | * | ** | |
| BAHA 2 | * | * | - | ** | |
| T-CROS | * | ** | ** | - | |
| 4000 Hz | Unaided | - | * | * | * |
| BAHA 1 | * | - | * | * | |
| BAHA 2 | * | * | - | ** | |
| T-CROS | * | * | ** | - |
BAHA, bone anchored hearing aid; T-CROS, transcranial contralateral routing of offside signal.
*Significantly different (P<0.05)
**not significantly different (P>0.05).
Table 4.
Pairwise-comparison of the unaided and aided conditions for speech identification scores and signal to noise ratio-50 indirect values.
| Measure | Condition | Unaided | BAHA 1 | BAHA 2 | T-CROS |
|---|---|---|---|---|---|
| SIS | Unaided | - | * | * | * |
| BAHA 1 | * | - | ** | * | |
| BAHA 2 | * | ** | - | * | |
| T-CROS | * | * | * | - | |
| SNR-50 indirect | Unaided | - | * | ** | ** |
| BAHA 1 | * | - | * | * | |
| BAHA 2 | ** | * | - | ** | |
| T-CROS | ** | * | ** | - |
BAHA, bone anchored hearing aid; T-CROS, transcranial contralateral routing of offside signal; SIS, speech identification scores; SNR-50, signal to noise ratio-50.
*Significantly different (P<0.05)
**not significantly different (P>0.05).
Table 4 depicts that the unaided SIS scores were significantly different from the aided scores. On comparison of the unaided condition and the T-CROS aided condition, it is seen in Table 1 that the T-CROS was beneficial for the participants in quiet condition when the better ear was blocked with earplugs and earmuffs. This is not in agreement with Niparko et al.8 who reported that the participants scored higher in the unaided condition when compared to the conventional CROS aided condition. This discrepancy must be due to the methodological differences between the studies, where they have measured speech perception in quiet condition without blocking the better ear. It was also seen that the BAHA was beneficial for speech perception in quiet condition for the participants of the present study when compared to the unaided condition as reported earlier.8
It is also evident from Table 4 that the SIS measured in quiet with both the BAHA devices were significantly different than those with the T-CROS hearing aid, with no difference between BAHA 1 and BAHA 2. From Table 1, both the BAHAs yielded higher scores than the T-CROS. This is in agreement with the study where they also found that the participants performed well with the BAHA when compared to the conventional CROS.8 With respect to the SNR-50 measured in indirect condition, only BAHA 1 made a significant difference from the unaided condition while BAHA 2 and CROS were similar to the unaided condition. Also, BAHA 1 differed significantly from the BAHA 2 and T-CROS, however, there was no significant difference between BAHA 2 and T-CROS. This indicates that only BAHA 1 was beneficial for the individuals with unilateral hearing loss in noisy condition. This can be speculated to be due to an additional feature named positional compensation present only in BAHA 1 when compared to BAHA 2 along with better fine tuning facility.8 reported that the unaided condition was significantly different from both the BAHA and CROS aided conditions and that the aided scores were better than the unaided scores. Similar to the current study there are reports that the participants scored higher with the BAHA when compared to the conventional CROS.1,8
Subjective quality rating
The mean and standard deviation of the ranks for each of the five parameters for each of the devices have been displayed in Figure 1. From Figure 1, it can be deduced that both the BAHAs scored higher than the T-CROS and that there was no noticeable difference across the parameters (P<0.05).
Figure 1.
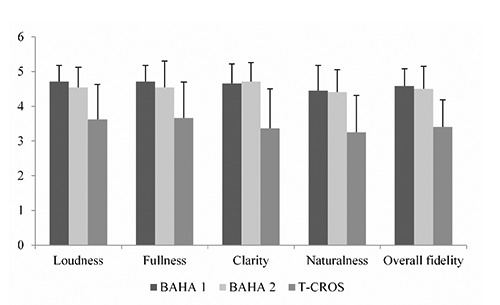
Mean and standard deviation of the ranks across the devices for each of the parameters of the subjective rating scale. BAHA, bone anchored hearing aid; T-CROS: transcranial-contralateral routing of offside signal.
Freidman test was administered to find out whether any significant difference existed across the hearing devices in terms of the quality perceived by the participants. It was observed that the hearing devices were significantly different (P<0.05) from each other in terms of their perceived sound quality. Consequently, Wilcoxon’s signed rank test was applied wherever significant differences were observed across the hearing devices. The results of all the parameters have been presented in the Table 5.
Table 5.
Pairwise comparison of the aided conditions for all the parameters of subjective quality rating.
| Sample no. | Parameter | Condition | BAHA 1 | BAHA 2 | T-CROS |
|---|---|---|---|---|---|
| 1 | Loudness | BAHA 1 | - | ** | * |
| BAHA 2 | ** | - | * | ||
| T-CROS | * | * | - | ||
| 2 | Fullness | BAHA 1 | - | ** | * |
| BAHA 2 | ** | - | * | ||
| T-CROS | * | * | - | ||
| 3 | Clarity | BAHA 1 | - | ** | * |
| BAHA 2 | ** | - | * | ||
| T-CROS | * | * | - | ||
| 4 | Naturalness | BAHA 1 | - | ** | * |
| BAHA 2 | ** | - | * | ||
| T-CROS | * | * | - | ||
| 5 | Overall fidelity | BAHA 1 | - | ** | * |
| BAHA 2 | ** | - | * | ||
| T-CROS | * | * | - |
BAHA, bone anchored hearing aid; T-CROS, transcranial contralateral routing of offside signal.
*Significantly different (P<0.05)
**not significantly different (P>0.05).
It is evident from Table 5, that the subjective quality in terms of all the parameters of both the BAHA 1 and BAHA 2 did not differ significantly, however a difference was observed between the two BAHAs and the T-CROS. It was also seen that the BAHAs obtained a higher quality rating than the T-CROS. The same was reported by several authors,1,3 who compared the performance of conventional CROS and BAHA in individuals with unilateral hearing loss using the abbreviated profile of hearing aid benefit.
Correlation between the functional and subjective measures
From the previous section it is understood that the BAHA 1 did not significantly differ from BAHA 2 in terms of the subjective quality rating. Additionally, both BAHA 1 and BAHA 2 were not significantly different from each other in terms of the SIS measured in quiet as shown in Table 4. Therefore, only BAHA 1 and T-CROS were subjected to correlational analysis, omitting BAHA 2, since results of BAHA 1 would apply to BAHA 2 as well. Furthermore, it was noted previously that the hearing devices differed among themselves in a similar fashion for all the parameters. Hence, only the overall fidelity parameter was considered for correlational analysis and the result was generalized across the other parameters of the rating scale. The correlation between the aided SIS obtained in the quiet condition with the BAHA 1 and the T-CROS and the overall fidelity parameter in the subjective quality rating was checked using Spearman’s correlation. The results showed no significant correlation between the two measures with both BAHA 1 and TCROS. However, this can be speculated to be due to the reduced range of both the SIS and the subjective quality rating with the BAHA 1 and also with the T-CROS as depicted in Figure 2.
Figure 2.
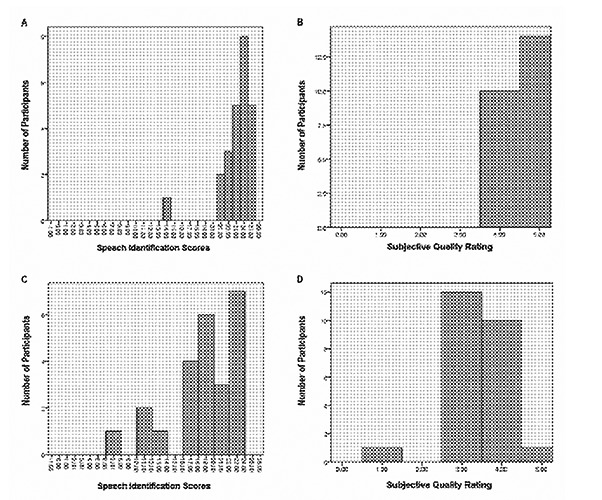
A) Depiction of the range of speech identification scores (SIS) across number of participants with the programmable digital bone anchored hearing aid (BAHA) 1; B) Depiction of the range of subjective quality rating across number of participants with the BAHA 1; C) Depiction of the range of SIS across number of participants with the transcranial contralateral routing of offside signal (T-CROS). D) Depiction of the range of subjective quality rating across number of participants with the T-CROS.
As can be seen in Figure 2A and C, the speech identification scores measured in quiet in the aided condition were all clustered towards the higher end. Similarly in Figure 2B and D, the overall fidelity parameter in the subjective quality rating, reveals that the ratings were cornered towards the higher scores. Hence, due to the reduced range of the variables, the results of the correlation analysis can be considered to be less reliable.
Conclusions
Both BAHA attached to the headband and the T-CROS provide significant benefit for individuals with unilateral hearing loss. However, the participants performed better with the BAHA than the T-CROS in both quiet and noise for most of the measures, with both the digitally programmable and the trimmer digital BAHA performing more or less to the same extent. Furthermore, BAHA can be expected to provide greater improvements after implantation20 that implanted BAHA yields 5 to 20 dB better thresholds compared to pre-implant BAHA. In terms of speech perception, this post implant increment can lead to a bettering of the speech reception threshold by up to 4 to 7 dB, which in turn improves the SIS by about 20 to 40%.
Clinical implications
The current study helps in prioritizing the hearing amplification devices for the trial and also helps in arriving at the appropriate hearing amplification device for the individuals with unilateral hearing loss. The present study provides a comparison of the digitally programmable BAHA, the trimmer digital BAHA and the T-CROS, which will help in the counseling of the individuals with unilateral hearing concerning the available rehabilitation options and their comparative performance. The current study confirms that there are rehabilitation options for the individuals with unilateral hearing loss, which prove to be beneficial, compared to the performance without amplification. The results of the current study show that both the T-CROS and BAHA provided significant benefit when compared to the unaided condition with BAHA being better than T-CROS. From this, it can be deduced that, if the individuals with unilateral hearing loss cannot afford the higher cost of the BAHA, they can opt the T-CROS, which is also beneficial to some extent.
Acknowledgements
The authors would like to thank the Director, All India Institute of Speech and Hearing for granting the funds for the study and the participants for their cooperation.
Funding Statement
Funding: this data is a part of a project funded by the AIISH Research Fund.
References
- 1.Wazen JJ, Ghossaini SN, Spitzer JB, Kuller M. Localization by unilateral BAHA users. Otolaryngol Head Neck Surg 2005;132:928-32. [DOI] [PubMed] [Google Scholar]
- 2.Hol MK, Bosman AJ, Snik AF, Mylanus EA, Cremers CW. Bone anchored hearing aid in unilateral inner ear deafness: a study of 20 patients. Audiol Neurootol 2004;9:274-81. [DOI] [PubMed] [Google Scholar]
- 3.Bosman AJ, Hol MK, Snik AF, Mylanus EA, Cremers CW. Bone anchored hearing aids in unilateral inner ear deafness. Acta Otolaryngol 2003;123:258-60. [DOI] [PubMed] [Google Scholar]
- 4.Chiossoine-Kerdel JA, Baguley DM, Stoddart RL, Moffat DA. An investigation of the audiologic handicap associated with unilateral sudden sensorineural hearing loss. Am J Oto 2000;21:645-51. [PubMed] [Google Scholar]
- 5.McDermott AL, Dutt SN, Tziambazis E, Reid A P, Proops DW. Disability, handicap and benefit analysis with the bone-anchored hearing aid: the Glasgow hearing aid benefit and difference profiles. J Laryngol Otol Suppl 2002;116:29-36. [DOI] [PubMed] [Google Scholar]
- 6.Harford E, Musket C. Binaural hearing with one hearing aid. J Speech Hear Dis 1964;29:133-46. [DOI] [PubMed] [Google Scholar]
- 7.Valente M, Potts LG, Valente M, Goebel J. Wireless CROS versus transcranial CROS for unilateral hearing loss. Am J Audiol 1995;4:52-9.26649844 [Google Scholar]
- 8.Niparko JK, Cox KM, Lustig LR. Comparison of the bone anchored hearing aid implantable hearing device with contralateral routing of offside signal amplification in the rehabilitation of unilateral deafness. Otol Neurotol 2003;24:73-8. [DOI] [PubMed] [Google Scholar]
- 9.Hol MKS, Kunst SJW, Snik AFM, Cremers CW. Pilot study on the effectiveness of the conventional CROS, the transcranial CROS and the BAHA transcranial CROS in adults with unilateral inner ear deafness. Eur Arch Otorhinolaryngol 2010;267:889-96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.American National Standards Institute. Maximum permissible ambient noise levels for audiometric test rooms (ANSI S3.1.1991). New York: ANSI; 1991. [Google Scholar]
- 11.Shaw EAG. Transformation of sound pressure from the free field to the ear drum in the horizontal plane. J Acoust Soc Am 1974;56:1 848-61. [DOI] [PubMed] [Google Scholar]
- 12.Kompis M, Dillier N. Simulation transfer functions in a reverberant room including source directivity and head shadow effect. J Acoust Soc Am 1993;93:2779-87. [Google Scholar]
- 13.Algazi VR, Duda RO, Duralswami R, Gumerov NA, Tang Z. Approximating the head-related transfer function using simple geometric models of the head and torso J Acoust Soc Am 2002;112:2053-64. [DOI] [PubMed] [Google Scholar]
- 14.Pfiffner F, Kompis M, Flynn M, Asnes K, Arnold A, Stieger C. Benefits of low-frequency attenuation of BAHA in single-sided sen-sorineural deafness. Ear Hear 2010;32:40-5. [DOI] [PubMed] [Google Scholar]
- 15.Wazen JJ, Spitzer JB, Ghossani SN, Kacker A, Zschommler A. Results of the bone-anchored hearing aid in unilateral hearing loss. Laryngoscope 2001;111:955-8. [DOI] [PubMed] [Google Scholar]
- 16.Yathiraj A, Vijayalakshmi CS. Phonemically balanced word list in Kannada. Mysore: Department of Audiology, AIISH; 2005. [Google Scholar]
- 17.Sahgal A, Manjula P. A comparative study of proprietary and generic prescriptive procedures for nonlinear hearing aids. Master’s Degree Diss. University of Mysore; 2005. [Google Scholar]
- 18.Eisenberg LS, Dirks DD. Reliability and sensitivity of paired comparisons and category rating in children. J Speech Hear Res 1995;38:1157-67. [DOI] [PubMed] [Google Scholar]
- 19.Sairam VVS, Manjula P. Long term average speech spectrum in kannada. Master’s Degree Diss. University of Mysore; 2002. [Google Scholar]
- 20.Verstraeten N, Zarowski AJ, Somers T, Riff D, Offeciers EF. Comparison of the audiologic results obtained with the bone-anchored hearing aid attached to the headband, the test band, and to the “snap” abutment. Otol Neurotol 2009;30:70-5. [DOI] [PubMed] [Google Scholar]