

Abstract
This study assessed qualities of adolescent peer relationships as long-term predictors of physical health quality in adulthood. In an intensive multimethod, multireporter study of a community sample of 171 individuals assessed repeatedly from the ages of 13 to 27 years, physical health quality in adulthood was robustly predicted by independent reports of early-adolescent close-friendship quality and by a pattern of acquiescence to social norms in adolescent peer relationships. Predictions remained after accounting for numerous potential confounds, including prior health problems, concurrent body mass index, anxious and depressive symptoms, personality characteristics, adolescent-era financial adversity, and adolescent-era physical attractiveness. These findings have important implications for understanding the unique intensity of peer relationships in adolescence.
Keywords: adolescent development, health, social interaction
The puzzling intensity of the adolescent drive to connect with peers has long been recognized (Hall, 1904), with adolescents often treating peer challenges similarly to threats to physical well-being and willingly sacrificing their autonomy to fit in with peers. Peer relationships provide some of the most emotionally intense experiences in adolescents’ lives (Brown & Larson, 2009), and conformity to peer norms often occurs even when it brings significant costs to the individual (G. L. Cohen & Prinstein, 2006). The present study examined the possibility that this intense adolescent peer focus may be partly connected to long-term links of peer-relationship quality not just to social and psychological well-being but also to physical health well into adulthood.
Although no prospective, non-self-report research on adolescence has yet identified consistent links between relationships and health into adulthood, research within adulthood argues for their presence. Failure to establish supportive relationships in adulthood creates as great a risk for early mortality as well-known risk factors such as cigarette smoking or obesity (Holt-Lunstad, Smith, & Layton, 2010; House, Landis, & Umberson, 1988). Although health risks were initially thought to be mediated primarily by poor health-maintenance behavior (Umberson, 1987), more recent human and primate research suggests that anxiety and depressive symptoms may be primary mediators of the effects of relationship difficulties on health (Arthur, 2006; Friedmann et al., 2006; Grippo et al., 2007).
Social isolation appears to function in part by creating a degree of low-level but chronic stress that exerts a pathological effect over time (Kawachi & Berkman, 2001; Kawachi, Subramanian, & Kim, 2008). The human stress-reaction system can handle even severe stressors quite efficiently if they are transient, but it does not appear to have evolved to manage chronic activation well (Sapolsky, 2000). The chronic stress of social isolation has been linked to an array of negative physiological changes, from increased ambulatory blood pressure to impaired immune functioning (Cacioppo & Patrick, 2008; S. Cohen, Janicki-Deverts, & Miller, 2007). These findings raise the possibility that the quality of social relationships established in adolescence might well have long-term links to health. Supporting this notion, findings have shown that self-reported cross-sex friendship closeness in adolescence predicts reduced risk of problematic adult metabolic functioning, although only for females (Ehrlich, Hoyt, Sumner, McDade, & Adam, 2015).
Beyond the potential effects of social isolation and relationship quality, another potential adolescent-era social predictor of future health is adolescents’ conformity or nonconformity to peer norms. Perhaps surprisingly, evidence in adulthood suggests that nonconformity is actually likely to be associated with increased risks to health. Viewing the world differently than one’s social group views it has been found at times to produce increased amygdala activation associated with unpleasant emotions—a phenomenon termed “the pain of independence” (Berns et al., 2005, p. 252). Ongoing conflict with peers in adulthood can create chronic stress linked to a broad array of health difficulties (Kiecolt-Glaser et al., 2005; Nealey-Moore, Smith, Uchino, Hawkins, & Olson-Cerny, 2007; Wright & Loving, 2011).
In sharp contrast, cross-cultural research has found that an approach to social interactions that emphasizes placing the desires of one’s peers ahead of one’s own goals—much as adolescents do when they conform to peer norms—is linked to reduced life stress and may act as a form of antipathogen (Chiao & Blizinsky, 2010; Fincher, Thornhill, Murray, & Schaller, 2008). This approach—termed collectivism at the cultural level and allocentrism at the individual level (Triandis, 1989, 2000)—stands in sharp contrast to traditional Western cultural valuing of individual autonomy and of adolescent resistance to peer pressure (McElhaney, Allen, Stephenson, & Hare, 2009). Yet many adolescents follow precisely such an allocentric, peer-focused approach, often to the puzzlement and consternation of their elders (Fuligni, Eccles, Barber, & Clements, 2001). While close-friendship quality may reduce stress by indicating the likely availability of social, instrumental, or emotional support when needed, allocentrism, in contrast, may act by reducing the likelihood of conflict and threat within the broader social group.
Neither the independently assessed quality of adolescent friendships nor adolescents’ allocentric behaviors have been previously considered as predictors of long-term physical health outcomes. However, given the role of adult relationships in health outcomes and continuity in qualities of social relationships from adolescence to adulthood (Allen, Chango, & Szwedo, 2014; Chango, Allen, Szwedo, & Schad, 2014; Englund, I-Chun Kuo, Puig, & Collins, 2011), peer-relationship qualities appear to be strong candidates for predictors of long-term physical health outcomes. Findings of enduring health implications from social adversity in early childhood (Bardone et al., 1998; Fagundes & Way, 2014; Temcheff et al., 2011) further suggest the plausibility of such linkages.
Identifying long-term linkages between social relationships and health is key to fleshing out a life-span model of the link between social-relationship quality and physical health (Uchino, 2009). Factors related to adolescent social relationships might also serve as potential targets in health-promotion efforts across the life span. Finally, identifying long-term linkages to health may help explain some of the intensity of adolescents’ focus on peer relationships and peer conformity. This intense focus may even be viewed as a form of pack behavior that evolved over time because it had long-term survival value (Cacioppo & Patrick, 2008); assessing a connection to long-term health outcomes would test one key element of this perspective.
This multimethod, multireporter study examined the long-term health implications of early-adolescent peer behavior in a diverse community sample followed intensively from the ages of 13 to 27 years. We examined the following hypotheses:
Long-term physical health quality should be predicted by peer-reported adolescent close-friendship quality and adolescent allocentric behavior with peers.
Links from adolescent peer-relationship qualities to adult health should be potentially mediated by adult anxiety and depressive symptoms.
Predictions should remain even after one accounts for a broad range of potential third-variable confounds.
Method
Participants
This study was conducted using data from a larger longitudinal investigation of adolescent peer influences on adult development. The final sample of 171 participants was drawn from an initial sample of 184 individuals who had adult health-quality data and had been initially assessed at the age of 13 years (a 93% retention rate across 14 years). The final sample included 74 males and 97 females followed from ages 13 to 27. The sample was racially and ethnically as well as socioeconomically diverse and was representative of the community from which it was drawn: 99 adolescents (58%) identified themselves as Caucasian, 49 (29%) as African American, 15 (9%) as of mixed race or ethnicity, and 8 (5%) as being from other minority groups. Adolescents’ parents reported a median family income in the $40,000 to $59,999 range at the initial assessment. Adolescents were recruited from the seventh and eighth grades of a public middle school whose students are from suburban and urban populations in the Southeastern United States. Information about the study was provided in an initial mailing to parents and follow-up presentations to students at school lunches. Parents were formally recruited via telephone. Students who had already served as close-peer informants in the study were not eligible to serve as primary participants. Of students eligible for participation, 63% of adolescents and parents agreed to participate when parents were contacted. Adolescents provided informed assent before each interview session, and parents and adult participants provided informed consent. Interviews took place in private offices within a university academic building.
Participants were first assessed annually along with their close peers over a 5-year period in early and mid-adolescence—mean ages = 13.33 years (SD = 0.64), 14.25 years (SD = 0.77), 15.20 years (SD = 0.82), 16.33 years (SD = 0.88), and 17.30 years (SD = 0.87). At the age 13 through age 17 assessments, adolescents also nominated their closest same-gendered friend to be included in the study (not necessarily the same friend across ages). Close friends and their parents also provided informed consent. Close friends reported that they had known the adolescents for an average of 4.08 years (SD = 2.93) at the first wave of data collection, 4.19 years (SD = 3.07) at the second wave of data collection, 5.07 years (SD = 3.37) at the third wave, and 5.69 (SD = 3.81) at the fourth wave.
Personality traits were assessed when participants reached a mean age of 23.77 years (SD = 0.98). Health and concurrent covariate assessments were obtained annually across three waves at the ages of 25 (M = 25.67, SD = 0.96), 26 (M = 26.64, SD = 1.01), and 27 (M = 27.64, SD = 0.97).
Attrition analyses
Attrition analyses examined missing data for each type of data available at baseline. Females were more likely than males to have continued in the study and to have provided follow-up health data (99% continuation rate for females vs. 86% for males, p < .001). Other than that one difference, there were no attrition effects on any of the adolescent-era assessments, which suggests that attrition was modest overall and not likely to have distorted any of the findings reported. Gender was entered as a covariate in all analyses. To best address any potential biases due to attrition in longitudinal analyses or missing data within waves, we used full-imputation maximum-likelihood methods with analyses including all variables that were linked to future missing data (i.e., where data were not missing completely at random). Because these procedures have been found to yield the least-biased estimates when all available data are used for longitudinal analyses (vs. listwise deletion of missing data; Arbuckle, 1996), the entire original sample of 184 was utilized for these analyses. This full sample thus provided the best possible estimates of variances and covariances in measures of interest and was least likely to be biased by missing data.
Procedure
In the initial introduction and throughout all sessions, we assured all participants that their responses would be kept confidential. Participants’ data were covered under a confidentiality certificate issued by the U.S. Department of Health and Human Services, which protects information from subpoena by federal, state, and local courts. Transportation and childcare were provided if necessary. Adolescent participants, their parents, and adolescents’ peer reporters were all paid for participation.
Measures
Adult health quality was assessed annually at the ages of 25, 26, and 27 years, with results averaged across these assessments to produce a summary index of health quality in early adulthood. We used the five-item Likert-type, self-report general-health scale from the Medical Outcomes Study Short-Form Health Survey (Ware, Kosinski, Dewey, & Gandek, 2000), in which participants first answered one question about the overall state of their health: “In general, would you say your health is poor, fair, good, very good, or excellent?” This was followed by four additional statements which participants rated on a 5-point scale (i.e., definitely true, mostly true, don’t know, mostly false, definitely false). These included items such as “I tend to get sick a little easier than other people,” “I am as healthy as anybody I know,” and “My health is excellent.” Scores within each assessment were summed across the five items, which yielded scores that could range from 0 to 25. This approach has been used extensively and found not only to be strongly related to concurrent biological markers of health but also to consistently yield strong predictions about future health, including mortality, even after adjustment for key covariates, such as functional status, depression, and comorbidity (DeSalvo, Bloser, Reynolds, He, & Muntner, 2006; McHorney, Ware, & Raczek, 1993; Stewart, Hays, & Ware, 1988). Internal consistency for the composite score was high (Cronbach’s α = .89).
Close-friendship quality was assessed at age 13, in part by the named closest friend of each primary participant. Friendship quality was assessed as the mean of standardized item scores from two instruments. The Inventory of Parent and Peer Attachment (Armsden & Greenberg, 1987) asked the close friend to assess the overall quality of the friendship, with the primary participant using 25 five-point items on a Likert-type scale regarding the degree of trust, communication, and alienation (reverse-scored) in the relationship. The Friendship Quality Questionnaire (Parker & Asher, 1993) assessed positive (e.g., support, validation) as well as negative (e.g., conflict, betrayal; reverse-scored) aspects of the friendship with the primary participant. Items were standardized and summed to yield the final scale. Internal consistency for the composite score was high (Cronbach’s α = .93).
Allocentrism vis-à-vis peers was assessed repeatedly each year from ages 14 through 17 using ratings obtained from the participant’s named closest friend each year. Once each year across this age span, the named closest friend at that age (not necessarily the same across ages) answered 20 questions: 5 questions about the participant’s acquiescence to peer norms (e.g., to what extent is the following statement applicable to the participating teen: “Some teens do things just because other teens do them”), 7 Likert-type-scale questions regarding how readily the participating teen was influenced by the close friend (e.g., “Overall how much do you actually influence how much [participant’s name] hangs out with other people”), and 8 questions on a Likert-type scale assessing teen assertiveness from the Interpersonal Competence Questionnaire (Buhrmester, 1990; e.g., how good is [participant] at “voicing his/her desires and opinions,” “getting his/her own way with others,” etc.).
To create the overall scale of allocentrism vis-à-vis peers, we reverse-scored assertiveness items, and all items were then standardized, summed, and aggregated across the annual assessments from ages 14 through 17 to create the overall allocentrism scale. Internal consistency for the aggregated allocentrism scale was quite good (Cronbach’s α = .80), particularly given that the scale combines reports of multiple individuals for behaviors assessed across different ages. Given that Cronbach’s alpha is dependent on the number of items in a measure, the alpha for allocentrism likely reflects only modest interitem correlations, which suggests that allocentrism might be more appropriately considered as an inventory or emergent construct (in which items sum to predict outcomes but for which strong interitem correlations are not necessarily expected; P. Cohen, Cohen, Teresi, Marchi, & Velez, 1990). Said differently, the allocentrism measure might be considered more appropriately as reflecting a sampling of actual allocentric behavior across time and contexts—with the effects of such behavior adding up rather than serving as indicators of an underlying latent construct.
Adult anxiety and depressive symptoms were assessed annually at the ages of 25, 26, and 27 years, and results were averaged across ages to yield an overall measure. The 20-item trait anxiety scale from the state-trait anxiety inventory (Spielberger, 1983; Spielberger, Sydeman, Owen, & Marsh, 1999) was used to measure stable individual differences in anxiety proneness. Responses used a 4-point Likert-type scale on which participants indicated their agreement with statements such as “I worry too much over something that doesn’t really matter.” The overall trait anxiety scale has demonstrated strong psychometric properties and external validity (Spielberger, 1983; Spielberger et al., 1999), and internal consistency for the scale in this study was high (Cronbach’s α = .93).
Participants also completed the Beck Depression Inventory, a 21-item measure designed to assess the degree of depressive symptoms in late adolescents and adults (Beck & Steer, 1987). Items were rated on a Likert-type scale and summed to yield a total depressive-symptoms score. This instrument is a well-validated and widely accepted self-report measure of adult depressive symptomatology (Kazdin, 1990). Internal consistency for this measure in this study was high (Cronbach’s α = .91). Given that these measures of adult anxiety and depressive symptoms were highly correlated (r = .78, p < .001), an overall measure of adult internalizing symptoms was constructed by first standardizing and then summing these two measures together.
The total number of a series of 43 distinct significant possible health problems first experienced prior to age 18 and leading at some point to hospitalization was reported by participants during the adult phase of the study as a baseline marker of health difficulties. This measure was a significant predictor of current adult health quality (r = .24, p = .006) and was therefore used as a covariate in all analyses. Other possible indices of prior health problems, including the total number of health problems experienced, and dichotomous measures of the presence or absence of any significant problem or the presence or absence of any problem leading to hospitalization were also examined but were not as strongly predictive of adult health as the present measure. Alternative analyses indicated that their use would not have substantially altered any of the substantive findings reported.
Household income was assessed in terms of the total family income reported by parents in the adolescent’s household at the age 13 assessment, on a scale ranging from 1 (under $5,000 annually) to 8 (more than $60,000 annually). Body mass index was assessed at ages 25, 26, and 27 and averaged across these three assessments. Height (in meters) and weight (in kilograms) were assessed while participants wore light clothing, and body mass index was calculated using the standard formula (weight/height2).
Adolescent or adult use of hard drugs was assessed at ages 14 and 15, and again at ages 25, 26, and 27 as the total number of reported instances of use of each of eight classes of hard drugs (hallucinogens, barbiturates, tranquilizers, amphetamines, inhalants, heroin, cocaine, oxycontin) during the 12 months prior to the study on a scale ranging from 1 (none) to 5 (10 or more times), using a widely regarded and oft-used self-report format (Johnston, O’Malley, Bachman, & Schulenberg, 2010). Use levels were averaged across the age 14 and 15 assessments as an index of adolescent use of hard drugs, and at ages 25, 26, and 27 as an index of adult use.
At age 24, participants’ personality traits were assessed with the 50-item International Personality Item Pool (Goldberg, 1999; Goldberg et al., 2006), using a 5-point Likert-type scale with 10 items each assessing constructs of extraversion, agreeableness, conscientiousness, emotional stability, and imagination. This measure has previously demonstrated strong internal consistency, retest reliability, convergence with longer Big Five personality measures, and self-peer agreement (Goldberg et al., 2006). For this sample, internal consistency for the scales was good (Cronbach’s αs = .74–.89).
At ages 13, 14, and 15, respondents rated their experience of 21 anxiety symptoms in the week prior to the study on a 4-point Likert-type scale using the Beck Anxiety Inventory (Beck, Epstein, Brown, & Steer, 1988); responses averaged across measurement points. Internal consistency for this measure in this study was high (Cronbach’s α = .90).
Adolescents reported the degree of their depressive symptoms using the Child Depression Inventory (Kovacs & Beck, 1977) at ages 13, 14, and 15. This 27-item inventory is based on the Beck Depression Inventory and has been well-validated as a measure of depressive symptomatology in children and adolescents and linked to poor self-esteem, hopelessness, and negative cognitive attributions (Kazdin, 1990). Scores were summed and then averaged across assessments at all three ages to produce a baseline depressive-symptoms score for early adolescence. Internal consistency for this measure in this study was high (Cronbach’s α = .93).
Physical attractiveness in adolescence at ages 13, 14, and 15 was coded using raters naive to the purpose of the study (Kopera, Maier, & Johnson, 1971; Patzer, 1985). In a naive coding system, raters coded code information without any specific instruction regarding the construct; instead, coders are asked to apply their lay understanding of the meaning of the given construct or term. In this case, lay coders were told to rate attractiveness based on their own understanding of the common meaning of the term “physical attractiveness.” The coding team (N = 8) was ethnically diverse and included both males and females. Coding was based on observation of video recordings of adolescents during the first 30 s of an interaction task with peers (with sound off and image of the peer obscured). Coding systems in which raters are naive attain reliability by compositing ratings from multiple raters, and in this case yielded highly reliable ratings at ages 13, 14, and 15 (intraclass correlation coefficients = .93, .89, and .87, respectively). Assessments of physical attractiveness across these ages were averaged to create an index of adolescent physical attractiveness across ages 13 to 15. Internal consistency of the combined measure across ages was good (Cronbach’s α = .77).
Results
Preliminary analyses
Means and standard deviations for all substantive variables examined in the study are presented in Table 1. Intercorrelations among primary variables in the study are presented in Table 2. Given initial findings suggesting relations of gender and family income to other variables in the study, gender and family income were included as covariates in all analyses. We also examined possible moderating effects of these demographic factors on each of the relationships examined in the primary analyses. Moderating effects were assessed by creating interaction terms based on the product of the centered main-effect variables. No moderating effects of gender or income on any of the primary relations observed were found.
Table 1.
Means and Standard Deviations for All Variables Examined
| Variable | M | SD |
|---|---|---|
| Primary variables | ||
| Adult health quality (ages 25–27) | 14.7 | 3.42 |
| Close-friendship quality (age 13) | .01 | .55 |
| Allocentrism vis-à-vis peers (ages 14–17) | .01 | .27 |
| Internalizing symptoms (ages 25–27) | .00 | .82 |
| Body mass index (ages 25–27) | 26.8 | 7.9 |
| History of serious illness prior to age 18 | .18 | .46 |
| Family income (age 13) | 6.1 | 2.0 |
| Additional potential confounds | ||
| Depressive symptoms (ages 13–15) | 5.8 | 4.6 |
| Anxiety (ages 13–15) | 6.6 | 8.0 |
| Physical attractiveness (ages 13–15) | 3.7 | 0.7 |
| Hard-drug use (ages 14–15) | 1.04 | 0.27 |
| Hard-drug use (ages 25–27) | 0.54 | 2.04 |
| Extraversion (age 23) | 35.0 | 7.5 |
| Agreeableness (age 23) | 39.8 | 5.5 |
| Conscientiousness (age 23) | 37.4 | 6.1 |
| Emotional stability (age 23) | 34.2 | 8.7 |
| Imagination (age 23) | 38.8 | 5.7 |
Note: For variables assessed across a range of years, items were assessed annually, and the scores were averaged.
Table 2.
Intercorrelations Among Variables in the Primary Model
| Variable | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|
| 1. Health quality (ages 25–27) | .15* | .25*** | −.46*** | −.14 | −.24** | −.01 | −.13 |
| 2. Close-friendship quality (age 13) | — | .09 | −.13 | −.01 | −.01 | .17* | .19** |
| 3. Allocentrism vis-à-vis peers (ages 14–17) | — | −.23** | −.07 | .05 | −.19** | −.03 | |
| 4. Internalizing symptoms (ages 25–27) | — | −.10 | .14 | −.07 | .13 | ||
| 5. Body mass index (ages 25–27) | — | −.12 | −.09 | .13 | |||
| 6. History of serious illness prior to age 18 | — | −.07 | .14 | ||||
| 7. Family income (age 13) | — | −.11 | |||||
| 8. Gender (male = 1, female = 2) | — |
p < .05.
p ≤ .01.
p < .001.
Primary analyses
For all primary analyses, we used SAS PROC CALIS (Version 9.4; SAS Institute, Cary, NC) to assess key relations in hierarchical regression models. Full-information maximum-likelihood methods were used to handle missing data.
Hypothesis 1
We first examined the quality of early-adolescent close friendships and midadolescent allocentric behavior as predictors of adult physical health at ages 25 through 27. Models also accounted for adolescent gender, baseline income in adolescents’ family, history of serious health problems prior to age 18, and current adult body mass index. Results, presented in Table 3, indicated that adolescent close-friendship quality and allocentric behavior each independently predicted greater adult health quality and together accounted for 8.7% of the observed variation in adult health quality.
Table 3.
Results of the Model Predicting Adult Health Quality
| Step and predictor | β | 95% confidence interval |
|---|---|---|
| Step 1 (ΔR2 = .017, total R2 = .017) | ||
| Gender (male = 1, female = 2) | −0.10 | [−0.25, 0.04] |
| Total family income (age 13) | −0.05 | [−0.19, 0.10] |
| Step 2 (ΔR2 = .041**, total R2 = .068*) | ||
| History of serious illness prior to age 18 | −0.26*** | [−0.41, 0.11] |
| Step 3 (ΔR2 = .025*, total R2 = .093**) | ||
| Body mass index (ages 25–27) | −0.15* | [−0.28, −0.00] |
| Step 4 (ΔR2 = .087***, total R2 = .180***) | ||
| Peer-rated close-friendship quality (age 13) | 0.17** | [0.02, 0.31] |
| Peer-rated allocentrism vis-à-vis peers (ages 14–17) | 0.23*** | [0.09, 0.37] |
Note: Betas are from the final model.
p < .05.
p ≤ .01.
p < .001.
Hypothesis 2
We tested the significance of these hypothesized mediated paths using the MODEL INDIRECT option in MPlus (Version 7.2; Muthén & Muthén, 2015). Bootstrapping procedures were used to determine the proper confidence band around the indirect point estimate (Hayes & Scharkow, 2013). Figure 1 depicts the results of a path analysis in which concurrent and adolescent-era anxiety and depressive symptoms were added to the variables in the predictive model shown in Table 3; effects of early-adolescent friendship quality were fully mediated via adult levels of internalizing symptoms (indirect effect: β = 0.07, p = .03, 95% confidence interval, or CI = [0.01, 0.15]). Effects of adolescent allocentric behavior displayed both direct links to adult health quality and an additional link mediated via adult internalizing symptoms (indirect effect: β = 0.07, p = .049, 95% CI = [0.001, 0.13]). Figure 1 presents the full model, with the exception of adolescent anxiety symptoms, which displayed no direct or indirect links to adult health quality. The path model displayed in Figure 1 fit the data well—goodness-of-fit index = .98; adjusted goodness-of-fit index = .95; root-mean-square error of approximation = 0; χ2(21) = 115.6, p = .79, with modification indices revealing no additional significant pathways not included in the model.
Fig. 1.
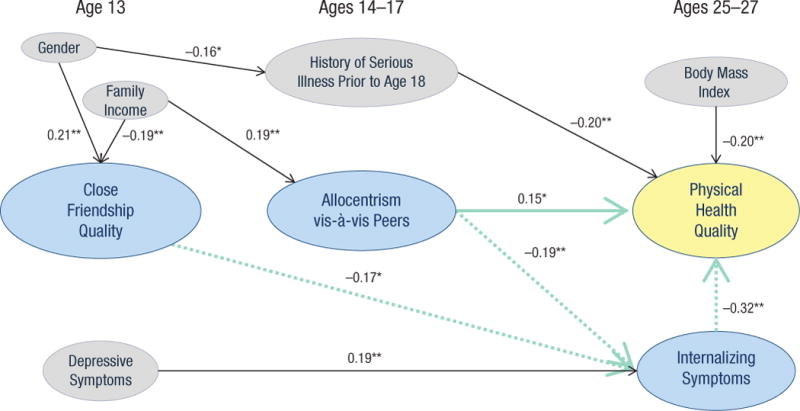
Mediation model predicting adult health (ages 25–27 years) from adolescent qualities (ages 13–17). Key predictors are highlighted in blue. For these variables, solid arrows indicate direct paths; dashed arrows indicate mediated paths. Though this is not depicted, the model also included adolescent-era anxiety symptoms as a covariate. Standardized coefficients are shown. Asterisks indicate significant paths (*p < .05, **p ≤ .01).
Hypothesis 3
Other factors that might serve as potential third-variable confounds—predicting both relationship quality and health—were examined next. These included observer ratings of participant physical attractiveness in early adolescence, history of either adolescent-era or adult-era use of hard drugs, and personality measures of neuroticism, extraversion, conscientiousness, openness to experience, and agreeableness. Taken together, these covariates accounted for significant variance in adult health quality, with adult hard-drug use (β = −0.16, p = .03, 95% CI = [−0.30, −0.01]), and emotional stability (β = 0.26, p = .001, 95% CI = [0.10, 0.41]) contributing to predicting health quality. These covariates do include a number of self-report measures, however, which creates a methods confound with self-reported health quality that would tend to lead to an overestimate of the effect of these variables. Even after including this block of potential third-variable confounds, both adolescent friendship quality (β = 0.16, p = .02, 95% CI = [0.02, 0.30]) and allocentric behavior (β = 0.23, p < .001, 95% CI = [0.09, 0.37]) continued to predict adult health quality, with their effect sizes remaining relatively unchanged; together, they accounted for 7.2% of the variance in adult health quality (p < .001).
Discussion
These results indicate that remaining close to as opposed to separating oneself from the peer pack in adolescence has long-term implications for adult physical health. Peer-relationship qualities, assessed as early as the age of 13 years, were linked to adult health quality at the ages of 25 to 27 years, even after accounting for a broad array of potential confounding factors. These predictions were from social-relationship qualities as observed and reported not by the participants but by their peers. Thus, any potential methods confound with later health reports was avoided. Together, the two adolescent-peer-relationship constructs added more to the explained variance in adult health quality than the combined effect of current body mass index and a measure of prior serious illnesses, which thus indicates the potential magnitude of the type of peer-relationship effects observed.
The observed predictive link between adult health quality and adolescent close-friendship quality, assessed more than a decade earlier, suggests the long-term implications of adolescent friendships for adult physical health. This link can be understood as the inverse of the previously established connection between social isolation and poor health within adulthood (Hawkley & Cacioppo, 2010; Holt-Lunstad et al., 2010). The present finding expands the understanding of the potential health relevance of friendships in adolescence and indicates the importance of a positive indicator of relationship quality as opposed to a simple lack of isolation.
Allocentric behavior—acting as a follower more than a leader, being low in assertiveness, and being readily influenced by peers—involves placing one’s own desires second to those of the peer group. In this study, it was a robust predictor of increased long-term physical health quality. This finding is consistent both with emerging theory and research on the links among collectivist culture, collectivist behavior, and positive health outcomes (Talhelm et al., 2014), as well as with primate research on the physiological stresses of being separated from the larger social pack (Sapolsky, 2004).
Both of these long-term predictive relationships potentially cast a range of adolescent behaviors in a new light. The intense adolescent focus on forming and maintaining peer relationships may well result from an instinctive recognition that these relationships are linked to well-being. Links of adolescent allocentric behavior to future health suggests a need to at least reconsider the role of such pack behavior. Currently, resisting peer pressure and establishing one’s autonomy are all primary values that adults in Western cultures attempt, with only mixed success, to inculcate in adolescents (McElhaney et al., 2009). Yet these values are somewhat at odds with the allocentric, peer-centered approach linked to health quality in this study. Although autonomy-establishing behavior is clearly of value in modern Western society, in which daily survival threats are minimal, it may have become linked to stress reactions over the course of human evolution, when separation from the larger human pack was likely to bring grave danger (Talhelm et al., 2014).
Notably, allocentrism and close-friendship quality were uncorrelated, and each uniquely added to the prediction of future adult health quality. One explanation for these findings is that both close-friendship quality and allocentrism may function as pack behaviors that reduce stress levels, albeit via different mechanisms (e.g., provision of support vs. avoidance of conflict with the broader group, respectively). It was not clear from this study whether allocentrism is best considered as a latent construct (e.g., a personality trait vs. an emergent construct such as the additive effect of multiple allocentric behaviors), although this would be important for future research to consider.
Consistent with prior research within adulthood, our findings showed that the effects of adolescent relationship qualities on adult health appeared to be potentially mediated via decreased levels of later anxiety and depressive symptoms (Curhan et al., 2014). Given that health and internalizing measures were assessed concurrently, we cannot, of course, rule out the possibility that mediation proceeds via the opposite path, from adolescent relationship factors through health quality to internalizing symptoms. Indeed, it is quite plausible that both pathways exist, and it remains for future research to explore these possibilities. Future research is also needed to examine the physiological and behavioral mediators of the long-term links found in this study. Candidate mediating processes include risk behavior, cardiovascular and immune functioning, and metabolic processing (Arthur, 2006; Cacioppo & Patrick, 2008; Friedmann et al., 2006; Grippo et al., 2007).
From a risk and prevention perspective, difficulty forming close relationships early in adolescence may now be considered a marker of risk for long-term health difficulties. Current national pediatric recommendations for the prevention of future health risks in adolescence do not address any relational factors (Institute of Medicine, 2012). Yet relational factors may be at least as modifiable as other identified risks in adolescence (e.g., smoking and obesity) (Walton & Cohen, 2011). Addressing the link between allocentric behavior and future health is more challenging, given the Western valuing of individual autonomy and links of autonomy to success in domains beyond physical health (Allen et al., 2014). Recognition of the challenge that adolescents face in balancing the costs and benefits of seeking autonomy versus acquiescing to peer influence appears to be a reasonable first step.
Several limitations to these findings should be noted. Although our results are consistent with findings from research in adulthood, and they extend these findings with far more intensive and independent observations of social behavior in adolescence than have heretofore been available, direct causal conclusions cannot be inferred from these data. Even controlling for a wide range of third-variable explanations is not sufficient to establish a causal relationship between adolescent social factors and adult health. Indeed, it is plausible that the measured factors were indicators of adolescent propensities linked to a range of social behaviors that may have combined to influence health outcomes. Additionally, adolescent-era health problems were reported retrospectively, which may have added bias to this measure. Despite these limitations, these data are the first to link peer ratings of adolescent relationship quality to adult physical health, and they open up new questions regarding the long shadows that early peer relationships might cast on health quality across the life span.
Acknowledgments
Funding
This study was supported by grants from the National Institute of Child Health and Human Development (9R01 HD058305-11A1) and the National Institute of Mental Health (R01-MH58066).
Footnotes
Author Contributions
J. P. Allen designed the study, led the analyses, and drafted the manuscript. B. N. Uchino contributed to designing the study, interpreting and analyzing the data, and drafting and editing the manuscript. C. A. Hafen contributed to analytic plans for the study, the interpretation of results, and drafting and editing of the manuscript.
Declaration of Conflicting Interests
The authors declared that they had no conflicts of interest with respect to their authorship or the publication of this article.
References
- Allen JP, Chango J, Szwedo DE. The adolescent relational dialectic and the peer roots of adult social functioning. Child Development. 2014;85:192–204. doi: 10.1111/cdev.12106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Arbuckle JL. Full information estimation in the presence of incomplete data. In: Marcoulides GA, Schumacker RE, editors. Advanced structural modeling: Issues and techniques. Mahwah, NJ: Erlbaum; 1996. pp. 243–277. [Google Scholar]
- Armsden GC, Greenberg MT. The Inventory of Parent and Peer Attachment: Individual differences and their relationship to psychological well-being in adolescence. Journal of Youth and Adolescence. 1987;16:427–454. doi: 10.1007/BF02202939. [DOI] [PubMed] [Google Scholar]
- Arthur HM. Depression, isolation, social support, and cardiovascular disease in older adults. Journal of Cardiovascular Nursing. 2006;21(5):S2–S7. doi: 10.1097/00005082-200609001-00002. [DOI] [PubMed] [Google Scholar]
- Bardone AM, Moffitt TE, Caspi A, Dickson N, Stanton WR, Silva PA. Adult physical health outcomes of adolescent girls with conduct disorder, depression, and anxiety. Journal of the American Academy of Child & Adolescent Psychiatry. 1998;37:594–601. doi: 10.1097/00004583-199806000-00009. [DOI] [PubMed] [Google Scholar]
- Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: Psychometric properties. Journal of Consulting and Clinical Psychology. 1988;576:893–897. doi: 10.1037//0022-006x.56.6.893. [DOI] [PubMed] [Google Scholar]
- Beck AT, Steer RA. Manual for the revised Beck Depression Inventory. San Antonio, TX: Psychological Corp; 1987. [Google Scholar]
- Berns GS, Chappelow J, Zink CF, Pagnoni G, Martin-Skurski ME, Richards J. Neurobiological correlates of social conformity and independence during mental rotation. Biological Psychiatry. 2005;58:245–253. doi: 10.1016/j.biopsych.2005.04.012. [DOI] [PubMed] [Google Scholar]
- Brown BB, Larson J. Peer relations in adolescence. In: Lerner RM, Steinberg L, editors. Handbook of adolescent psychology. 3rd. New York, NY: John Wiley & Sons; 2009. pp. 74–103. [Google Scholar]
- Buhrmester D. Intimacy of friendship, interpersonal competence, and adjustment during preadolescence and adolescence. Child Development. 1990;61:1101–1111. [PubMed] [Google Scholar]
- Cacioppo JT, Patrick W. Loneliness: Human nature and the need for social connection. New York, NY: W. W. Norton; 2008. [Google Scholar]
- Chango JM, Allen JP, Szwedo D, Schad MM. Early adolescent peer foundations of late adolescent and young adult psychological adjustment. Journal of Research on Adolescence. 2014 doi: 10.1111/jora.12162. Advance online publication. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chiao JY, Blizinsky KD. Culture-gene coevolution of individualism-collectivism and the serotonin transporter gene. Proceedings of the Royal Society B: Biological Sciences. 2010;277:529–537. doi: 10.1098/rspb.2009.1650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen GL, Prinstein MJ. Peer contagion of aggression and health risk behavior among adolescent males: An experimental investigation of effects on public conduct and private attitudes. Child Development. 2006;77:967–983. doi: 10.1111/j.1467-8624.2006.00913.x. [DOI] [PubMed] [Google Scholar]
- Cohen P, Cohen J, Teresi J, Marchi M, Velez CN. Problems in the measurement of latent variables in structural equations causal models. Applied Psychological Measurement. 1990;14:183–196. [Google Scholar]
- Cohen S, Janicki-Deverts D, Miller GE. Psychological stress and disease. The Journal of the American Medical Association. 2007;298:1685–1687. doi: 10.1001/jama.298.14.1685. [DOI] [PubMed] [Google Scholar]
- Curhan KB, Sims T, Markus HR, Kitayama S, Karasawa M, Kawakami N, Ryff CD. Just how bad negative affect is for your health depends on culture. Psychological Science. 2014;25:2277–2280. doi: 10.1177/0956797614543802. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DeSalvo KB, Bloser N, Reynolds K, He J, Muntner P. Mortality prediction with a single general self-rated health question. Journal of General Internal Medicine. 2006;21:267–275. doi: 10.1111/j.1525-1497.2005.00291.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ehrlich KB, Hoyt LT, Sumner JA, McDade TW, Adam EK. Quality of relationships with parents and friends in adolescence predicts metabolic risk in young adulthood. Health Psychology. 2015 doi: 10.1037/hea0000213. Advance online publication. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Englund MM, I-Chun Kuo S, Puig J, Collins WA. Early roots of adult competence: The significance of close relationships from infancy to early adulthood. International Journal of Behavioral Development. 2011;35:490–496. doi: 10.1177/0165025411422994. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fagundes CP, Way B. Early-life stress and adult inflammation. Current Directions in Psychological Science. 2014;23:277–283. [Google Scholar]
- Fincher CL, Thornhill R, Murray DR, Schaller M. Pathogen prevalence predicts human cross-cultural variability in individualism/collectivism. Proceedings of the Royal Society B: Biological Sciences. 2008;275:1279–1285. doi: 10.1098/rspb.2008.0094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Friedmann E, Thomas SA, Liu F, Morton PG, Chapa D, Gottlieb SS, Sudden Cardiac Death in Heart Failure Trial Investigators Relationship of depression, anxiety, and social isolation to chronic heart failure outpatient mortality. American Heart Journal. 2006;152(5):940.e1–940.e8. doi: 10.1016/j.ahj.2006.05.009. [DOI] [PubMed] [Google Scholar]
- Fuligni AJ, Eccles JS, Barber BL, Clements P. Early adolescent peer orientation and adjustment during high school. Developmental Psychology. 2001;37:28–36. doi: 10.1037//0012-1649.37.1.28. [DOI] [PubMed] [Google Scholar]
- Goldberg LR. A broad-bandwidth, public-domain, personality inventory measuring the lower-level facets of several Five-Factor models. Personality Psychology in Europe. 1999;7:7–28. [Google Scholar]
- Goldberg LR, Johnson JA, Eber HW, Hogan R, Ashton MC, Cloninger CR, Gough HG. The international personality item pool and the future of public-domain personality measures. Journal of Research in Personality. 2006;40:84–96. [Google Scholar]
- Grippo AJ, Gerena D, Huang J, Kumar N, Shah M, Ughreja R, Carter CS. Social isolation induces behavioral and neuroendocrine disturbances relevant to depression in female and male prairie voles. Psychoneuroendocrinology. 2007;32:966–980. doi: 10.1016/j.psyneuen.2007.07.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hall GS. Adolescence. New York, NY: Appleton; 1904. [Google Scholar]
- Hawkley LC, Cacioppo JT. Loneliness matters: A theoretical and empirical review of consequences and mechanisms. Annals of Behavioral Medicine. 2010;40:218–227. doi: 10.1007/s12160-010-9210-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hayes AF, Scharkow M. The relative trustworthiness of inferential tests of the indirect effect in statistical mediation analysis: Does method really matter? Psychological Science. 2013;24:1918–1927. doi: 10.1177/0956797613480187. [DOI] [PubMed] [Google Scholar]
- Holt-Lunstad J, Smith TB, Layton JB. Social relationships and mortality risk: A meta-analysis. PLoS Medicine. 2010;7(7):Article e1000316. doi: 10.1371/journal.pmed.1000316. Retrieved from http://journals.plos.org/plosmedicine/article?id=10.1371/journal.pmed.1000316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- House JS, Landis KR, Umberson D. Social relationships and health. Science. 1988;241:540–545. doi: 10.1126/science.3399889. [DOI] [PubMed] [Google Scholar]
- Institute of Medicine. Accelerating progress in obesity prevention: Solving the weight of the nation. Washington, DC: Author; 2012. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. (NIH Publication No. 10-7584).Monitoring the future: National survey results on drug use, 1975–2009. Vol. I: Secondary school students. 2010 Retrieved from http://monitoringthefuture.org/pubs/monographs/vol1_2009.pdf.
- Kawachi I, Berkman LF. Social ties and mental health. Journal of Urban Health. 2001;78:458–467. doi: 10.1093/jurban/78.3.458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kawachi I, Subramanian S, Kim D. Social capital and health. New York, NY: Springer; 2008. [Google Scholar]
- Kazdin AE. Childhood depression. Journal of Child Psychology and Psychiatry and Allied Disciplines. 1990;31:121–160. doi: 10.1111/j.1469-7610.1990.tb02276.x. [DOI] [PubMed] [Google Scholar]
- Kiecolt-Glaser JK, Loving TJ, Stowell JR, Malarkey WB, Lemeshow S, Dickinson SL, Glaser R. Hostile marital interactions, proinflammatory cytokine production, and wound healing. Archives of General Psychiatry. 2005;62:1377–1384. doi: 10.1001/archpsyc.62.12.1377. [DOI] [PubMed] [Google Scholar]
- Kopera AA, Maier RA, Johnson JE. Perception of physical attractiveness: The influence of group interaction and group coaction on ratings of women; Paper presented at the annual meeting of the American Psychological Association; Washington, DC. 1971. Sep, [Google Scholar]
- Kovacs M, Beck AT. An empirical clinical approach toward a definition of childhood depression. New York, NY: Raven Press; 1977. [Google Scholar]
- McElhaney KB, Allen JP, Stephenson JC, Hare AL. Attachment and autonomy during adolescence. In: Lerner RM, Steinberg L, editors. Handbook of adolescent psychology: Vol. 1. Individual bases of adolescent development. 3rd. Hoboken, NJ: John Wiley & Sons; 2009. pp. 358–403. [Google Scholar]
- McHorney CA, Ware JE, Jr, Raczek AE. The MOS 36-Item Short-Form Health Survey (SF-36): II. Psychometric and clinical tests of validity in measuring physical and mental health constructs. Medical Care. 1993;31:247–263. doi: 10.1097/00005650-199303000-00006. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide, Version 7.2. Los Angeles, CA: Author; 2015. [Google Scholar]
- Nealey-Moore JB, Smith TW, Uchino BN, Hawkins MW, Olson-Cerny C. Cardiovascular reactivity during positive and negative marital interactions. Journal of Behavioral Medicine. 2007;30:505–519. doi: 10.1007/s10865-007-9124-5. [DOI] [PubMed] [Google Scholar]
- Parker JG, Asher SR. Friendship and friendship quality in middle childhood: Links with peer group acceptance and feelings of loneliness and social dissatisfaction. Developmental Psychology. 1993;29:611–621. [Google Scholar]
- Patzer GL. The physical attractiveness phenomena. New York, NY: Springer; 1985. [Google Scholar]
- Sapolsky RM. Stress hormones: Good and bad. Neurobiology of Disease. 2000;7:540–542. doi: 10.1006/nbdi.2000.0350. [DOI] [PubMed] [Google Scholar]
- Sapolsky RM. Why zebras don’t get ulcers. New York, NY: Henry Holt; 2004. [Google Scholar]
- Spielberger CD. Manual for the State-Trait Anxiety Inventory (Form Y) Palo Alto, CA: Mind Garden; 1983. [Google Scholar]
- Spielberger CD, Sydeman SJ, Owen AE, Marsh BJ. Measuring anxiety and anger with the State-Trait Anxiety Inventory (STAI) and the State-Trait Anger Expression Inventory (STAXI) In: Maruish ME, editor. The use of psychological testing for treatment planning and outcomes assessment. 2nd. Mahwah, NJ: Erlbaum; 1999. pp. 993–1021. [Google Scholar]
- Stewart AL, Hays RD, Ware JE. The MOS short-form general health survey: Reliability and validity in a patient population. Medical Care. 1988;26:724–735. doi: 10.1097/00005650-198807000-00007. [DOI] [PubMed] [Google Scholar]
- Talhelm T, Zhang X, Oishi S, Shimin C, Duan D, Lan X, Kitayama S. Large-scale psychological differences within China explained by rice versus wheat agriculture. Science. 2014;344:603–608. doi: 10.1126/science.1246850. [DOI] [PubMed] [Google Scholar]
- Temcheff CE, Serbin LA, Martin-Storey A, Stack DM, Ledingham J, Schwartzman AE. Predicting adult physical health outcomes from childhood aggression, social withdrawal and likeability: A 30-year prospective, longitudinal study. International Journal of Behavioral Medicine. 2011;18:5–12. doi: 10.1007/s12529-010-9082-0. [DOI] [PubMed] [Google Scholar]
- Triandis HC. The self and social behavior in differing cultural contexts. Psychological Review. 1989;96:506–520. [Google Scholar]
- Triandis HC. Cultural syndromes and subjective well-being. In: Diener E, Suh EM, editors. Culture and subjective well-being. Boston, MA: MIT Press; 2000. pp. 13–36. [Google Scholar]
- Uchino BN. What a lifespan approach might tell us about why distinct measures of social support have differential links to physical health. Journal of Social and Personal Relationships. 2009;26:53–62. doi: 10.1177/0265407509105521. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Umberson D. Family status and health behaviors: Social control as a dimension of social integration. Journal of Health and Social Behavior. 1987;28:306–319. [PubMed] [Google Scholar]
- Walton GM, Cohen GL. A brief social-belonging intervention improves academic and health outcomes of minority students. Science. 2011;331:1447–1451. doi: 10.1126/science.1198364. [DOI] [PubMed] [Google Scholar]
- Ware JE, Kosinski M, Dewey JE, Gandek B. SF-36 health survey: Manual and interpretation guide. Eden Prairie, MN: Quality Metric; 2000. [Google Scholar]
- Wright BL, Loving TJ. Health implications of conflict in close relationships. Social & Personality Psychology Compass. 2011;5:552–562. doi: 10.1111/j.1751-9004.2011.00371.x. [DOI] [Google Scholar]