

Abstract
Diaphragms were dissected out intact from 29 male and 9 female cadavers at necropsy. Fifteen of the males and eight of the females were grouped as controls, having no history of chest disease. Fourteen of the males and one female gave a history of chronic bronchitis. Point-counting and other methods were employed to measure the mean area, thickness, and volume of the diaphragmatic muscle, excluding the central tendon.
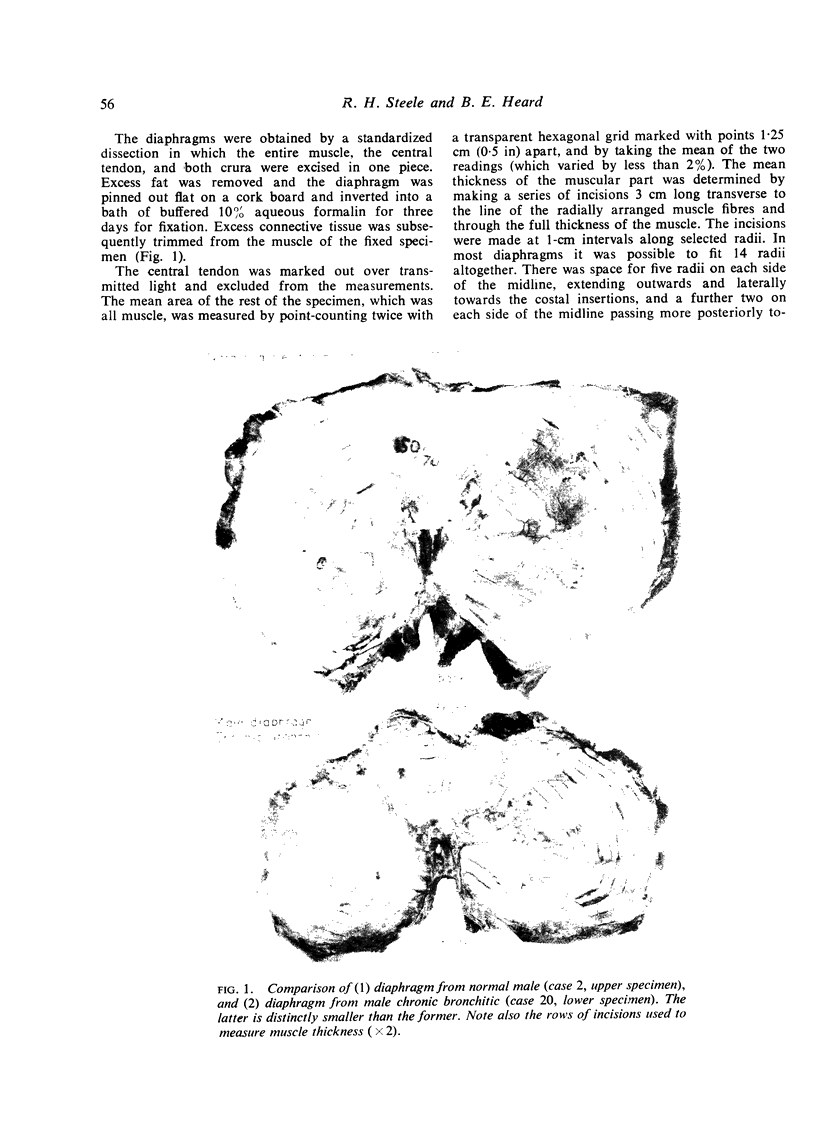
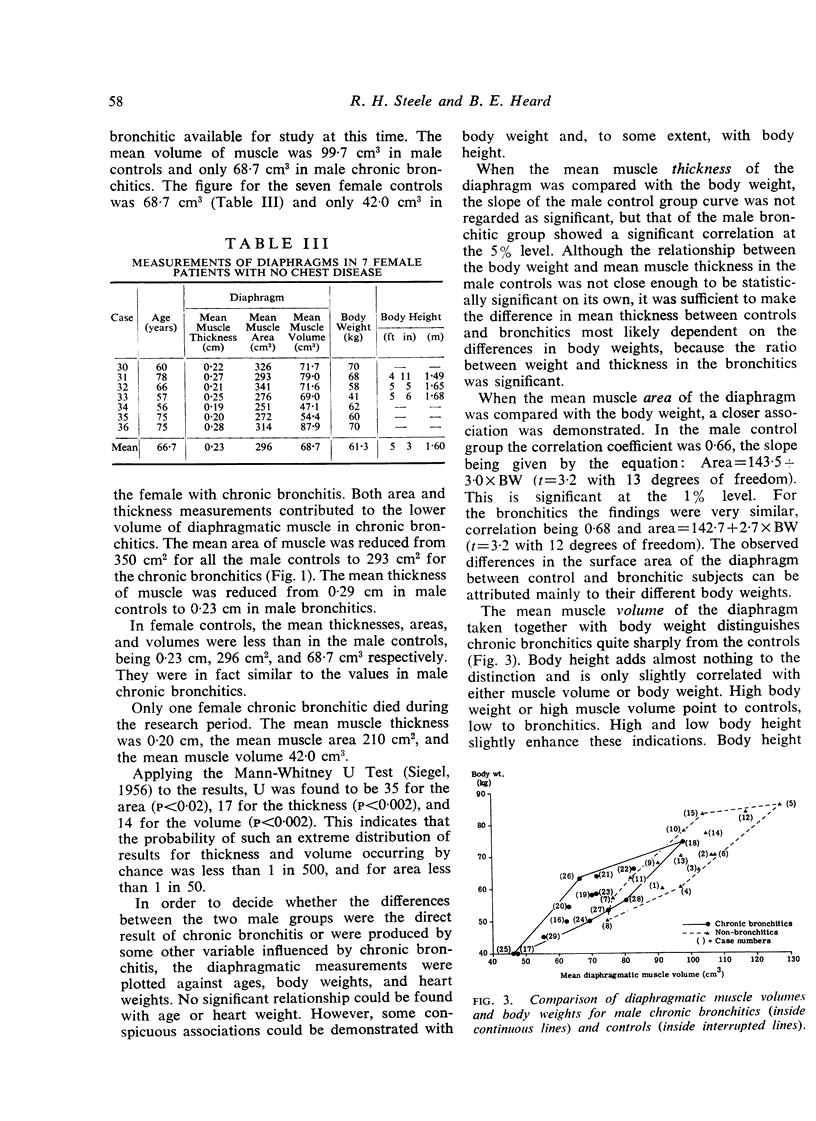
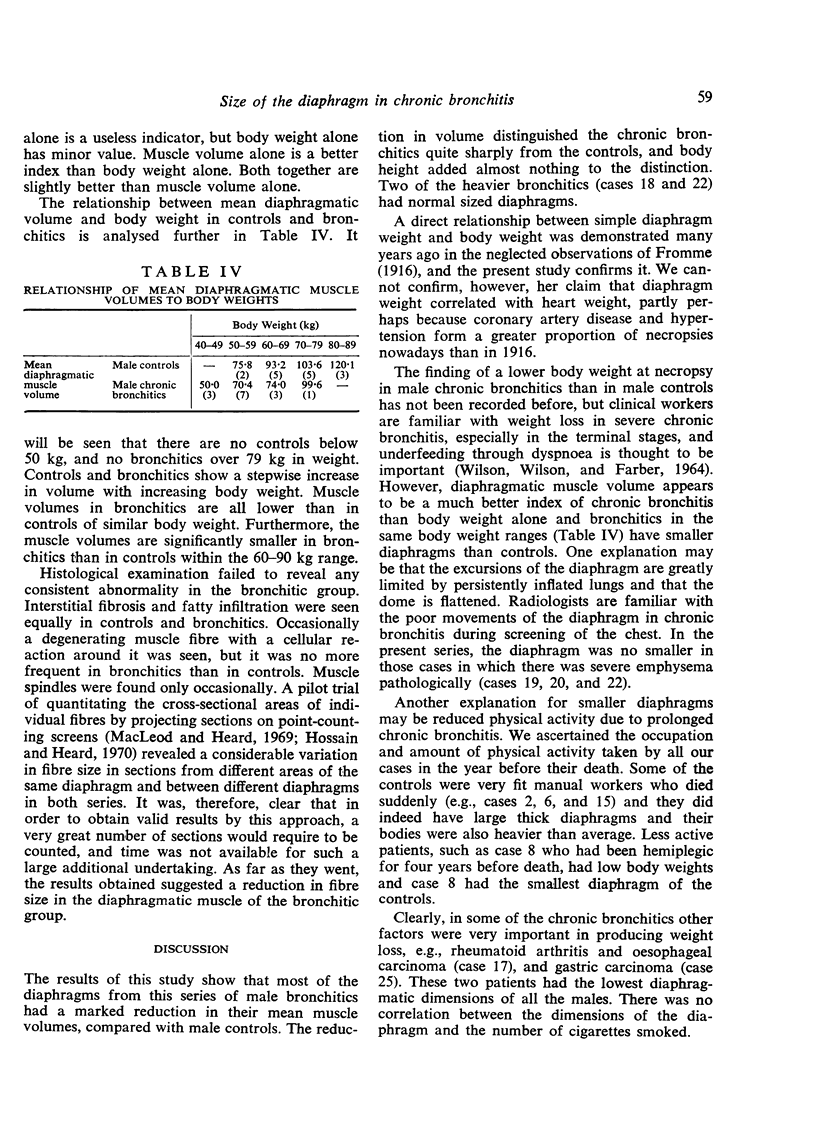
The results showed that the diaphragm was reduced in area, thickness, and volume in the chronic bronchitics, the figures being 350 cm2, 0·29 cm, and 99·7 cm3 respectively in male controls, and 295 cm2, 0·23 cm, and 68·7 cm3 in the bronchitics. In the female controls, the values were significantly lower than in the male controls. The one female bronchitic had a muscle volume of only 40 cm3. The male controls were similar in height to the bronchitics, but their mean weight was higher, being 69·4 kg against 56·0 kg in male bronchitics.
It is concluded that the diaphragm is smaller in chronic bronchitics than in controls at necropsy and that while a major factor in causation is an associated low body weight, other factors such as the mechanical consequences of flattening of the diaphragm, longstanding reduction in physical activity, and other diseases such as cancer may also play a part. No histological changes by non-quantitative methods were found in the diaphragm in the chronic bronchitics, but muscle fibre shrinkage was suspected. By contrast, a few cases of asthma examined to date have shown no evidence of reduction in diaphragm size. The mechanical implications are discussed.
Full text
PDF
Images in this article


Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BARACH A. L., SEAMAN W. B. Role of diaphragm in chronic pulmonary emphysema. N Y State J Med. 1963 Feb 1;63:415–417. [PubMed] [Google Scholar]
- BERGOFSKY E. H. RELATIVE CONTRIBUTIONS OF THE RIB CAGE AND THE DIAPHRAGM TO VENTILATION IN MAN. J Appl Physiol. 1964 Jul;19:698–706. doi: 10.1152/jappl.1964.19.4.698. [DOI] [PubMed] [Google Scholar]
- BRUN J., PERRIN-FAYOLLE M. Insuffisance diaphragmatique et insuffisance respiratoire chronique. Rev Prat. 1959 Jan 11;9(2):117–passim. [PubMed] [Google Scholar]
- BRUN J., POZZETTO H. L'emphysème pulmonaire et ses facteurs aggravants d'origine diaphragmatique. J Fr Med Chir Thorac. 1958;12(6):655–665. [PubMed] [Google Scholar]
- Boyd W. H. Coordinated electrical activity of diaphragm and intercostal muscles in rabbits during quiet breathing. Arch Phys Med Rehabil. 1969 Mar;50(3):127–132. [PubMed] [Google Scholar]
- COUCH A. H. Paralysis of the diaphragm after pneumonia and of undetermined cause. Thorax. 1953 Dec;8(4):326–328. doi: 10.1136/thx.8.4.326. [DOI] [PMC free article] [PubMed] [Google Scholar]
- DOUGLASS B. E., CLAGETT O. T. The prognosis in idiopathic diaphragmatic paralysis. Dis Chest. 1960 Mar;37:294–297. [PubMed] [Google Scholar]
- Hossain S., Heard B. E. Hyperplasia of bronchial muscle in chronic bronchitis. J Pathol. 1970 Jun;101(2):171–184. doi: 10.1002/path.1711010212. [DOI] [PubMed] [Google Scholar]
- KEEFER C. S. The diaphragm: some reflections on its function and its diseases. Bull Johns Hopkins Hosp. 1957 Apr;100(4):147–172. [PubMed] [Google Scholar]
- MCKELDEN SMITH THE EFFECT OF HEMIPLEGIA ON THE DIAPHRAGM. Am Rev Respir Dis. 1964 Mar;89:450–452. doi: 10.1164/arrd.1964.89.3.450. [DOI] [PubMed] [Google Scholar]
- Macleod L. J., Heard B. E. Area of muscle in tracheal sections in chronic bronchitis, measured by point-counting. J Pathol. 1969 Jan;97(1):157–161. doi: 10.1002/path.1710970124. [DOI] [PubMed] [Google Scholar]
- Milne E. N., Bass H. Relationship between specific dynamic pulmonary compliance and diaphragmatic excursion. Radiology. 1969 Mar;92(3):615–615. doi: 10.1148/92.3.615. [DOI] [PubMed] [Google Scholar]
- Mognoni P., Saibene F., Sant'ambrogio G. Contribution of the diaphragm and the other inspiratory muscles to different levels of tidal volume and static inspiratory effort in the rabbit. J Physiol. 1969 Jun;202(3):517–534. doi: 10.1113/jphysiol.1969.sp008825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Simon G., Bonnell J., Kazantzis G., Waller R. E. Some radiological observations on the range of movement of the diaphragm. Clin Radiol. 1969 Apr;20(2):231–233. doi: 10.1016/s0009-9260(69)80181-9. [DOI] [PubMed] [Google Scholar]
- WILSON N. L., WILSON R. H., FARBER S. M. NUTRITION IN PULMONARY EMPHYSEMA. J Am Diet Assoc. 1964 Dec;45:530–536. [PubMed] [Google Scholar]
- WYATT J. P., FISCHER V. W., SWEET H. C. THE PATHOMORPHOLOGY OF THE EMPHYSEMA COMPLEX. II. Am Rev Respir Dis. 1964 May;89:721–735. doi: 10.1164/arrd.1964.89.5.721. [DOI] [PubMed] [Google Scholar]