

Abstract
Background:
Clinical competency is one of the most important requirements in nursing profession, based on which nurses are assessed. To obtain an effective and improved form of clinical competency, several factors are observed and monitored by the health educational systems. Among these observed factors, spiritual intelligence is considered as one of the most significant factors in nurses’ success and efficacy. In this study, it is aimed to determine the spiritual intelligence status and its relationship with clinical competency.
Materials and Methods:
The descriptive–correlational research was carried out on 250 nurses in Mashhad educational hospitals, selected by multi-stage sampling. Demographic, clinical competency, and spiritual intelligence questionnaires were used for data collection and 212 questionnaires were analyzed.
Results:
About 53.3% of nurses obtained above average scores in spiritual intelligence. Clinical competency was evaluated by both self-evaluation and head nurse evaluation methods. Most nurses (53.8%) were having good level of clinical competency based on self-evaluation, 48.2% were at average level based on head nurse evaluation, and 53.3% were at average level based on overall score. A significant correlation was found between spiritual intelligence and clinical competency.
Conclusions:
In this study, the positive significant correlation between nurses’ spiritual intelligence and their clinical competency is investigated. Because of the positive effects of spiritual intelligence on nurses’ clinical competency and quality of care, it is recommended to develop nurses’ spiritual intelligence during their education and by way of continuous medical education.
Keywords: Clinical competency, competency, Iran, nurse training, nurses, spiritual intelligence
INTRODUCTION
Clinical competency is a combination of morality, values, and their reflection on knowledge and skills. Honesty, care, communication skills, and adaptability are recognized as individual competency factors.[1] Nurses constitute about 70% of health care teams which are the greatest health care providers [2] and play a crucial role in continuity of care and related services.[3] In 1990, Delbueno emphasized regarding the clinical tasks of nurses that they should have technical and communicational skills and creative mind.[4] Yekta stated that the need of the individuals seeking health according to an unwritten contract should be met by health care providers. To this extent, clinical competency is required. With respect to the management and health care providing concerns.,[5] the quality of care and then the nurses’ clinical competency would be guaranteed.[3,4] Clinical competency plays an important role as a practical discipline in nursing profession.[6] Nowadays, development of quality of care and the capabilities of the nurses have a high priority in nursing management.[4,7]
The most effective factors on clinical skills are experience, environment, use of opportunities, motivation, theoretical knowledge and personal characteristics.[8] Furthermore, most studies have been performed in institutes mainly on the effect of spirituality and individual performance development,[9,10,11] which are introduced as powerful factors for adaptation and adjustment in facing the problems.[12] Several studies also confirmed the relationship between success and spirituality, and indicated that spiritual values would not only lead to working quality [13] but also develop the organization entirely. So, introduction of spirituality into the workspace is a young phenomenon which affects positively the individual performance, the competency, and the organizational development.[14,15]
Spiritual intelligence is a new construction, i.e. a collection of individual capabilities in terms of spiritual resources which contain the effective kind of adaptation and problem-solving behavior.[16,17,18] It includes the highest developmental levels of cognitive, moral, interpersonal aspects, etc., and assists the person to adjust with his environmental phenomena and achieve an internal and external integration.[17] This intelligence provides a general view of life in terms of the experiences and spiritual resources including the important decisions made and the daily solved problems.[19]
According to Shabani et al., spiritual intelligence affects mental health.[20] Bagheri et al. (2010) showed that spiritual intelligence is effective on nurses’ happiness. This indicates the better adaptability of nurses in facing daily stress with a higher spiritual intelligence.[21] The authors could not find any particular study conducted in Iran investigating the relation between nurses’ spiritual intelligence and clinical competency. Therefore, it seemed necessary to determine the relationship between spiritual intelligence and clinical competency.
MATERIALS AND METHODS
This descriptive–correlational research was conducted on 250 nurses undergoing training in Mashhad Hospitals. Ethical considerations were confirmed by the MUMS ethics committee, and an introduction letter was received from Mashhad School of Nursing and Midwifery which was presented to the hospitals before multi-stage sampling was conducted. At first, different wards were divided into four groups: General, Special, Intensive care, and Emergency. Then, 48 wards were selected randomly from all the hospitals. The number of nurses was based on the hospital size. To this extent, 88 nurses from Imam Reza Hospital, 82 from Quaem Hospital, 23 from Dr. Sheikh Hospital, and 19 from Hashemi Nejad Hospital were selected. Based on the grouping of wards, 58 nurses from general, 61 from special, 61 from intensive care, and 32 from emergency were selected. By the permission of head nurses, the nurses were selected randomly from each ward. Then, they were given research consent, necessary explanations, and a brief introduction of the research objectives. The inclusion criteria for the nurses included: Holding a B. Sc. degree of nursing with at least 6 months of nursing experience in the observed ward and working neither as a supervisor nor as a head nurse. The questionnaires were kept anonymous and confidential. Also, the selected nurses were assured that their responses had no effect on their organizational evaluation, so they were asked to answer all the questions honestly and precisely. Then, at the second stage of the research, the nurses and head nurses were instructed to complete the competency questionnaires. The questionnaires were presented at the beginning of the work shift when the workload was low and the nurses were fresh. They were asked to fill the questionnaires separately. The coded questionnaires of clinical competency were given to the head nurses to be completed under their direct supervision. The questionnaires were collected after the end of each shift. In case of lack of time, they were collected in the next shift.
Demographic, clinical competency, and spiritual intelligence [19] questionnaires were used for data collection.[22] Nurses’ clinical competency assessment tool contains 55 items and 7 domains (caring, interpersonal communication, ethics and professional morality, professional development, education, critical thinking, and management) scored by Likert scaling as follows:
I am not competent 0
I am less competent 1
I am roughly competent 2
I am sufficiently competent 3
I am highly competent 4.
Spiritual intelligence questionnaire contains 97 questions which evaluated the eight aspects of patience, beliefs, spiritual religious practices, meaning and goal in life, divinity and slavery, internal peace, spiritual experience, self-cognition, and forgiveness. Its total score was between 97 and 388. The reliability of questionnaires was confirmed using Cronbach's alpha coefficient as 87% for spiritual intelligence, 96% for patience, 90% for beliefs and spiritual religious practices, 88% for meaning and goal in life, 84% for divinity and slavery, 96% for internal peace, 82% for spiritual experience, 85% for self-cognition, 93% for forgiveness, 84% for clinical competency, 87% for aspects of care, 91% for interpersonal communication, 84% for ethics and professional morality, 89% for professional development, 90% for education, 82% for critical thinking, and 94% for management.[19] Finally, data collected from 212 nurses were analyzed by SPSS 11.5 using descriptive statistics; for comparing means, analysis of variance (ANOVA), Kruskal–Wallis, t-test, Mann–Whitney test were used for spiritual intelligence and its domains; correlation test and simple linear regression were used for determining the relationship between spiritual intelligence with clinical competency, and covariance analysis for controlling the interfering variables.
RESULTS
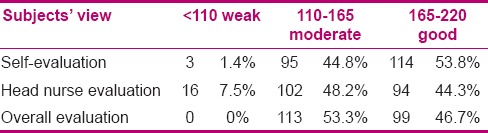
The participants consisted of 70.3% (175) female and 29.7% (75) male nurses, aged 34.15 ± 6.8 years, and their average nursing experience was 9 years. Table 1 demonstrates their demographic data [Table 1]. Spiritual intelligence score of participants was 297.20 ± 31.93 (min = 220, max = 377). The mean of nurses’ spiritual intelligence score was 3.1 ± 0.3 (range between 1 and 4). According to the results, 53.3% of nurses scored above the mean value [Chart 1]. With respect to the spiritual intelligence domains, the maximum score was related to divinity and slavery (3.5 ± 0.3) and the minimum was related to patience (205 ± 0.5). Kruskal–Wallis test showed a significant difference between spiritual intelligence domains [Chart 2]. The average of nurses’ clinical competency score was 167.1 ± 25.8 based on self-evaluation, 160.3 ± 31.3 based on head nurse evaluation, and 163.7 ± 25.8 based on overall evaluation. The mean of clinical competency score was 3.1 ± 0.5 based on self-evaluation, 2.9 ± 0.6 based on head nurse evaluation, and 0.3 ± 0.4 based on overall evaluation. Based on the total score, the maximum clinical competency was related to ethics and professional morality (3.1 ± 0.4). Most nurses (53.8%, 114 nurses) were having good level of clinical competency based on self-evaluation. Also, 48.2% (102 nurses) showed an average level based on head nurse evaluation and 43.3% (113 nurses) were at an average level based on total evaluation. There was significant correlation between the three clinical competency scores which is shown in Table 2. There was a significant relationship between nurses’ clinical competency and spiritual intelligence (P = 0.003, r = 0.487). No significant relationship was found between total clinical competency and personal and professional variables, except for the hospital. However, significant relationship was found between spiritual intelligence domains such as internal peace with marriage (P = 0.3), patience with age (P = 0.01), and patience with word (P = 0.04).
Table 1.
Nurses’ distribution based on hospital, ward, shift, work hours, and second work
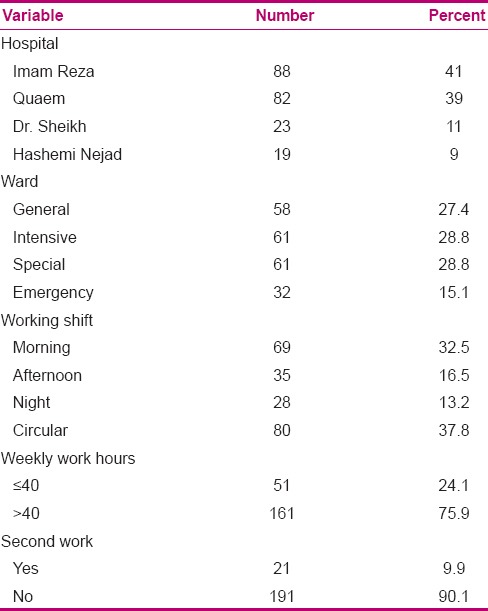
Chart 1.
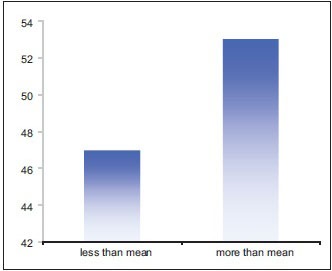
Spiritual intelligence mean score of nurses
Chart 2.
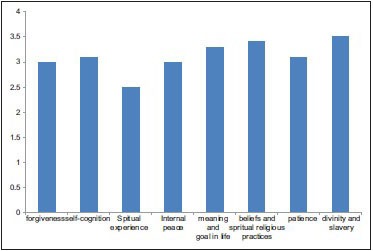
Nurses’ mean score of spiritual health
Table 2.
Nurses’ clinical competency level based on self-evaluation, head nurse evaluation, and overall evaluation
DISCUSSION
The study results showed that most of the subjects had high spiritual intelligence score. This result could not be unlikely for our society, where there is inclination and tendency toward religious and spiritual values. Lovasani et al. observed spirituality, job stress, organizational commitment, and job satisfaction among nurses in Tehran. They reported average to high level of spirituality,[1] which is in agreement with the findings of the current study.
Mazaheri et al. (2009), in their study on “nurses’ attitude toward spirituality and spiritual health in Razi educational psychiatric center,” showed high level of spirituality and spiritual health among nurses, while most of them were in third percentile.[2]
No study from Iran was found to measure nurses’ spiritual intelligence. Therefore, the results were compared with that of a study conducted in China. Yang and Mao [11] did not highlight spiritual intelligence among Chinese nurses. In their study, among 117 nurses, 82.9% had low and 17.1% had average spiritual intelligence and none of the nurses had high spiritual intelligence. Surely, there is limitation about this concept in countries like China.[3] According to Iranian studies, there is a general positive attitude toward spirituality, so the spiritual intelligence is above the average level in this country. The results of the present study show that 45% of nurses still had below average level of spirituality. Therefore, it is necessary to promote nurses’ spirituality due to its importance in nursing. It should be noted that the religious atmosphere in Iran could have influenced the responses to the questions, which would result in higher evaluation of nurses about themselves, whereas Yang's study did not have this situation. Further studies are needed to confirm this effect. Spiritual intelligence is not related to just divinity and slavery, but covers other domains such as forgiveness, patience, meaning and goal in life, spiritual experience, self-cognition, and internal peace. When spirituality affects all activities and behaviors, it could be considered valuable. Although being very intelligent spiritually (high level of spiritual intelligence), many people are not religious at all.
In this study, two methods, self-evaluation and head nurse evaluation, were applied to assess the clinical competency. In studies such as Bahreini et al.[7] and Liu et al.,[22] self-evaluation was used as a valid assessment tool for nurses’ clinical competency and based on their recommendations,[7,22] the head nurse evaluation was also used to assess the nurses’ clinical competency. In terms of clinical competency level, most of the nurses were at a good level based on self-evaluation. Most of the nurses were at an average level based on the head nurse evaluation, and also based on the total evaluation. Bahreini et al., in their study entitled “Clinical competency of nurses in university-affiliated hospitals in Bushehr by self-evaluation,” reported a good level of nurses’ clinical competency.[7] In Liu et al.'s study, a good level of clinical competency using self-evaluation method is reported.[22] The results of these two studies confirmed the present findings in terms of self-evaluation. Based on self-evaluation, 53.8% of nurses had a good level of clinical competency, which indicates that most of the nurses considered their competency to be at this level, regarding the present conditions. However, because of the important role of the clinical competency in patients’ health and quality of care, the average clinical competency based on head nurse evaluation is noticeable (44.8% from nurses’ points of view and 48.2% from head nurses’ points of view). This could be related to nursing educational systems. Lack of motivation, job distress, low quality of continuing education programs, lack of job satisfaction and interest, improper nurse/patient ratio, and lack of standards for clinical competency could be considered as the reasons of low level of clinical competency.[6] In the study of Ghalje et al. (2000) about the relationship between nurses’ clinical competency and patients’ satisfaction, it was shown that most nurses got average score of clinical competency, which is compatible with the head nurse score in the present study.[6] From nurses’ points of view and based on overall evaluation, most competencies were related to ethics and professional morality and interpersonal communication (3.2 ± 0.5), which is in agreement with Liu et al.'s study.[22] The maximum score in their study was related to interpersonal communication, whereas the remaining domains were at an eq ual level. However, the present study result was not compatible with that of Bahreini et al. (2007)[6] which reported the maximum score in management domain. It seems that the differences between scores are related to the different evaluation methods and various points of views and expectations of the individuals of their own roles.
To conclude, a significant correlation was found between spiritual intelligence and clinical competency (self-evaluation/head nurse evaluation/overall evaluation). Therefore, it could be predicted that increasing spiritual intelligence leads to clinical competency development. No study was found investigating the relationship between spiritual intelligence and clinical competency, but studies such as Bagheri et al. (2010)[6] on the relationship between spiritual intelligence and happiness, Shabani et al.,[20] Tabrizi (entitled “Effect of spiritual intelligence on mental health”),[23] and Amram (entitled “Effect of spiritual and excited intelligence on efficient management”)[13] have shown the effect of spiritual intelligence on the mental health in managers. So, it could be concluded that spirituality could be effective on adaptation and, consequently, on work life and promotion of performance. Also, the results showed a significant correlation between spiritual intelligence and clinical competency domain (self-evaluation, head nurse evaluation, overall evaluation) in which the effect of spiritual intelligence on all aspects and a higher competency of more intelligent people in all domains were indicated. Spiritual intelligence is not merely have a good feeling toward others, but is the way of treating, making decision in stressful conditions, and reacting in difficult situations. No significant relationship was found between personal and job variables. Also, there was not any relationship between nursing background and spiritual intelligence. In the present study, significant relationship was found between nursing background and patience, age and patience, and spiritual experi ences. Some life events such as death of relatives, spiritual trauma, etc., can lead to patience and spiritual experience. The cause of this relationship seems to be related to professional nature and to the way that the nurses face the stressful events such as death and spiritual trauma.
CONCLUSION
Clinical competency and its domains are related to spiritual intelligence. Spiritual intelligence is related to clinical competency and its domains. People with high spiritual intelligence have holistic considerations of life, solve their problems by positive moral characteristics, and adapt themselves effectively. As nurses face numerous problems and stress daily, the spiritual intelligence could develop their clinical competency and quality of care. It is recommended to improve the nurses’ spiritual intelligence during their education and by way of continuing education programs.
Footnotes
Source of Support: This article was extracted from a master thesis approved and financially supported by Mashhad University of Medical Sciences, Iran (No88749.)
Conflict of Interest: None declared.
REFERENCES
- 1.Meretoja R, Isoaho H, Leino-Kilpi H. Nurse competence scale: Development and psychometric testing. J Adv Nurs. 2004;47:124–33. doi: 10.1111/j.1365-2648.2004.03071.x. [DOI] [PubMed] [Google Scholar]
- 2.Toloei M, Dehghan Nayeri N, Faghihzadeh S, Sadooghi Asl A. The nurses’ motivating factors in relation to patient training. Hayat. 2006;12:43–51. [Google Scholar]
- 3.Memarian R, Salsali M, Vanaki Z, Ahmadi F, Hajizadeh E. Factors affecting the process of obtaining clinical competency. ZUMS Journal. 2006;14:40–9. [Google Scholar]
- 4.Mazlum R, Ghalje M, SA R. Thesis for master degree, Mashhad Uiversity of Medical Sciences. 2008. Survey relationship clinical competency and patient satisfaction from nursing service in hospital of Zahedan University. Persian. [Google Scholar]
- 5.Parsa Yekta Z, Ramezani Badr F, Khatoni A. Nursing students’ view points about their clinical competencies and it's achievement level. J Nurs Res. 2007;1:7–14. [Google Scholar]
- 6.Bagheri Nesami M, Rafiee F, Parvizi S, Esmaeili R. Concept analysis of competency in nursing: Qualitative research and delivery of a Hybrid model. Journal of Mazandaran University of Medical Sciences. 2008;67:1. [Google Scholar]
- 7.Bahreini M, Moathari M, Kavah MH. Self assessment of the clinical competence of nurses in a major educational hospital of Shiraz University of Medical Sciences. Iranian Journal of Medical Education. 2010;8:28–36. [Google Scholar]
- 8.Parsa-Yekta Z, Ahmadi F, Tabari R. Factors defined by nurses as influential upon the development of clinical competence. Journal of Gilan University of Medical Sciences. 2005;14:9–22. [Google Scholar]
- 9.Wolman RN. Thinking with your soul: Spiritual intelligence and why it matters. 1st ed. New York: Harmony books; 2001. pp. 270–88. [Google Scholar]
- 10.Yang KP. The spiritual intelligence of nurses in Taiwan. J Nurs Res. 2006;14:24–35. doi: 10.1097/01.jnr.0000387559.26694.0b. [DOI] [PubMed] [Google Scholar]
- 11.Yang K, Mao X. A study of nurses’ spiritual intelligence: A cross-sectional questionnaire survey. Int J Nurs Stud. 2007;44:999–1010. doi: 10.1016/j.ijnurstu.2006.03.004. [DOI] [PubMed] [Google Scholar]
- 12.Saghrvany S, Ghauor SM. Spirituality and their flourishing spiritual intelligence at work. Journal Community Management Group, Imam Reza University. 2009;8(1):27–31. Persian. [Google Scholar]
- 13.Karakas F. Spirituality and Performance in Organizations: A Literature review. Journal of Business Ethics. 2010;94:89–106. [Google Scholar]
- 14.Amram Y. The Contribution of Emotional and Spiritual intelligences to Effective Business Leadership. Doctoral dissertation, Institute of Transpersonal Psychology. 2009. [Last accessed 2014 Oct 25]. Available from: http://yosiamramnet/docs/EI_and_SI_in_Leadership_Amram_Dissert.pdf .
- 15.Amram Y. The Seven Dimensions of Spiritual Intelligence: An Ecumenical, Grounded Theory. Palo Alto, CA: CiteSeer; 2007. pp. 1–7. [Google Scholar]
- 16.Ashmos Donde P, Duchon D. Spirituality at work: A conceptualization and measure. Journal of Management Inquiry. 2000;9:134–45. [Google Scholar]
- 17.Ghobari bonab B, Salimi M, Selyani L, Noori Moghaddam S. [Intelligence spiritual] Andishe-e-Novin-e-Dini. 2007;3:125–47. [Google Scholar]
- 18.Jurkiewicz CL, Giacalone RA. A values framework for measuring the impact of workplace spirituality on organizational performance. Journal of Business Ethics. 2004;49:129–42. [Google Scholar]
- 19.Abdolah Zade H, Bagherpour M, Boujmehrani SM. Spritual Inteligence. Tehran: Ravansanji; 2009. p. 1388. [Google Scholar]
- 20.Sohrabi F, Fatali Nejad MR, Eskandari H. For degree postgraduate of phsychology. Allameh: Tabatabai University of Tehran; 2006. I. N. Concept of spiritual intelligence components and build an instrument to measure the Allameh Tabatabai University in Tehran between the 1387-1386. [Google Scholar]
- 21.Shabani J, Hassan S, Ahmad A, Baba M. Age as Moderated Influence on the Link of Spiritual and Emotional Intelligence with Mental Health in High School Students. Journal of American Science (J Am Sci) 2010;66:394–400. [Google Scholar]
- 22.Faribors B, Fatemeh A, Hamidreza H. The relationship between nurses’ spiritual intelligence and happiness in Iran. Procedia-Social and Behavioral Sciences (Procedia Soc. Behav. Sci) 2010;5:1556–61. [Google Scholar]
- 23.Liu M, Kunaiktikul W, Senaratana W, Tonmukayakul O, Eriksen L. Development of competency inventory for registered nurses in the People's Republic of China: Scale development. Int J Nurs Stud. 2007;44:805–13. doi: 10.1016/j.ijnurstu.2006.01.010. [DOI] [PubMed] [Google Scholar]