

Abstract
Colorectal cancer remains a major cause of cancer mortality in the Western world both in men and women. In this manuscript a concise overview and recommendations on adjuvant chemotherapy in colon cancer are presented. An executive team from the Hellenic Society of Medical Oncology was assigned to develop a consensus statement and guidelines on the adjuvant treatment of colon cancer. Fourteen statements on adjuvant treatment were subjected to the Delphi methodology. Voting experts were 68. All statements achieved a rate of consensus above than 80% (>87%) and none revised and entered to a second round of voting. Three and 8 of them achieved a 100 and an over than 90% consensus, respectively. These statements describe evaluations of therapies in clinical practice. They could be considered as general guidelines based on best available evidence for assistance in treatment decision-making. Furthermore, they serve to identify questions and targets for further research and the settings in which investigational therapy could be considered.
Keywords: Colon cancer, adjuvant chemotherapy, guidelines, Hellas, Cyprus
Introduction
Colorectal cancer (CC) remains a major cause of cancer mortality in Europe both in men and women. Notably, it is the second most common malignancy and cause of cancer death [1]. Despite the fact that its incidence and mortality still remain high, they both declined the last 40 years in the developed world [2]. Cancer prevention through screening tests and better treatment modalities are thought to be the major factors of this improvement. Furthermore, it was shown that patients with high-risk stage II and stage III CC who received treatment adhering to National Comprehensive Cancer Network guidelines had a survival benefit [3].
Focusing on better management and improved outcomes, the Hellenic Society of Medical Oncology (HeSMO) chose an executive team with proven experience in CC, assigned to develop a consensus statement and guidelines on the main topics, based on the review of literature and the principles of the evidence-based medicine: image staging, pathology, surgical treatment, chemotherapy in the adjuvant and metastatic setting and follow up. In the present study, the guidelines on the adjuvant chemotherapy for CC are presented. Consensus documents on: a) surgical treatment of rectal cancer; b) surgical treatment of CC; and c) management of metastatic colorectal disease are presented elsewhere.
HeSMO considers adherence to these guidelines to be voluntary. The ultimate determination regarding their application is to be made by the physician in light of each patient’s individual circumstances. In view of the consulting, these guidelines cannot form the basis for legal action or litigation for compliance or absence of compliance in the clinical practice setting. They could only be considered as general guidelines based on best available evidence for assistance in decision-making. Any person seeking to apply or consult the evidence-based series is expected to use independent medical judgment in the context of individual clinical circumstances or seek out the supervision of a qualified clinician. HeSMO disclaims any responsibility for their application or use in any way. In addition, these guidelines describe evaluations and administration of therapies in clinical practice; they cannot be assumed to apply to interventions performed in the context of clinical trials, given that such clinical studies are designed to test innovative management strategies in a disease for which better treatment is sorely needed. However, by reviewing and synthesizing the latest literature, this practice guideline serves to identify questions for further research and the settings in which investigational therapy should be considered.
Methodology
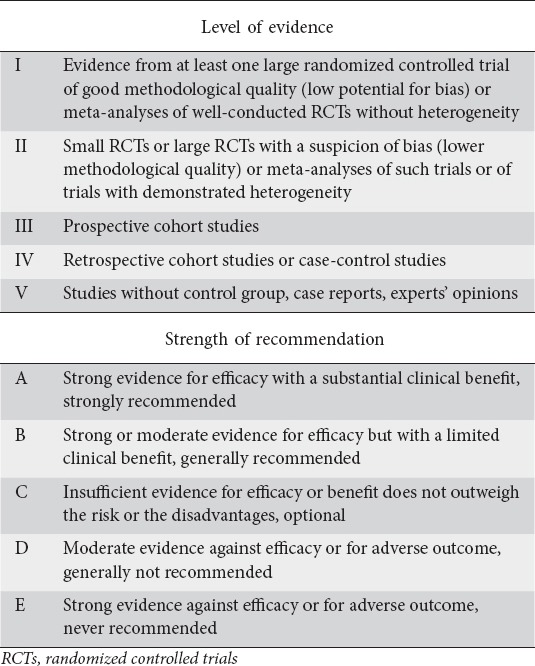
Through online communication of the executive team members drafting, statements, recommendations and amendments were processed from February 2011 to August 2013. Furthermore, a Hellenic-Cypriot task force meeting convened on May 5-6, 2011 in Heraklion, Crete. During the initial meeting an overview of main aspects in CC management was presented by one of the task force experts and comments were invited from the other group members. Levels of evidence (LOE) and grades of recommendation presented according to their strength, based on the version adopted by the ESMO Consensus Guidelines for CC (Table 1) [4]. Thereafter, consensus on statements was developed by using Delphi methodology [5].
Table 1.
Evidence levels and recommendation grades
Initially, one round of anonymous online voting and feedback by experts were conducted. Experts were identified from a systematic search of published literature and recommendations of other experts. The round of the online voting process started on November 10th, 2014 and ended on April 30th, 2015. At voting, options were: agree (AG), disagree (D), or abstain (A). Abstaining votes were intended for non-experts and did not count towards the overall percentage agreement (rate of voting consensus, ROVC). Statements achieving an agreement of 80% or more were considered as having reached consensus. Those statements achieving an agreement of less than 80% were considered as having achieved a low consensus and were planned to be a subject of a major revision and amendments by the members of the executive team. Thereafter, they would enter a second round of online voting process.
At the present document all statements are presented as recommendations of care. At the end of each recommendation the LOE and the strength of recommendation (SOR) are mentioned, followed by the ROVC. In this manuscript an overview and recommendations on the adjuvant chemotherapy in CC are presented.
Finally, fourteen statements entered the Delphi methodology and 68 experts participated in the online voting procedure. All statements achieved a rate of consensus above 80% (>87%) and none was revised or entered a second round of voting. Three and 8 statements achieved a 100% and an over 90% consensus, respectively. The median abstain rate was 8.2% (1.5-13.2).
Adjuvant therapy after primary tumor resection aims at reducing the risk of relapse and death by eliminating residual micro-metastatic disease[6]. It has to be started as soon as it is practically feasible and ideally not later than 8 weeks from surgery [7]. Treatment administration based on current evidence should last for 6 months. Shorter treatment duration (3 months) is currently under prospective evaluation by the International Duration Evaluation of Adjuvant Chemotherapy (IDEA) trial [8].
RECOMMENDATIONS
-
1.
Adjuvant chemotherapy has to be started within 3-8 weeks after surgery. It is questionable whether adjuvant chemotherapy commencing beyond 12 weeks is of any benefit (LOE II, SOR B), (ROVC: 95% - AG: 62, D: 3, A: 3)
-
2.
IDEA, a large international collaboration, will give a definitive answer regarding the duration of therapy in stage III patients (LOE I), (ROVC: 98% - AG: 60, D: 1, A: 7)
Currently, the majority of patients with stage I or II CC are treated and cured by surgery. The Pathology staging system used is based on American Joint Committee on Cancer, AJCC, 7th edition [9]. Chemotherapy should be considered for all patients with high-risk stage II disease (defined by the presence of at least one of the following risk factors: lymph nodes sampling <12, poorly differentiated tumor, vascular, lymphatic or perineural invasion, obstruction or perforation and pT4 stage) and stage III (Fig. 1). Moreover, the various therapeutic options need to be discussed with the patient on an individual basis taking into account the performance status, age, comorbidities and preferences, as well as tumor characteristics (pathological stage, grading, and overall risk of relapse).
Figure 1.
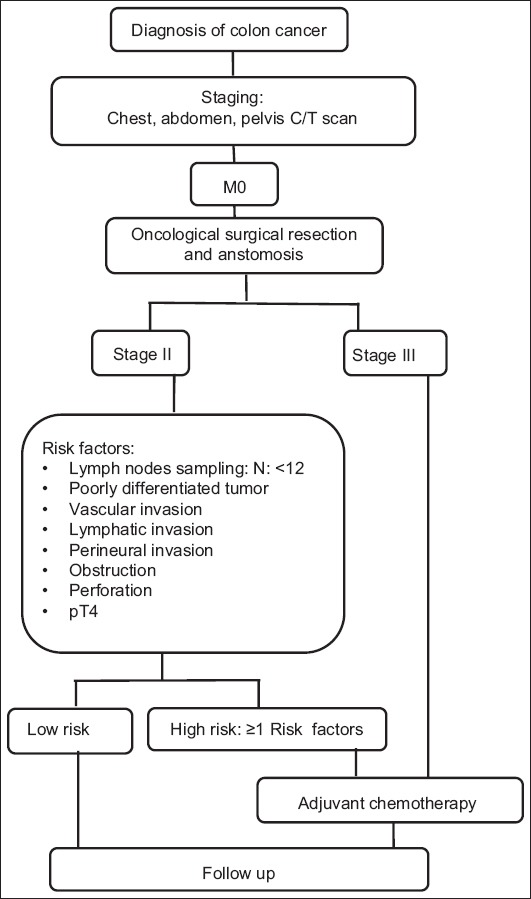
Colon cancer treatment algorithm
C/T, computed tomography
RECOMMENDATIONS
-
3.
Adjuvant chemotherapy should not be recommended for stage I disease (LOE I, SOR E), (ROVC: 100% - AG: 67, D: 0, A: 1)
-
4.
Adjuvant chemotherapy should be recommended to all patients with high-risk stage II and stage III disease (LOE I, SOR A), (ROVC: 88% - AG: 56, D: 8, A: 4)
There is no consensus about the survival benefit of postoperative chemotherapy in stage II CC [10]. Due to this uncertainty and its relative toxicity, cost, and inconvenience there is no clear justification for the administration of chemotherapy. For that reason it should not be routinely offered to unselected cases. Although direct evidence from randomized controlled trials does not exist for a survival benefit of adjuvant chemotherapy in high-risk stage II disease, oncologists who recommend therapy in this setting accept the results from stage III disease as indirect evidence of improvement. Moreover, because of a possible small absolute benefit with single agent 5-fluorouracil (5-FU), chemotherapy could be considered for medically fit high-risk stage II patients [11]. Combination chemotherapy with oxaliplatin could also be discussed for selected cases with high-risk features. However, it should be noted that the current definition of high-risk stage II CC is inadequate, given the fact that many patients deemed to be of average risk may have a recurrence and patients with high-risk features may not.
RECOMMENDATIONS
-
5.
For low-risk stage II disease, single agent fluoropyrimidine could be considered, but the absolute risk reduction for recurrence is limited (LOE II, SOR B), ROVC: 87% - AG: 55, D: 8, A: 5)
-
6.
High-risk stage II patients should be considered for adjuvant chemotherapy with single agent fluoropyrimidine or FOLFOX for a duration of 6 months (LOE II, SOR B), (ROVC: 87%-AG: 54, D: 8, A: 6)
For stage III disease, combination chemotherapy with a backbone of fluoropyrimidine and oxaliplatin (FLOX, FOLFOX, XELOX) is superior when compared to single agent 5-FU, in terms of disease-free survival (DFS) and overall survival (OS), and is the current standard of care [12,13]. It is well established that adjuvant therapy in CC reduces the risk of death by 10-15% in stage III with fluoropyrimidines alone plus a further 4-5% with oxaliplatin-containing combinations [14,15]. Furthermore, with a 10-year follow up in the Multicenter International Study of oxaliplatin/5-FU/leucovorin (LV) in the Adjuvant Treatment of Colon Cancer (MOSAIC), benefit of oxaliplatin as adjuvant therapy for stage III disease is preserved for DFS and OS [16]. The results for OS and DFS for stage II patients are eagerly awaited.
RECOMMENDATIONS
-
7.
Stage III patients should receive fluoropyrimidine- and oxaliplatin-based adjuvant chemotherapy for a duration of 6 months (LOE I, SOR A), (ROVC= 97% - AG: 58, D: 2, A: 8)
-
8.
Whenever fluoropyrimidine- and oxaliplatin-based combination is contraindicated, single agent fluoropyrimidine could be considered (LOE II, SOR B), (ROVC: 98% - AG: 60, D: 1, A: 7)
Certainly, there are several reports giving conflicting evidence on the degree of oxaliplatin benefits in the elderly patients. Efficacy and safety of adjuvant XELOX/FOLFOX versus LV/5-FU or capecitabine were compared with respect to age in several trials and pooled analysis. In the National Surgical Adjuvant Breast and Bowel Project (NSABP) C-07 trial, patients ≥70 years of age failed to derive a statistically significant benefit from the addition of oxaliplatin [17]. Furthermore, in the MOSAIC trial, the DFS and OS benefits in the same group of patients were similar to those of younger patients after a 3-year follow up, but were lost later due to deaths from other causes and different management or outcome of relapses [18]. In addition, ACCENT database analysis suggests that patients ≥70 years of age may not receive additional benefit from combination chemotherapy as opposed to single agent fluoropyrimidine [19]. On the other hand, in the XELOXA trial benefits were maintained although to a lesser degree with a hazard ratio for survival of 0.94 [20]. Analysis of the X-ACT trial showed improved outcomes of capecitabine when compared with bolus 5-FU/LV in patients ≥70 years and at least equivalency in stage III disease [21]. A recently published pooled analysis of NSABP C-08, XELOXA, X-ACT, and AVANT support the administration of combined oxaliplatin/5-FU in stage III patients irrespective of their age and comorbidity [22]. However, even in this highly selected clinical trial patient population, the benefit was modestly attenuated in patients ≥70 years of age. In addition, there are potential concerns about the methodology used, as it involves the indirect comparison of treatments not randomized against each other.
Available data from numerous retrospective studies strongly support the assessment of microsatellite instability (MSI) testing to become routine clinical practice [23]. Twenty five percent of tumors proximal to the splenic flexure will be deficient mismatch repair, and, knowing that such tumors have a 50% lower risk for primary tumor recurrence, will help guide the use of chemotherapy in this subset of patients [24]. These patients should not be excluded from receiving chemotherapy if this is otherwise indicated (e.g. for high-risk pathology such as T4 stage, lympho-vascular invasion, neural invasion). Regarding the value of MSI status there are still grey zones and questions to be answered. In addition, routine testing would aid identification of insidious hereditary non-polyposis CC in individuals showing loss of staining of hMSH2 or hMLH1, in the absence of BRAF mutations.
RECOMMENDATIONS
-
9.
Patients older than 70 years of age with high risk for recurrence could be considered for adjuvant chemotherapy with single agent fluoropyrimidine for 6 months. Although combination treatment with oxaliplatin is an option for stage III disease, it should be noted that the additional benefit conferred is questionable for this age group (LOE I, SOR B), (ROVC: 97% - AG: 62, D: 2, A: 4)
-
10.
For stage II patients MSI testing should be strongly considered as it can have a significant impact on prognosis and outcome (LOE II, SOR B), (ROVC: 98% - AG: 59, D: 1, A: 8)
-
11.
Infusional 5-FU should be preferred over bolus 5-FU (LOE II, SOR B), (ROVC: 93% - AG: 55, D: 4, A: 9)
-
12.
Oral capecitabine is an effective alternative to intravenous fluorouracil plus LV in the adjuvant treatment of colon cancer (LOE II, SOR B), (ROVC: 100% - AG: 62, D: 0, A: 6)
Infusional 5-FU should be preferred compared to bolus 5-FU due to better tolerability, although the need for a port device and its potential associated complications (thrombosis, lung embolism, infection) should be also considered.
There is no evidence suggesting that infusional 5-FU is superior regarding efficacy to bolus 5-FU in the adjuvant setting [25]. The use of capecitabine in combination with oxaliplatin, which does not require central venous access, is another option.
Irinotecan administration in combination with 5-FU was also studied in several trials (CALGB 89803, PETACC3, ACCORD02/FFCD9802, N0147) [26-29]. The addition of irinotecan did not translate into improved outcomes.
RECOMMENDATIONS
-
13.
Irinotecan combinations cannot be recommended for use in the adjuvant setting (LOE I, SOR E), (ROVC: 98% - AG: 58, D: 1, A: 9)
In the era of targeted therapy, NSABP C-08 and AVANT trials evaluated the addition of Bevacizumab to FOLFOX/XELOX combinations for stage II/III disease, but no benefit was demonstrated [30,31]. Also, addition of cetuximab to FOLFOX combination in the adjuvant setting did not improve the outcomes [32].
RECOMMENDATIONS
-
14.
Monoclonal antibodies [anti-vascular endothelial growth factor (bevacizumab) or anti-epidermal growth factor receptor (cetuximab/panitumumab)] cannot be recommended for use in the adjuvant setting (LOE I, SOR E), (ROVC: 100% - AG: 60, D: 0, A: 8)
Concluding remarks
Adjuvant chemotherapy should be recommended for all patients with high-risk stage II and stage III disease. For stage III patients the benefit is clear with the administration of fluoropyrimidine- and oxaliplatin-based adjuvant chemotherapy. Patients older than 70 years of age with high risk for recurrence could be considered for adjuvant chemotherapy with single agent fluoropyrimidine, although combination treatment with oxaliplatin is an option for stage III disease. Irinotecan, bevacizumab or cetuximab combinations should not be recommended for use in the adjuvant setting.
Biography
B.O.C. Oncology Center, Nicosia, Cyprus; University of Crete, Heraklion, Hellas; Metropolitan Hospital, Piraeus, Hellas; Venizeleion Hospital, Heraklion, Hellas; Koutlibaneion Hospital, Larissa, Hellas; Bioclinic, Thessaloniki, Hellas; Interbalcan Medical Center, Thessaloniki, Hellas; Chelsea and Westminster NHS Foundation Trust, London, UK; Dexeus University Institute, Barcelona, Spain; Iaso General Hospital, Athens, Hellas; University of Patras, Patra, Hellas; Hippokration Hospital, Athens, Hellas; University of Ioannina, Ioannina, Hellas; Theageneio Cancer Hospital, Thessaloniki, Hellas; Agioi Anargyroi Hospital, Athens, Hellas; Iatriko Medical Center, Athens, Hellas; George Gennimatas General Hospital, Athens, Hellas; InterClinic Hospital, Herakleion Crete, Hellas; Metaxas Atnicancer Hospital, Piraeus, Hellas
Footnotes
Conflict of Interest: None
References
- 1.Ferlay J, Steliarova-Foucher E, Lortet-Tieulent J, et al. Cancer incidence and mortality patterns in Europe: estimates for 40 countries in 2012. Eur J Cancer. 2013;49:1374–1403. doi: 10.1016/j.ejca.2012.12.027. [DOI] [PubMed] [Google Scholar]
- 2.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin. 2015;65:5–29. doi: 10.3322/caac.21254. [DOI] [PubMed] [Google Scholar]
- 3.Boland GM, Chang GJ, Haynes AB, et al. Association between adherence to National Comprehensive Cancer Network treatment guidelines and improved survival in patients with colon cancer. Cancer. 2013;119:1593–1601. doi: 10.1002/cncr.27935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Schmoll HJ, van Cutsem E, Stein A, et al. ESMO Consensus Guidelines for management of patients with colon and rectal cancer. a personalized approach to clinical decision making. Ann Oncol. 2012;23:2479–2516. doi: 10.1093/annonc/mds236. [DOI] [PubMed] [Google Scholar]
- 5.Rowe GW. The Delphi technique as a forecasting tool: issues and analysis. Int J Forecast. 1999;4:353–375. [Google Scholar]
- 6.Saltz LB. Adjuvant therapy for colon cancer. Surg Oncol Clin N Am. 2010;19:819–827. doi: 10.1016/j.soc.2010.07.005. [DOI] [PubMed] [Google Scholar]
- 7.Biagi JJ, Raphael MJ, Mackillop WJ, et al. Association between time to initiation of adjuvant chemotherapy and survival in colorectal cancer: a systematic review and meta-analysis. JAMA. 2011;305:2335–2342. doi: 10.1001/jama.2011.749. [DOI] [PubMed] [Google Scholar]
- 8.Andre T, Iveson T, Labianca R, et al. The IDEA (International Duration Evaluation of Adjuvant Chemotherapy) Collaboration: prospective combined analysis of phase III trials investigating duration of adjuvant therapy with the FOLFOX (FOLFOX4 or modified FOLFOX6) or XELOX (3 versus 6 months) regimen for patients with stage III colon cancer: trial design and current status. Curr Colorectal Cancer Rep. 2013;9:261–269. doi: 10.1007/s11888-013-0181-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Edge SB, Byrd DR, Compton CC, Fritz AG, Greene FL, Trotti A. AJCC cancer staging manual. 7th ed. New York, NY: Springer; 2010. [Google Scholar]
- 10.Gill S, Loprinzi CL, Sargent DJ, et al. Pooled analysis of fluorouracil-based adjuvant therapy for stage II and III colon cancer: who benefits and by how much? J Clin Oncol. 2004;22:1797–1806. doi: 10.1200/JCO.2004.09.059. [DOI] [PubMed] [Google Scholar]
- 11.Gray R, Barnwell J, McConkey C, et al. Adjuvant chemotherapy versus observation in patients with colorectal cancer: a randomised study. Lancet. 2007;370:2020–2029. doi: 10.1016/S0140-6736(07)61866-2. [DOI] [PubMed] [Google Scholar]
- 12.Andre T, Boni C, Mounedji-Boudiaf L, et al. Oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment for colon cancer. N Engl J Med. 2004;350:2343–2351. doi: 10.1056/NEJMoa032709. [DOI] [PubMed] [Google Scholar]
- 13.Schmoll HJ, Twelves C, Sun W, et al. Effect of adjuvant capecitabine or fluorouracil, with or without oxaliplatin, on survival outcomes in stage III colon cancer and the effect of oxaliplatin on post-relapse survival: a pooled analysis of individual patient data from four randomised controlled trials. Lancet Oncol. 2014;15:1481–1492. doi: 10.1016/S1470-2045(14)70486-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Labianca R, Nordlinger B, Beretta GD, et al. Early colon cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2013;24(Suppl 6):vi64–vi72. doi: 10.1093/annonc/mdt354. [DOI] [PubMed] [Google Scholar]
- 15.Sanoff HK, Carpenter WR, Martin CF, et al. Comparative effectiveness of oxaliplatin vs non-oxaliplatin-containing adjuvant chemotherapy for stage III colon cancer. J Natl Cancer Inst. 2012;104:211–227. doi: 10.1093/jnci/djr524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.André T, De Gramont A, Chibaudel B, et al. MOSAIC Study: actualization of overall survival (OS) with 10 years follow up and evaluation of BRAF. By GERCOR and MOSAIC investigators. Ann Oncol. 2014;25(Suppl 4):iv169. [Google Scholar]
- 17.Kuebler JP, Wieand HS, O’Connell MJ, et al. Oxaliplatin combined with weekly bolus fluorouracil and leucovorin as surgical adjuvant chemotherapy for stage II and III colon cancer: results from NSABP C-07. J Clin Oncol. 2007;25:2198–2204. doi: 10.1200/JCO.2006.08.2974. [DOI] [PubMed] [Google Scholar]
- 18.Andre T, Boni C, Navarro M, et al. Improved overall survival with oxaliplatin, fluorouracil, and leucovorin as adjuvant treatment in stage II or III colon cancer in the MOSAIC trial. J Clin Oncol. 2009;27:3109–3116. doi: 10.1200/JCO.2008.20.6771. [DOI] [PubMed] [Google Scholar]
- 19.McCleary NJ, Meyerhardt JA, Green E, et al. Impact of age on the efficacy of newer adjuvant therapies in patients with stage II/III colon cancer: findings from the ACCENT database. J Clin Oncol. 2013;31:2600–2606. doi: 10.1200/JCO.2013.49.6638. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Haller DG, Tabernero J, Maroun J, et al. Capecitabine plus oxaliplatin compared with fluorouracil and folinic acid as adjuvant therapy for stage III colon cancer. J Clin Oncol. 2011;29:1465–1471. doi: 10.1200/JCO.2010.33.6297. [DOI] [PubMed] [Google Scholar]
- 21.Twelves C, Scheithauer W, McKendrick J, et al. Capecitabine versus 5-fluorouracil/folinic acid as adjuvant therapy for stage III colon cancer: final results from the X-ACT trial with analysis by age and preliminary evidence of a pharmacodynamic marker of efficacy. Ann Oncol. 2012;23:1190–1197. doi: 10.1093/annonc/mdr366. [DOI] [PubMed] [Google Scholar]
- 22.Haller DG, O’Connell MJ, Cartwright TH, et al. Impact of age and medical comorbidity on adjuvant treatment outcomes for stage III colon cancer: a pooled analysis of individual patient data from four randomized, controlled trials. Ann Oncol. 2015;26:715–724. doi: 10.1093/annonc/mdv003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Sinicrope FA, Foster NR, Thibodeau SN, et al. DNA mismatch repair status and colon cancer recurrence and survival in clinical trials of 5-fluorouracil-based adjuvant therapy. J Natl Cancer Inst. 2011;103:863–875. doi: 10.1093/jnci/djr153. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sargent DJ, Marsoni S, Monges G, et al. Defective mismatch repair as a predictive marker for lack of efficacy of fluorouracil-based adjuvant therapy in colon cancer. J Clin Oncol. 2010;28:3219–3226. doi: 10.1200/JCO.2009.27.1825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Andre T, Colin P, Louvet C, et al. Semimonthly versus monthly regimen of fluorouracil and leucovorin administered for 24 or 36 weeks as adjuvant therapy in stage II and III colon cancer: results of a randomized trial. J Clin Oncol. 2003;21:2896–2903. doi: 10.1200/JCO.2003.10.065. [DOI] [PubMed] [Google Scholar]
- 26.Huang J, Nair SG, Mahoney MR, et al. Comparison of FOLFIRI with or without cetuximab in patients with resected stage III colon cancer;NCCTG (Alliance) intergroup trial N0147. Clin Colorectal Cancer. 2014;13:100–109. doi: 10.1016/j.clcc.2013.12.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Saltz LB, Niedzwiecki D, Hollis D, et al. Irinotecan fluorouracil plus leucovorin is not superior to fluorouracil plus leucovorin alone as adjuvant treatment for stage III colon cancer: results of CALGB 89803. J Clin Oncol. 2007;25:3456–3461. doi: 10.1200/JCO.2007.11.2144. [DOI] [PubMed] [Google Scholar]
- 28.Van Cutsem E, Labianca R, Bodoky G, et al. Randomized phase III trial comparing biweekly infusional fluorouracil/leucovorin alone or with irinotecan in the adjuvant treatment of stage III colon cancer: PETACC-3. J Clin Oncol. 2009;27:3117–3125. doi: 10.1200/JCO.2008.21.6663. [DOI] [PubMed] [Google Scholar]
- 29.Ychou M, Raoul JL, Douillard JY, et al. A phase III randomised trial of LV5FU2 +irinotecan versus LV5FU2 alone in adjuvant high-risk colon cancer (FNCLCC Accord02/FFCD9802) Ann Oncol. 2009;20:674–680. doi: 10.1093/annonc/mdn680. [DOI] [PubMed] [Google Scholar]
- 30.Allegra CJ, Yothers G, O’Connell MJ, et al. Phase III trial assessing bevacizumab in stages II and III carcinoma of the colon: results of NSABP protocol C-08. J Clin Oncol. 2011;29:11–16. doi: 10.1200/JCO.2010.30.0855. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.de Gramont A, Van Cutsem E, Schmoll HJ, et al. Bevacizumab plus oxaliplatin-based chemotherapy as adjuvant treatment for colon cancer (AVANT): a phase 3 randomised controlled trial. Lancet Oncol. 2012;13:1225–1233. doi: 10.1016/S1470-2045(12)70509-0. [DOI] [PubMed] [Google Scholar]
- 32.Alberts SR, Sargent DJ, Nair S, et al. Effect of oxaliplatin, fluorouracil, and leucovorin with or without cetuximab on survival among patients with resected stage III colon cancer: a randomized trial. JAMA. 2012;307:1383–1393. doi: 10.1001/jama.2012.385. [DOI] [PMC free article] [PubMed] [Google Scholar]