

Abstract
Cholangiocarcinoma and pancreatic head cancer are still linked with extremely high 5-year mortality in the western world. The management of such patients is complex and typically requires a multidisciplinary approach in a tertiary care center. Interventional radiology offers minimally invasive, image-guided treatment for a variety of diseases and conditions. Regarding patients with malignant biliary obstruction, IR options are considered for more than two decades as a valid management tool for both operable and non-operable cases. The options include placement of percutaneous transhepatic biliary drains, preoperative embolization of the portal vein and deployment of covered and uncovered biliary stents. The purpose of this review is to describe the current evidence in this continuously evolving field.
Keywords: Malignant biliary obstruction, percutaneous interventions, transhepatic biliary drainage, biliary stents
Introduction
Malignant jaundice occurs when there is a blockage of the biliary tree, either by direct tumor infiltration or by external compression. The underlying malignancies in the vast majority of cases are cholangiocarcinoma and adenocarcinoma of the pancreatic head [1]. Other tumors of the area may be gallbladder or gastric cancer, intrahepatic metastases or metastatic hilar lymph nodes. In all cases, dilatation of the biliary ducts occurs and the bile is prevented from flowing towards the duodenum. The main presentation symptom is jaundice, however in some cases of advanced disease cholangitis and sepsis may also occur. The management of such patients typically requires a multidisciplinary setting in a tertiary care center, involving gastroenterologists, hepato-pancreato biliary surgeons, oncologists and radiologists. The purpose of this review is to describe the role of interventional radiology (IR) in the management of such complex patients.
Management of patients with malignant biliary obstruction
The first-line imaging examination for patients presenting with jaundice is usually an abdominal ultrasound (US) scan that confirms the dilatation of the biliary ducts; US is usually followed by cross sectional imaging that may be either computed tomography or magnetic resonance imaging to delineate the nature of the occlusion (benign or malignant). When a suspicious lesion is confirmed the next step will be to obtain tissue diagnosis. This is usually feasible with endoscopic US (EUS) guidance and fine needle aspiration of cells from the lesion. The multidisciplinary meeting will decide on the stage the disease and define weather the lesion may be excised surgically or not. IR has an important role in both operable and non-operable lesions.
The role of IR in the management of operable lesions
Percutaneous biliary drainage
If a lesion may be excised surgically, preoperative decompression of the biliary tree and normalization of the levels of bilirubin and of liver function are required. In such cases, placement of a percutaneous transhepatic external biliary drain is considered as the best option. The drain needs to be external only to limit the risk of ascending cholangitis that may jeopardize surgical treatment.
A percutaneous transhepatic cholangiogram is usually performed with the use of a 21G needle system, preferably under US guidance. Once access in the biliary tree is obtained, contrast injection under fluoroscopy delineates the level of the occlusion. Then a 0.021” microwire is advanced through the 21G needle into the biliary tree and over this a 0.035” coaxial system is advanced; the 0.021” microwire is then exchanged for a 0.035” glidewire usually of the stiff type. Further contrast injection may follow at this stage if the patient is not septic. If the patient is septic, contrast injection needs to be very limited due to the risk of septicemia. Then, over the 0.035” guidewire, a multihole all-purpose locking pigtail drain catheter is inserted and connected to an external bag (Fig. 1A). The drain needs to be fixed to the skin as it may easily be dislodged. If histology under EUS guidance is not feasible, a transbiliary biopsy may also be obtained from the transhepatic access prior to drain insertion (Fig. 1B).
Figure 1.
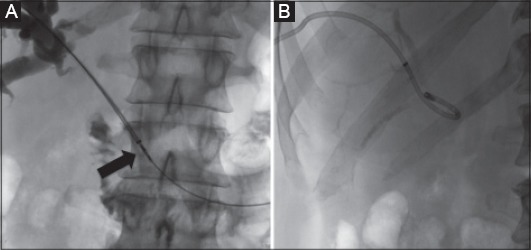
(A) Cholangiogram revealing occlusion of the common hepatic and common bile ducts. The occluded segment is recanalized and a biopsy forceps is advanced within the area of the tumor (arrow). A safety wire is advanced to the duodenum parallel to the biopsy device. (B) An 8.5Fr external drain is advanced
Percutaneous transhepatic biliary drainage may lead to complications such as bleeding, sepsis, peritonitis and bile leak. Procedure-related death is reported between 0.6-5.6% [2-5]. The British Society of Interventional Radiology (BSIR) published a registry in 2011 [6], in which factors responsible for increased mortality of the procedure were noted. The registry included 610 patients who received percutaneous biliary drainage for malignant biliary obstruction. The total mortality reported was 19.8% (121/610), mainly attributed to the presence of ascites, advanced disease status and the poor general conditions of the patients included in the registry. However, another factor was that not all cases were performed is tertiary care specialist centers. In the effort to perform a risk stratification analysis Tapping et al [7] published their experience on 704 patients with obstructive jaundice who received percutaneous transhepatic biliary drainage over a 7-year period and concluded that a scoring system using mainly the following factors: high white cell count; high C-reactive protein; low hemoglobin; and high bilirubin may be a reliable predictor of complications and mortality. In this study performed in a tertiary care center the procedure-related mortality rate was 2%.
Portal vein embolization (PVE)
In case of large lesions, where a significant percentage of the liver parenchyma needs to be excised, PVE may be considered as necessary in addition to the drainage of the bile ducts. The embolization of the portal vein induces hypertrophy of the contralateral liver lobe to achieve a satisfactory residual percentage of liver parenchyma post-excision. Technically, PVE is performed after percutaneous US-guided access to the portal system. Usually a 21G needle is used as described for the biliary tree access, and then the system is upsized to 0.035”. Embolization may be performed with the use of coils, plugs, particles or histoacryl glue [8] (Fig. 2). PVE and drainage may be performed in a sequential approach as a two-stage procedure or as recently published study by Guiu et al [9] during the same session.
Figure 2.

Fluoroscopic picture showing contrast cast after embolization of the right portal vein branches. A right external and a left internal-external drain is also placed prior to surgical resection of the right liver lobe
The role of IR in the management of non-operable lesions
In non-operable lesions palliation is required with the use of stents. Drainage of the biliary tree is of paramount importance for the quality of life of the oncologic patients as normal liver function is required for the administration of chemotherapy [10]. Prior to the era of cross-sectional imaging, palliation is such cases was historically performed surgically through an exploratory laparotomy which, among others, was necessary to define the stage of disease. However, for more than two decades accurate staging is now performed with cross sectional imaging and such patients are treated with the use of stents inserted either endoscopically or percutaneously [11,12].
Bare stents
Bare self-expandable metallic stents (SEMS) were introduced in the clinical practice more than 25 years ago. They were mainly developed to overcome problems of the initially used plastic stents. The main problem of plastic stents was their relative small lumen. The size of plastic stents is limited to 12Fr when placed endoscopically (this is the maximum size that may fit though the accessory channel of the endoscope), or to 14Fr when placed percutaneously, whereby the created large intrahepatic tract can be challenging to seal. On the other hand, SEMS are typically mounted over a 6 or 7Fr carrying catheter, however they reach a lumen of up to 30 Fr when deployed. This way, SEMS offer significantly longer patency times than plastic stents [13,14]. The initial cost of SEMS was significantly higher than the cost of the plastic stents, however their placement was considered as cost-effective due to the longer patency [15]. More recent studies have confirmed the results of the mid 90’s. In particular, two systematic reviews confirm that that SEMS are less likely to get occluded compared to plastic stents without significant difference on technical failure, complication rate and mortality [16,17]. The superiority of SEMS over plastic ones is also confirmed in two recently published randomized controlled trials and a meta-analysis [18-20].
Bare SEMS are made from either stainless steel or nitinol and are formed from a mesh placed in a tubular fashion. The fact that a mesh is used permits to the endoprosthesis to be embedded into the biliary wall [21] and diminishes the risk of migration. However, within the next six months, neoplastic tissue is growing through the mesh of the stent (ingrowth) and the endoprosthesis gets occluded, thereby requiring an additional stent to be deployed. The rate of this process has been reported in the range of 20-50% [13-15,22]. In order to limit ingrowth, covered biliary stents were developed.
Covered biliary stents
Covered biliary stents are also made from a tubular mesh, however, this is covered by a thin membrane [23-28]. Covered stents are not integrated within the biliary wall and can be removed if so required. This is also a disadvantage because migration may occur. Therefore covered stents with anti-migrational mechanism were designed and integrated in the clinical practice [29-31]. The covering material may be polyurethane, silicone or ePTFE/FEP. The latter has shown satisfactory results in preventing from tumor ingrowth [32]. There are some technical limitations in the deployment of covered stents in relation with the location of the cystic duct that should not be covered by the membrane in order to avoid cholecystitis (Fig. 3). Therefore, a measuring pigtail needs to be used in order to measure the exact length of the lesion prior to deployment of a covered stent. The carrying catheter of the covered stents is usually larger (10Fr) than the one of the bare stents (6-7Fr).
Figure 3.
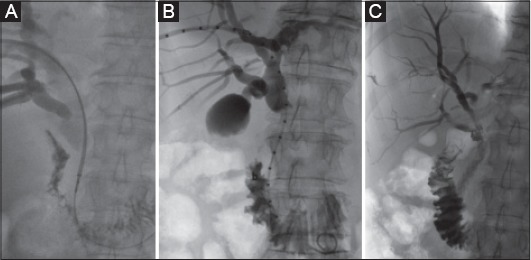
(A) Transbiliary biopsy of a low common bile duct lesion. (B) A measuring pigtail is inserted to delineate the size of the required stent. (C) A 10x80 mm covered stent with anchoring fins was deployed caudally to the origin of the cystic duct
Hilar lesions
For hilar lesions (Bismuth types III and IV) bilateral access and simultaneous deployment of two stents is required in a “Y” configuration. The stents used in such occasions are usually bare, however covered stents may also be used as far as the cystic duct is not obstructed. In case bilateral access is not feasible, then bare stents in a “7” configuration is suggested. There are specifically designed stents with less dense struts in the central portion that permit the insertion of another stent through their mesh.
Endobiliary radiofrequency ablation (RFA)
RFA is an established method of tumor treatment based on high frequency rapidly alternating electric current [33,34]. The energy is usually delivered through an electrode that is placed under imaging guidance in the tumoral tissue. There has been a lot of interest lately on the use of biliary intraductal RFA devices initially in animal experiments and then in patients with non-resectable pancreatic head adenocarcinoma or cholangiocarcinoma [35,36]. In the initial studies the device used was placed endoscopically, however in the study of Mizandari et al [37] the authors describe a percutaneous transhepatic placement in 39 patients with malignant biliary stricture. In all patients, a bare metallic stent was deployed in the stenotic area post-ablation without major complications. However, long-term results are required to evaluate further this innovative technique.
Concluding remark
IR offers a valid minimally invasive therapeutic option for both operable and non-operable cases with malignant biliary obstruction and plays a significant role in the management of such patients in a tertiary care multidisciplinary setting.
Biography
University Hospital of Heraklion, Crete, Greece; Cambridge University Hospitals, UK; Imaging University Hospital Sf. Spiridon, Iasi, Romania; Democritus University of Thrace, Alexandroupolis, Greece
Footnotes
Conflict of Interest: None
References
- 1.Jaganmohan S, Lee JH. Self-expandable metal stents in malignant biliary obstruction. Expert Rev Gastroenterol Hepatol. 2012;6:105–114. doi: 10.1586/egh.11.95. [DOI] [PubMed] [Google Scholar]
- 2.Mueller PR, van Sonnenberg E, Ferrucci JT., Jr Percutaneous biliary drainage: technical and catheter-related problems in 200 procedures. AJR Am J Roentgenol. 1982;138:17–23. doi: 10.2214/ajr.138.1.17. [DOI] [PubMed] [Google Scholar]
- 3.Yee AC, Ho CS. Complications of percutaneous biliary drainage: benign vs malignant diseases. AJR Am J Roentgenol. 1987;148:1207–1209. doi: 10.2214/ajr.148.6.1207. [DOI] [PubMed] [Google Scholar]
- 4.Clark RA, Mitchell SE, Colley DP, Alexander E. Percutaneous catheter biliary decompression. AJR Am J Roentgenol. 1981;37:503–509. doi: 10.2214/ajr.137.3.503. [DOI] [PubMed] [Google Scholar]
- 5.Carrasco CH, Zornoza J, Bechtel WJ. Malignant biliary obstruction: complications of percutaneous biliary drainage. Radiology. 1984;152:343–346. doi: 10.1148/radiology.152.2.6739796. [DOI] [PubMed] [Google Scholar]
- 6.Uberoi R, Das N, Moss J, Robertson I. British Society of Interventional Radiology: biliary drainage and stenting registry (BDSR) Cardiovasc Interv Radiol. 2012;35:127–138. doi: 10.1007/s00270-011-0103-4. [DOI] [PubMed] [Google Scholar]
- 7.Tapping C, Byass O, Cast J. Percutaneous transhepatic biliary drainage (PTCD) with or without stenting- complications, re-stent rate and new risk stratification score. Eur Radiol. 2011;21:1948–1955. doi: 10.1007/s00330-011-2121-7. [DOI] [PubMed] [Google Scholar]
- 8.Geisel D, Malinowski M, Powerski M, et al. Improved hypertrophy of future remnant liver after portal vein embolization with plugs, coils and particles. Cardiovasc Intervent Radiol. 2013;37:1251–1258. doi: 10.1007/s00270-013-0810-0. [DOI] [PubMed] [Google Scholar]
- 9.Guiu B, Bize P, Demartines N, et al. Simultaneous biliary drainage and portal vein embolization before extended hepatectomy for hilar cholangiocarcinoma: preliminary experience. Cardiovasc Intervent Radiol. 2014;37:698–704. doi: 10.1007/s00270-013-0699-7. [DOI] [PubMed] [Google Scholar]
- 10.Castaño R, Lopes TL, Alvarez O, Calvo V, Luz LP, Artifon EL. Nitinol biliary stent versus surgery for palliation of distal malignant biliary obstruction. Surg Endosc. 2010;24:2092–2098. doi: 10.1007/s00464-010-0903-7. [DOI] [PubMed] [Google Scholar]
- 11.Lee BH, Choe DH, Lee JH, Kim KH, Chin SY. Metallic stents in malignant biliary obstruction: prospective long-term clinical results. AJR Am J Roentgenol. 1997;168:741–745. doi: 10.2214/ajr.168.3.9057527. [DOI] [PubMed] [Google Scholar]
- 12.Gwon DI, Ko GY, Kim JH, et al. Percutaneous bilateral metallic stent placement using a stentin-stent deployment technique in patients with malignant hilar biliary obstruction. AJR Am J Roentgenol. 2013;200:909–914. doi: 10.2214/AJR.12.8780. [DOI] [PubMed] [Google Scholar]
- 13.Davids P, Groen A, Rauws E, Tytgat G, Huidregtse K. Randomized trial of self-expanding metal stents versus polyethylene stents for distal malignant biliary obstruction. Lancet. 1992;340:1488–1492. doi: 10.1016/0140-6736(92)92752-2. [DOI] [PubMed] [Google Scholar]
- 14.Knyrim K, Wagner H, Pausch J, Vakil N. A prospective, randomized, controlled trial of metal stents for malignant obstruction in the common bile-duct. Endoscopy. 1993;25:207–212. doi: 10.1055/s-2007-1010294. [DOI] [PubMed] [Google Scholar]
- 15.Lammer J, Hausegger KA, Fluckiger F, et al. Common bile duct obstruction due to malignancy: Treatment with plastic versus metal stents. Radiology. 1996;201:167–172. doi: 10.1148/radiology.201.1.8816539. [DOI] [PubMed] [Google Scholar]
- 16.Soderlund C, Linder S. Covered metal versus plastic stents for malignant common bile duct stenosis: a prospective, randomized, controlled trial. Gastrointest Endosc. 2006;63:986–995. doi: 10.1016/j.gie.2005.11.052. [DOI] [PubMed] [Google Scholar]
- 17.Moss AC, Morris E, Leyden J, MacMathuna P. Do the benefits of metal stents justify the costs? A systematic review and meta-analysis of trials comparing endoscopic stents for malignant biliary obstruction. Eur J Gastroenterol Hepatol. 2007;19:1119–1124. doi: 10.1097/MEG.0b013e3282f16206. [DOI] [PubMed] [Google Scholar]
- 18.Moss AC, Morris E, Mac Mathuna P. Palliative biliary stents for obstructing pancreatic carcinoma. Cochrane Database Syst Rev. 2006:CD004200. doi: 10.1002/14651858.CD004200.pub2. [DOI] [PubMed] [Google Scholar]
- 19.Mukai T, Yasuda I, Nakashima M, et al. Metallic stents are more efficacious than plastic stents in unresectable malignant hilar biliary strictures: a randomized controlled trial. J Hepatobiliary Pancreat Sci. 2013;20:214–222. doi: 10.1007/s00534-012-0508-8. [DOI] [PubMed] [Google Scholar]
- 20.Sangchan A, Kongkasame W, Pugkhem A, Jenwitheesuk K, Mairiang P. Efficacy of metal and plastic stents in unresectable complex hilar cholangiocarcinoma: a randomized controlled trial. Gastrointest Endosc. 2012;76:93–99. doi: 10.1016/j.gie.2012.02.048. [DOI] [PubMed] [Google Scholar]
- 21.Silvis S, Sievert C, Vennes JA, Abeyta B, Brennecke L. Comparisson of covered versus uncovered wire mesh stents in the canine biliary tract. Gastrointest Endosc. 1994;40:17–21. doi: 10.1016/s0016-5107(94)70004-4. [DOI] [PubMed] [Google Scholar]
- 22.Prat F, Chapat O, Ducot E, et al. A randomized trial of endoscopic drainage methods for inoperable malignant strictures of the common bile duct. Gastrointest Endosc. 1998;47:1–7. doi: 10.1016/s0016-5107(98)70291-3. [DOI] [PubMed] [Google Scholar]
- 23.Hong WD, Chen XW, Wu WZ, Zhu QH, Chen XR. Metal versus plastic stents for malignant biliary obstruction: an update meta-analysis. Clin Res Hepatol Gastroenterol. 2013;37:496–500. doi: 10.1016/j.clinre.2012.12.002. [DOI] [PubMed] [Google Scholar]
- 24.Rossi P, Bezzi M, Salvatori FM, Panzetti C, Rossi M, Pavia G. Clinical experience with covered Wallstents for biliary malignancies: 23-month follow-up. Cardiovasc Intervent Radiol. 1997;20:441–447. doi: 10.1007/s002709900190. [DOI] [PubMed] [Google Scholar]
- 25.Hausegger KA, Thurnher S, Bodendorfer G, et al. Treatment of malignant biliary obstruction with polyurethane covered Wallstents. AJR Am J Roentgenol. 1998;170:403–408. doi: 10.2214/ajr.170.2.9456954. [DOI] [PubMed] [Google Scholar]
- 26.Miyayama S, Matsui O, Terayama T, Tatsu H, Yamamoto T, Takashima T. Covered Gianturco stents for malignant biliary obstruction: preliminary clinical evaluation. J Vasc Interv Radiol. 1997;8:641–648. doi: 10.1016/s1051-0443(97)70624-9. [DOI] [PubMed] [Google Scholar]
- 27.Han YM, Jin GY, Lee S, Kwak HS, Chung GH. Flared polyurethane-covered self expandable nitinol stent for malignant biliary obstruction. J Vasc Interv Radiol. 2003;14:1291–1301. doi: 10.1097/01.rvi.0000092902.31640.39. [DOI] [PubMed] [Google Scholar]
- 28.Kanasaki S, Furukawa A, Kane T, Murata K. Polyurethane- covered nitinol Strecker stents as primary palliative treatment of malignant biliary obstruction. Cardiovasc Intervent Radiol. 2000;23:114–120. doi: 10.1007/s002709910023. [DOI] [PubMed] [Google Scholar]
- 29.Bezzi M, Zolovkins A, Cantisani V, et al. New ePTFE/FEP-covered stent in the palliative treatment of malignant biliary obstruction. J Vasc Interv Radiol. 2002;13:581–589. doi: 10.1016/s1051-0443(07)61651-0. [DOI] [PubMed] [Google Scholar]
- 30.Krokidis M, Fanelli F, Orgera G, et al. Percutaneous palliation of pancreatic head cancer: randomized comparison of ePTFE/FEP-covered versus uncovered nitinol biliary stents. Cardiovasc Intervent Radiol. 2011;34:352–361. doi: 10.1007/s00270-010-9880-4. [DOI] [PubMed] [Google Scholar]
- 31.Krokidis M, Fanelli F, Orgera G, Bezzi M, Passariello R, Hatzidakis A. Percutaneous treatment of malignant jaundice due to extrahepatic cholangiocarcinoma: covered Viabil stent versus uncovered Wallstents. Cardiovasc Intervent Radiol. 2010;33:97–106. doi: 10.1007/s00270-009-9604-9. [DOI] [PubMed] [Google Scholar]
- 32.Hatzidakis A, Krokidis M, Kalbakis K, Romanos J, Petrakis I, Gourtsoyiannis N. ePTFE/FEP-covered metallic stents for palliation of malignant biliary disease: can tumor ingrowth be prevented? Cardiovasc Intervent Radiol. 2007;30:950–958. doi: 10.1007/s00270-007-9049-y. [DOI] [PubMed] [Google Scholar]
- 33.Organ LW. Electrophysiologic principles of radiofrequency lesion making. Appl Neurophysiol. 1976-1977;39:69–76. doi: 10.1159/000102478. [DOI] [PubMed] [Google Scholar]
- 34.Sutherland LM, Williams JA, Padbury RT, Gotley DC, Stokes B, Maddern GJ. Radiofrequency ablation of liver tumors: a systematic review. Arch Surg. 2006;141:181–190. doi: 10.1001/archsurg.141.2.181. [DOI] [PubMed] [Google Scholar]
- 35.Steel AW, Postgate AJ, Khorsandi S, et al. Endoscopically applied radiofrequency ablation appears to be safe in the treatment of malignant biliary obstruction. Gastrointest Endosc. 2011;73:149–153. doi: 10.1016/j.gie.2010.09.031. [DOI] [PubMed] [Google Scholar]
- 36.Zacharoulis D, Lazoura O, Khorsandi S, et al. EndoHPB: a novel endobiliary radiofrequency ablation device. An experimental study. J Invest Surg. 2013;26:6–10. doi: 10.3109/08941939.2012.681832. [DOI] [PubMed] [Google Scholar]
- 37.Mizandari M, Pai M, Xi F, et al. Percutaneous intraductal radiofrequency ablation is a safe treatment for malignant biliary obstruction: feasibility and early results. Cardiovasc Intervent Radiol. 2013;36:814–819. doi: 10.1007/s00270-012-0529-3. [DOI] [PubMed] [Google Scholar]