

Abstract
The high societal and personal costs of child maltreatment make identification of effective early prevention programs a high research priority. Early Head Start (EHS), a dual generational program serving low-income families with children prenatally through age three years, is one of the largest federally funded programs for infants and toddlers in the United States. A national randomized trial found EHS to be effective in improving parent and child outcomes, but its effectiveness in reducing child maltreatment was not assessed. The current study used administrative data from state child welfare agencies to examine the impact of EHS on documented abuse and neglect among children from seven of the original seventeen programs in the national EHS randomized controlled trial. Results indicated that children in EHS had significantly fewer child welfare encounters between the ages of five and nine years than did children in the control group, and that EHS slowed the rate of subsequent encounters. Additionally, compared to children in the control group, children in EHS were less likely to have a substantiated report of physical or sexual abuse, but more likely to have a substantiated report of neglect. These findings suggest that EHS may be effective in reducing child maltreatment among low-income children, in particular, physical and sexual abuse.
Keywords: Child maltreatment, Prevention, Intervention, Evaluation, Early childhood, Randomized control trial
1. Introduction
More than 676,500 children in the U.S. were abused and neglected in 2011 (U.S. Department of Health and Human Services [USDHHS], 2012). The prevalence of child maltreatment and its serious short- and long-term consequences for children's health (Anda et al., 2006; Leeb, Lewis, & Zolotor, 2011), development, and education (Bolger & Patterson, 2003; Veltman & Browne, 2001), as well as its societal costs (Fang, Brown, Florence, & Mercy, 2012) make finding effective strategies for child maltreatment prevention a research and policy priority (Whitaker, Lutzker, & Shelley, 2005). Although recent reviews (MacMillan et al., 2009a, 2009b; Mikton & Butchart, 2009; Reynolds, Mathieson, & Topitzes, 2009; Selph, Bougatsos, Blazina, & Nelson, 2013) have identified a few rigorously evaluated promising approaches, program effects have been inconsistent upon replication and difficult to take to scale. More rigorous research on scalable preventive interventions is needed to determine the most effective means of addressing this public health issue.
There is a general agreement that child abuse and neglect by caregivers occur as the result of multiple interacting risk factors at the level of the child, parent, family, and broader childrearing environment (Belsky, 1993; Chalk, Gibbons, & Scarupa, 2002; Institute of Medicine and National Research Council, 2013). Thus, preventive interventions may be more efficacious when they attend to both the family's social environment (e.g., social support, economic stability, housing, neighborhood conditions, parental mental health, community linkages and resources) as well as abusive and neglectful parenting behaviors (Child Welfare Information Gateway, 2012). Further, very young children (birth through age three) are most likely to suffer serious injury and death related to maltreatment, with children younger than three years of age accounting for 74% of maltreatment-related deaths (USDHHS, 2012). These very young children may be more vulnerable for a variety of reasons, including their inability to defend themselves, their small size, their relative social isolation, and the fact that infancy is a sensitive period of brain development that may be severely disrupted by trauma (Brodowski et al., 2008). Given the multifactorial etiology of child maltreatment and its high incidence among infants and toddlers (USDHHS, 2012), prevention programs that begin as early as possible and use a bioecological approach (Bronfenbrenner & Morris, 2006) addressing child and family well-being in addition to problematic parenting behaviors are especially promising. Early Head Start (EHS), a comprehensive, two-generation program providing parenting, educational, nutritional, health, and social services to low-income families with infants and toddlers (birth to age three years), represents a promising approach in preventing child maltreatment in this vulnerable age group.
1.1. Identifying effective child maltreatment prevention strategies
Child maltreatment prevention efforts have expanded considerably over the past three decades (MacMillan et al., 2009a, 2009b; Paxson & Haskins, 2009). A variety of approaches have been implemented to prevent child abuse and neglect, including parent education, home visitation, community-wide programs, media, and multi-component strategies (Mikton & Butchart, 2009). Many of these efforts have been found to have favorable program impacts on risk factors for child abuse and neglect, especially parenting behavior and maternal well-being, but fewer show success in directly reducing child maltreatment (Howard & Brooks-Gunn, 2009; Reynolds et al., 2009).
Home visiting has become one of the most popular approaches in preventing child maltreatment. In 2009, the U.S. Department of Health and Human Services launched the Home Visiting Evidence of Effectiveness (HomVEE) to review research on the efficacy of home visiting programs that serve families with pregnant women and children from birth to age five (Avellar, Paulsell, Sama-Miller, & Del Grosso, 2012). HomVEE identified 13 home visiting programs that met the USDHHS criteria for rigorous methodology and showed positive effects in promoting family, parent, and/or child well-being. Of these 13 programs, however, only five showed any evidence of reducing child maltreatment, and only two had replicable and sustained child abuse or neglect outcomes (Nurse-Family Partnership Program, Olds et al., 1997; Zielinski, Eckenrode, & Olds, 2009; and Healthy Families America, DuMont et al., 2008). EHS (Home Visiting Model) was included among the 13 meeting USDHHS criteria and was rated as having strong sustained outcomes for child development, positive parenting, and family self-sufficiency.
The HomVEE review, as well as other reviews of child maltreatment prevention efforts, documents a number of the methodological challenges in examining maltreatment outcomes in evaluation studies (Avellar et al., 2012; MacMillan et al., 2009a, 2009b; Mikton & Butchart, 2009; Reynolds et al., 2009). First, many studies lack adequate sample size to have sufficient power to detect the relatively infrequent occurrence of documented abuse or neglect (Howard & Brooks-Gunn, 2009; Reynolds et al., 2009). Second, there have been questions regarding the appropriateness of using documented or substantiated maltreatment reports as a primary outcome measure for maltreatment prevention research, both because it likely underrepresents the actual occurrence of maltreatment and because of the heightened surveillance by mandated reporters for children in the “treatment group” in the form of prevention service providers (Howard & Brooks-Gunn, 2009; Reynolds et al., 2009). Third, many studies of potentially promising prevention programs lack sufficient methodological rigor in terms of study design, and in particular, the child maltreatment prevention field lacks studies using randomized controlled trials (MacMillan et al., 2009a, 2009b; Mikton & Butchart, 2009). Finally, preliminary evidence suggests that long-term follow-up may be needed to fully understand child maltreatment prevention outcomes, which may not be detected until several years after the programs have ended (Zielinski et al., 2009). Such longitudinal studies are expensive and difficult to implement, and many potentially promising programs have not had on-going longitudinal research that can examine their effectiveness over the life course.
EHS is one of the most widely implemented comprehensive early childhood development and family support services serving low-income infants and toddlers and their families. Results from the randomized controlled trial of EHS show favorable effects of the program for both children and their parents (Administration for Children and Families [ACF], 2002b; Love, Chazan-Cohen, Raikes, & Brooks-Gunn, 2013). However, prior to the current study, the effectiveness of EHS in preventing child abuse and neglect has never been tested. Building on the original large-scale randomized study, the current study addresses a number of the methodological challenges listed above and provides a first look at whether this popular and scalable prevention program prevents child abuse and neglect among low-income families.
1.2. The EHS program and the national EHS randomized controlled trial
EHS was authorized in 1994, with the first 68 grantees funded in 1995, and now serves over 110,000 children per year in a little over 1000 programs, making it one of the largest programs serving low-income infants and toddlers in the United States. EHS aims to promote positive development in children directly, by providing services to children from birth to three years of age, and indirectly, by providing supports to parents in their role as primary caregivers, as well as by promoting parent self-sufficiency and healthy family functioning. EHS programs use two primary service approaches: (1) home visiting, in which weekly 90-minute home visits are provided to families, coupled with group socialization activities; and (2) center-based child development services with at least two home visits per year. Many programs provide EHS services using both models.
Original Congressional authorization of EHS services mandated that the program be rigorously evaluated, and a randomized controlled trial referred to as the Early Head Start Research and Evaluation Project (EHSREP) was launched in 1996, at the same time the program began. In all, 3001 low-income families with a pregnant woman or an infant under the age of 12 months in 17 sites across different geographic regions of the U.S. were enrolled in the study (between July 1996 and September 1998) and randomly assigned to EHS or a control group. Control group participants could access any services in the community other than EHS. Data on the children and their families were collected at enrollment and when children were about 1, 2, 3, 5, and 10 years of age.
To date, findings from this randomized control trial suggest that EHS benefits families across a wide range of child, parent, and family self-sufficiency outcomes (ACF, 2002b; Love et al., 2013). Importantly for the field of child maltreatment, EHS showed effects on known risk factors for physical abuse or neglect (Stith et al., 2009). Specifically, at one or more data points, EHS parents were more emotionally supportive and less detached during play, less stressed and depressed, spanked less, and reported less family confiict and substance abuse in the household (Vogel, Brooks-Gunn, Martin, & Klute, 2013). A consistent pattern of larger positive impacts has been observed at each data collection wave for African American children and their families and for families at moderate demographic risk (Raikes, Vogel, & Love, 2013). Impacts also have varied by program approach, with long-term benefits being more evident in those programs that provided home-based services (Love et al., 2013). Given the support that EHS provides to parents and its positive effects on parental and family well-being, as well as parenting and child behaviors, we hypothesized that EHS also would decrease the risk of child maltreatment. The EHSREP provided a unique opportunity to rigorously test this hypothesis. This study, known as the Early Head Start Child Welfare Study (EHS CWS), represents an important first step toward understanding how a family's participation in EHS might impact a child's involvement in the child welfare system.
2. Method
2.1. Approach
To contribute to the evidence base on child maltreatment prevention, we obtained child welfare administrative data to retrospectively identify and describe child welfare involvement among a subset of participants in the national EHSREP. The current study utilized data for participants in 7 of the original 17 sites included in the EHSREP. Families were originally eligible for the EHSREP study if they: (1) met federal income requirements (at or below the Federal Poverty Level) for Early Head Start; and (2) mothers were pregnant or had a child under the age of 12 months. Families were randomly assigned at program enrollment by the national cross-site evaluation team (for details see ACF, 2002a, 2002b). This study uses an intent-to-treat design including all study participants randomly assigned at enrollment. We used administrative child welfare records to examine the likelihood, frequency, and timing of child welfare encounters for these children from the time of enrollment and random assignment (1996–1998) through December 31, 2009.
We selected the subsample of sites for this study based on: (a) the presence of a local EHS researcher with a history of working with the local or state child welfare agency; (b) geographic representation of sites in the United States; (c) ethnic/racial diversity in EHS populations served; (d) representation of both home-based and center-based EHS program models; and (e) availability of locally collected data that might be particularly useful in informing child abuse prevention outcomes. We contacted a representative from the state child welfare authority in seven states to determine the availability of electronic data for the proposed study period (January 1, 1996–December 31, 2009) their initial willingness to share individual-level data, and to identify procedures for developing a data-sharing agreement. One of the seven states contacted denied this request. As a result, this study used child welfare data from seven sites located in six states for a thirteen-year period (1996–2009). Portland State University's and Harvard University's Institutional Review Boards granted approval for data collection, as well as waivers for informed consent to access these data. Four of the six states required and granted state-operated Institutional Review Board approval.
The seven EHS programs included in this study are diverse in relation to service delivery models, community contexts, and populations served. One program provided only center-based services, four programs provided home-based services, and two programs provided a mix (some families received home based services while others received center-based services). Three of the programs are located in rural communities. Two of the programs served primarily Hispanic families, while three programs served primarily White families, and the remaining two sites served a more demographically diverse low-income population.
2.2. Study sample
A total of 1247 young children and their families were included in the present study, comprising all families in the seven sites who had enrolled in the original EHSREP. There were a few observed differences in the sample characteristics for the seven participating sites in this project compared to the EHS national study sample as a whole (see Table 1); thus, it is clear that the participants in the current study are not completely representative of the larger EHSREP study. Specifically, primary caregivers in the current sample were significantly more likely to be white and less likely to be African American; more likely to be unemployed; less likely to be very low income (less than 33% of Federal Poverty Level); somewhat more likely to have been enrolled prenatally and less likely to be enrolled when children were over five months of age. In the current sample, half (51%) of the mothers had less than a high school education at enrollment; many were White (45%), with 19% African American and 31% Hispanic; 64% were unemployed; 27% were living with a spouse; and 22% were earning less than 33% of the federal poverty limit. At EHSREP enrollment (1996–1998), 66% of study children were less than 5 months of age or not yet born. At the end of the current study period (December 31, 2009), the age range for participating children was 11.6 years to 14.3 years, with an average age of 13.2 years.
Table 1.
Baseline demographic characteristics for the current study sample and the national Early Head Start Research and Evaluation Project sample.
| EHS – 7 sites sample |
EHSREP national sample |
p | |
|---|---|---|---|
| (n = 1247) |
(n = 3001) |
||
| % | % | ||
| Family and parent characteristics | |||
| Applicant is biological mother | 99.8 | 99.4 | 0.15 |
| Highest grade completed | 0.09~ | ||
| Less than 12 | 51.0 | 47.6 | |
| 12 or earned a GED | 27.9 | 28.7 | |
| More than 12 | 21.1 | 23.7 | |
| Race and ethnicity | 0.00*** | ||
| White non-Hispanic | 45.0 | 37.2 | |
| Black non-Hispanic | 19.3 | 34.7 | |
| Hispanic | 31.4 | 23.6 | |
| Other (Asian or Pacific Islanders, American Indian, etc.) | 4.3 | 4.6 | |
| Primary occupation | 0.00*** | ||
| Employed | 22.8 | 23.4 | |
| In school or training program | 13.7 | 21.8 | |
| Other unemployed | 63.5 | 54.9 | |
| Living arrangements | 0.27 | ||
| Living with a spouse | 27.2 | 25.2 | |
| Living with other adults | 36.4 | 38.7 | |
| Living with no other adults | 36.4 | 36.1 | |
| Household income as a percent of the poverty level (percent) | 0.00*** | ||
| Less than 33 | 22.2 | 30.1 | |
| 33 to 67 | 41.3 | 30.9 | |
| 67 to 99 | 27.4 | 25.3 | |
| 100 or more | 9.0 | 13.8 | |
| Characteristics of focus child | |||
| Age at random assignment | 0.00*** | ||
| Unborn | 31.8 | 26.7 | |
| Less than 5 months | 37.3 | 35.8 | |
| 5 or more months | 30.8 | 37.5 | |
| Female | 48.5 | 47.8 | 0.70* |
p < .001.
** p < .01.
p < .05.
p < .10.
2.3. Child welfare outcome data collection and measures
We obtained administrative records from child welfare agencies for EHSREP participants via electronic matching of identifying information for a thirteen-year period (January 1, 1996–December 31, 2009). We used mother and child names, birthdates, and social security numbers (available for 68% of this subsample) to match EHS study participants to child welfare administrative records. All originally randomized study participants were submitted for matching to state child welfare records. It is important to note, however, that once children and parents moved out of the state in which the EHS programs were located, associated abuse records would not be located in the state's child welfare data system unless the child welfare encounter happened prior to the family's move, or if a family moved out of state and then returned (although they may have had reports in other states). Only 3% of the sample had moved permanently out of the original state of residence by grade five.
When a match was found, administrative records were used to collect information on the following outcome variables:
Number and date of substantiated reports of child maltreatment. All states recorded dates of substantiated maltreatment reports. However, in one state, many cases are not formally substantiated if the child welfare system determines that services are needed. In this state, we worked with their administrative data research team to operationally define reports that likely would have been substantiated as those in which a report resulted in either opening a child welfare case or in the state's provision of child welfare services.
Number and date of out-of-home placements. We calculated the number of out-of-home placements as the number of unique non-consecutive removals for each child (i.e., consecutive placement changes were not counted as a unique out-of-home placements). For example, if data indicated that a child was removed from his or her home on January 1, 2000, and placed in foster care until June 30, 2000, at which point there was a placement change to a therapeutic group home, this was counted as one out-of-home placement.
Maltreatment type of each substantiated report. States varied considerably in codes used to document the type of maltreatment experienced (Green et al., 2013). Further, because one state only reported a “primary” type of maltreatment for each substantiated report, we were not able to account for children who experienced more than one type of maltreatment in relation to a single substantiated report for the full sample. Therefore, we created a primary abuse type code for each report by synthesizing codes used across sites as follows: (1) physical abuse; (2) sexual abuse (physical and sexual abuse reports were combined for the analyses because of the small number of sexual abuse reports); (3) neglect; and (4) emotional abuse. If multiple abuse type codes were available, we assigned a code to refiect the specific ordering of abuse types (e.g., if a report included physical abuse and neglect allegations, we coded the report as physical abuse). To check the accuracy of administrative data for maltreatment type, we conducted case file reviews for children with either substantiated reports or out-of-home placements in four sites. Three reports of neglect were recoded as physical abuse based on the review of the case files, suggesting high accuracy in type of maltreatment recorded in the electronic administrative data.
Because there were too few out-of-home placements to reliably estimate impact effects for this variable alone, and because some children had out-of-home placements without a corresponding substantiated maltreatment report (and without any type of maltreatment specified), we created a variable to represent any child welfare encounter by combining substantiated child maltreatment reports and out-of-home placements. Thus, a child welfare encounter occurred when the child had either a substantiated maltreatment report or an out-of-home placement, or both.
2.4. Case file reviews
We requested permission to review children's case files for those identified with child welfare involvement in four sites in three states. Members of the study team traveled to states to conduct the file reviews for this study. A standardized template was developed to extract key data from the child welfare files. Case file data provided additional information about the circumstances surrounding maltreatment for these children and cross-validated the information contained in the electronic administrative data. Detailed information from the case file reviews is presented elsewhere (Green et al., 2013).
2.5. Covariates: baseline child and family data collection and measures
Baseline data were collected from all study participants at enrollment using the Head Start Family Information System Enrollment Form (ACF, 2002a). Parents or EHS program staff completed forms at the time the family applied for enrollment to the program (prior to random assignment). The form included the following baseline demographic and family characteristics, which were used as covariates in all impact models: (a) whether the mother was a teen parent at the birth of her first child (b 20 years of age); (b) whether the family currently received welfare assistance (at that time, Aid to Families with Dependent Children, AFDC), yes or no; (c) mother's race/ethnicity, recoded for the current study as White, Hispanic, African American, or Other; further dichotomized into White or non-White; (d) mother's marital status, recoded for the current study as single or partnered/married; (e) mother's highest educational level, recoded for the current study as whether or not mother had received a high school diploma; (f) mother's employment status, recoded for the current study as unemployed or employed full or part time; (g) whether mother's current partner (at enrollment) was the biological father or not; (h) whether the family had been homeless at any time during the 12 months prior to study enrollment (yes/no); and (i) the number of children in the household, recoded for the current study as whether or not there were 3 or more children living in the home at study enrollment (yes/no). Additionally, we calculated the age of child at enrollment (coded as 0 if the mother was pregnant at enrollment) for inclusion as a covariate. We selected covariates to maintain consistency with impact analyses conducted in the main EHS national study (U.S.D.H.H.S., 2010).
2.6. Data analysis
2.6.1. Impact models
We calculated adjusted odds ratios (OR) using logistic regression (controlling for selected covariates) to examine the likelihood that EHS children, as compared to controls, had any child welfare encounter (overall) and in each of the following four age groups: (a) 0–31/2 years old (up to 42 months, and thus refiecting the designated end of EHS services); (b) 43 months to age five (60 months), representing the preschool period; (c) five years old (61 months) to nine years old (108 months) representing the early elementary period (kindergarten through third grade); and (d) over age nine (109 months), representing older elementary ages to the beginning of middle school. We also examined the likelihood of having a first child welfare encounter during each of these age groups. Due to the highly skewed distribution of data related to the total number of encounters, we used negative binomial regression models to calculate incidence rate ratios (IRR) in order to assess the impact of EHS intervention on the total number of child welfare encounters, the total number of substantiated reports of neglect, and the total number of physical or sexual abuse reports during the data collection period. Models examining the number of neglect and abuse reports only were conducted for the full study period, as the number of these events within a given developmental period was often quite small (especially in the case of physical abuse).
For consistency, all models included the ten covariates described above, even if each variable did not significantly predict variance in child welfare outcomes. Model-building using these covariates in different constellations confirmed that EHS effects were robust to variations in covariate selection. We tested all pair-wise interactions between EHS intervention and covariates and retained statistically significant interaction terms in final models. Finally, we included dummy variables representing six of the seven EHS sites in all models to account for variability in outcomes between sites. Interactions between EHS intervention and site were included as a block when they jointly predicted variability in child welfare outcomes.
Additionally, we used recurrent events survival analysis to assess whether EHS had an impact on the timing of the first child welfare encounter, as well as the timing of subsequent encounters. We fit a Prentice–Williams–Peterson counting process model (PWP-CP), an extension of the Cox model (Prentice, Williams, & Peterson, 1981). The PWP-CP is a conditional model in which a subject is assumed not to be at risk for a subsequent event until a current event has terminated. The baseline hazard function was stratified by event order to estimate event-specific baseline hazards. A test of the proportion hazard assumption for EHS site revealed that baseline hazards were not proportional at different levels of site, X2 = 12.19, p = .08, so baseline hazard also was stratified by site. We used a sandwich estimator to adjust for dependence of events within subjects (Kelly & Lim, 2000). Differences in timing of events vis-à-vis EHS program involvement were expressed as hazard ratios (HR).
For all statistical tests, we report an alpha level of .05 as statistically significant and identify associations that trend toward significance when p < .10.
2.6.2. Missing data
Rates of nonresponse for baseline demographic and family characteristics (model covariates) ranged from 0% to 11.2%; the mean nonresponse rate for these variables was 2.9%. Chi-squared tests compared nonresponse rates for program and control participants and compared nonresponse rates for children who had child welfare involvement with those who did not. Nonresponse rates were significantly different between the EHS and control group for 1 of the 10 covariates. Control group families were more likely to have missing data if they had ever been homeless, X2 (1, 1247) = 31.3, p < .001. Nonresponse rates for model covariates did not differ according to whether a child had welfare involvement.
We utilized Full Information Maximum Likelihood (FIML) for all analyses examining the overall effects of the EHS program on child welfare outcomes using Mplus 6.1 (Muthén & Muthén, 2005). FIML is preferable to other maximum likelihood methods because it uses the raw data as input and therefore uses all the available information in the data (Hunter & Lange, 2004).
3. Results
Comparisons between the EHS program group and the control group showed only two significant differences (p < .05) among the ten covariates examined. Specifically, EHS participants were less likely (25%) than the control group participants (36%) to report that the family had moved more than once in the past year (X2 (1, 1247) = 17.89, p < .001) and EHS families were more likely (13.7%) than controls (9.4%) to report having more than three children in the household (X2 (1, 1247) = 5.71, p = .04).
3.1. Child maltreatment in the study sample
The percentage of children in this sample with a substantiated report of child maltreatment was 15.8% (i.e., 158 per 1000 children); 6.7% had an out-of-home placement, and 18.0% had at least one child welfare encounter. Approximately 82.0% of all children had no child welfare encounters, 8.5% had a single encounter, and 9.4% had two or more encounters. A first encounter was most likely to occur during the birth to three and five to nine year-old periods; on average, children had their first encounter with the child welfare system at 69.9 months (5.8 years; SD = 44.23; range = 0.03–184.3). Children between the ages of five and nine had the highest percentage of child welfare encounters (8.6% of all children), with the lowest proportion of children experiencing an encounter when they were under the age of five (4% in three to five age group and 5% among birth to three). Among children in this sample, 10.7% (n = 133) had one or more substantiated reports with a primary allegation of neglect, 4.4% (n = 55) had one or more substantiated reports with a primary allegation of physical abuse, and 3.3% (n = 41) had one or more substantiated reports with a primary allegation of sexual abuse. Thus, in terms of primary report allegations, over two-thirds of children with one or more substantiated reports of maltreatment (n = 197) experienced neglect (67.5%; n = 133); over half (58.4%; n = 115) were victimized by their mothers, 32.0% (n = 63) by some other individual(s), and 9.6% by both (n = 19). The most commonly occurring form of substantiated maltreatment was neglect by a biological mother (65.2%; n = 65).
3.2. Impact of EHS on child maltreatment
As shown in Table 2, children between the ages of five and nine years who had participated in EHS were less likely to have a child welfare encounter (adjusted OR = 0.64, p = .04) during this developmental period. EHS participants also had significantly fewer total number of encounters (38% less) during the period of age five to nine years (B = −2.50, adjusted IRR = 0.63, p = .002) and after the age of nine (B = −0.67, adjusted IRR = .52, p = .04). Although there were no significant differences between EHS and control participants in the number of encounters in the other developmental periods, all coefficients were negative, suggesting a pattern of fewer encounters for EHS participants. To examine this pattern further, we fit the full model predicting the number of child welfare encounters seven different times with a different reference (base) category for site in each model. This yields a main effect of EHS program group status for each site, adjusting for covariates and interactions. These results indicated that five of the seven EHS sites had lower rates of total child welfare encounters among EHS participants when compared to controls (IRR range: 0.29–0.99), though rates between EHS and control were only significantly or marginally different in two of these five sites. Two of the seven sites had higher rates of total encounters when compared to controls, though these differences did not reach statistical significance. There were no significant differences between EHS participants and controls in terms of the likelihood of ever having a child maltreatment welfare encounter (see Table 2).
Table 2.
Difference in odds of having at least one child welfare encounter, a first encounter, and incidence of total encounters for EHS and non-EHS children overall and by developmental period, adjusted for covariatesa.
| Odds of at least one encounter |
Odds of first encounter |
Number of encounters |
|
|---|---|---|---|
| Adjusted OR (SE) | Adjusted OR (SE) | Adjusted IRR (SE) | |
| Overall | 0.96 (0.40) | Not applicable | 0.84 (0.51) |
| 0–3.5 years of age | 1.15 (0.30) | 1.20 (0.32) | 0.78 (0.76) |
| 3.5–5 years of age | 1.54 (0.44) | 1.55 (0.51) | 1.38 (0.28) |
| 5–9 years of age | 0.64 (0.14)* | 0.74 (0.18) | 0.63 (0.80)* |
| 9+ years of age | 1.00 (0.25) | 1.13 (0.39) | 0.52 (0.60)* |
Note. OR = odds ratio; IRR = incident rate ratio; SE = standard error.
Adjusted for age of child at random assignment, family on welfare (AFDC), family is White, mother is single, mother has no high school diploma, mother is not employed or in school, family has been homeless, mother's partner is not the biological father, family has more than three children in the household, family has moved more than once in the past year.
p < .05.
EHS program group participants also had fewer physical/sexual abuse reports compared to controls (B = −1.24, adjusted IRR = 0.71, p < .001). However, there were more neglect reports per child (B = 0.52, adjusted IRR = 1.30, p = .04), on average. To examine this finding further, we looked descriptively at the percentage of EHS versus control group children who had neglect reports in different developmental periods. These data suggest some evidence of surveillance; specifically, in children from birth to three (during the EHS program period), 3% of EHS children had neglect reports, compared to 2.1% of control children. Further, 3.3% of EHS children had neglect reports during the three to five age period, compared to only 1.9% of the control group. After age five, the rates of neglect in the intervention and control group were more similar (5.1% for EHS children vs. 4.5% for controls). These higher rates of neglect reporting may be associated with the documented higher rates of involvement by EHS children in Head Start and other formal prekindergarten services (compared to controls; Love et al., 2013).
The EHS program had a significant effect on time to the second child welfare encounter, controlling for site and covariates representing family risk (see Fig. 1). Specifically, children in the control group were 2.71 times more likely (estimated hazard) of experiencing a second child welfare encounter earlier than the children in the EHS program group (HR = 0.37, p < .001). Hazard rates for time to second encounter for program and control children are displayed in Fig. 1, which shows that at nearly every age (especially if the second encounter occurred in the birth to three year range) control group children had a higher rate of child welfare encounters than program children.
Fig. 1.
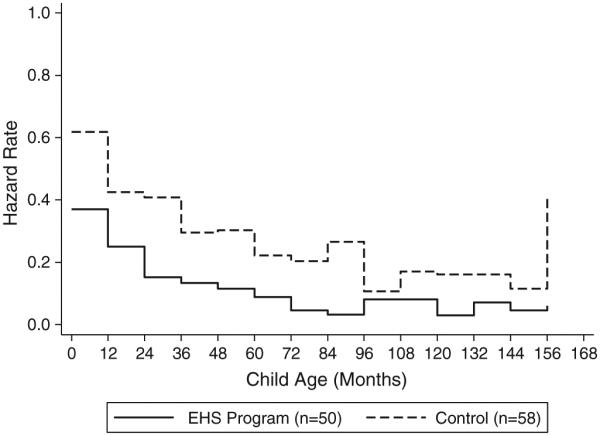
Probability (hazard rates) of time to second child welfare encounter, by program group, for children of average risk (n = 108).
4. Discussion
In this study, we examined child welfare involvement for participants in seven of the 17 original EHSREP project sites. Results indicate that children who had participated in the EHS program were less likely to be physically or sexually abused and less likely to be abused or neglected a second time. Additionally, in the majority of the program sites, there was an overall pattern of fewer total child welfare encounters for EHS children compared to controls. Interestingly, the primary maltreatment prevention effect for the EHS program appears when children reached school age, with children in the EHS group <eing less likely, overall, to have a report between the ages of five and nine, and to have fewer reports after age five. However, EHS children were also somewhat more likely to be reported for neglect than were children in the control group.
Others have found impacts of interventions to prevent child maltreatment after program participation has ended (Olds et al., 1997; Reynolds & Robertson, 2003). Later detection of effects may be related to increased surveillance and reporting of child maltreatment by program staff, or there may be other factors. For example, Olds et al. (1997) suggest that reductions in maltreatment observed after the end of their home visiting program may be due to improvements in maternal life course, especially reductions in maternal substance abuse and in subsequent births (e.g., smaller families). In the EHSREP, later program impacts for the entire EHS sample provide some insight into the factors that may be contributing to subsequent reductions in maltreatment. For example, when children were both three and five years of age, mothers in the EHS program reported less punitive parenting and more positive (responsive, warm, nurturing) parenting compared to controls (Vogel et al., 2013). These changes in parenting behavior may be associated with the reduced incidence of physical abuse among these children, as well as with the reduced likelihood of either neglect or abuse after age five. By age ten, while there were no significant differences in parenting, children in the EHS program group showed higher levels of social competence and social-emotional well-being (ACF, 2001, 2002b; Jones-Harden et al., 2010). Children who lack social competencies are more likely to be maltreated (Black, Smith Slep, & Heyman, 2001) so to the extent that EHS children are higher in social competency they may also be at reduced risk for abuse. Future research exploring time-varying mediators, such as changes in parenting and child development, are needed to explore these and other mechanisms and further explain the reductions in maltreatment among school-age EHS children.
The key strengths of the current study are its longitudinal nature, random assignment design, and the tracking of participating children from birth through age ten. First, as discussed previously, this allowed us to assess EHS program impacts at differing developmental periods and to assess the points at which maltreatment prevention effects are manifest. Short-term studies that involve less than five years of follow-up may be unlikely to detect these longer-term outcome effects.
Further, we were able to examine the effects of EHS on maltreatment recurrence. Over the course of this ten-year span, children in the control group with a single child welfare encounter had almost three times the risk of having a second encounter by the end of the next year when compared to children in EHS with a single encounter. There is currently little known about the effectiveness of programs in reducing maltreatment once the child welfare system has become involved with a family and in fact, numerous studies have found that previous child welfare encounters are associated with elevated risk of future reports (DePanfilis & Zuravin, 2002; Drake & Pandey, 1996; Fluke, Shusterman, Hollinshead, & Yuan, 2005; Kohl & Barth, 2007; Waldfogel, 2009). Other risk factors for maltreatment recurrence include lack of social support, being a victim of neglect (as opposed to physical abuse), family stress, and child health problems (DePanfilis & Zuravin, 2002). The current study findings suggest that EHS reduced the likelihood of subsequent reports later in the child's life, perhaps by connecting the family with needed support and services earlier and thereby reducing stress and health problems. A larger sample that is more representative of all EHS families, coupled with a longer follow-up period would help to further elucidate the role of EHS in preventing maltreatment recurrence.
Our findings also indicate that EHS reduced the likelihood of substantiated reports that involved allegations of physical and/or sexual abuse. Children in EHS had 29% fewer substantiated reports involving abuse (physical and/or sexual) than did their peers in the control group. This is important given that rates of serious physical abuse appear to have increased, especially among young children (Leventhal & Geither, 2012) and that many early intervention programs have not been consistently effective in reducing child maltreatment (Howard & Brooks-Gunn, 2009; Selph et al., 2013). Unfortunately, the number of instances of physical versus sexual abuse was too small in the current sample to disentangle these two different report types.
A somewhat unexpected finding was that children in the EHS group had more substantiated reports of neglect than did their counterparts in the control group. As it seems unlikely that the program increased child neglect, an alternative explanation may be surveillance bias. Neglect is notoriously difficult to detect, especially during infancy, when it is most common; infants tend to have few interactions with individuals outside of the family who might report neglectful caregiving practices to authorities (DePanfilis, 2006; USDHHS, 2012). Enrollment in EHS may increase the visibility of very young children experiencing neglect who might otherwise have gone unnoticed. As a result, being under the watchful eye of EHS staff may trigger intervention by child welfare services with neglectful families, which in turn obscures the program's positive impacts by elevating the rate of neglect in the program group and not the control group. A key outcome documented in the original EHS study was that EHS children were significantly more likely to be enrolled in formal Head Start or other Prekindergarten services after EHS enrollment, compared to controls (Love et al., 2013). Thus, the period of higher surveillance due to involvement in early childhood interventions may have extended through age five for children in the EHS group. Several other researchers have observed the phenomenon of higher rates of substantiated reports of neglect in the intervention group compared to the control group (e.g., Easterbrooks et al., 2012; Olds, Henderson, Kitzman, & Cole, 1995). This is a serious methodological challenge for prevention research, and one that led Howard and Brooks-Gunn (2009) to posit that “the difference in surveillance between the treatment and control groups probably explains why so few home-visiting programs have measurable effects on rates of abuse and neglect” (p. 122). Unfortunately, without clear data about the source of the maltreatment report (data not retained in most administrative data systems), it is difficult to know whether surveillance, or some other factors, are contributing to these patterns.
4.1. Limitations
The current study represents a first look at the impact of Early Head Start on child maltreatment, and these findings need to be considered in the context of the study limitations. One of the potential limitations of this work is the quality and accuracy of data matching, although significant efforts were made to match with multiple identifiers. Matching was conducted by state agency affiliated research staff. About twothirds (68%) of this subsample had a valid social security number, which was likely to increase the probability of a successful match. The variables used for matching included mother and child names and birthdates; the use of two sets of identifiers to match records was also likely to increase the probability of a successful match. The use of case files to validate administrative data records (specifically, comparing report dates, dispositions, perpetrator types, and other characteristics) helps to increase our confidence in the accuracy of these records in terms of describing those incidents that were successfully linked to these EHS children, but unfortunately does little to provide insight into whether study participants with valid reports may have been missed through unsuccessful matching processes.
Further, children and parents who moved out of the state in which the EHS programs were located could not be matched in the state's child welfare data system unless the child welfare encounter happened prior to the family's move, or if families moved out of state and then returned (although they may have had reports in other states). Based on tracking data collected by local and national EHS study researchers through grade 5, only 3% of EHSREP children moved out of the original study state for all of the primary data collection points; however, over a third of families had a pattern of moving in and out of the state in which they originally received services (41%). One-third of the families were in the original study state for all subsequent data collection periods (37%). Future research that could obtain additional maltreatment records from other states would provide a more complete picture of child welfare involvement for these children.
Another limitation was the inability to access historical records related to unsubstantiated reports. Some research (Leiter, Myers, & Zingraff, 1994) has suggested that unsubstantiated reports are a critical source of information about child maltreatment, especially given the variability across states in how, when, and to what extent reports are investigated (Daro, 1993; Ocasio, Morton, & Simmel, 2013). However, most states that we contacted were unable to provide this due to purging of records from state data systems.
Child maltreatment that was not reported at all is another issue to consider. Official reports seriously underestimate the occurrence of child maltreatment (Theodore et al., 2005) and differential rates of unreported child maltreatment between EHS participants and controls, for example, due to the likelihood of contact with mandated reporters could mask intervention impacts because of surveillance bias, as discussed previously.
Sample size, along with the low frequency of substantiated maltreatment (outcome) events, limited our power to examine differences in program impact for physical abuse separately from sexual abuse and for each developmental period while controlling for covariates. Effect sizes, as refiected in odds ratios and relative risk ratios, suggest that the magnitude of the effects in this study were modest. Larger samples are needed to examine differences in types of abuse with adequate power. However, such analysis is important given the evidence of distinct etiology and outcomes for children by type of maltreatment (Barnett, Manly, & Cicchetti, 1993) and age of child when maltreatment occurs (Bolger & Patterson, 2003). Future exploration, currently underway with the remaining EHS program sites to increase statistical power, will allow us to look at overall impacts by type of maltreatment.
Finally, we want to note that several significant site by program group interactions suggest that the effects of EHS on child welfare involvement varied across sites. Site-level characteristics, such as program model (home versus center based), quality of program implementation, organizational norms related to child maltreatment reporting, or the nature of relationships between local EHS programs and child welfare authorities could all infiuence the effectiveness of a given program on maltreatment outcomes. Unfortunately, with the limited number (n = 7) of programs in the current study it is not possible to directly test these variables in terms of their potential impact on site-level variability.
4.2. Implications for practice
Increasing access to programs like EHS for high-risk children may reduce child maltreatment rates directly (through its effects on parents and children) or indirectly, by connecting families with needed services to help them provide safer, more stable and nurturing environments. Safe, stable, nurturing relationships and environments can protect children from toxic stress and its impacts on lifelong health and development (Shonkoff et al., 2012). While EHS was not originally designed as a child maltreatment prevention program, these results suggest that EHS services may impact, over the long term, children's likelihood of victimization. Given this finding, it is important to further identify the pathways through which this maltreatment effect may be strengthened, and those family and child factors that can be the target of interventions specifically designed to reduce likelihood of abuse and neglect. Recent federal efforts to increase collaboration between child welfare agencies and early childhood programs highlight the importance of providing services like the EHS program to those children who are involved, or at highest risk of involvement, with the child welfare system. This study underscores the potential benefits of these collaborations.
4.3. Conclusions
Despite these limitations, this study presents promising, if preliminary, evidence that EHS reduces the likelihood of maltreatment when children are between the ages of five and nine years old, reduces the rate of subsequent child maltreatment, and reduces the frequency of substantiated reports with a primary allegation of physical and/or sexual abuse. Early Head Start families, while they are high in demographic risks related to poverty, were not selected based on particular risks associated with child abuse and neglect. The EHS program was designed as an early learning and child development program, and impacts on maltreatment were not envisioned as a direct benefit of services. That said, the annual victimization rates for these EHS study participants were relatively high, ranging from 11 per 1000 to 27 per 1000 (averaged from 1997 to 2010). The national maltreatment victimization rate in 2011, by comparison, was 9.1 victims per 1000 children in the general population (USDHHS, 2012). Thus, this study suggests that children and families in Early Head Start programs may benefit from these services in ways never directly intended by program designers. Programs that provide services to infants and toddlers at high risk, such as EHS, represent an opportunity for supporting these families early, before maltreatment occurs, or before a pattern of ongoing recurrent maltreatment develops. More research on which families are particularly at risk for maltreatment, as well as on program and practice strategies that are most associated with preventing maltreatment are needed to increase the ability of early childhood programs to target those families most in need.
Acknowledgments
Support for this study was provided by the Centers for Disease Control and Prevention. The findings and conclusions in this paper are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. The authors would like to offer special thanks to those members of the Early Head Start Research Consortium who attended the Early Head Start-Child Welfare Study (EHS-CWS) Data Camps, and contributed to the development of this report: Judy Carta (University of Kansas), Lori Roggman (Utah State University), and Leanne Whiteside-Mansell (University of Arkansas-Little Rock). We also greatly appreciate the statistical consultation provided by John Willett (Harvard University) and Jason Newsom (Portland State University), who provided us with invaluable statistical consultation. We would also like to acknowledge the important roles played by states' child welfare agency research staff in the six EHS-CWS study states that participated in this project, without whose assistance this project would not have been possible: Arkansas, California, Kansas, Michigan, Washington, and Vermont.
Finally, we are indebted to the years of work by the Early Head Start Research Consortium. The findings reported here are based on research conducted as part of the national Early Head Start Research and Evaluation Project funded by the Administration for Children and Families (ACF), U.S. Department of Health and Human Services under Contract 105-95-1936 to Mathematica Policy Research, Princeton, NJ, and Columbia University's National Center for Children and Families, Teachers College, in conjunction with the Early Head Start Research Consortium. The Consortium consists of representatives from 17 programs participating in the evaluation, 15 local research teams, the evaluation contractors, and ACF. Research institutions in the Consortium (and principal researchers for conducting this research through 36 months of age) have included: ACF (Rachel Chazan Cohen, Judith Jerald, Esther Kresh, Helen Raikes, and Louisa Tarullo); Catholic University of America (Michaela Farber, Harriet Liebow, Nancy Taylor, Elizabeth Timberlake, and Shavaun Wall); Columbia University (Lisa Berlin, Christy Brady-Smith, and Jeanne Brooks-Gunn); Harvard University (Catherine Ayoub, Barbara Alexander Pan, and Catherine Snow); Iowa State University (Dee Draper, Gayle Luze, Susan McBride, Carla Peterson); Mathematica Policy Research (Kimberly Boller, Jill Constantine, Ellen Eliason Kisker, John M. Love, Diane Paulsell, Christine Ross, Peter Schochet, Susan Sprachman, Cheri Vogel, and Welmoet van Kammen); Medical University of South Carolina (Richard Faldowski, Gui-Young Hong, and Susan Pickrel); Michigan State University (Hiram Fitzgerald, Tom Reischl, and Rachel Schiffman); New York University (Mark Spellmann and Catherine Tamis-LeMonda); University of Arkansas (Robert Bradley, Richard Clubb, Andrea Hart, Mark Swanson, and Leanne Whiteside-Mansell); University of California, Los Angeles (Allison Sidle Fuligni, Carollee Howes and Claire Hamilton); University of Colorado at Denver (Robert Emde, Jon Korfmacher, JoAnn Robinson, Paul Spicer, and Norman Watt); University of Kansas (Jane Atwater, Judith Carta; and Jean Ann Summers); University of Missouri-Columbia (Mark Fine, Jean Ispa, and Kathy Thornburg); University of Pittsburgh (Beth Green, Carol McAllister, and Robert McCall); University of Washington College of Education (Eduardo Armijo and Joseph Stowitschek); University of Washington School of Nursing (Kathryn Barnard and Susan Spieker), and Utah State University (Lisa Boyce, Gina Cook, Catherine Callow-Heusser, and Lori Roggman).
Footnotes
Authors' note: This project was funded by contract #200-2010-35155, Division of Violence Prevention, National Center for Injury Prevention and Control, Centers for Disease Control and Prevention. Findings and conclusions in this report are those of the authors and do not necessarily represent the official views of the Centers for Disease Control and Prevention.
References
- Administration for Children and Families . Building their futures: How Early Head Start programs are enhancing the lives of infants and toddlers in low-income families. U.S. Department of Health and Human Services; Washington, DC: 2001. [Google Scholar]
- Administration for Children and Families Making a difference in the lives of infants and toddlers: The impacts of Early Head Start. 2002a Final technical report appendices, Vol. II, (Retrieved March 20, 2013 from http://www.acf.hhs.gov/sites/default/files/main/impacts_vol2.pdf)
- Administration for Children and Families . Making a difference in the lives of infants and toddlers and their families: The impacts of Early Head Start. U. S. Department of Health and Human Services; Washington, D.C.: 2002b. Final technical report. [Google Scholar]
- Anda RF, Felitti VJ, Bremner JD, Walker JD, Whitfield C, Perry BD, et al. The enduring effects of abuse and related adverse experiences in childhood. A convergence of evidence from neurobiology and epidemiology. European Archives of Psychiatry and Clinical Neuroscience. 2006;256:174–186. doi: 10.1007/s00406-005-0624-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Avellar S, Paulsell D, Sama-Miller E, Del Grosso P. Home Visiting Evidence of Effectiveness Review: Executive Summary. 2012 [Google Scholar]
- Barnett D, Manly JT, Cicchetti D. Defining child maltreatment: The interface between policy and research. In: Cicchetti D, Toth SL, editors. Child abuse, child development, and social policy. Ablex; Norwood, NJ: 1993. pp. 7–74. [Google Scholar]
- Belsky J. Etiology of child maltreatment: A developmental–ecological analysis. Psychological Review. 1993;75:81–95. doi: 10.1037/0033-2909.114.3.413. [DOI] [PubMed] [Google Scholar]
- Black D, Smith Slep AM, Heyman R. Risk factors for child psychological abuse. Aggression and Violent Behavior. 2001;6:189–201. [Google Scholar]
- Bolger KE, Patterson CJ. Sequelae of child maltreatment: Vulnerability and resilience. In: Luthar SS, editor. Resilience and vulnerability: Adaptation in the context of childhood adversities. Cambridge University Press; New York: 2003. pp. 156–181. [Google Scholar]
- Brodowski ML, Nolan CM, Gaudiosi JA, Yuan YY, Zikratova L, Oritz MJ, et al. Nonfatal maltreatment of infants — United States, October 2005–September 2006. Morbidity and Mortality Weekly Report. 2008;57(13):336–338. [PubMed] [Google Scholar]
- Bronfenbrenner U, Morris PA. The bioecological model of human development. Handbook of child psychology. 2006 [Google Scholar]
- Chalk R, Gibbons A, Scarupa HJ. The multiple dimensions of child abuse and neglect: New insights into an old problem. Child Trends; Washington, D.C.: 2002. (Retrieved March 11, 2013 from www.childtrends.org/Files/ChildAbuseRB.pdf) [Google Scholar]
- Child Welfare Information Gateway 2012 Retrieved from https://www.childwelfare.gov/famcentered, March 2012.
- Daro D. Child maltreatment research: Implications for program design. In: Cicchetti D, Toth S, editors. Child abuse, child development, and social policy: Advances in applied developmental psychology. Ablex; Norwood: 1993. pp. 331–367. [Google Scholar]
- DePanfilis D. Child neglect: Guide for prevention, assessment and intervention. U.S. Department of Health and Human Services, Child Welfare Information Gateway; Washington, D.C.: 2006. [Google Scholar]
- DePanfilis D, Zuravin SJ. The effect of services on the recurrence of child mal-treatment. Child Abuse & Neglect. 2002;26:187–205. doi: 10.1016/s0145-2134(01)00316-7. [DOI] [PubMed] [Google Scholar]
- Drake B, Pandey S. Understanding the relationship between neighborhood poverty and specific types of child maltreatment. Child Abuse & Neglect. 1996;20:1003–1018. doi: 10.1016/0145-2134(96)00091-9. [DOI] [PubMed] [Google Scholar]
- DuMont K, Mitchell-Herzfeld S, Greene R, Lee E, Lowenfels A, Rodriguez M, et al. Healthy Families New York (HFNY) randomized trial: Effects on early child abuse and neglect. Child Abuse & Neglect. 2008;32(3):295–315. doi: 10.1016/j.chiabu.2007.07.007. [DOI] [PubMed] [Google Scholar]
- Easterbrooks MA, Jacobs FH, Bartlett JD, Goldberg J, Contreras MM, Kotake C, et al. Initial findings from a randomized, controlled trial of Healthy Families Massachusetts: Early program impacts on young mothers' parenting. Pew Charitable Trusts; Washington, D. C.: 2012. [Google Scholar]
- Fang X, Brown DS, Florence CS, Mercy JA. The economic burden of child maltreatment in the US and implications for prevention. Child Abuse & Neglect. 2012;36:156–165. doi: 10.1016/j.chiabu.2011.10.006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fluke JD, Shusterman GR, Hollinshead D, Yuan YT. Rereporting and recurrence of child maltreatment: Findings from NCANDS. U.S. Department of Health and Human Services, Office of the Assistant Secretary for Planning and Evaluation; Washington, DC: 2005. [Google Scholar]
- Green BL, Ayoub C, Bartlett J, Furrer C, Von Ende A, Chazan-Cohen R, et al. The Early Head Start Child Welfare Study: Results from seven-site study of child welfare system involvement among national Early Head Start Research and Evaluation Project participants. Final report to the Centers for Disease Control and Prevention. 2013 Mar; [Google Scholar]
- Howard KS, Brooks-Gunn J. The role of home-visiting programs in preventing child abuse and neglect. Future of Children. 2009;19:119–146. doi: 10.1353/foc.0.0032. [DOI] [PubMed] [Google Scholar]
- Hunter DR, Lange K. A tutorial on MM algorithms. The American Statistician. 2004;58(1):30–37. [Google Scholar]
- Institute of Medicine and National Research Council . New directions in child abuse and neglect research. The National Academies Press; Washington, DC: 2013. [PubMed] [Google Scholar]
- Jones-Harden B, Chazan-Cohen R, Raikes H, Vogel C. Early Head Start home visitation: The role of implementation in bolstering program benefits. 2010 Unpublished manuscript. [Google Scholar]
- Kelly PJ, Lim LL. Survival analysis for recurrent event data: An application to childhood infectious diseases. Statistical Medicine. 2000;19(1):13–33. doi: 10.1002/(sici)1097-0258(20000115)19:1<13::aid-sim279>3.0.co;2-5. [DOI] [PubMed] [Google Scholar]
- Kohl PL, Barth RP. Child maltreatment recurrence among children remaining in-home: Predictors of re-reports. In: Haskins R, Wulczyn F, editors. Using research to improve policy and practice. Brookings Institution Press; Washington, D.C.: 2007. pp. 207–225. [Google Scholar]
- Leeb R, Lewis T, Zolotor AJ. A review of physical and mental health consequences of child abuse and neglect and implications for practice. American Journal of Lifestyle Medicine. 2011;5(5):454–468. [Google Scholar]
- Leiter J, Myers KA, Zingraff MT. Substantiated and unsubstantiated cases of child maltreatment: Do their consequences differ? Social Work Research. 1994;18(2):67–82. [Google Scholar]
- Leventhal JM, Geither JR. Incidence of serious injuries due to physical abuse in the United States: 1997 to 2009. Pediatrics. 2012;130:e847–e852. doi: 10.1542/peds.2012-0922. [DOI] [PubMed] [Google Scholar]
- Love JM, Chazan-Cohen R, Raikes HH, Brooks-Gunn J. What makes a difference: Early Head Start evaluation findings in a developmental context. Monographs of the Society for Research in Child Development. 2013;78(1):vii–viii. doi: 10.1111/j.1540-5834.2012.00699.x. [DOI] [PubMed] [Google Scholar]
- MacMillan HL, Wathan CN, Barlow J, Fergusson DM, Leventhal JM, Taussig HN. Interventions to prevent child maltreatment and associated impairment. Lancet. 2009;373:250–266. doi: 10.1016/S0140-6736(08)61708-0. [DOI] [PubMed] [Google Scholar]
- MacMillan HL, Wathen CN, Barlow J, Fergusson DM, Leventhal JM, Taussig HN. Child maltreatment: Interventions to prevent child maltreatment and associated impairment. The Lancet. 2009;373:250–266. doi: 10.1016/S0140-6736(08)61708-0. [DOI] [PubMed] [Google Scholar]
- Mikton C, Butchart A. Child maltreatment prevention: A systematic review of reviews. Bulletin of the World Health Organization. 2009;83:355–361. doi: 10.2471/BLT.08.057075. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO. Mplus user's guide. Author; Los Angeles, CA: 2005. [Google Scholar]
- Ocasio K, Morton C, Simmel C. An exploration of child welfare disparity differences between states. Journal of Public Child Welfare. 2013;7(1):79–97. [Google Scholar]
- Olds DL, Eckenrode J, Henderson CR, Kitzman H, Powers J, Cole R, et al. Long term effects of home visitation on maternal life course and child abuse and neglect: Fifteen year follow-up of a randomized trial. JAMA. 1997;278:637–643. [PubMed] [Google Scholar]
- Olds D, Henderson CR, Kitzman H, Cole R. Effects of prenatal and infancy nurse home visitation on surveillance of child maltreatment. Pediatrics. 1995;95(3):365–372. [PubMed] [Google Scholar]
- Paxson C, Haskins R. Preventing child maltreatment. Introducing the issue. Future of Children. 2009;19:3–18. [Google Scholar]
- Prentice RL, Williams BJ, Peterson AV. On the regression analysis of multivariate failure time data. Biometrika. 1981;68:373–379. [Google Scholar]
- Raikes HH, Vogel C, Love JM. Family subgroups and impacts at 2, 3, and 5: Variability by race/ethnicity and demographic risk. Monographs of the Society for Research in Child Development. 2013;78:64–92. [Google Scholar]
- Reynolds AJ, Mathieson L, Topitzes J. Do early childhood interventions prevent child maltreatment? A review of research. Child Maltreatment. 2009;14:182–206. doi: 10.1177/1077559508326223. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reynolds AJ, Robertson DL. School-based early intervention and later child maltreatment in the Chicago Longitudinal Study. Child Development. 2003;74:3–26. doi: 10.1111/1467-8624.00518. [DOI] [PubMed] [Google Scholar]
- Selph SS, Bougatsos C, Blazina I, Nelson HD. Behavioral interventions and counseling to prevent child abuse and neglect: A systematic review to update the U.S. preventive services task force recommendation. Annals of Internal Medicine. 2013;158:179–190. doi: 10.7326/0003-4819-158-3-201302050-00590. [DOI] [PubMed] [Google Scholar]
- Shonkoff JP, Garner AS, The Committee on Psychosocial Aspects of Child and Family Health. Committee on Early Childhood, Adoption, and Dependent Care, & Section on Developmental and Behavioral Pediatrics The lifelong effects of early childhood adversity and toxic stress. Pediatrics. 2012;129:e232–e246. doi: 10.1542/peds.2011-2663. [DOI] [PubMed] [Google Scholar]
- Stith SM, Lui T, Davies C, Boykin EL, Alder MC, Harris JM, et al. Risk factors in child maltreatment: A meta-analytic review of the literature. Aggression and Violent Behavior. 2009;14:13–29. [Google Scholar]
- Theodore A, Chang JJ, Runyan DK, Hunter WM, Bangdiwala SI, Agans R. The epidemiology of the physical and sexual maltreatment of children in the Carolinas. Pediatrics. 2005;115(3):e331–e333. doi: 10.1542/peds.2004-1033. [DOI] [PubMed] [Google Scholar]
- U.S. Department of Health and Human Services. Administration for Children and Families. Administration on Children, Youth, and Families, Children's Bureau Child maltreatment 2011. 2012 Retrieved January 28, 2013 from. http://www.acf.hhs.gov/programs/cb/resource/child-maltreatment-2011.
- U.S. Department of Health and Human Services, Administration for Children and Families, Administration on Children, Youth, and Families, Office of Planning, Research & Evaluation Early Head Start children in grade 5: Long-term follow-up of the Early Head Start Research and Evaluation Project study sample, final report. 2010 Retrieved March 30, 2013 from. http://www.acf.hhs.gov/programs/opre/resource/early-head-start-children-in-grade-5-long-term-followup-of-the-early-head.
- Veltman MW, Browne KD. Three decades of child maltreatment research: Implications for the school years. Trauma Violence Abuse. 2001;2:215–239. [Google Scholar]
- Vogel C, Brooks-Gunn J, Martin A, Klute MM. Impacts of Early Head Start participation on child and parent outcomes at 2, 3, and 5. Monographs of the Society for Research in Child Development. 2013;78:36–63. doi: 10.1111/j.1540-5834.2012.00699.x. [DOI] [PubMed] [Google Scholar]
- Waldfogel J. In: Differential response. Preventing child maltreatment. Dodge K, Coleman DL, editors. Guilford Press; New York: 2009. [Google Scholar]
- Whitaker DJ, Lutzker JR, Shelley G. Child maltreatment prevention priorities at the Centers for Disease Control and Prevention. Child Maltreatment. 2005;10(3):245–259. doi: 10.1177/1077559505274674. [DOI] [PubMed] [Google Scholar]
- Zielinski DS, Eckenrode J, Olds DL. Nurse home visitation and the prevention of child maltreatment: Impact on the timing of official reports. Development and Psychopathology. 2009;21(2):441–453. doi: 10.1017/S0954579409000248. [DOI] [PubMed] [Google Scholar]