

Abstract
Lowenthal, R. M., Gumpel, J. M., Kreel, L., McLaughlin, J. E., and Skeggs. D. B. L. (1974).Thorax, 29, 553-558. Carcinoid tumour of the thymus with systemic manifestations: a radiological and pathological study. Following recent reports of an unusual mediastinal tumour described as `mediastinal endocrine neoplasm of probable thymic origin, related to carcinoid tumour' (Rosai and Higa, 1972), a further case, in a 72-year-old man, has been studied.
Polyarthropathy was the presenting feature, and the patient also had clubbing of the fingers and clinical evidence of a probable proximal myopathy and a peripheral neuropathy. These non-metastatic systemic manifestations have not previously been described with this type of tumour.
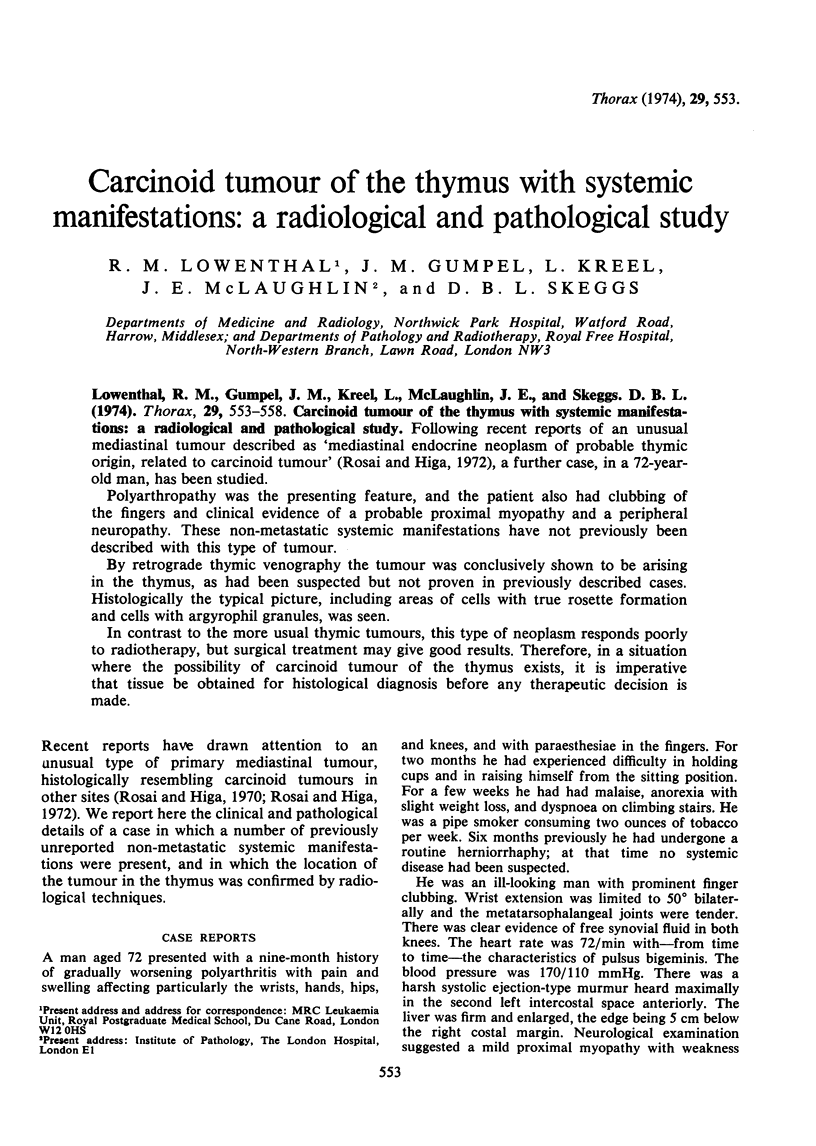
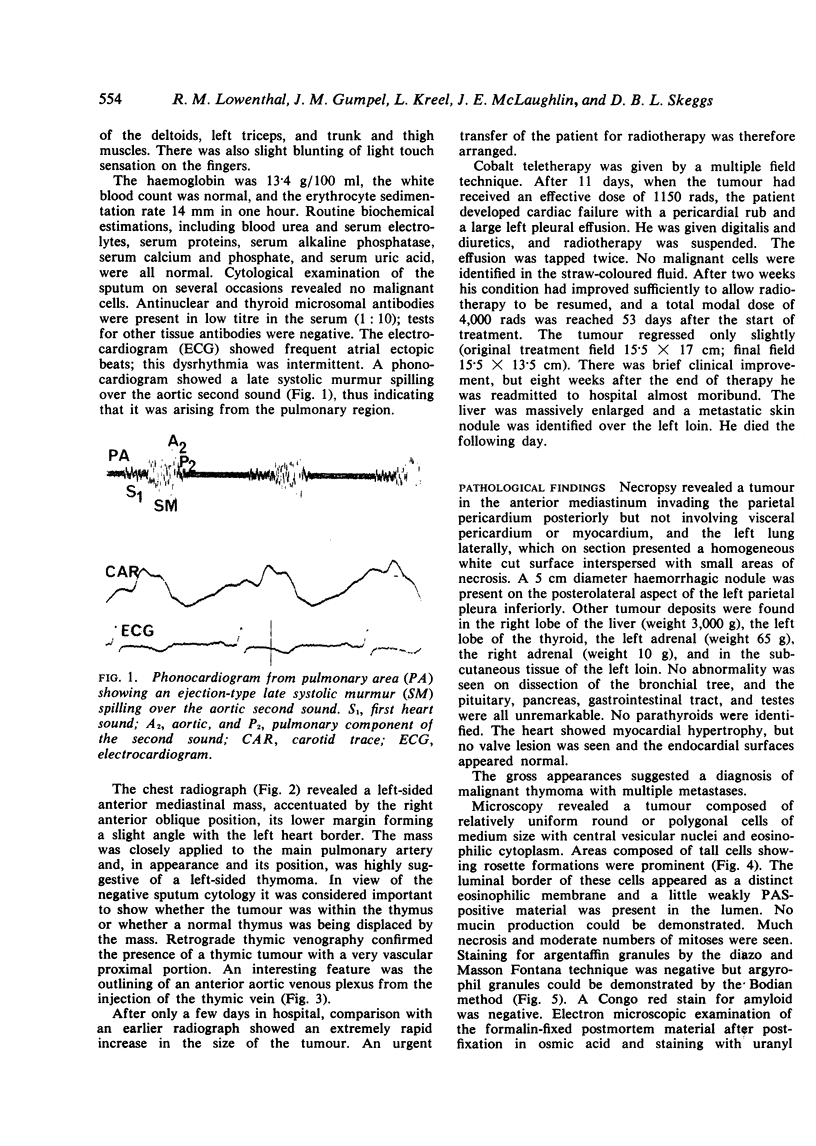
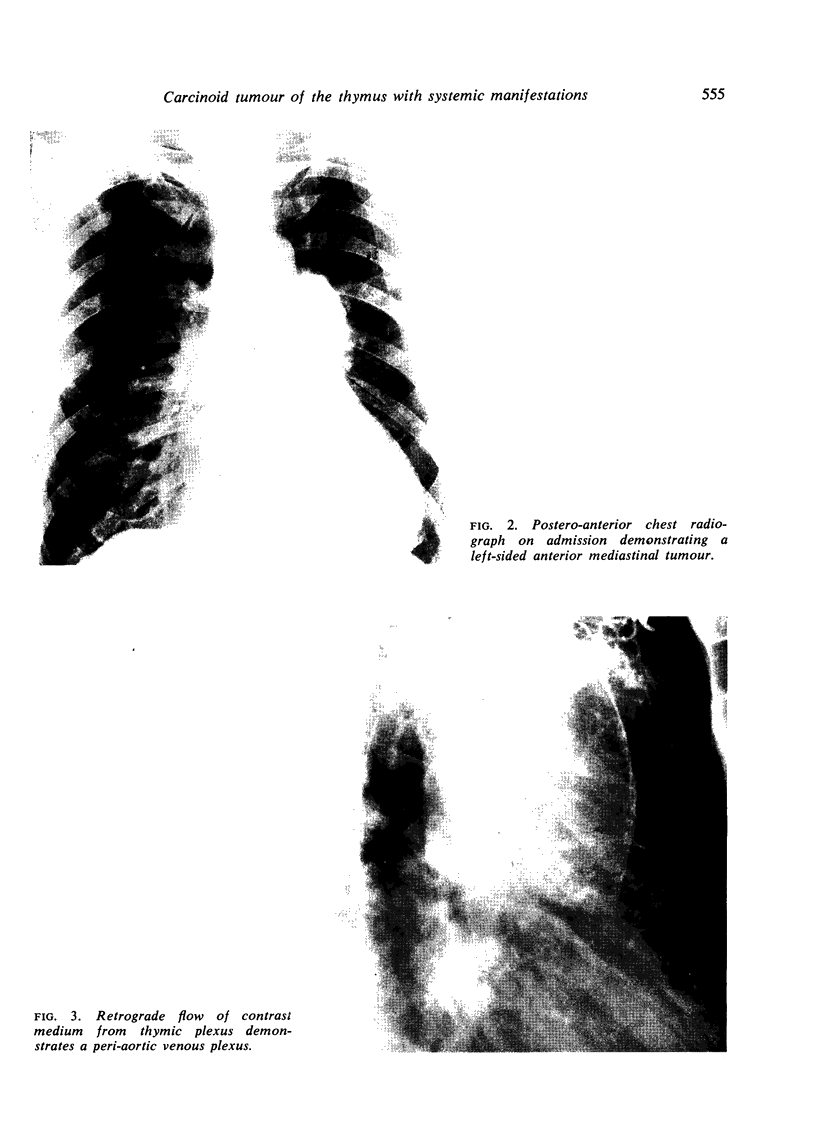
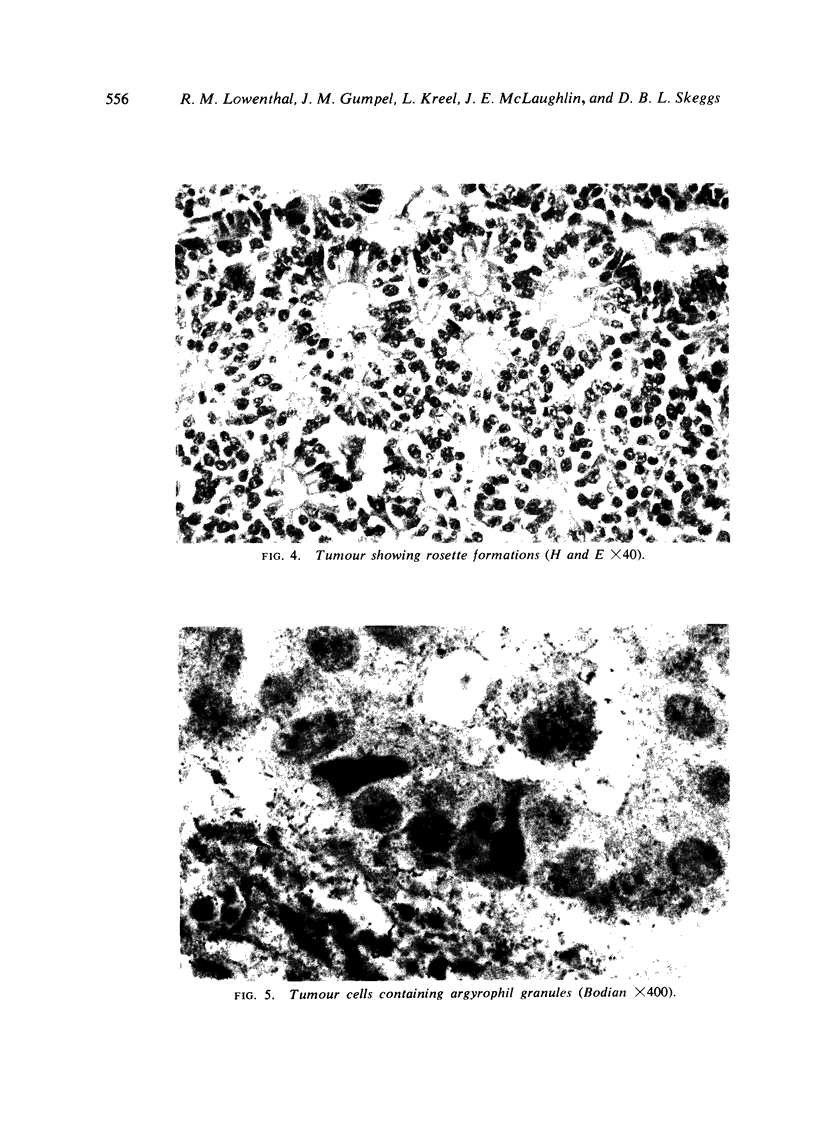
By retrograde thymic venography the tumour was conclusively shown to be arising in the thymus, as had been suspected but not proven in previously described cases. Histologically the typical picture, including areas of cells with true rosette formation and cells with argyrophil granules, was seen.
In contrast to the more usual thymic tumours, this type of neoplasm responds poorly to radiotherapy, but surgical treatment may give good results. Therefore, in a situation where the possibility of carcinoid tumour of the thymus exists, it is imperative that tissue be obtained for histological diagnosis before any therapeutic decision is made.
Full text
PDF
Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Lemon F. C., Fine M. B., Grasso S. G., Kinsell L. W. ACTH-like activity in a thymoma associated with gonadal dysgenesis. J Clin Endocrinol Metab. 1966 Jan;26(1):1–5. doi: 10.1210/jcem-26-1-1. [DOI] [PubMed] [Google Scholar]
- Macadam R. F., Vetters J. M. Fine structural evidence for hormone secretion by a human thymic tumour. J Clin Pathol. 1969 Jul;22(4):407–409. doi: 10.1136/jcp.22.4.407. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pearse A. G. The cytochemistry and ultrastructure of polypeptide hormone-producing cells of the APUD series and the embryologic, physiologic and pathologic implications of the concept. J Histochem Cytochem. 1969 May;17(5):303–313. doi: 10.1177/17.5.303. [DOI] [PubMed] [Google Scholar]
- Rosai J., Higa E., Davie J. Mediastinal endocrine neoplasm in patients with multiple endocrine adenomatosis. A previously unrecognized association. Cancer. 1972 Apr;29(4):1075–1083. doi: 10.1002/1097-0142(197204)29:4<1075::aid-cncr2820290457>3.0.co;2-o. [DOI] [PubMed] [Google Scholar]
- Skeggs D. B. Radiotherapy of thymic tumours in myasthenia gravis. Proc R Soc Med. 1968 Aug;61(8):760–762. doi: 10.1177/003591576806100808. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Weichert R. F., 3rd The neural ectodermal origin of the peptide-secreting endocrine glands. A unifying concept for the etiology of multiple endocrine adenomatosis and the inappropriate secretion of peptide hormones by nonendocrine tumors. Am J Med. 1970 Aug;49(2):232–241. doi: 10.1016/s0002-9343(70)80079-1. [DOI] [PubMed] [Google Scholar]