

Why was the cohort set up?
The effects of exposure to ionizing radiation have been studied for decades. The health effects of moderate to high exposure are well characterized, but the effects of low-level, chronic exposure remain a subject of continued debate.1 Moreover, repeated or protracted low-dose rate exposures to ionizing radiation have become increasingly common over the past quarter-century.1 The largest contributor to this trend has been medical radiation expos-ure.2,3 Since the 1980s, studies of nuclear industry workers have been conducted to provide direct information about these effects.2,3 These cohorts are well suited for this purpose: they include large number of workers, with individual (person-specific) monitoring of external doses and many years of follow-up. Estimates from early, cohort-specific studies, were, however, compatible with a wide range of possibilities, from a reduction of risk at low doses to risks higher than those on which current radiation protection recommendations are based.
To further improve the precision of estimates of radiation-induced cancer risk following protracted low doses of ionizing radiation and to strengthen the scientific basis of radiation protection standards, an International Collaborative Study of Cancer Risk among Radiation Workers in the Nuclear Industry, the ‘15-Country Study’, was carried out using a common core protocol in 15 coun-tries.3–5 Information was collected on nearly 600000 workers and a thorough study of errors in recorded doses was carried out to evaluate the comparability of recorded dose estimates across facilities and time, and to identify and quantify sources of bias and uncertainties in dose estimates, which were taken into account in the statistical analyses of the results.6
Within the 15-country study, the cohorts of nuclear workers from France, the UK and the USA provided the vast majority of the information available on early nuclear workers. They provided 62% of the person-years of follow-up and 67% of cancer and leukaemia deaths. In recent years, the cohorts from France, the UK and the USA have been updated.
The International Nuclear Workers Study (INWORKS) was therefore established to provide a basis for deriving more precise quantitative estimates of the risk of chronic, low-level exposure to ionizing radiation, through an improved understanding of the association between protracted low-dose exposure to ionizing radiation and mortality due to solid and haematological cancers, and circulatory diseases. Specifically, the INWORKS consortium builds upon the work conducted for the 15-country study by taking advantage of data from the most informative cohorts involved in that study. INWORKS has the potential to improve on estimates obtained from the 15-country study and the knowledge derived from the information on workers exposed to chronic, low-dose exposures will contribute to the understanding of risks to members of the public exposed to background (low-level, chronic) radiation. INWORKS is organized by, and data are housed at, the International Agency for Research on Cancer (IARC).
Who is in the cohort?
INWORKS is a retrospective cohort study of workers employed by: the Atomic Energy Commission (CEA), AREVANuclear Cycle (formerly COGEMA) and the National Electricity Company (EDF) in France; the Departments of Energy and Defense in the USA; and, in the UK, by nuclear industry employers included in the National Registry for Radiation Workers (NRRW). Table 1 lists the facilities and companies represented in the study countries. Inclusion criteria are based on completeness and quality of data, start of facility operations and other considerations; details of the country-specific inclusion criteria can be found elsewhere.7–10 Workers who were employed in the nuclear industry for less than 1 year were excluded from INWORKS. In France, workers were given the opportunity, required by the French Data Protection Authority, to refuse participation; however, none refused to participate. In the USA, worker information is based on existing records, with no effort made to directly contact any participants; because there is minimal risk to participants, the National Institute for Occupational Safety and Health Institute Review Board (NIOSH IRB) waived requirements for informed consent. Finally, UK workers have the opportunity to refuse to participate in the NRRW and associated studies; less than 1% of UK radiation workers refused to participate.
Table 1.
Nuclear facilities included in the INWORKS cohort, 1943–2005
| County | Facilities/companies included |
|---|---|
| France | Atomic Energy Commission (CEA) AREVA Nuclear Cycle (formerly General Company of Nuclear Fuel COGEMA) National Electricity Company (EDF) |
| USA | Hanford Site (Richland, WA) Savannah River Site (SRS, Aiken, SC) Oak Ridge National Laboratory (ORNL, Oak Ridge, TN) Idaho National Laboratory (INL, Idaho Falls, ID) Portsmouth Naval Shipyard (PNS, Kittery, ME) |
| UK | Atomic Weapons Establishment British Energy Generation and Magnox Electric Ltd British Nuclear Fuels plc Ministry of Defence UK Atomic Energy Authority |
Table 2 summarizes the number of workers included in INWORKS by country and by some key characteristics. Approximately 20% of the US workers are women. In contrast, the UK and French cohorts include approximately 9% and 13% female workers, respectively. The mean year of birth for the USA cohort is 1934, and the mean years of birth for French and UK cohort members are 1947 and 1944, respectively; this reflects the differing employment dates of the different cohorts. The average age at the start of employment is similar for workers from each country, ranging from age 27 to 30 years. The mean age at the end of follow-up for the USA cohort members is, on average, nearly a decade greater than for the UK and French cohorts. In total these workers contributed 8.2 million person-years of observation to the study. A summary of the person-time and number of mortality events experienced by each cohort grouped by categories of age, birth cohort, socioeconomic status and sex can be found in the eSupplement (available as Supplementary data at IJE online).
Table 2.
Characteristics of INWORKS cohorts, 1943–2005
| Characteristics | France (n=59003) | UK (n=147866) | US (n=101 428) | Total (n=308297) | ||||
|---|---|---|---|---|---|---|---|---|
| Sex | ||||||||
| Male | 51567 | 87.40% | 134812 | 91.17% | 81883 | 80.73% | 268262 | 87.01% |
| Female | 7436 | 12.60% | 13054 | 8.83% | 19545 | 19.27% | 40035 | 12.99% |
| Year of birth | ||||||||
| Mean(SD) | 1947 (13) | 1944 (18) | 1934 (17) | 1941 (18) | ||||
| Range | 1894–1975 | 1877–1983 | 1873–1973 | 1873–1983 | ||||
| Mean age, years (SD) | ||||||||
| At start employment | 27 (7) | 28 (11) | 30 (9) | 28 (10) | ||||
| At last observation | 56 (13) | 54 (15) | 65(1) | 58 (15) | ||||
| Mean duration of employment (SD) in years | 21 (10) | 13 (10) | 14 (11) | 15 (11) | ||||
| Mean duration of follow-up (SD) in years | 25 (9) | 23 (12) | 33 (13) | 27 (12) | ||||
| Total person-years | 1469500 | 3410483 | 3341049 | 8221032 | ||||
| Vital status | ||||||||
| Alive | 52565 | 89.09% | 118775 | 80.33% | 65573 | 64.65% | 236913 | 76.85% |
| Deceased | 6310 | 10.69% | 25307 | 17.11% | 35015 | 34.52% | 66632 | 21.61% |
| Emigrated or lost to follow-up | 128 | 0.22% | 3784 | 2.56% | 840 | 0.83% | 4752 | 1.54% |
SD, standard deviation.
Table 3 reports the distribution of individuals in categories of cumulative dose, average annual dose, average cumulative dose and total measured whole-body dose by country and for the pooled cohort. Workers in the USA and UK cohorts received higher ionizing radiation doses than the workers in the French cohort, both in terms of average annual dose and average cumulative dose.
Table 3.
Distribution of whole-body dose (mSv) among INWORKS cohort participants, 1943–2005
| Cohort | Cumulative dose category
|
Individual mean (SD)
|
Total collective dose | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 0 | > 0–5 | > 5–10 | > 10–20 | > 20–50 | > 50–100 | > 100–200 | > 200–300 | > 300–400 | > 400–500 | 500+ | Annual dose | Cumulative dose | ||
| France | 16797 | 19391 | 4958 | 5534 | 6684 | 3518 | 1726 | 302 | 69 | 17 | 7 | 0.81 (1.68) | 16 (36) | 948,157 |
| UK | 17493 | 62238 | 16352 | 15295 | 17310 | 9215 | 5676 | 1947 | 937 | 598 | 805 | 2.17 (5.09) | 27 (76) | 4,063,380 |
| USA | 16839 | 41632 | 10292 | 10343 | 10534 | 5488 | 3719 | 1496 | 622 | 242 | 221 | 1.39 (2.96) | 23 (60) | 2,355,205 |
| Total | 51129 | 123261 | 31602 | 31172 | 34528 | 18221 | 11121 | 3745 | 1628 | 857 | 1033 | 1.66 (4.02) | 24 (65) | 7,366,742 |
The number of deaths in INWORKS is 66632. The total number of deaths from cancer and circulatory disease is summarized in Table 4 by subtype. International Classification of Disease codes used to group outcomes can be found in the eSupplement (available as Supplementary data at IJE online). Cancer and circulatory disease rates increase with age, and therefore the number of deaths due to these causes has approximately tripled since the last time that the French, USA and UK cohorts were analysed together with a reported 19748 deaths due to solid and haematological cancers and 27 848 deaths due to circulatory disease (Table 4).
Table 4.
Number of deaths in INWORKS by category of underlying cause of death, 1943–2005
| Cause of death | Cohort
|
|||
|---|---|---|---|---|
| France | UK | USA | Total | |
| All solid cancers | 2356 | 6994 | 8607 | 17957 |
| Bladder | 56 | 273 | 250 | 579 |
| Brain | 84 | 227 | 283 | 594 |
| Breast | 75 | 75 | 260 | 410 |
| Colon / small intestine | 172 | 542 | 856 | 1570 |
| Connective tissue | 8 | 32 | 61 | 101 |
| Oesophagus | 92 | 329 | 226 | 647 |
| Kidney | 70 | 174 | 247 | 491 |
| Larynx | 57 | 63 | 65 | 185 |
| Liver/gallbladder/ biliary | 132 | 115 | 206 | 453 |
| Lung/trachea/bronchus | 595 | 2244 | 2963 | 5802 |
| Ovary | 21 | 22 | 79 | 122 |
| Pancreas | 139 | 325 | 512 | 976 |
| Peritoneum | 47 | 67 | 31 | 145 |
| Prostate | 149 | 630 | 906 | 1685 |
| Rectum | 61 | 313 | 165 | 539 |
| Stomach | 99 | 542 | 263 | 904 |
| Thyroid | 6 | 16 | 16 | 38 |
| Other solid cancers | 493 | 1005 | 1218 | 2716 |
| All haematopoietic and lymphoid cancers | 196 | 564 | 1031 | 1791 |
| Hodgkin disease | 17 | 33 | 54 | 104 |
| Non-Hodgkin lymphoma | 64 | 227 | 419 | 710 |
| All leukaemia | 79 | 208 | 397 | 684 |
| CLL | 19 | 41 | 78 | 138 |
| Leukaemia excluding CLL | 56 | 167 | 311 | 531 |
| Chronic myeloid leukaemia | 14 | 39 | 47 | 100 |
| Multiple myeloma | 36 | 96 | 161 | 293 |
| Circulatory diseases | 1483 | 11687 | 14678 | 27848 |
| Hypertension | 39 | 165 | 380 | 584 |
| Ischaemic heart disease | 587 | 7904 | 8972 | 17463 |
| Other heart diseases | 357 | 717 | 2324 | 3398 |
| Cerebrovascular | 338 | 2047 | 2059 | 4444 |
| Other cardiovascular diseases | 162 | 854 | 943 | 1959 |
Longer follow-up allows for better estimation of temporal factors affecting the relationship between low-level ionizing radiation and mortality; and the large number of observed events allows more effective consideration of the association of mortality risk of specific solid and haematological cancers and exposure to ionizing radiation.
How often has the cohort been followed up?
In France, follow-up commenced in 1968 because the French national death registry has only recorded information on individual causes of death since 1968; follow-up is updated biannually with cause of death obtained from the French National Institute for Medical Research.11 In the UK, follow-up commences from 1955 with updates of mortality information obtained on an ongoing basis from central registries for England, Wales and Scotland, as well as at intervals from regional offices for workers resident in the Channel Islands, the Isle of Man or Northern Ireland.9,10 In the USA, follow-up commenced with start of operations at each facility (1944 for the earliest nuclear facility in the USA), and cause of death is obtained from the National Death Index (from 1979 onwards, and from US State and multiple other sources before that year). The cause of death is confirmed through periodic searches of social security administration records conducted by the US National Institute for Occupational Safety and Health.7 Because information is obtained from employers and national registries, loss to follow-up is minimal: only 0.22%, 2.56% and 0.83% of employees were lost to follow-up or emigrated from the French, UK and US cohorts, respectively (Table 2).
What has been measured?
Information on demographic variables, including sex and date of birth, as well as race for US workers, was obtained from employment records. Information on periods of radiation work, job titles and facilities of employment, and a classification of workers according to socioeconomic status was collected as well. Information regarding date and cause of death is collected (and periodically updated) by linkage to population registries in each country. Because of the nature of the study, information regarding individual health-related behaviours could not be collected. Because a large percentage of the cohort is now deceased, and because of the large number of workers, it would not be feasible to collect this information for the current consortium.
Workers from the nuclear industry represent a unique population to study the health effects of ionizing radiation; they are mostly exposed to radiation at low levels over the course of their working life. Moreover, unlike typical occupational cohort studies, all workers included in INWORKS have records that provide individual quantitative radiation dose estimates. Workers in INWORKS were mainly exposed to external radiation, usually gamma-rays, and doses were measured regularly with personal dosimeters. For all participating cohorts, records of individual recorded doses have been kept since the very beginning of the industry in the 1940s.
The main sources of errors in recorded external doses were quantified in order to account for the evolution of technology since the beginning of the nuclear industry and for differences in practices between facilities or countries.6 Correction factors were derived by dosimeter type to account for bias and associated uncertainties and recorded doses were converted into organ doses.6 The International Commission for Radiological Protection (ICRP) provides conversion coefficients to obtain estimates of organ-specific doses from external radiation exposure. Previous studies utilized these estimates from ICRP-5112 and ICRP-7413 reports. Recently, these estimates have been updated by the ICRP,14 allowing separate organ dose estimation for men and women. This is important for diseases that are highly sex specific; for example, the revised coefficients allow a sex-specific estimation of dose to the breast for women. The revised coefficients have therefore been used in the INWORKS analyses.
What has been found? Key findings and publications
A summary of the published results regarding the participating cohorts and previous 15-country study is provided in Table 5; we also provide a brief summary of some of the more recent analyses undertaken within each country. Country-specific studies, as well as the previous 15-country study, find a positive relationship between mortality from solid cancer and leukaemia excluding chronic lymphocytic leukaemia (CLL) and occupational exposure to ionizing radiation with varying levels of magnitude and precision. Estimates for the excess relative risk for solid cancers associated with 1 Sv increase in external radiation exposure in the French, UK and US cohorts were 0.34 [90% confidence interval (CI): −0.56, 1.38,8 0.28 (90% CI: 0.02, 0.56)10 and 0.14 (95% CI: −0.17, 0.48),7 respectively. The excess relative risk for solid cancer estimated in the 15-country study was 0.87 (95% CI: 0.03, 1.88).3
Table 5.
Results from recent analyses of the member countries of the INWORKS consortium, 1943–2005
| Country | Cohorts included | Mortality | ERR per Sv (90% CI) |
|---|---|---|---|
| UK | full NRRW9 | All malignant cancer excluding leukemia Leukaemia excluding CLLa Circulatory disease Ischaemic heart disease Cerebrovascular disease |
0.28 (0.02, 0.56) 1.71 (0.06, 4.29) 0.25 (0.03, 0.49) 0.26 (0.00, 0.55) 0.16 (−0.34, 0.77) |
| France | AREVA NC, EDF, COGEMA8,11 | Solid cancer Leukaemia excluding CLLa Circulatory disease Ischaemic heart disease Cerebrovascular disease |
0.34 (−0.56,1.38) 3.96 (<0, 16.82) 0.31 (−0.90,1.74) 0.71 (−1.20, 3.18) 0.99 (< 0.00, 5.05) |
| USA | Hanford, SRS, ORNL, INL, PNS7 | Solid cancerb Leukaemia excluding CLLb Cardiovascular diseaseb |
0.14 (−0.17, 0.48) 1.7 (−0.22, 4.7) 0.026 (−0.25, 0.32) |
| 15-Country Study3–5 | Solid cancerb Leukaemia excluding CLLa Circulatory diseaseb Ischaemic heart diseaseb Cerebrovascular diseaseb |
0.87 (0.03, 1.88) 1.93 (<0, 8.47) 0.09 (−0.43, 0.70) −0.01 (−0.59 0.69) 0.88 (−0.67, 3.16) |
|
| INWORKS15 | Leukaemia excluding CLLa | 2.96 (1.17, 5.21) |
ERR, excess relative risk; CLL, chronic lymphocytic leukaemia; CI, confidence interval;<0 indicates that the lower bound of the confidence interval could not be calculated.
Indicates 2-year lag. Otherwise, a 10-year exposure lag is used.
Indicates 95% confidence interval rather than 90%.
All the previous studies, individual and pooled, find a positive relationship between mortality from leukaemia excluding CLL and occupational exposure to ionizing radiation with varying levels of magnitude; 3–5,7–9,11 generally, these estimates are statistically imprecise due to a low number of observed events. The excess relative risk estimates for leukaemia excluding CLL from French, UK, and US cohorts are: 3.96 (90% CI: < 0.0, 16.82),11 1.71 (90% CI: 0.06, 4.29)9 and 1.7 (95% CI: −0.22, 4.7),7 respectively. In the 15-country study, the risk estimate was 1.93 (95% CI: < 0.00, 8.47). In contrast, estimates from the Life Span Study (LSS) study of atomic bomb survivors, restricted to males ages 20 to 60, is 2.63 (90% CI: 1.50, 4.27).
To date, the key findings from INWORKS involve analyses of associations between radiation and leukaemia and lymphoma.15 Notably, the excess relative rate of mortality due to leukaemia excluding CLL was 2.96 (90% CI: 1.17, 5.21) per Gy estimated red bone marrow dose. Figure 1 provides a visualization of the change in the relative risk of leukaemia per unit increase in red bone marrow radiation dose. The estimated association between radiation dose and leukaemia excluding CLL, obtained from analysis of INWORKS, is substantially more precise than prior analyses of any specific cohort, larger than (and more precise than) the estimated association from the 15-country study and similar in magnitude and precision to the estimate from the LSS. Similarly to the previous analyses of the 15-country study data and the LSS, associations between radiation dose and leukaemia were based on estimated red bone marrow dose. In contrast, previous country-specific analyses were based on recorded whole-body dose estimates. The results represent a major finding from occupational cohort mortality studies involving personal quantitative estimates of dose derived from individual monitoring over decades of employment for exposure to an occupational carcinogen. These findings provide a stronger empirical basis for protection from protracted or repeated low-dose radiation exposure.
Figure 1.
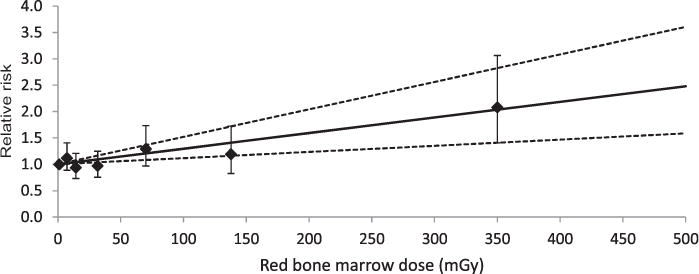
Relative risk of leukaemia, except chronic lymphocytic leukaemia, associated with dose to red bone marrow among nuclear workers. Nuclear Workers in France, the UK and the USA, 1943–2005 (Leuraud et al., in revision). The solid line is the fitted linear dose-response model (excess relative risk per Gy=2.96) and the dotted lines are the likelihood-based, linear fitted 90% CI. Bars represent 90% CI for relative risks. The diamonds represent the estimated relative risk at the level of exposure on the x-axis.
What are the main strengths and weaknesses of this study?
As can be seen in Tables 2–4, the INWORKS study, by including a substantial number of additional years of follow-up (9 in the NRRW and the Idaho National Laboratory, 10 in France, 19 at Hanford and 21 at the Oak Ridge National Laboratory), has considerably increased the statistical power and information that can be drawn about the effects of low-level chronic exposure to ionizing radiation compared with previous international studies. Further, workers who had potential for internal radiation dose and were excluded from the 15-country study are included in INWORKS. When compared with the 15-country study, the average length of follow-up has gone from 12.75 to 26.67 years; the number of cancer deaths has multiplied by 3.75 and the number of leukaemia deaths by 2.5. These increases will not only improve the statistical precision of direct estimates of risk following low-dose protracted radiation exposure, but also allow the investigation of risk from a number of different subtypes of cancer and specific non-cancer diseases and the investigation of the effect of age and time since exposure on risk of radiation-induced mortality. The international cohort is still young, however, with an average age of 58, an age at which the incidence of many cancer and non-cancer diseases is increasing. Further follow-up of this international cohort, in which much effort has been invested over the years to better characterize exposure, is thus likely to increase our understanding of radiation risk following low-dose protracted exposures in the next decades. Further, recent advances in classification of disease and in dosimetry (permitting more pertinent conversion factors to estimate doses to specific organs using the originally recorded dosi-metric quantities) allow now, and in the future, for the better quantification of risks associated with ionizing radiation. This better quantification of risk following low protracted exposure will also assist in understanding and explaining risk to the general population with exposures to either natural background or nuclear emissions at chronic low levels.
As with any pooling of cohorts there are, however, a number of limitations. Due to the size of the pooled cohort and the study design, it was not logistically feasible to obtain information on potential confounders (including smoking or other occupational exposures) for all cohort members. As with previous studies of radiation workers, it will be important to consider the patterns of exposure—in the main, nuclear workers accruing occupational exposure at low levels and over a long time. Further, occupational cohort studies are typically susceptible to a healthy worker hire effect, which has historically concerned the selection of workers into a cohort who are healthier than the general population and which therefore requires that care is taken in the interpretation of results.16 In terms of estimating radiation risks, an important limitation is the fact that we are unable to separately estimate the neutron component in radiation risk estimation. Measuring neutron exposure has been a challenging task, since the energy of neutrons could range from less than 1 electron volt (eV) to around 20 MeV and detectors were not able to measure all energies for relatively long periods of time.17 It is impossible to ensure that neutron exposure would have been correctly estimated for all workers in our international cohort. Some individuals might have had unrecorded or poorly estimated neutron doses. For some facilities and time periods, it was also impossible to separately estimate the neutron component of the external radiation dose. Because of this, and in order for our estimates of risk in relation to external radiation doses to be as accurate as possible, we have regrouped workers into categories of potential for neutron exposures.
Can I get hold of the data? Where can I find out more?
This study’s data are not freely available. For reasons of ethics and permissions from different agencies, the data are maintained at the International Agency for Research on Cancer (Lyon, France); further, it is not possible to send the data outside the agency. Proposals for possible collaborations in further analyses of the data should be addressed to Dr AusreleKesminiene [KesminieneA@iarc.fr] and will be reviewed by the INWORKS consortium.
Supplementary Material
Inworks in a Nutshell.
The INWORKS consortium was established to combine informative cohorts of nuclear workers from France, the UK and the USA, to study the association between cancer and non-cancer diseases and radiation exposure.
A total of 308 297 workers provided 8.2 million person-years of follow-up from 1944 to 2005.
The primary exposure of interest is external exposure to photon radiation. Records were obtained from selected employers and from employment elsewhere to estimate career radiation doses for each worker.
Proposals for possible collaborations in further analyses of the data should be addressed to Dr Ausrele Kesminiene [KesminieneA@iarc.fr] and will be reviewed by the INWORKS consortium.
Acknowledgments
The construction of the UK cohort was undertaken by Public Health England (PHE) which operates the UK’s NRRW (National Registry for Radiation Workers). PHE thank all of the organizations and individuals participating in the NRRW for their cooperation and the NRRW Steering Group for their continued support. The findings and conclusions in this report are those of the authors and do not necessarily represent views of the National Institute for Occupational Safety and Health.
Funding: The work reported in this paper was undertaken during the tenure of a postdoctoral fellowship awarded by the International Agency for Research on Cancer. This work was partly funded by the Centers for Disease Control and Prevention (5R03 0H010056-02) and the Ministry of Health, Labour and Welfare of Japan (GA No 2012-02-21-01). The construction of the French cohort was partially supported by IRSN, AREVA and EDF. For the US contribution, funding was provided by the National Institute for Occupational Safety and Health, by the U.S. Department of Energy through an agreement with the U.S. Department of Health and Human Services and through a grant received by the University of North Carolina from the National Institute for Occupational Safety and Health (R03 OH-010056).
Footnotes
Supplementary data are available at IJE online.
Conflict of interest: We have no competing financial interests to declare.
References
- 1.National Research Council (U.S.) Health Risks from Exposure to Low Levels of Ionizing Radiation : BEIR VII Phase 2. Washington, DC: National Academies Press; 2006. Committee to Assess Health Risks from Exposure to Low Level of Ionizing Radiation. [PubMed] [Google Scholar]
- 2.Cardis E, Vrijheid M, Blettner M, et al. The 15-Country Collaborative Study of Cancer Risk among Radiation Workers in the Nuclear Industry: estimates of radiation-related cancer risks. Radiat Res. 2007;167:396–416. doi: 10.1667/RR0553.1. [DOI] [PubMed] [Google Scholar]
- 3.Cardis E, Vrijheid M, Blettner M, et al. Risk of cancer after low doses of ionising radiation – retrospective cohort study in 15 countries. BMJ. 2005;331:77–80B. doi: 10.1136/bmj.38499.599861.E0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Vrijheid M, Cardis E, Ashmore P, et al. Ionizing radiation and risk of chronic lymphocytic leukemia in the 15-Country Study of nuclear industry workers. Radiat Res. 2008;170:661–65. doi: 10.1667/RR1443.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Vrijheid M, Cardis E, Ashmore P, et al. Mortality from diseases other than cancer following low doses of ionizing radiation: results from the 15-Country Study of nuclear industry workers. Int J Epidemiol. 2007;36:1126–35. doi: 10.1093/ije/dym138. [DOI] [PubMed] [Google Scholar]
- 6.Thierry-Chef I, Marshall M, Fix JJ, et al. The 15-Country Collaborative Study of Cancer Risk among Radiation Workers in the Nuclear Industry: study of errors in dosimetry. Radiat Res. 2007;167:380–95. doi: 10.1667/RR0552.1. [DOI] [PubMed] [Google Scholar]
- 7.Schubauer-Berigan M, Daniels RD, Tseng CY, Richardson DB. Cancer mortality through 2005 among a pooled cohort of U.S. nuclear workers exposed to external ionizing radiation. Radiat Res. 2015 May 26; doi: 10.1667/RR13988.1. [Epub ahead of print.] [DOI] [PubMed] [Google Scholar]
- 8.Metz-Flamant C, Samson E, Caer-Lorho S, Acker A, Laurier D. Solid cancer mortality associated with chronic external radiation exposure at the French atomic energy commission and nuclear fuel company. Radiat Res. 2011;176:115–27. doi: 10.1667/RR2528.1. [DOI] [PubMed] [Google Scholar]
- 9.Muirhead CR, O’Hagan JA, Haylock RG, et al. Mortality and cancer incidence following occupational radiation exposure: third analysis of the National Registry for Radiation Workers. Br J Cancer. 2009;100:206–12. doi: 10.1038/sj.bjc.6604825. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Muirhead CR, O’Hagan JA, Haylock RGE, et al. HPA-RPD-062 - Third Analysis of the National Registry for Radiation Workers: Occupational Exposure to Ionising Radiation in Relation to Mortality and Cancer Incidence. Didcot, UK: Health Protection Agency, Centre for Radiation, Chemical and Environmental Hazards; 2009. [Google Scholar]
- 11.Metz-Flamant C, Laurent O, Samson E, et al. Mortality associated with chronic external radiation exposure in the French combined cohort of nuclear workers. Occup Environ Med. 2013;70:630–38. doi: 10.1136/oemed-2012-101149. [DOI] [PubMed] [Google Scholar]
- 12.ICRP. Data for use in protection against external radiation. ICRP Publication 51. Ann ICRP. 1987;17:2–3. [PubMed] [Google Scholar]
- 13.ICRP. Conversion coefficients for use in radiological protection against external radiation. ICRP Publication 74. Ann IRCP. 1996;26:3–4. [PubMed] [Google Scholar]
- 14.ICRP. Conversion coefficients for radiological protection quantities for external radiation exposures. ICRP Publication 116. Ann ICRP. 2010;40:2–5. doi: 10.1016/j.icrp.2011.10.001. [DOI] [PubMed] [Google Scholar]
- 15.Leuraud K, Richardson DB, Cardis E, et al. Ionizing radiation and leukaemia and lymphoma: Findings from an international cohort study of radiation-monitored workers. Lancet Haematol. 2015;7:e276–e281. doi: 10.1016/S2352-3026(15)00094-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Naimi AI, Richardson DB, Cole SR. Causal inference in occupational epidemiology: accounting for the healthy worker effect by using structural nested models. Am J Epidemiol. 2013;178:1681–86. doi: 10.1093/aje/kwt215. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Tanner RJ, Thomas DJ, Bartless DT, Hager LG, Horwood N, Taylor GC. Effect of Energy Dependence of Response of Neutron Personal Dosimeters Routinely Used in the UK on Accuracy of Dose Estimation. Didcot, UK: National Radiological Protection Board; 2002. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.