

A 57-year-old man was referred to our department from another hospital after major bleeding following thoracoscopic biopsy of an undiagnosed giant mass in the posterior mediastinum. The bleed had been controlled by emergency posterolateral thoracotomy and diagnosis of low grade malignant solitary fibrous tumor of the pleura (SFTP) then obtained, but radical resection was not performed.
A chest computed tomography (CT) scan showed a large hypervascular posterolateral mediastinal mass adherent to the mediastinal pleura, the left lung, the thoracic aorta, and close to the esophagus (Figs 1, 2).
Figure 1.
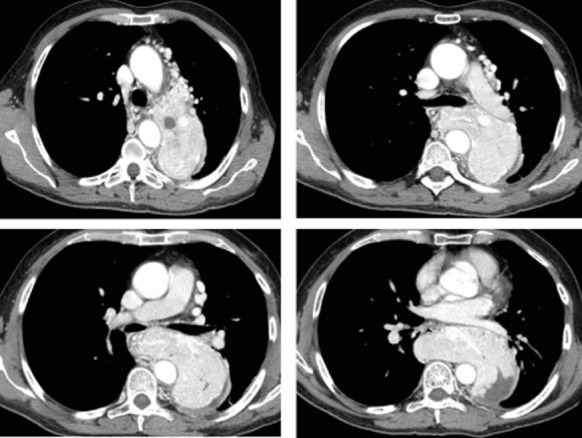
Axial post-contrast computed tomography (CT) images at four different levels of the chest (shown here at the mediastinum window level), disclosed a large left-posterior mediastinal lesion characterized by many intralesional and surrounding vessels, strictly adherent to the mediastinal pleura and the left lung, and very close to the esophagus (medially dislocated by the mass).
Figure 2.

Sagittal reformatted computed tomography (CT) image shows the craniocaudal extension of the mass and its extensive contact with the thoracic aorta.
We performed redo posterolateral thoracotomy. The mass was then dissected and effectively separated from the esophagus and pericardium. However, the mediastinal pleura of the left lung was widely infiltrated and intrapericardial left pneumonectomy was required to achieve radical en bloc resection (Fig 3). No residual disease was observed at the end of the procedure.
Figure 3.
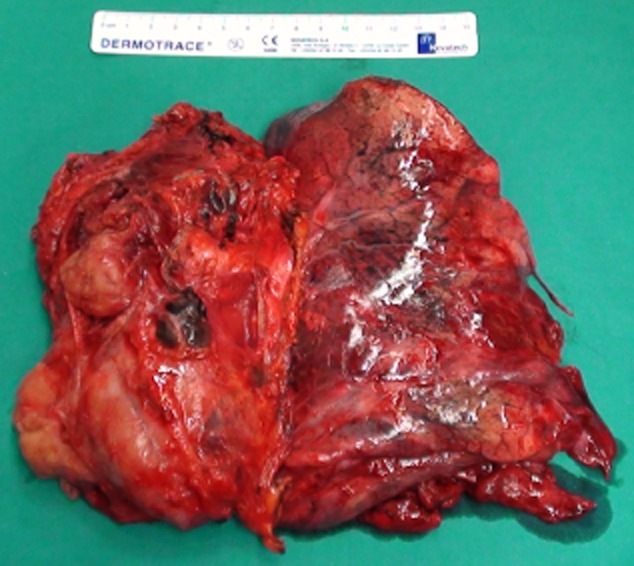
Surgical specimen disclosing the radically resected solitary fibrous tumor of the pleura involving the mediastinal surface of the left lung completely resected en bloc by left intrapericardial pneumonectomy.
Histological examination confirmed malignant SFTP CD 34 and CD 99 positive, cytokeratin negative, weighing 985 grams without the left lung.
Postoperative paramedian left vocal cord paralysis resulting in moderate dysphonia was documented by video laryngoscopy and a speech therapy program was instituted. The patient was discharged two weeks after surgery without any major complication.
Two years of follow up, performed by chest CT scan every four months, did not disclose any local or distant relapse.
SFTP is a rare, slow-growing tumor whose origin is widely recognized as the mesenchymal cells of submesothelial tissues of the pleura, rather than mesothelial cells.1 The tumor tends to grow into a huge mass before local compression symptoms develop. Angiography or CT scan frequently discloses multiple feeding vessels, including several intercostal, internal mammary, inferior phrenic, and bronchial arteries.2 The ideal treatment of SFTP is based on radical surgical excision that is generally curative in all benign cases and in approximately half of malignant ones.1 Complete resection of giant SFTP may be challenging because of poor exposure, significant blood supply, strong adhesions, and often the direct involvement of nearby structures, however, there is little evidence for alternative management of this particular tumor (radiotherapy and chemotherapy).3
The prognosis for patients with benign SFTP is generally favorable with a five-year overall survival rate ranging from 79 to 100%, however, the risk of recurrence is high after the resection of a malignant sessile SFTP, although long-term survival is possible, ranging from 46 to 100%.4
Adequate pre-operative blood storage is recommended in cases of planned giant SFTP resection, together with a detailed explanation to acquaint patients with details of the therapeutic schedule, including major lung and mediastinal resection.
Acknowledgments
Anne Collins edited the English text.
Disclosure
No authors report any conflict of interest.
References
- England DM, Hochholzer L, McCarthy MJ. Localized benign and malignant fibrous tumors of the pleura. A clinicopathologic review of 223 cases. Am J Surg Pathol. 1989;13:640–658. doi: 10.1097/00000478-198908000-00003. (Published erratum appears in 1991; 818.) [DOI] [PubMed] [Google Scholar]
- Guo J, Chu X, Sun YE, Zhang L, Zhou N. Giant solitary fibrous tumor of the pleura: an analysis of five patients. World J Surg. 2010;34:2553–2557. doi: 10.1007/s00268-010-0715-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marak CP, Dorokhova O, Guddati AK. Solitary fibrous tumor of the pleura. Med Oncol. 2013;30:573. doi: 10.1007/s12032-013-0573-0. [DOI] [PubMed] [Google Scholar]
- Cardillo G, Lococo F, Carleo F, Martelli M. Solitary fibrous tumors of the pleura. Curr Opin Pulm Med. 2012;18:339–346. doi: 10.1097/MCP.0b013e328352f696. [DOI] [PubMed] [Google Scholar]