

Abstract
Background
The National Central Cancer Registry of China (NCCR) is responsible for cancer surveillance. Local cancer registries in each province submit data for annual publication. The incidence and mortality of lung cancer in China in 2010 by age, gender, and area is reported in this article.
Methods
In 2013, 145 of 219 population-based cancer registries' 2010 data were selected after quality evaluation. Classification included Western, Middle, and Eastern areas, and the crude incidence and mortality rates of lung cancer were calculated by age, gender, and urban and rural. Age-standardized rates were determined by China and World standard population data. The 6th National Population Census data of China was used, combined with the registries' data to estimate the lung cancer burden in China in 2010.
Results
Lung cancer had the highest incidence and mortality in China for men and women. It was estimated that 605 946 lung cancer cases were diagnosed in China in 2010, with a crude incidence rate of 46.08/100 000, and 486 555 patients died from lung cancer, with a crude mortality rate of 37.00/100 000. Age-standardized rates for incidence were 35.23/100 000 and 35.04/100 000, respectively. Incidence and mortality rates for lung cancer were higher in men and urban areas than those in women and rural areas, reaching a peak for subjects of 80–84 years old.
Conclusion
Lung cancer has the highest incidence and mortality of all cancers in China, especially for males in urban areas. Our findings justify the need to plan and develop effective interventions, such as air pollution control and smoking deterrents, to control and prevent the spread of lung cancer in China.
Keywords: Cancer epidemiology, Chinese data, lung cancer
Introduction
Incidence and mortality attributed to lung cancer has risen steadily since the 1930s. Efforts to improve outcomes have not only led to a greater understanding of the etiology of lung cancer, but also the histologic and molecular characteristics of individual lung tumors. Lung cancers, primarily caused by tobacco smoking, are the major public health problem in the United States and many other parts of the world.1–9 In China, lung cancer has been the leading cancer diagnosed and the cause of cancer-related death for many years.8–10 Recent reports also describe an increasing trend of lung cancer in China.11 Lung cancer is particularly prevalent in civil cities and in males. Cigarette smoking and air pollution have been established as risk factors of the disease. Population-based cancer registries play an important role in collecting and providing cancer data. In China, the first population-based cancer registry was established in 1958 in Linzhou, Henan Province.12 But the development of cancer registries was limited in the 20th century. In 2002, the National Central Cancer Registry (NCCR) of China was established, acting as a federal bureau for systematic management of cancer surveillance. The population-based cancer registries located around China routinely collect data on patient demographics, primary tumor site and tumor morphology. In this study, the lung cancer burden, and the incidence and mortality of lung cancer in China were estimated by using 145 population-base cancer registries' data of 2010. Incidence and mortality by age group, gender, and geographic areas were calculated. The updated results from this study will provide important policy suggestions and practical implications.
Material and methods
Data source
The NCCR of China is responsible for cancer data collection, evaluation, and publication from each population-based cancer registry located in China. All new cancer cases were reported to the local cancer registries when first diagnosed in any hospitals, community health centers or first discovered in other departments, including the Basic Medical Insurances for Urban Residents and the New-Rural Cooperative Medical System. The Vital Statistical Database was linked with the cancer database for updating vital statistics and also as a data supplement.
By 1 June 2013, 219 cancer registries (92 cities and 157 counties) from 31 provinces submitted 2010 data to the NCCR. Data covered about 207 229 403 people, accounting for 15.42% of the 2010 national population. The cancer registries coded data with the International Classification of Diseases for Oncology 3rd edition (ICD-O-3) and the International Statistical Classification of Diseases and Related Health Problems 10th Revision (ICD-10). Invasive cases of lung cancer (ICD10: C33-C34) were extracted and analyzed from the overall cancer database.
The National Statistics Bureau of China provided the sixth National Population Census data.13
Quality control
Based on the Guideline of Chinese Cancer Registration and the standard of data inclusion in Cancer Incidence in Five Continents Volume IX, cancer registration data were evaluated by the quality indicators of proportion of morphological verification (MV%), percentage of death certification only (DCO%) and mortality to incidence ratio (M/I).14–18 The detailed standard for data inclusion has been published previously.19 Generally, data with a DCO% less than 20%, an overall MV% between 50% to 95%, and a M/I between 0.55–0.95 were considered acceptable.
Statistical analysis
Based on the standards of the National Statistics Bureau, China was classified into Eastern, Middle, and Western areas. We calculated the cancer registration data by strata variables of each area (Eastern/Middle/Western), kind (urban/rural), and gender (men/women). The age-specific incidence and mortality rate in the three different areas, and the 2010 National Census Population data were used to estimate incidence and mortality. The classification criteria were as follows:
According to the GB2260-2009 standard, prefecture-level cities were classified into urban areas, whereas counties and county-level cities were classified into rural areas.
The classification of Eastern, Middle, and Western areas is based on the standards of the National Statistics Bureau.
The Eastern areas: Beijing, Tianjin, Hebei, Liaoning, Shanghai, Jiangsu, Zhejiang, Fujian, Shandong, Guangdong and Hainan province.
The Middle areas: Heilongjiang, Jilin, Shanxi, Anhui, Jiangxi, Henan, Hubei and Hunan.
The Western areas: Inner Mongolia, Guangxi, Chongqing, Sichuan, Guizhou, Yunnan, Tibet, Shanxi, Gansu, Qinghai, Ningxia and Xinjiang.
Crude incidence and mortality rates of lung cancer were prepared by gender, area, and for 19 age groups (0–, 1–4, 5–84 by 5 years, 85+ years). Age-standardized rates were calculated using the Chinese population (2000) and Segi's World population. The cumulative risk of developing or dying from cancer before 75 years of age (in the absence of competing causes of death) was calculated and presented as a percentage. Software including MS-Excel, IARCcrgTools2.05 issued by IARC and IACR were used for data checking and evaluation. SAS software was used to calculate the incidence and mortality rates.
Results
A total of 145 population-based cancer registries were selected for this study after quality evaluation. The population covered by these registries was 158 403 248, including 80 355 188 men and 78 048 060 women, accounting for 11.86% of the 2010 national population. Among them, 63 registries were from urban areas, covering a total of 92 433 739 of the population. Eighty-two registries were from rural areas, covering a total of 65 969 509 of the population. The MV%, DCO%, and M/I ratio for the national pooled data were 54.20%, 4.37%, and 0.84 respectively. In urban areas, the MV%, DCO%, and M/I ratio were 59.31%, 3.90%, and 0.85 respectively. In rural areas, they were 45.47%, 5.16%, and 0.82, respectively.
Incidence
In 2010, it was estimated that there were 605 946 new lung cancer diagnoses in China (416 333 men and 189 613 in women), with a crude incidence rate of 46.08 per 100 000 (age-standardized rates by Chinese population [CASIR] of 35.23 per 100 000; age-standardized rates by world population [WASIR] of 35.04 per 100 000), accounting for 19.59% of all new cancer cases. Among the new cases, 348 107 (57.45%) came from urban areas and 257 839 (42.55%) from rural areas. Among the 605 946 new lung cancer diagnoses, there were 240 858 (39.75%) cases from Eastern areas, 207 748 (34.28%) cases from Middle areas and 157 340 (25.97%) cases from Western areas in China (Table 1).
Table 1.
The quality control index of lung cancer in China in 2010
| Areas | Gender | M/I | MV% | DCO% | UB% |
|---|---|---|---|---|---|
| ALL | Both | 0.84 | 54.20 | 4.37 | 0.73 |
| Male | 0.85 | 54.47 | 4.29 | 0.70 | |
| Female | 0.83 | 53.65 | 4.53 | 0.77 | |
| Urban areas | Both | 0.85 | 59.31 | 3.90 | 0.89 |
| Male | 0.86 | 59.58 | 3.88 | 0.86 | |
| Female | 0.84 | 58.76 | 3.95 | 0.94 | |
| Rural areas | Both | 0.82 | 45.47 | 5.16 | 0.46 |
| Male | 0.83 | 46.04 | 4.97 | 0.45 | |
| Female | 0.81 | 44.23 | 5.58 | 0.47 |
DCO, death certification only; MI, mortality to incidence; MV, morphological verification; UB, unknown basis of diagnosis.
The crude incidence rate for lung cancer was 46.08/100 000 in 2010, accounting for 19.59% of overall new cancer cases in China. The CASIR and WASIR were 35.23/100 000 and 35.04/100 000, respectively. Among the patients aged 0–74, the cumulative incidence rate was 4.28%.
Lung cancer occurred more often in men than women. For men, the crude incidence rate was 61.86/100 000, whereas the CASIR and WASIR were 49.27/100 000 and 49.16/100 000, respectively. For women, the crude incidence rate was 29.54/100 000, whereas the CASIR and WASIR were 21.66/100 000 and 21.40/100 000, respectively. The crude incidence rate in urban areas was 52.52/100 000, which was remarkably higher than that in rural areas (39.54/100 000). After age standardization, the incidence rate in urban areas (36.39/100 000 for WASIR) was still higher than that in rural areas (33.25/100 000 for WASIR) (Table 2).
Table 2.
Lung cancer incidence in China in 2010
| Areas | Gender | No. of cases | Crude rate | Ratio | CASIR | WASIR | Cum rate | TASR | Rank |
|---|---|---|---|---|---|---|---|---|---|
| (1/105) | (%) | (1/105) | (1/105) | 0–74 (%) | 35–64 (1/105) | ||||
| ALL | Both | 605 946 | 46.08 | 19.59 | 35.23 | 35.04 | 4.28 | 50.61 | 1 |
| Male | 416 333 | 61.86 | 23.03 | 49.27 | 49.16 | 5.98 | 69.26 | 1 | |
| Female | 189 613 | 29.54 | 14.75 | 21.66 | 21.40 | 2.56 | 31.33 | 2 | |
| Urban | Both | 348 107 | 52.52 | 20.48 | 36.62 | 36.39 | 4.42 | 50.48 | 1 |
| Male | 238 816 | 70.39 | 24.48 | 51.22 | 51.05 | 6.15 | 68.80 | 1 | |
| Female | 109 291 | 33.78 | 15.10 | 22.52 | 22.24 | 2.63 | 31.36 | 2 | |
| Rural | Bot | 257 839 | 39.54 | 18.50 | 33.39 | 33.25 | 4.10 | 50.74 | 1 |
| Male | 177 517 | 53.20 | 21.33 | 46.75 | 46.73 | 5.75 | 69.85 | 1 | |
| Female | 80 322 | 25.23 | 14.31 | 20.49 | 20.25 | 2.47 | 31.25 | 2 | |
| Eastern | Bot | 240 858 | 43.80 | 18.74 | 33.05 | 32.78 | 4.03 | 46.58 | 1 |
| Male | 160 454 | 57.00 | 21.99 | 45.24 | 45.01 | 5.52 | 62.13 | 1 | |
| Female | 80 404 | 29.95 | 14.47 | 21.41 | 21.07 | 2.52 | 30.56 | 2 | |
| Middle | Bot | 207 748 | 49.17 | 20.62 | 37.92 | 37.88 | 4.72 | 56.06 | 1 |
| Male | 146 787 | 68.09 | 25.21 | 54.22 | 54.31 | 6.73 | 78.44 | 1 | |
| Female | 60 961 | 29.46 | 14.33 | 22.03 | 21.87 | 2.67 | 32.98 | 2 | |
| Western | Both | 157 340 | 45.95 | 19.66 | 35.56 | 35.34 | 4.14 | 50.33 | 1 |
| Male | 109 092 | 62.01 | 21.98 | 49.82 | 49.64 | 5.76 | 69.39 | 1 | |
| Female | 48 248 | 28.98 | 15.86 | 21.60 | 21.39 | 2.47 | 30.44 | 1 |
CASIR, Age-standardized rate (China standard population, 2000); WASIR, Age-standardized rate (World standard population); Cum, cumulative; TASR, Truncated age-standardized rate (World standard population).
Age-specific incidence rates of lung cancer for both genders and areas were compared. The lung cancer age-specific incidence rates were relatively low up to 45 years of age in each area then increased dramatically, peaking in age group 80–84 or above 85 years old (378.82/100 000). Generally, lung cancer among men had a higher age-specific incidence rate than that among women, except for those in younger age groups (<30 years old). Similarly, the age-specific lung cancer rates in urban areas were generally higher than that in rural areas, except for subjects in younger age groups. The age-specific incidence rates varied in different areas with a similar curve (Table 3).
Table 3.
Age-specific incidence rates of lung cancer in China in 2010 (1/105)
| Age group | All areas | Urban areas | Rural areas | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Both | Male | Female | Both | Male | Female | Both | Male | Female | |
| ALL | 46.08 | 61.86 | 29.54 | 52.52 | 70.39 | 33.78 | 39.54 | 53.20 | 25.23 |
| 0– | 0.22 | 0.00 | 0.47 | 0.35 | 0.00 | 0.76 | 0.00 | 0.00 | 0.00 |
| 1– | 0.01 | 0.02 | 0.00 | 0.00 | 0.00 | 0.00 | 0.03 | 0.06 | 0.00 |
| 5– | 0.01 | 0.00 | 0.01 | 0.01 | 0.00 | 0.03 | 0.00 | 0.00 | 0.00 |
| 10– | 0.05 | 0.03 | 0.08 | 0.07 | 0.00 | 0.14 | 0.04 | 0.08 | 0.00 |
| 15– | 0.17 | 0.18 | 0.15 | 0.15 | 0.10 | 0.20 | 0.19 | 0.26 | 0.11 |
| 20– | 0.53 | 0.59 | 0.46 | 0.34 | 0.45 | 0.24 | 0.67 | 0.71 | 0.64 |
| 25– | 1.11 | 1.42 | 0.79 | 1.09 | 1.37 | 0.81 | 1.12 | 1.46 | 0.78 |
| 30– | 2.46 | 2.62 | 2.30 | 2.52 | 2.60 | 2.43 | 2.42 | 2.64 | 2.20 |
| 35– | 6.34 | 7.18 | 5.46 | 6.08 | 6.67 | 5.45 | 6.56 | 7.61 | 5.46 |
| 40– | 14.95 | 17.72 | 12.07 | 13.69 | 16.40 | 10.93 | 16.20 | 19.01 | 13.22 |
| 45– | 29.69 | 37.90 | 21.19 | 28.57 | 36.13 | 20.97 | 30.81 | 39.61 | 21.41 |
| 50– | 55.38 | 75.59 | 34.15 | 57.89 | 80.63 | 34.09 | 52.78 | 70.39 | 34.21 |
| 55– | 97.15 | 136.34 | 57.14 | 98.50 | 136.86 | 58.78 | 95.52 | 135.72 | 55.21 |
| 60– | 149.40 | 211.73 | 84.92 | 147.86 | 206.76 | 85.59 | 151.39 | 218.26 | 84.08 |
| 65– | 207.58 | 295.21 | 118.30 | 216.11 | 306.55 | 121.20 | 196.22 | 279.60 | 114.57 |
| 70– | 290.83 | 408.52 | 174.42 | 310.50 | 434.61 | 184.63 | 266.00 | 374.64 | 161.89 |
| 75– | 353.01 | 508.54 | 213.67 | 382.63 | 552.22 | 233.61 | 314.79 | 453.48 | 187.41 |
| 80– | 378.82 | 560.71 | 234.77 | 420.21 | 629.00 | 264.41 | 323.29 | 475.89 | 192.47 |
| 85+ | 315.40 | 486.29 | 213.10 | 366.15 | 570.77 | 251.05 | 247.02 | 382.27 | 159.08 |
The lung cancer incidence and mortality rates were higher in urban than those in rural areas. The incidence and mortality rates of lung cancer in Middle urban areas were remarkably higher than those in Eastern and Western urban areas. But in rural areas, however, Western areas had the highest rates of lung cancer incidence and mortality (Fig 1).
Figure 1.
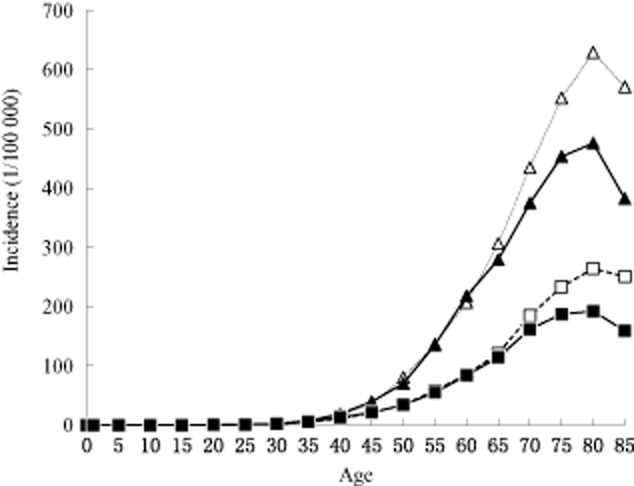
Age-specific incidence rate of lung cancer in China in 2010 (1/105).  , Urban male;
, Urban male;  , Urban female;
, Urban female;  , Rural male;
, Rural male;  , Rural female.
, Rural female.
Mortality
It was estimated that about 486 555 people died of lung cancer in 2010 (336 786 men and 149 769 women), with a crude mortality rate of 37.00 per 100 000 (age-standardized rates by Chinese population [CASMR] 27.93 per 100 000; age-standardized rates by world population [WASMR] of 27.72 per 100 000). The cumulative rates of incidence and mortality from age 0 to 74 were 4.28% and 3.24%, respectively. Among the 486 555 lung cancer deaths, 279 919 (57.53%) came from urban areas and 206 636 (42.47%) from rural areas, with 206 044 (42.35%) from Eastern areas, 161 784 (33.25%) from Middle and 118 727 (24.40%) from Western areas, respectively.
The mortality rate of lung cancer was much higher in men than that in women. In men, the crude mortality rates, CASMR, and WASMR were 50.04/100 000, 39.79/100 000, and 39.62/100 000, respectively. In women, they were 23.33/100 000, 16.62/100 000, and 16.41/100 000, respectively. In urban areas, the crude mortality rates, CASMR, and WASMR were 42.23/100 000, 28.88/100 000, and 28.62/100 000, respectively. In rural areas, they were 31.69/100 000, 26.61/100 000, and 26.47/100 000, respectively, which were much lower than those in urban areas (Table 4).
Table 4.
Age-specific mortality rates of lung cancer in China in 2010 (1/105)
| Areas | Gender | No. of cases | Crude rate | Ratio | CASMR | WASMR | Cum rate | TASR | Rank |
|---|---|---|---|---|---|---|---|---|---|
| (1/105) | (%) | (1/105) | (1/105) | 0–74 (%) | 35–64 (1/105) | ||||
| ALL | Both | 486 555 | 37.00 | 24.87 | 27.93 | 27.72 | 3.24 | 34.36 | 1 |
| Male | 336 786 | 50.04 | 26.85 | 39.79 | 39.62 | 4.59 | 48.49 | 1 | |
| Female | 149 769 | 23.33 | 21.32 | 16.62 | 16.41 | 1.86 | 19.75 | 1 | |
| Urban | Both | 279 919 | 42.23 | 27.05 | 28.88 | 28.62 | 3.32 | 33.10 | 1 |
| Male | 192 438 | 56.72 | 29.46 | 41.04 | 40.81 | 4.69 | 46.95 | 1 | |
| Female | 87 481 | 27.04 | 22.92 | 17.31 | 17.04 | 1.91 | 18.65 | 1 | |
| Rural | Both | 206 636 | 31.69 | 22.42 | 26.61 | 26.47 | 3.12 | 35.76 | 1 |
| Male | 144 348 | 43.26 | 24.02 | 38.09 | 38.00 | 4.45 | 50.19 | 1 | |
| Female | 62 288 | 19.56 | 19.42 | 15.64 | 15.50 | 1.81 | 21.02 | 1 | |
| Eastern | Both | 206 044 | 37.47 | 25.20 | 27.80 | 27.46 | 3.23 | 32.99 | 1 |
| Male | 137 924 | 49.00 | 26.78 | 38.69 | 38.35 | 4.48 | 45.37 | 1 | |
| Female | 68 120 | 25.37 | 22.51 | 17.57 | 17.24 | 1.98 | 20.23 | 1 | |
| Middle | Both | 161 784 | 38.29 | 26.33 | 29.20 | 29.10 | 3.43 | 36.91 | 1 |
| Male | 115 490 | 53.57 | 29.31 | 42.72 | 42.65 | 5.01 | 53.59 | 1 | |
| Female | 46 294 | 22.37 | 21.00 | 16.20 | 16.08 | 1.82 | 19.69 | 1 | |
| Western | Both | 118 727 | 34.67 | 22.64 | 26.64 | 26.55 | 3.02 | 33.32 | 1 |
| Male | 83 372 | 47.39 | 24.15 | 38.03 | 38.03 | 4.27 | 47.07 | 1 | |
| Female | 35 355 | 21.23 | 19.71 | 15.59 | 15.48 | 1.74 | 18.98 | 1 |
ASRcn, Age-standardized rate (China standard population, 2000); ASRwld, Age-standardized rate (World standard population); Cum, cumulative; TASR, Truncated age-standardized rate (World standard population).
Age-specific mortality rates by gender and area are shown in Table 5. The trend for lung cancer mortality in different age groups was similar to the trend of incidence. Both for men and women, in urban and in rural areas, the mortality reached a peak in subjects of 80–84 years old (Fig 2).
Table 5.
Age-specific mortality of lung cancer in cancer registration areas in 2010 (1/105)
| Age group | All areas | Urban areas | Rural areas | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Both | Male | Female | Both | Male | Female | Both | Male | Female | |
| ALL | 37.00 | 50.04 | 23.33 | 42.23 | 56.72 | 27.04 | 31.69 | 43.26 | 19.56 |
| 0– | 0.10 | 0.09 | 0.11 | 0.00 | 0.00 | 0.00 | 0.27 | 0.25 | 0.29 |
| 1– | 0.04 | 0.06 | 0.00 | 0.02 | 0.03 | 0.00 | 0.06 | 0.12 | 0.00 |
| 5– | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 | 0.00 |
| 10– | 0.03 | 0.02 | 0.04 | 0.00 | 0.00 | 0.00 | 0.06 | 0.04 | 0.09 |
| 15– | 0.09 | 0.13 | 0.04 | 0.11 | 0.17 | 0.05 | 0.07 | 0.10 | 0.04 |
| 20– | 0.32 | 0.40 | 0.24 | 0.24 | 0.33 | 0.14 | 0.39 | 0.46 | 0.32 |
| 25– | 0.57 | 0.79 | 0.35 | 0.60 | 0.80 | 0.39 | 0.55 | 0.78 | 0.33 |
| 30– | 1.68 | 1.93 | 1.42 | 1.57 | 1.79 | 1.34 | 1.77 | 2.05 | 1.48 |
| 35– | 3.71 | 4.42 | 2.96 | 3.39 | 3.71 | 3.05 | 3.98 | 5.02 | 2.89 |
| 40– | 8.98 | 11.46 | 6.39 | 7.97 | 9.68 | 6.23 | 9.97 | 13.18 | 6.56 |
| 45– | 18.05 | 24.21 | 11.66 | 17.19 | 23.47 | 10.87 | 18.90 | 24.92 | 12.47 |
| 50– | 36.84 | 51.16 | 21.80 | 35.10 | 49.12 | 20.43 | 38.64 | 53.26 | 23.21 |
| 55– | 67.32 | 96.94 | 37.09 | 65.59 | 96.50 | 33.58 | 69.39 | 97.48 | 41.22 |
| 60– | 106.83 | 154.78 | 57.22 | 104.24 | 150.64 | 55.20 | 110.14 | 160.23 | 59.75 |
| 65– | 159.65 | 229.70 | 88.29 | 166.59 | 237.73 | 91.92 | 150.43 | 218.63 | 83.63 |
| 70– | 243.07 | 342.03 | 145.18 | 261.52 | 363.37 | 158.23 | 219.78 | 314.33 | 129.16 |
| 75– | 336.02 | 482.82 | 204.50 | 361.51 | 515.20 | 226.45 | 303.13 | 442.00 | 175.58 |
| 80– | 395.34 | 579.20 | 249.72 | 442.03 | 650.13 | 286.73 | 332.70 | 491.08 | 196.92 |
| 85+ | 379.08 | 579.26 | 259.24 | 426.45 | 648.02 | 301.83 | 315.23 | 494.60 | 198.61 |
Figure 2.
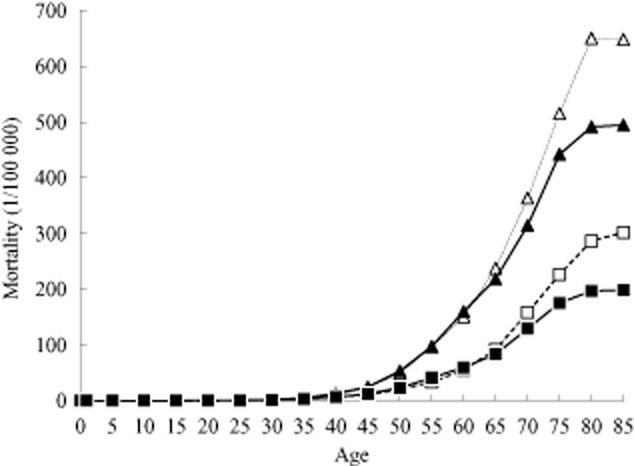
Age-specific mortality of lung cancer in China in 2010 (1/105).  , Urban male;
, Urban male;  , Urban female;
, Urban female;  , Rural male;
, Rural male;  , Rural female.
, Rural female.
Discussion
This study provides updated incidence and mortality rates of lung cancer in 2010 in China, based on 145 population-based cancer registries' data. The crude incidence and mortality of lung cancer in China were 46.08/100 000 and 37.00/100 000. The age-standardized incidence and mortality rates by World standard population were 35.04/100 000 and 27.72/100 000. Men have a higher risk of lung cancer than women, and people in urban areas have a higher risk than in rural areas. The most recent lung cancer statistics and burden estimation may provide basic information for lung cancer prevention and control in China.
In 2010 in China, lung cancer was the leading cause of cancer death, as well as the most commonly diagnosed cancer. However, compared to the cancer incidence and mortality of 2009 in cancer registry areas in China,20 we found the crude rates of lung cancer were lower than those in 2009, and also lower than those of 2003–2007.21 After age standardization, however, the incidence and mortality rates were relatively stable. This result shows that aging is a major cause for the difference of lung cancer incidence and mortality between the areas covered by cancer registries and nationwide in China. Tobacco smoking and air pollution22 were identified as risk factors for lung cancer. About 80% of the lung cancer burden in men and 50% of the burden in women were attributed to the two risk factors. Effective smoking control has been shown to reduce lung cancer incidence in the US since 1999.23 Despite a nationwide intervention on smoking control – no smoking in public places – China still has the largest smoking population. It is expected that through primary and secondary prevention, the prevalence of lung cancer may be controlled in the future.
Conclusion
Our study reports the most up-to-date data on incidence and mortality, reflecting the only available population-based information on lung cancer in China. As explained in previous articles,24 urban population coverage makes up a great part of the overall population, therefore, we classified our data in different levels with Eastern, Middle, and Western areas and adjusted the weight of the urban and rural population so this study may provide an accurate representation. The Chinese government is still making efforts to improve the quality of cancer registration data, especially in rural areas. It is expected that the accuracy and representation of population-based cancer statistics will improve in the future.
Acknowledgments
We wish to thank all of the staff from local cancer registries that have made a great contribution in providing their cancer registration databases.
Disclosure
No authors report any conflict of interest.
References
- Frauenfelder T, Puhan MA, Lazor R, et al. Early detection of lung cancer: a statement from an expert panel of the Swiss university hospitals on lung cancer screening. Respiration. 87:254–264. doi: 10.1159/000357049. [DOI] [PubMed] [Google Scholar]
- Naimi AI, Cole SR, Hudgens MG, Richardson DB. Estimating the effect of cumulative occupational asbestos exposure on time to lung cancer mortality: using structural nested failure-time models to account for healthy-worker survivor bias. Epidemiology. 2014;25:246–254. doi: 10.1097/EDE.0000000000000045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Aldrich MC, Grogan EL, Munro HM, Signorello LB, Blot WJ. Stage-adjusted lung cancer survival does not differ between low-income blacks and whites. J Thorac Oncol. 2013;8:1248–1254. doi: 10.1097/JTO.0b013e3182a406f6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ridge CA, McErlean AM, Ginsberg MS. Epidemiology of lung cancer. Semin Intervent Radiol. 2013;30:93–98. doi: 10.1055/s-0033-1342949. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Furlow B. Low-dose computed tomography lung cancer screening. Radiol Technol. 2014;85:297–314. [PubMed] [Google Scholar]
- El-Basmy A. Profile of lung cancer in Kuwait. Asian Pac J Cancer Prev. 2013;14:6181–6184. doi: 10.7314/apjcp.2013.14.10.6181. [DOI] [PubMed] [Google Scholar]
- Field JK, Hansell DM, Duffy SW, Baldwin DR. CT screening for lung cancer: countdown to implementation. Lancet Oncol. 2013;14:e591–600. doi: 10.1016/S1470-2045(13)70293-6. [DOI] [PubMed] [Google Scholar]
- Li Y, Dai M, Chen Y, et al. Estimates of lung cancer mortality at the province level in China. Chin J Lung Cancer. 2011;14:120–126. doi: 10.3779/j.issn.1009-3419.2011.02.03. (In Chinese.) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Han R, Zheng R, Zhang S, Ming WU. Wanqing C. Trend analyses on the differences of lung cancer incidence between gender, area and average age in China during 1989–2008. Chin J Lung Cancer. 2013;16:445–451. doi: 10.3779/j.issn.1009-3419.2013.09.02. (In Chinese.) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen Beijing Z. 2008. The 3th National Death Cause Survey Report. Chinese Academy of Medical Sciences & Peking Union Medical College Press.
- Chen W, Zhang S, Zou X. Evaluation on the incidence, mortality and tendency of lung cancer in China. Thoracic Cancer. 2010;1:35–40. doi: 10.1111/j.1759-7714.2010.00011.x. [DOI] [PubMed] [Google Scholar]
- Zhang SW, Cheng W, Wang L. The 30 years of cancer registration in China. China Cancer. 2009;18:256–259. [Google Scholar]
- National_Statistics_Bureau. 2012. Tabulation in the 2010 Population Census of the People's Republic of China. Cited 12 March 2014.] Available from URL: http://www.stats.gov.cn/tjsj/pcsj/rkpc/6rp/indexch.htm.
- Curado M, Edwards B, Shin H. Storm, H., Ferlay, J., Heanue, M., & Boyle, P . Cancer Incidence in Five Continents. IX. Lyon: International Agency for Research on Cancer; 2008. [Google Scholar]
- Parkin DM, Chen VW, Ferlay J, Galceran HH, Storm HH, Whelan SL. 1994. Comparability and Quality Control in Cancer Registration. Lyon: IARC Technical Report No. 19.
- Ferlay J, Burkhard C, Whelan S, Parkin DM. Check and conversion programs for cancer registries (IARC/IACR tools for cancer registries) 2005. Lyon: International Agency for Research on Cancer.
- Parkin DM, Bray F. Evaluation of data quality in the cancer registry: principles and methods Part II. Completeness. Eur J Cancer. 2009;45:756–764. doi: 10.1016/j.ejca.2008.11.033. [DOI] [PubMed] [Google Scholar]
- Bray F, Parkin DM. Evaluation of data quality in the cancer registry: principles and methods. Part I: comparability, validity and timeliness. Eur J Cancer. 2009;45:747–755. doi: 10.1016/j.ejca.2008.11.032. [DOI] [PubMed] [Google Scholar]
- Zhao P, Chen W, Kong L. Chinese Cancer Incidence and Mortality 2003–2007. Beijing: Military Medical Science Press; 2011. [Google Scholar]
- Chen W, Zheng R, Zhang S, Zou X, Zhao P, He J. Lung cancer incidence and mortality in China, 2009. Thoracic Cancer. 2013;4:102–108. doi: 10.1111/1759-7714.12025. [DOI] [PubMed] [Google Scholar]
- Chen W, Zheng R, Zhang S, et al. An Analysis of Lung Cancer Incidence and Mortality in China, 2003–2007. Practical Oncology Journal. 2012;26:6–10. [Google Scholar]
- Loomis D, Grosse Y, Lauby-Secretan B, et al. The carcinogenicity of outdoor air pollution. Lancet Oncol. 2013;14::1262–1263. doi: 10.1016/s1470-2045(13)70487-x. [DOI] [PubMed] [Google Scholar]
- Kort EJ, Paneth N, Woude GFV. The decline in US cancer mortality in people born since 1925. Cancer Res. 2009;69:6500–6505. doi: 10.1158/0008-5472.CAN-09-0357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chen WQ, Zhang SW. A representative study of cancer registry in China. China Cancer. 2008;17:832–834. [Google Scholar]