

Introduction
Foreign bodies in the pharynx or trachea are medical emergencies. Accidental aspiration or ingestion of a foreign body may arise from any procedure involving the oral cavity. Patients undergoing dental treatment are particularly susceptible to this complication due to large variety of small instruments involved such as teeth, burs, broken mirrors, rubber dam clamps, endodontic instruments and prosthesis. Appropriate preventive measures to avoid foreign body aspiration should be practiced as a matter of routine. However, even under the most ideal circumstances aspiration may still occur. Successful removal depends on several factors, including location of the foreign body, type of material, the physician's dexterity and the patient's cooperation.1, 2
The purpose of this article is to describe a clinical case of accidental aspiration of an endodontic file with emphasis on the preventive measures to avoid such an accident and management if such mishap occurs.
Case report
A 32-year-old male patient reported to dental center with complains of pain and swelling in the lower left first molar since one week. Root canal therapy was planned for its management. Rubber dam isolation was not possible because of considerable loss of tooth structure and associated intraoral swelling. Gauze screen placement to block access to the oropharynx was not possible because of excessive gag reflex. Access opening was done and Protaper® Sx endodontic file (Dentsply Limited, United Kingdom) was utilized for widening of root canal orifice. While removal of the file from root canal, sudden movement by the patient resulted in slippage of the endodontic file by the operator and accidental passage into the oropharynx. Vigorous attempts at removing the instrument with an aspirator were unsuccessful. The operator tried performing Heimlich maneuver to retrieve the instrument but it was also unsuccessful. However, patient was asymptomatic without coughing, wheezing or airway obstruction. An anteroposterior chest radiograph was taken immediately revealing presence of file in midline at the level of fifth intercostal space (Fig. 1). The patient was immediately transferred to the hospital for emergency expert management. A computed tomography scan of thorax was performed that revealed presence of file in the left main bronchus (Fig. 2). Rigid bronchoscopy was performed under general anesthesia and with the help of C-arm fluoroscopy, the file was successfully retrieved. The patient's post-operative period was without any complications.
Fig. 1.
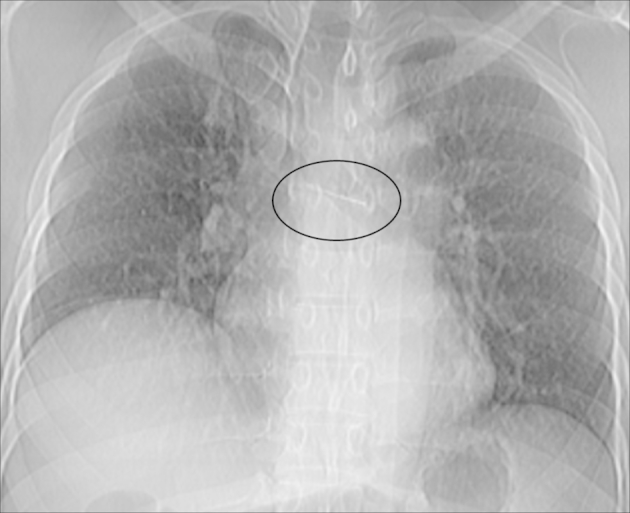
An anteroposterior chest radiograph showing the radioopaque instrument in midline at the level of fifth intercostal space.
Fig. 2.
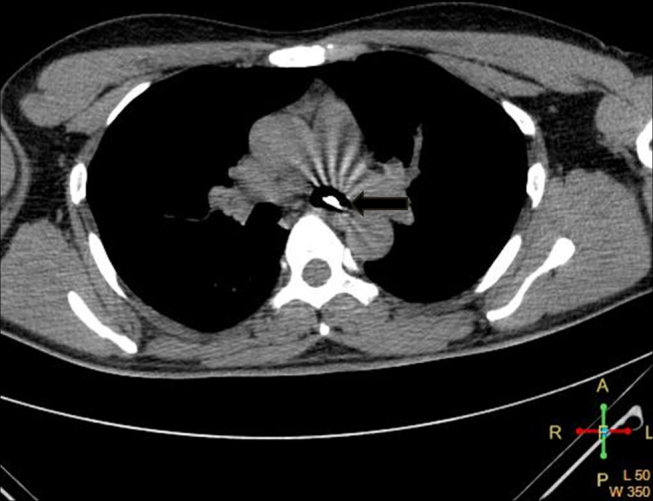
An axial computed tomography section of thorax revealing the presence of foreign body in the left main bronchus.
Discussion
Accidental aspiration or ingestion of foreign bodies is a complication encountered across all age groups. It normally affects pediatric patients or unconscious, mentally ill or disabled people whose coordination or control of deglutition is impaired. Swallowed foreign objects can get lodged in the pharynx, esophagus, stomach, intestine or simply pass through the gastrointestinal tract.3 Aspirated foreign objects can get lodged in the larynx, trachea or bronchus and is more serious situation with the possibility of suffocating.1, 2 Susini et al reported the incidence of aspiration for endodontic instruments was 0.001 per 100,000 root canal treatments and the incidence of ingestion was 0.12 per 100,000 root canal treatments.4
The majority of ingested foreign bodies pass through the gastrointestinal tract without any signs and symptoms. However, coughing, gagging, dysphagia, odynophagia, nausea and vomiting may occur. Complications such as impaction, perforation or obstruction may also develop with swallowing of a sharp object.5 Signs and symptoms of aspiration ranges from relatively benign partial obstruction to the immediately life-threatening total airway obstruction. It depends on size and shape of the object and the level where the object becomes impacted. If it is trapped above the vocal cords, an emergency situation in the form of acute respiratory distress can result. Smaller foreign bodies often pass through the vocal cords and lodge in the tracheobronchial tree without causing airway obstruction. The commonest symptoms of laryngotracheal foreign bodies are dyspnea, cough and stridor; those of bronchial foreign bodies are cough, decreased air entry, dyspnea and wheezing. In some cases small foreign bodies might have no initial effects and go unrecognized until later, when pulmonary complications such as infection, lung abscess formation, pneumonia, atelectasis or bronchiectasis develop.6, 7 The present case enlightens an important finding that any foreign body getting dislodged from the oral cavity without producing initial symptoms, need not necessarily be ingested.
The present case emphasizes basic principles to be followed while providing dental care are prevention of aspiration, early diagnosis and treatment. A physical barrier, such as a curtain of gauze or a rubber dam, should be placed in the mouth to prevent objects from entering the oropharynx. In patients with gag reflexes who will not tolerate this safety precaution, chair position becomes increasingly important and patients should be seated more upright, with the head turned to one side.7 In present case, rubber dam and gauze pack isolation was not possible because of considerable loss of tooth structure and hyperactive gag reflex respectively. Furthermore sudden brisk movement by the patient resulted in slippage of the endodontic file by the operator and accidental passage into the oropharynx. Therefore operator should be extra vigilant while performing root canal treatment in such patients.
Once the object gets accidentally swallowed or aspirated, clinician should make every possible effort to locate and retrieve it. Patient should be placed in dependent position and coughing encouraged, thereby expelling it. If upper airway obstruction occurs, immediate steps to establish the airway must be taken. The Heimlich maneuver, back blows in infants, chest or abdominal thrust in obese or pregnant patients should be performed to dislodge the object. Foreign objects lodged in the upper aspect of trachea or esophagus may be retrieved with simple instrumentation such as hemostats, DeBakey forceps, Magill forceps, high-vacuum suction and a laryngoscope. If all these steps are unsuccessful, rapid localization of the foreign body is indicated. In present case, early localization of aspirated endodontic file was made possible by plain chest radiography and computed tomography. Computed tomography provides better contrast and improved three-dimensional localization.8 A bronchoscopic examination with localization and removal of the object as soon as possible after aspiration is the treatment of choice. The use of fluoroscopy during the bronchoscopic examination is highly recommended. When aspirated foreign bodies are removed within 24 h, minimal mucosal changes are found. Bronchoscopy has been reported 99% effective with a complication rate between 2.4% and 5%.9 Objects refractory to bronchoscopy may necessitate thoracotomy, although biplane imaging and intravascular retrieval devices used in interventional cardiovascular procedures have been successfully utilized for removal of dental post from the lungs.10 Therefore, preventive measures can greatly reduce the frequency of aspiration and even if aspiration occurs, early localization of foreign body facilitates appropriate and timely management.
Conflicts of interest
All authors have none to declare.
References
- 1.Eren S., Balci A.E., Dikici B., Doblan M., Eren M.N. Foreign body aspiration in children: experience of 1160 cases. Ann Trop Paediatr. 2003;23:31–37. doi: 10.1179/000349803125002959. [DOI] [PubMed] [Google Scholar]
- 2.Cameron S.M., Whitlock W.L., Tabor M.S. Foreign body aspiration in dentistry: a review. J Am Dent Assoc. 1996;127:1224–1228. doi: 10.14219/jada.archive.1996.0415. [DOI] [PubMed] [Google Scholar]
- 3.Eisen G.M., Baron T.H., Dominitz J.A. Guideline for the management of ingested foreign bodies. Gastrointest Endosc. 2002;55:802–806. doi: 10.1016/s0016-5107(02)70407-0. [DOI] [PubMed] [Google Scholar]
- 4.Susini G., Pommel L., Camps J. Accidental ingestion and aspiration of root canal instruments and other dental foreign bodies in a French population. Int Endod J. 2007;40:585–589. doi: 10.1111/j.1365-2591.2007.01249.x. [DOI] [PubMed] [Google Scholar]
- 5.Zitzmann N.U., Elsasser S., Fried R., Marinello C.P. Foreign body ingestion and aspiration. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999;88:657–660. doi: 10.1016/s1079-2104(99)70004-1. [DOI] [PubMed] [Google Scholar]
- 6.Fields R.T., Jr., Schow S.R. Aspiration and ingestion of foreign bodies in oral and maxillofacial surgery: a review of the literature and report of five cases. J Oral Maxillofac Surg. 1998;56:1091–1098. doi: 10.1016/s0278-2391(98)90263-4. [DOI] [PubMed] [Google Scholar]
- 7.Israel H.A., Leban S.G. Aspiration of an endodontic instrument. J Endod. 1994;10:452–454. doi: 10.1016/S0099-2399(84)80268-X. [DOI] [PubMed] [Google Scholar]
- 8.Newton J.P., Abel R.W., Lloyd C.H., Yemn R. The use of computed tomography in the detection of radiolucent denture base material in the chest. J Oral Rehabil. 1987;14:193–202. doi: 10.1111/j.1365-2842.1987.tb00709.x. [DOI] [PubMed] [Google Scholar]
- 9.Black R.E., Johnson D.G., Matlak M.E. Bronchoscopic removal of aspirated foreign bodies in children. J Pediatr Surg. 1994;29:682–684. doi: 10.1016/0022-3468(94)90740-4. [DOI] [PubMed] [Google Scholar]
- 10.Gibbs J.S., Murdoch L.J., Goldstraw P., Buller N.P. Removal of a dental post from the bronchus by interventional cardiovascular techniques. Thorax. 1994;49:526–527. doi: 10.1136/thx.49.5.526. [DOI] [PMC free article] [PubMed] [Google Scholar]