

Abstract
The China Jintan Child Cohort study began in 2004 with 1656 pre-school participants and a research focus on studying the impact of environmental exposures, such as lead, on children’s neurobehavioural outcomes. This population cohort now includes around 1000 of the original participants, who have been assessed three times over a period of 10 years. Since the original IJE cohort profile publication in 2010, participants have experienced a critical developmental transition from pre-school to school age and then adolescence. The study has also witnessed an increase in breadth and depth of data collection from the original aim of risk assessment. This cohort has added new directions to investigate the mechanisms and protective factors for the relationship between early health factors and child physical and mental health outcomes, with an emphasis on neurobehavioural consequences. The study now encompasses 11 domains, composed of repeated measures of the original variables and new domains of biomarkers, sleep, psychophysiology, neurocognition, personality, peer relationship, mindfulness and family dynamics. Depth of evaluation has increased from parent/teacher report to self/peer report and intergenerational family report. Consequently, the cohort has additional directions to include: (i) classmates of the original cohort participants for peer relationship assessment; and (ii) parental and grandparental measures to assess personality and dynamics within families. We welcome interest in our study and ask investigators to contact the corresponding author for additional information on data acquisition.
Key Messages
Since its inception in 2004, the China Jintan Child Cohort Study has grown to include three waves of data collection and has followed its participants through the critical transition from childhood into adolescence; during this time, the study has investigated several early health risk factors of childhood development, with a particular focus on the relationship between environmental toxicant exposure, such as lead, and child neurocognitive and behavioural outcomes.
The database has broadened in the breadth and depth of measures and now includes new domains such as psychophysiology, positive psychology, peer relationship, and intergenerational family dynamics; consequently, the study has evolved beyond risk assessment to an investigation of the social and brain mechanisms of early health risk factors.
New waves of data collection allow for convergent analyses with the use of multiple informants and several different instruments to measure the same outcome.
What is the rationale for the new data collection?
The China Jintan (As of June 1, 2015, Jintan City became the Jintan District of Changzhou City, Jiangsu Province, China) Child Cohort Study is a longitudinal pre-school cohort1,2 that was designed to study the impact of environmental exposure, such as lead, on children’s neurobehavioural outcomes. Since the publication of our 2010 cohort profile, this cohort has expanded from a focus on risk assessment to understanding the mechanisms and protective factors for this lead-behaviour relationship, and from an original emphasis on environmental exposure to the inclusion of broad early health factors. These changes are guided by the ‘Early Health Model’ conceptual framework3 and have been driven by the following three factors.
First, the new wave expanded from risk assessment to understanding the mechanism, protective factors and general early health factors, in child mental and physical health development. Specifically, there is increasing evidence that lead exposure may result in decreased IQ4 and increased disruptive behaviour,5 but the mechanism underlying this relationship in children is unclear. This new wave of data collection sought to elucidate the mediating mechanisms by measuring psychophysiology and other biomarkers. Furthermore, Wave 1 findings suggested that children with frequent breakfast consumption have lower blood lead concentrations (BLC) compared with their breakfast-skipping counterparts.6 This suggested the need for a more comprehensive assessment of nutrition (e.g. food frequency questionnaire) as a potential protective factor in Wave 2 data collection. Furthermore, in order to understand factors that contribute to overall adolescent health, we included physiological assessments such as metabolic indicators (e.g. glucose, cholesterol, body mass index) and sleep patterns.
Second, as cohort participants transition from childhood into adolescence, they begin to experience more complex and salient peer relationships6 which may contribute to their behaviour. Consequently, the cohort has evolved to include current classmates of the original cohort participants in order to assess these peer relationships. We also include measures of personality traits, such as positive psychology capital, in order to better understand behavioural development during this transition into adolescence.
Third, research has documented intergenerational transmission of personality traits and behaviours.7,8 As a result, this new wave of data collection sought to include a cross-generational assessment of family dynamics and behavioural outcomes in the child, parent and grandparent generations.9,10
Given these rationales, the new waves of data collection provides a more comprehensive view of the complex process of child mental and physical health development, from risk assessment to understanding mechanisms to elucidating protective factors, as well as investigating the influence of peer and intergenerational factors.
What will be the new areas of research?
The new areas of research can be summarised into the following categories, with the rationale detailed below:
inclusion of new domains of health factors;
mechanistic investigation between health factors and neurobehavioural development;
peer relationships between cohort participants and current classmates;
cross-generational assessment of personality traits and behaviours.
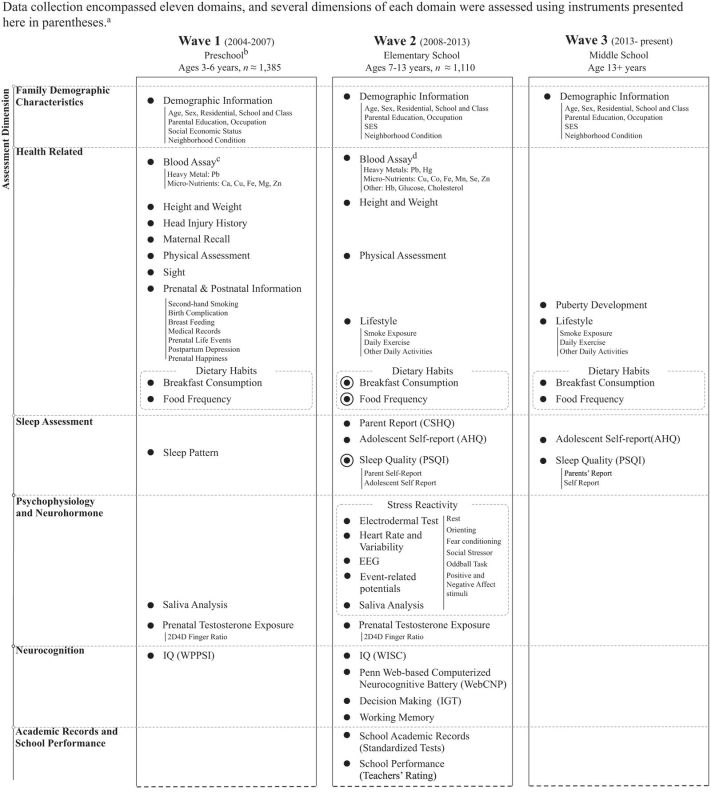
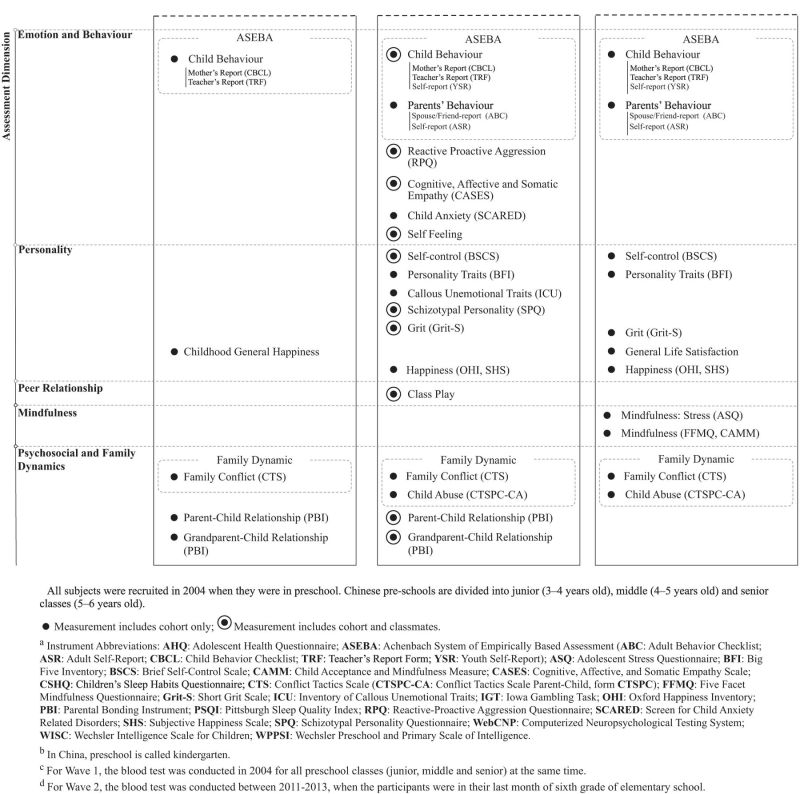
Specifically, the new areas of research include biomarkers, sleep, psychophysiology, neurocognition, personality, peer relationships, mindfulness and family dynamics. As mentioned in our previously published cohort profile,1 child development is complex and is the result of the interaction of physical, social and psychological environments. Collectively, these domains allow us to assess risk and protective factors and the mechanisms underlying neurobehavioural outcomes. Details regarding instrumentation are presented in Table 1.
Table 1.
Domains and measures assessed in Waves 1–3 of the China Jintan Child Cohort Study
 |
 |
Biomarkers
In addition to blood lead, other heavy metals and nutrients have been linked to neurobehavioural outcomes.11 Therefore, the new wave assessed an additional heavy metal (mercury) and micronutrients (selenium, cobalt, manganese). The new wave also measures fasting glucose and cholesterol levels to screen for metabolic disorders such as pre-diabetes and pre-hyperlipidaemia.
Sleep
Poor sleep and sleep disorders are highly prevalent in children, and like lead exposure, these conditions are associated with significant neurobehavioural impairment and other health outcomes such as increased fasting glucose (unpublished data). The cohort now employs several sleep questionnaires12–17 to assess both child and parent sleep quality in order to study the developmental effects of sleep and intergenerational effects of sleep patterns.
Psychophysiology
This cohort has previously reported on the relationship between lead exposure and children’s behavioural problems, but the mechanism underlying this association is unclear. Assessing psychophysiology helps to elucidate mechanisms of action between early health factors and neurobehavioural development. It was hypothesised, for example, that lead exposure can affect autonomic arousal that may predispose children to cognitive and emotional dysfunction, which in turn impacts behaviour.
Neurocognition
Previous measures of IQ have strong psychometric properties and are easy to use, but these measures were geared to assess general intelligence.18–21 Neuropsychological tests are instead designed to target specific cognitive domains and are more sensitive in detecting the effects of neurological changes related to risk factors such as environmental exposure to lead. These tests include: (i) a computerised neuropsychological testing system, known as WebCNP™,22 to assess neurocognitive functions such as abstraction, attention and motor speed; (ii) a working memory instrument;23 and (iii) a risk-taking behaviour instrument.24,25
Personality
Recent research suggests that positive psychological capital is a protective factor in child development. In new waves of data collection, we collected self-reported measures of different aspects of personality26–29 and positive psychological constructs, including happiness,30,31 grit32 and self-control.29 We supplemented these measures with data collected from multiple informants, including their classmates, parents and teachers.
Peer relationships
As children grow into adolescence, social interaction becomes a more prominent feature of their daily lives and influences emotional and behavioural outcomes.6 As a result, the cohort included peer relationship measurements through a class play instrument,33 which is reported by the participants’ classmates.
Mindfulness
Mindfulness is the state of non-judgemental attention to the present. It is a concept that has been implicated in child and adolescent behavioural development and as an aid to coping with stress.34 As the participants of the cohort age and gain an awareness of themselves and their surroundings, this cohort piloted a study in 2014 in a small subsample to gauge their level of mindfulness and its associations with neurobehavioural outcomes.35
Family dynamics
Positive family dynamics, such as parental bonding, have been shown to serve as protective factors for children’s neurobehavioural outcomes.36,37 Conversely, negative family dynamics are considered risk factors for child development.38,39 As a result, we measured parental bonding9,10,40 and family conflicts41,42 in the new wave of data collection. In order to gauge intergenerational effects of family dynamics,7 we also included the grandparental generation in our surveys.
Who is in the cohort?
The Jintan Cohort is a pre-school cohort that initially recruited 1656 children in 2004. Briefly, the first phase of Wave 1 of data collection occurred in 2004–07, when the children were 3–6 years old and in pre-school; the second phase of Wave 1 of data collection occurred in 2008–10, when the children were 7–9 years old and in elementary school. During Wave 2 of data collection in 2011–13, the children were 11–13 years old and in their last few months of 6th grade, just prior to matriculation into middle school. Wave 3 data collection is ongoing. Descriptive statistics on several key biomarker measures are presented in Table 2 and descriptive statistics on behavioural and cognitive scores are presented in Table 3. As the children matriculated from pre-school, data collection for certain instruments expanded to include their new classmates in order to better understand the social implications of neurobehavioural development (e.g. peer relationships). Attrition data can be found in Figure 1. Complete data were available on 1385 (55% males) children in Wave 1, and 1110 (54% males) in Wave 2. The original and current cohort participants were compared on sex, residence, age, IQ and behaviour scores to assess bias due to attrition. Results of these analyses are shown in Table 4.
Table 2.
Descriptive statistics of key Wave 2 demographic and biomarker data from the China Jintan Cohort Study
| Sex |
Total | |||
|---|---|---|---|---|
| Male | Female | |||
| Demographic Information | ||||
| Agea | Nb | 585 | 506 | 1091 |
| M (SD)b | 11.89 (0.44) | 11.83 (0.41) | 11.86 (0.42) | |
| Blood Assay | ||||
| Heavy Metal (µg/dL) | ||||
| Lead | N | 595 | 513 | 1108 |
| M (SD) | 3.21 (1.16) | 3.01 (1.16) | 3.12 (1.17) | |
| G (SD) | 3.02 (1.17) | 2.83 (1.16) | 2.93 (1.04) | |
| Manganese | N | 154 | 151 | 305 |
| M (SD) | 0.22 (0.11) | 0.26 (0.18) | 0.24 (0.25) | |
| Micronutrient (µg/dL) | ||||
| Copper | N | 594 | 514 | 1108 |
| M (SD) | 97.60 (23.11) | 95.36 (20.42) | 95.63 (22.00) | |
| Iron | N | 592 | 514 | 1106 |
| M (SD) | 113.20 (39.73) | 113.55 (41.87) | 113.36 (40.72) | |
| Zinc | N | 594 | 514 | 1108 |
| M (SD) | 91.83 (22.32) | 91.34 (22.34) | 91.60 (22.32) | |
| Cobalt | N | 584 | 508 | 1092 |
| M (SD) | 0.44 (0.52) | 0.52 (0.70) | 0.48 (0.61) | |
| Selenium | N | 595 | 513 | 1108 |
| M (SD) | 145.56 (53.42) | 145.48 (50.26) | 145.52 (51.96) | |
| Other Blood Tests | ||||
| Haemoglobin (g/dL) | N | 553 | 488 | 1041 |
| M (SD) | 13.28 (0.84) | 13.10 (0.79) | 13.20 (0.81) | |
| Glucose (mmol/L) | N | 568 | 497 | 1065 |
| M (SD) | 5.18 (0.54) | 5.08 (0.54) | 5.13 (0.54) | |
| Cholesterol (mmol/L) | N | 568 | 497 | 1065 |
| M (SD) | 3.98 (0.72) | 3.96 (0.63) | 3.98 (0.68) | |
| Red Blood Cell (106/µL) | N | 553 | 488 | 1041 |
| M (SD) | 4.82 (0.34) | 4.69 (0.33) | 4.76 (0.34) | |
a Age of senior class is as of April 15th, 2011; age of middle class is as of April 15th, 2012; age of junior class is as of April 15th, 2013; total statistics is calculated with age attained with above the method(s). All above assessments were conducted when the children were at last semester of 6th grade.
b M (SD) stands for mean (standard deviation); G (SD) stands for geometric mean (standard deviation); N stands for sample size.
Table 3.
Participant cognition and behaviour scores in Wave 2 at around age 12 years
| Sex |
Total | |||
|---|---|---|---|---|
| Male | Female | |||
| Cognitive Ability (IQ) | ||||
| N | 436 | 360 | 798 | |
| Verbal IQ | M (SD) | 102.07 (12.17) | 99.84 (11.59) | 101.05 (11.94) |
| Performance IQ | M (SD) | 106.96 (12.25) | 103.51 (11.35) | 105.41 (11.95) |
| Full-scale IQ | M (SD) | 105.31 (11.94) | 102.07 (11.61) | 103.84 (11.88) |
| Behaviour (Youth Self-Report) | ||||
| N | 308 | 277 | 585 | |
| Internalizing | M (SD) | 9.83 (6.96) | 10.13 (7.00) | 9.98 (6.97) |
| Externalizing | M (SD) | 8.44 (6.67) | 6.63 (5.38) | 7.58 (6.16) |
Figure 1.

Participant attrition diagram for the China Jintan Child Cohort study.
Table 4.
Comparison of key variables in the original cohort participants between those with and without follow up in Wave 2
| Variable | Follow-up | Exited cohort | Test statistics |
|
|---|---|---|---|---|
| % | % | Chi-squared | P-value | |
| Sex | ||||
| Male | 53.2 | 59.6 | 4.216 | 0.040* |
| Female | 46.8 | 40.4 | ||
| Location | ||||
| Rural | 20.7 | 19.6 | 0.404 | 0.817 |
| Suburban | 40.2 | 39.5 | ||
| City | 39.1 | 40.9 | ||
| Mean (SD) | Mean (SD) | t test | P-value | |
|---|---|---|---|---|
| Age | 13.72 (0.89) | 13.67 (0.91) | −1.06 | 0.291 |
| IQ | ||||
| VIQ | 104.26 (14.78) | 102.95 (15.01) | 1.372 | 0.170 |
| PIQ | 104.25 (14.64) | 103.42 (16.41) | 0.846 | 0.397 |
| FIQ | 104.46 (14.03) | 103.29 (15.26) | 1.266 | 0.206 |
| Behaviour | ||||
| Parent report (CBCL) | 33.83 (20.96) | 32.88 (20.91) | 0.736 | 0.462 |
| Teacher report (TRF) | 19.77 (17.14) | 19.74 (16.73) | 0.027 | 0.978 |
* Significant at P < 0.05.
What has been measured?
All measures used in this cohort are listed in Table 1. These measures highlight several key features of this expanding cohort study. First, the scope of the study encompasses several new domains, including psychophysiology, neurocognition, personality, peer relationships, mindfulness and family dynamics, in addition to expanding previous domains of family demographic characteristics, health-related measures, sleep patterns and emotion and behaviour. Second, several instruments and multiple informants were used in each domain to provide a multi-informant perspective; questionnaire-based assessments were completed by the cohort children, their classmates, parents, grandparents and teachers (see Table 1). Third, we conducted follow-ups on several longitudinal measures18,19,43–46 as the cohort participants transitioned from pre-school to school age to adolescence. These follow-ups capture the neurobehavioural changes occurring during this important period of physical, social and psychological growth. Fourth, we included intergenerational data in order to compare cross-generational effects of behaviour and lifestyle practices.
What has been found?
To date, 31 published journal articles have been derived from the Jintan Cohort on topics including baseline methodology,1,2,10,46,47 sociodemographic variables,48–52 environmental lead exposure,4,5,48,53,54 child cognitive4,20,21,55–59 and behavioural development5,37,49,60–62 assessment, and cross-cultural comparisons.63–67 A selection of these manuscripts, which have been integral in directing the new research focus, is presented in Table 5. These publications represent the multidisciplinary nature of data collection and a selection of key findings is listed below.
Table 5.
Key published findings from the China Jintan Child Cohort Study
| Key variables |
Findings | Link to new research Direction |
|---|---|---|
| Lead-related | ||
| Behaviour | Blood lead levels are positively associated with behavioural and emotional problems among Chinese children.5 | While lead exposure has been associated with decreased IQ and increased behavioural problems, the mechanisms of these relationships are unclear. These findings led to the need for 1) comprehensive neurobehavioural measurements (e.g. psychophysiology) as one of the new measurements in the new wave of data collection; 2) an investigation of nutrition as a protective factor due to the negative association between lead and various aspects of child nutrition (e.g. breakfast consumption, iron status, breastfeeding in infancy); and 3) further studies on the role of lead in sleep disturbance. |
| Breakfast consumption | Preschool children with frequent breakfast consumption have lower blood lead levels than their counterparts who skip breakfast.53 | |
| Haemoglobin | Blood lead levels are negatively associated with haemoglobin concentrations in preschool children in China.54 | |
| IQ | Blood lead levels are negatively associated with IQ and school performance in Chinese children.4 | |
| Sleep | Early elevated blood lead levels are positively associated with sleep disturbance in preadolescence.69 | |
| Sociodemographic factors | Sociodemographic factors (e.g. being male, increased age, presence of siblings), community conditions (e.g. living in crowded neighbourhoods), and parental factors (e.g. lower maternal education, paternal occupation, parental smoking) are positively associated with blood lead levels.48 | |
| Behaviour | ||
| Breastfeeding | Breastfeeding and active bonding are negatively associated with children’s internalizing behaviour problems.37 | These findings suggest there is a biological process underlying behavioural development. However, the social environment also plays a role and can interact with these biological processes. This cohort now seeks to understand the social determinants of behaviour by analysing peer relationships and family dynamics. |
| Head injury | Parent-reported mild head injury history positively associated and behavioural problems in children at 6 years.60 | |
| Micronutrient | Low blood zinc and iron are positively associated with increased behaviour problems in pre-schoolers.49 | |
| Testosterone exposure | 2D:4D ratio, a marker for prenatal testosterone exposure, is positively associated with externalizing behaviour problems in children.62 | |
| Tobacco exposure | Mother's environmental tobacco smoke exposure during pregnancy is positively associated with externalizing behaviour problems in children.61 | |
| Nutrition | ||
| Breakfast and IQ | Regular breakfast consumption is positively associated with IQ performance in kindergarten children.55 | These findings suggest lifestyle choices, which are influenced by sociodemographic characteristics, can in turn influence various aspects of neurobehavioural development. These relationships suggest that nutrition should be explored further as a protective factor in child development. |
| Breastfeeding and sociodemographic | Social factors (e.g. city residents) and demographic determinants (e.g. parental education and professional occupational status) are associated with breastfeeding practices in South East China.50 | |
| Haemoglobin and IQ | Haemoglobin status as a proxy for iron status is positively associated with performance IQ but not verbal IQ in Chinese pre-school children.57 | |
| Obesity and sociodemographic | Prevalence of overweight and obesity in China has risen; maternal employment is negatively associated with overweight and obese status.52 | |
| Sleep | ||
| IQ and sleep problems | Sleep problems and fatigue are negatively associated with cognitive performance in Chinese kindergarten children.58 | Findings provide new insights in understanding the role of sleep in the association between early health risk factors and neurobehavioural outcomes, along with the effect of nutritional factors on sleep quality. Further studies are being conducted to analyse cross-generational sleep patterns. |
| Micronutrient and sleep quality | Blood zinc concentrations at preschool age are predictive of later sleep quality in adolescence.68 | |
| Positive psychology | ||
| Parental bonding instrument | Psychometric properties of the Chinese version of the Parental Bonding Instrument.10 | A strong familial relationship may have consequences on a child’s positive psychology capital and as a result, the PBI instrument is used in current studies to analyse family dynamics. |
| Sociodemographic and intergenerational bonding | Child bonding relationships with parent and grandparent generations are positive correlated and associated with several sociodemographic factors.40 | |
Lead exposure
The study has shown that in Wave 1, the mean of BLC was higher in boys than in girls and increased with age at the time of the blood lead test.48 Compared with children with BLC <8 µg/dl, those with BLC ≥8 µg/dl scored 2–3 points lower in IQ and 5–6 points lower in school tests.4 BLC, even at a mean of 6.4 µg/dl, was associated with increased risk of externalizing, internalizing and pervasive developmental problems.5 The mechanisms behind these associations are unclear and as a result, further neurobiological testing is needed.
Nutrition
We have observed significant effects of nutritional status on health outcomes. Micronutrient (e.g. zinc and iron) deficiency was associated with increased behavioural problems.49 Sufficient blood micronutrient concentrations, such as that of zinc, has been observed to be associated with good sleep quality at different developmental stages in childhood.68 Reduced breastfeeding consumption was also negatively associated with internalizing behaviour problems.37 Nutrition in the form of frequent and regular breakfast consumption has been shown to be associated with lower BLC53 and increased IQ performance55 in pre-schoolers, suggesting that nutrition may serve as a protective factor in neurobehavioural development.
Behaviour
Prenatal risk factors for child behaviour problems have also been observed. Children of mothers exposed to second-hand smoking during pregnancy had higher scores for externalizing and total behaviour problems.61 A positive association between a marker for prenatal testosterone exposure [i.e. the ratio of the length of the second finger digit relative to the fourth digit (2D4D)] and externalizing behaviour problems in children was also observed.62
Descriptive statistics for the new data collected
Selected preliminary analyses from the new wave of data collection on sleep and positive psychological capital are presented in Tables 6 and 7, respectively. As indicated in Table 6, sleep problems in children are prevalent and some sleep problems in the child are correlated with parental sleep problems (e.g. sleep latency, daytime dysfunction and subjective sleep quality). It was hypothesised that sleep problems may be influenced by early health risk factors. For example, we recently found that elevated BLC at ages 3–5 years was associated with increased risk for sleep disorders in early adolescence, including sleep disruption and/or insomnia.69 This association may contribute to the overall negative effect of BLC on child behaviour. In addition, family dynamics also influenced child behaviour. Specifically, we found that early parental bonding reduced children’s behavioural problems and that parental bonding was positively associated with bonding with grandparents among Chinese children (Table 7).40
Table 6.
Descriptive statistics and correlations of adolescent and parent responses from the Pittsburgh Sleep Quality Index questionnaire
| Sleep Domainsa | Adolescent |
Parent |
Adolescent-Parent Correlationd | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| N | Mean ± SD | Scoresb |
N | Mean ± SD | Scoresb |
||||||||
| 0 | 1 | 2 | 3 | 0 | 1 | 2 | 3 | ||||||
| Sleep durationc | 971 | 1.027 ± 0.872 | 26.3% | 40.8% | 26.5% | 6.1% | 823 | 0.276 ± 0.618 | 78.5% | 18.5% | 0.0% | 3.0% | 0.10 |
| Sleep disturbances | 996 | 0.901 ± 0.500 | 17.7% | 74.9% | 7.1% | 0.3% | 842 | 0.956 ± 0.433 | 11.3% | 82.2% | 6.4% | 0.4% | 0.00 |
| Sleep latency | 1020 | 0.915 ± 0.846 | 35.0% | 43.9% | 15.7% | 5.4% | 837 | 0.968 ± 0.790 | 29.7% | 46.8% | 20.3% | 3.1% | 0.22* |
| Day dysfunction due to sleepiness | 998 | 0.908 ± 0.826 | 35.1% | 43.1% | 17.8% | 4.0% | 845 | 0.928 ± 0.747 | 29.7% | 49.8% | 18.5% | 2.0% | 0.14* |
| Sleep efficiency | 919 | 0.188 ± 0.535 | 86.5% | 9.5% | 2.7% | 1.3% | 827 | 0.203 ± 0.528 | 84.4% | 12.0% | 2.5% | 1.1% | −0.02 |
| Subjective sleep quality | 997 | 0.958 ± 0.765 | 27.5% | 54.3% | 15.4% | 3.9% | 862 | 0.836 ± 0.683 | 31.0% | 56.3% | 10.9% | 1.9% | 0.31* |
| Sleep medication use | 1022 | 0.074 ± 0.360 | 94.9% | 3.4% | 1.0% | 0.7% | 871 | 0.054 ± 0.308 | 96.2% | 2.8% | 0.5% | 0.6% | −0.09 |
a Sleep domains are measured by the Pittsburgh Sleep Quality Index (PSQI)13 instrument, which consists of 19 items that are grouped into 7 subdomains.
b Scores of sleep domains (except sleep duration): 0 = best, 3 = worst; a higher score indicates worse sleep quality.
Table 7.
Descriptive statistics of positive psychology questionnaires, reported by intergenerational informants
| Measurements & Domains | Mean (Standard Deviation) |
Correlation |
|||||||
|---|---|---|---|---|---|---|---|---|---|
| Children1 | Father2 | Mother3 | Grandparents4 | r1–2 | r1–3 | r2–3 | r2–4 | r3–4 | |
| Parent-Child Relationshipa | |||||||||
| Care | - | 13.83 (3.92) | 14.31 (3.64) | 14.87 (3.41) | - | - | 0.491** | 0.464** | 0.400** |
| Indifference | - | 4.74 (4.16) | 4.16 (3.77) | 4.44 (4.10) | - | - | 0.613** | 0.649** | 0.561** |
| Overprotection | - | 4.23 (3.98) | 4.60 (3.54) | 5.55 (4.23) | - | - | 0.650** | 0.643** | 0.532** |
| Autonomy | - | 12.59 (4.40) | 11.83 (4.32) | 13.29 (4.15) | - | - | 0.571** | 0.474** | 0.406** |
| Gritb | 3.14 (0.56) | 3.38 (0.37) | 3.34 (0.44) | - | 0.123** | 0.066 | 0.229** | - | - |
| Self Control | 47.11 (6.38) | 34.11 (5.35) | 47.75 (7.39) | - | 0.128** | 0.007 | −0.152** | - | - |
** P < 0.01
1–4 Superscripts are used to designate the correlation relationships. For example, r1–2 is the correlation between Children (1) and Father (2) questionnaire scores.
a Parent-child relationship is measured using the Parental Bonding Instrument (PBI),9 which consists of 24 items and 4 sub-domains with each item rated from 0–3. A higher total score of each sub-domain indicates stronger bonding style. The sample size of father, mother and grandparents were 968, 974 and 910, respectively.
b The Grit Questionnaire32 contains 12 items with each item rated from 1–5. A higher average score indicates higher grit. The sample size of children, father and mother were 655, 592 and 655, respectively.
c Range for short-term Self Control Questionnaire29 contains 13 items with each item rated from 1–5. A higher score indicates better self-control ability. The sample size of children, father and mother were 610, 592 and 531, respectively.
What are the main strengths and weaknesses?
There are several strengths of the multiple-wave data collection model of this cohort. First, the cohort has now expanded to include the new direction of understanding the neurobiological mechanisms between environmental toxicants and children’s neurobehavioural outcomes and the protective factors that may attenuate negative risk exposures. Second, the use of the same instruments allows for continuity in our longitudinal study and ease of comparison across years so that variability can be attributed to changes in the individual rather than changes in the instrument. Third, the study encompasses multiple dimensions to give greater depth to each outcome variable. The present cohort now includes specific physiological measures such as psychophysiology and neurohormonal data in order to gain a more focused understanding of the effects of environmental and social exposures. Fourth, the new waves of data collection have expanded from the original cohort to include the participants’ classmates and grandparents in addition to the participants themselves and their parents. This expansion allows for a better understanding of the complexity of children’s neurobehavioural outcomes, as measured through peer relationships and family dynamics.
There are several limitations to this cohort design. First, the retrospective nature of the data collection relied on maternal recall for the earlier years of development, which may lead to recall bias. However, a similar recall vs medical record validation with the same instrument in a different study suggests that maternal recall measures are reliable for certain prenatal events.70 Nevertheless, we will validate maternal recall with collected medical records. Another limitation is the lack of direct income data to measure socioeconomic status. Instead, we estimated socioeconomic status by utilising parental education, occupation, size of house and household, and living conditions to account for the variation in the make-up of the nuclear family. Third, like any cohort study, there are attrition limitations since not everyone in the original sample can be followed up.
Can I get hold of the data? Where can I find out more?
The China Jintan Cohort welcomes interest and offers of collaboration. Applicants for data access should contact Dr Jianghong Liu [jhliu@nursing.upenn.edu], the principal investigator.
Funding
This work was supported by National Institute of Environmental Health Sciences grants R01-ES018858, K01-ES015877, K02-ES019878 and P30-ES013508; the University of Pennsylvania Center of Excellence in Environmental Toxicology; the Wacker Foundation; the JintanCity Government; and Jintan Hospital.
Acknowledgements
Thanks are extended to the participating children and their families from Jintan City, and to the China Jintan Cohort Study Group. We are very grateful to the Jintan City Government and the Jintan Hospital for their support and assistance. Xiaoming Shen, PhD, provided an early contribution during blood lead analysis; and Herbert Needleman, PhD, provided instrumental support for the Jintan lead study. There was no financial compensation for these services.
Members of the Jintan Cohort Study Group: Guiju Sun, Hua Yang, Tunong Chen, Wenting You, Lingyi Wang, Richard Liu, Anna Rudo-Hutt, Naixue Cui, Xiaopeng Ji, Hui Liu, Yuli Li, Bowen Yao, Lezhou Wu and Xianchen Liu.
Conflict of interest: Ethical approval was obtained from the Institutional Review Board at the University of Pennsylvania and Jintan Hospital. Patrick W Leung is the Hong Kong distributor of the ASEBA rating scales (e.g. CBCL, TRF, YSR, etc.) used in this study. None of the other authors declare any conflict of interest regarding the data and materials presented in this paper.
Contributor Information
Collaborators: Guiju Sun, Leslie Rescorla, Catherine Tuvblad, Hua Yang, Tunong Chen, Richard Liu, Anna Rudo-Hutt, Naixue Cui, Xiaopeng Ji, Hui Liu, Yuli Li, Bowen Yao, Lezhou Wu, and Xianchen Liu
References
- 1.Liu J, McCauley LA, Zhao Y, Zhang H, Pinto-Martin J; Jintan Cohort Study Group. Cohort Profile: The China Jintan Child Cohort Study. Int J Epidemiol 2010;39:668–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Liu J, McCauley L, Leung P, et al. Community-based participatory research (CBPR) approach to study children's health in China: experiences and reflections. Int J Nurs Stud 2011;48:904–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Liu J. Early health risk factors for violence: conceptualization, review of the evidence, and implications. Aggress Violent Behav 2011;16:63–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Liu J, Li L, Wang Y, Yan C, Liu X. Impact of low blood lead concentrations on IQ and school performance in Chinese children. PLoS One 2013;8:e65230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Liu J, Liu X, Wang W, et al. Blood lead concentrations and children's behavioral and emotional problems: a cohort study. JAMA Pediatr 2014. 168:737–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Brown BB, Larson J. Peer Relationships in Adolescence. Handbook of Adolescent Psychology. New York, NY: John Wiley, 2009. [Google Scholar]
- 7.Swartz TT. Intergenerational Family Relations in Adulthood: Patterns, Variations, and Implications in the Contemporary United States. Annu Rev Sociol 2009;35:191–212. [Google Scholar]
- 8.van Meurs I, Reef J, Verhulst FC, van der Ende J. Intergenerational transmission of child problem behaviors: a longitudinal, population-based study. J Am Acad Child Adolesc Psychiatry 2009;48:138–45. [DOI] [PubMed] [Google Scholar]
- 9.Parker G, Tupling H, Brown LB. A Parental Bonding Instrument. Br J Med Psychol 1979;52:1–10. [Google Scholar]
- 10.Liu J, Li L, Fang F. Psychometric properties of the Chinese version of the Parental Bonding Instrument. Int J Nurs Stud 2011;48:582–89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Yu XD, Yan CH, Shen XM, et al. Prenatal exposure to multiple toxic heavy metals and neonatal neurobehavioral development in Shanghai, China. Neurotoxicol Teratol 2011;33:437–43. [DOI] [PubMed] [Google Scholar]
- 12.Owens JA, Spirito A, McGuinn M. The Children's Sleep Habits Questionnaire (CSHQ): psychometric properties of a survey instrument for school-aged children. Sleep 2000;23:1043–51. [PubMed] [Google Scholar]
- 13.Buysse DJ, Reynolds CF, 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument forpsychiatric practice and research. Psychiatry Res 1989;28:193–213. [DOI] [PubMed] [Google Scholar]
- 14.Liu X, Liu L, Wang R. Bed sharing, sleep habits, and sleep problems among Chinese school-aged children. Sleep 2003;26:839–44. [DOI] [PubMed] [Google Scholar]
- 15.Liu X, Liu L, Owens JA, Kaplan DL. Sleep patterns and sleep problems among schoolchildren in the United States and China. Pediatrics 2005;115(Suppl 1):241–49. [DOI] [PubMed] [Google Scholar]
- 16.Liu X, Zhao Z, Jia C, Buysse DJ. Sleep patterns and problems among Chinese adolescents. Pediatrics 2008;121:1165–73. [DOI] [PubMed] [Google Scholar]
- 17.National Sleep Foundation Sleep in America Poll. http://sleepfoundation.org/sites/default/files/2006_summary_of_findings.pdf (5 April 2015, date last accessed). 2006. [Google Scholar]
- 18.Wechsler D. Manual for the Wechsler Intelligence Scale for Children – Revised. New York, NY: Psychological Coporation, 1974. [Google Scholar]
- 19.Yue MZ, Gao ES. School-age children Intelligence Scale, Wechsler the National Urban norm formulation. Pract Pediatr 1987;2:327–28. [Google Scholar]
- 20.Liu J, Yang H, Li L, Chen T, Lynn R. An increase of intelligence measured by the WPPSI in China, 1984–2006. Intelligence 2012;40:139–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Liu J, Lynn R. Chinese sex differences in intelligence: Some new evidence. Pers Individ Dif 2015;75:90–93. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gur RC, Richard J, Hughett P, et al. A cognitive neuroscience-based computerized battery for efficient measurement of individual differences: standardization and initial construct validation. J Neurosci Methods 2010;187:254–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Liu C. Working memory and processing speed in children with arithmetical difficulties. Journal of Nanjing Normal University 2013;41:479–81. [Google Scholar]
- 24.Bechara A, Damasio AR, Damasio H, Anderson SW. Insensitivity to future consequences following damage to human prefrontal cortex. Cognition 1994;50:7–15. [DOI] [PubMed] [Google Scholar]
- 25.Kester HM, Sevy S, Yechiam E, Burdick KE, Cervellione KL, Kumra S. Decision-making impairments in adolescents with early-onset schizophrenia. Schizophr Res 2006;85(1):113–23. [DOI] [PubMed] [Google Scholar]
- 26.John OP, Srivastava S. The Big-Five trait taxonomy: History, measurement and theoretical perspectives. In: Pervin LA, John OP. (eds). Handbook of Personality: Theory and Research. New York, NY: Guilford Press, 1999. [Google Scholar]
- 27.Goldberg LR. The structure of phenotypic personality traits. Am Psychol 1993;48:26–34. [DOI] [PubMed] [Google Scholar]
- 28.Raine A. The SPQ: a scale for the assessment of schizotypal personality based on DSM-III-R criteria. Schizophr Bull 1991;17:555–64. [DOI] [PubMed] [Google Scholar]
- 29.Tangney JP, Baumeister RF, Boone AL. High self-control predicts good adjustment, less pathology, better grades, and interpersonal success. J Pers 2004;72:271–324. [DOI] [PubMed] [Google Scholar]
- 30.Hills P, Argyle M. The Oxford Happiness Questionnaire: a compact scale for the measurement of psychological well-being. Pers Individ Dif 2002;33:1073–82. [Google Scholar]
- 31.Lyubomirsky S, Lepper HS. A measure of subjective happiness: preliminary reliability and construct validation. Soc Indic Res 1999;46:137–55. [Google Scholar]
- 32.Duckworth AL, Peterson C, Matthews MD, Kelly DR. Grit: perseverance and passion for long-term goals. J Pers Soc Psychol 2007;92:1087–101. [DOI] [PubMed] [Google Scholar]
- 33.Masten A, Morison P, Pellegrini D. A revised class play method of peer assessment. Dev Psychol 1985;2:523–33. [Google Scholar]
- 34.Baer RA, Smith GT, Hopkins J, Krietemeyer J, Toney L. Using self-report assessment methods to explore facets of mindfulness. Assessment 2006;13:27–45. [DOI] [PubMed] [Google Scholar]
- 35.Greco LA, Baer RA, Smith GT. Assessing mindfulness in children and adolescents: development and validation of the Child and Adolescent Mindfulness Measure (CAMM). Psychol Assess 2011;23:606–14. [DOI] [PubMed] [Google Scholar]
- 36.Kochanska G, Kim S. Early Attachment Organization with Both Parents and Future Behavior Problems: From Infancy to Middle Childhood. Child Dev 2013;84:283–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Liu J, Leung P, Yang A. Breastfeeding and active bonding protects against children's internalizing behavior problems. Nutrients 2013;6:76–89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Margolin G, Gordis EB. The Effects of Family and Community Violence on Children. Annu Rev Psychol 2000;51:445–79. [DOI] [PubMed] [Google Scholar]
- 39.Mchale JP, Rasmussen JL. Coparental and family group-level dynamics during infancy: Early family precursors of child and family functioning during pre-school. Dev Psychopathol 1998;10:39–59. [DOI] [PubMed] [Google Scholar]
- 40.Li Y, Cui N, Cao F, Liu J. Children’s bonding with parents and grandparents and its associated factors. Child Indicators Res 2015;in press. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Straus MA, Gelles RJ. Physical Violence in American Families: Risk Factors and Adaptations to Violence in 8145 Families. New Brunswick, NJ: Transaction Publishers, 1990. [Google Scholar]
- 42.Straus MA, Hamby SL, Finkelhor D, Moore DW, Runyan D. Identification of child maltreatment with the Parent-Child Conflict Tactics Scales: development and psychometric data for a national sample of American parents. Child Abuse Negl 1998;22:249–70. [DOI] [PubMed] [Google Scholar]
- 43.Achenbach TM, Rescorla LA. Manual for the ASEBA Adult Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families, 2003. [Google Scholar]
- 44.Achenbach TM, Rescorla LA. Manual for the ASEBA School-Age Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families, 2001. [Google Scholar]
- 45.Achenbach TM, Rescorla LA. Manual for the ASEBA Preschool Forms & Profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth, & Families, 2000. [Google Scholar]
- 46.Liu J, Cheng H, Leung PW. The application of the pre-school Child Behavior Checklist and the caregiver-teacher report form to Mainland Chinese children: syndrome structure, gender differences, country effects, and inter-informant agreement. J Abnorm Child Psychol 2011;39:251–64. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Liu J, Leung P, Sun R, Li HT, Liu JM. Cross-cultural application of Achenbach System of Empirically Based Assessment: instrument translation in Chinese, challenges, and future directions. World J Pediatr 2012;8:5–10. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Liu J, Ai Y, McCauley L, et al. Blood lead levels and associated sociodemographic factors among pre-school children in the South Eastern region of China. Paediatr Perinat Epidemiol 2012;26:61–69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Liu J, Hanlon A, Ma C, Zhao SR, Cao S, Compher C. Low blood zinc, iron, and other sociodemographic factors associated with behavior problems in pre-schoolers. Nutrients 2014;6:530–45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Liu J, Shi Z, Spatz D, Loh R, Sun G, Grisso J. Social and demographic determinants for breastfeeding in a rural, suburban and city area of South East China. Contemp Nurse 2013;45:234–43. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Liu J, Ai YX, Hanlon A, Shi Z, Dickerman B, Compher C. Micronutrients deficiency and associated sociodemographic factors in Chinese children. World J Pediatr 2011;7:217–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Sun G, Jia G, Peng H, Dickerman B, Compher C, Liu J. Trends of Childhood Obesity in China and Associated Factors. Clin Nurs Res 2015;24:156–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Liu J, McCauley L, Compher C, et al. Regular breakfast and blood lead levels among pre-school children. Environ Health 2011;10:10–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Liu J, McCauley L, Yan C, Shen X, Pinto-Martin J. Low blood lead levels and hemoglobin concentrations in pre-school children in China. Toxicol Environ Chem 2012;94:423_26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Liu J, Hwang WT, Dickerman B, Compher C. Regular breakfast consumption is associated with increased IQ in kindergarten children. Early Hum Dev 2013;89:257–62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Liu J, Lynn R. An Increase of Intelligence in China 1986-2012. Intelligence 2013;41doi: 10.1016/j.intell.2013.06.017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Ai Y, Zhao SR, Zhou G, Ma X, Liu J. Hemoglobin status associated with performance IQ but not verbal IQ in Chinese pre-school children. Pediatr Int 2012;54:669–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Liu J, Zhou G, Wang Y, Ai Y, Pinto-Martin J, Liu X. Sleep problems, fatigue, and cognitive performance in Chinese kindergarten children. J Pediatr 2012;161:520–25.e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Liu J, Lynn R. Factor structure and sex differences on the Wechsler Preschool and Primary Scale of Intelligence in China, Japan and United States. Pers Individ Dif 2011;50:1222–26. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 60.Liu J, Li L. Parent-reported mild head injury history and behavioural performance in children at 6 years. Brain Inj 2013;27:1263–70. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Liu J, Leung PW, McCauley L, Ai Y, Pinto-Martin J. Mother's environmental tobacco smoke exposure during pregnancy and externalizing behavior problems in children. Neurotoxicology 2013;34:167–74. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Liu J, Portnoy J, Raine A. Association between a marker for prenatal testosterone exposure and externalizing behavior problems in children. Dev Psychopathol 2012;24:771–82. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Ivanova MY, Achenbach TM, Rescorla LA, et al. Preschool psychopathology reported by parents in 23 societies: testing the seven-syndrome model of the child behavior checklist for ages 1.5-5. J Am Acad Child Adolesc Psychiatry 2010;49:1215–24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Ivanova MY, Achenbach TM, Rescorla LA, et al. Syndromes of collateral-reported psychopathology for ages 18-59 in 18 Societies. Int J Clin Health Psychol 2015;15:18–28. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65.Ivanova MY, Achenbach TM, Rescorla LA, et al. Syndromes of Preschool Psychopathology Reported by Teachers and Caregivers in 14 Societies Using the Caregiver-Teacher Report Form (C-TRF). J Early Child Infant Psychol 2011;7:99–116. [Google Scholar]
- 66.Rescorla LA, Achenbach TM, Ivanova MY, et al. International comparisons of behavioral and emotional problems in pre-school children: parents' reports from 24 societies. J Clin Child Adolesc Psychol 2011;40:456–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Rescorla LA, Achenbach TM, Ivanova MY, et al. Behavioral/Emotional Problems of Preschoolers: Caregiver/Teacher Reports From 15 Societies. J Emot Behav Disord 2012;20:68–81. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 68.Ji X, Liu J. Associations between blood zinc concentrations and sleep quality in childhood: A Cohort Study. Nutrients 2015;7:5684–96. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Wang Y, Yan C, Pinto-Martin J, Dinges D. Early blood lead levels and sleep disturbance in preadolescence. Sleep 2015;[Epub ahead of print]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Liu J, Tuvblad C, Li L, Raine A, Baker LA. Medical record validation of maternal recall of pregnancy and birth events from a twin cohort. Twin Res Hum Genet 2013;16:845–60. [DOI] [PMC free article] [PubMed] [Google Scholar]