

Abstract
After radioactive incidents, the exposure risk in daily activities among children is a major public concern. However, there are limited methods available for evaluation of this risk, which is essential to future health risk management. To this end, this study assessed the relationship between behavioral patterns of school children and radiation exposure for a period of 18–20 months following the 2011 Fukushima nuclear incident. The assessed population comprised 520 school children from Minamisoma city, located 20 km north of the nuclear plant. Data for the doses were obtained using individual dosimeters and from results of a behavior survey administered by the City Office. The mean value of the doses in the study period was 0.34 mSv, with a standard deviation of 0.14 mSv, indicating an annual dose of ∼1.36 mSv, which includes doses from natural sources. Our results showed that behavior with respect to outdoor activities had no statistically significant relationship to the dose. A 0.1 μSv/h increase in the air dose rate at home was associated with a 10% increase in the dose; however, a 0.01 μSv/h increase in the air dose rate on the school grounds was associated with a 2% increase in the dose. This study indicates that the air contamination levels at the places where children spend most of their day are the significant predictors of the dose, as opposed to the levels at those outdoor locations in which short periods of time spent.
Keywords: Fukushima nuclear incident, external radiation dose, school children, behavior pattern
INTRODUCTION
Following radioactive incidents, cumulative radiation exposure is a major concern for the general public, medical practitioners, and policy makers [ 1–2 ]. To reduce the radiation-related health risks, it is very important to gather scientific knowledge and information at both the individual and policy levels on risk factors associated with the exposure [ 1–2 ].
The radiation dose can be composed of both external and internal radiation exposure (from sources outside or inside the body, respectively) [ 3 ]. After the 2011 Fukushima nuclear incident in Japan, the government and local authorities responded quickly; hence, internal contamination in the majority of the population in the affected areas was marginal [ 4–7 ]. There was a special focus on foodstuff contamination management, including inspection of foodstuffs circulating on the market and screening for internal contamination using whole-body radiation counters [ 4 , 8 ]. Accordingly, most of the total radiation dose among the population has been attributed to external radiation exposure [ 9–10 ], and this has received increasing research interest with a view to collective action for reducing the radiation doses.
External exposure to radiation has been evaluated from the levels of air and/or soil contamination using individual radiation dosimetry and modeled estimation [ 1 , 11 ]. Direct measurement can only indicate the individual-level radiation dose at monitored time-points. Hence, it is difficult to directly measure long-term (year- or life-long) radiation exposure or dosage levels in large numbers of the population. Modeled estimation can be flexible and applicable to scope and timeliness of interest, depending on model constructs/parameters; thus, it is an important approach for dose evaluation [ 12 ]. However, owing to the lack of scientific knowledge and evidence concerning the risk factors of the exposure, model estimates have been accompanied with uncertainties of the assumed limited exposure scenarios [ 12 , 13 ]. This produces some levels of disagreement between the estimated doses and the direct measurements of doses [ 14 ]. To address this, Japanese researchers conducted the first study after the Fukushima incident that individually compared levels of exposure directly measured by radiation dosimeters and those reconstructed by the Japanese government–proposed equation model. Their results showed that 18–30 months after the incident, the modeled estimates of doses among school children were three times higher than the measured doses [ 15 ]. In addition, the levels of the disagreement had a large variance among the study population, indicating the potential absence of important variables in the estimation model, e.g. behaviors and/or living environment that could be significantly associated with chance of radiation exposure.
A rigorous investigation into an individual's potential risk factors is needed for a reliable evaluation of external exposure with accurate model estimates under more appropriate exposure scenarios. Since October 2011, voluntary external radiation exposure screening has been conducted among school children in the city of Minamisoma, Fukushima prefecture, using individual radiation dosimeters. The screened participants were also asked questions about their daily and weekly behavioral patterns. Data from these investigations were used to assess the relationship between the behavioral patterns of school children and the external dose 18 to 20 months after the incident. This is the first individual-level assessment of external radiation exposure risk in the aftermath of the 2011 nuclear incident in Japan.
MATERIALS AND METHODS
Ethics statement
Ethical approval for this study was granted by the ethics committee of the Minamisoma Municipal General Hospital (MMGH) in Minamisoma city, under authorization number 25–08. The ethics committee agreed that written informed consent was not necessary for participants in this study. Although the original participant data contained personal-identifiable information (i.e. household address), it was subsequently geocoded into latitude and longitude coordinates, and anonymized and de-identified in MMGH prior to data analyses by replacing the address information with air dose rate information (see the subsection Air dose rate at home below).
Data collection
Setting
In response to public requests, since 1 October 2011, Minamisoma city has been offering a free-screening program of external radiation exposure for infants, school children and pregnant women who are registered in the Minamisoma family registry. This program is jointly supported Chiyoda Technol Corporation, which is a privately held Japanese company that manufactures and sells radiation products used in medicine, pharmacology, biology, agriculture and other fields [ 16 ]. The program notification was released on the official website of MMGH and disseminated using the city's public magazine. The notification letter was also sent to all schools in Minamisoma city.
The screening program has been implemented once every three months, using the following procedures: (i) the city office sends a radiation dosimeter (Glass Badge: GD-450, Chiyoda Technol Corp.) to the program participants; (ii) the participants are instructed on proper use of the Glass Badge (i.e. hang the Glass Badge from the neck); (iii) after the 3-month measurement is completed, the Glass Badge is sent back to the City Office, and the measured dose is recorded at MMGH.
In response to public concern about risk behavior among children exposed to radiation, Minamisoma city also conducted a questionnaire survey for school children. The questionnaire was completed by the children or their parents. The answer sheet was returned to the City Office, along with the Glass Badge. This survey questioned children's behavioral patterns at home and school during the measurements. In addition, the survey included questions on the conditions in which the Glass Badge was worn, such as, the hours of use on school days and weekends. This allowed for an assessment of the degree of adherence to the Glass Badge equipment instructions.
Target population and analytical data
Given the large numbers of responses to the behavior survey, the present study used the data for school children that participated in the fourth screening program, conducted between 1 September 2012 and 31 November 2012. The study dataset comprises two records: (A) the Glass Badge records of the participants and (B) the corresponding behavior survey results.
Dataset A included demographic characteristics, such as gender, school level, school name, and dwelling area (i.e. rural or urban area). We considered an urban area to include 4000 people per km 2 . The dataset also contained the 3-month radiation dose (mSv), measured in terms of a dose equivalent at a tissue depth of 1 cm (Hp(10)) [ 17 ]. The dose attributed to natural sources, such as the universe (including cosmic rays) and the earth (including 222 Radon) was subtracted from the original Glass Badge measurements of dose by default. The Glass Badge data obtained were, therefore, referred to as the ‘additional’ dose after the Fukushima incident. These subtracted values were 0.053 mSv (0.024 μSv/h × 3 months) from the universe and 0.083 mSv (0.038 μSv/h × 3 months) from the earth, and these levels were measured before the incident by Chiyoda Technol Corp. using Glass Badges at Oarai, Ibaraki prefecture, located more than 100 km south of the Fukushima Nuclear Plant. Owing to errors in the Glass Badge measurements, the additional dose of some participants was below zero after automatic subtraction of the background doses, causing a left-censoring effect at zero mSv. However, note that for easier clinical and policy interpretations, these dose values (i.e. 0.14 mSv/3 months in total) were re-added to the collected data [ 18 ]. Namely, the Glass Badge measurements of additional dose were replaced with the measurements of ‘total’ doses; accordingly, the data were left-censored at 0.14 mSv. Note that the range of accuracy of the Glass Badge measurement of the cumulative dose in 35 days was ±4%. The Hp(10) values measured in the geometrical conditions of the affected areas are known to be comparable with the effective dose of isotropic (ISO), or rotational (ROT), irradiation geometries [ 12 , 19 ]. The effective dose is the weighted sum of equivalent doses to various tissues and organs.
Dataset B had four subsets regarding behavioral patterns: at home (e.g. a room in which most daytime hours were spent), during commute to school (e.g. school commuting time), at school (e.g. seat position in the classroom), and after school or on weekends (e.g. place where most after-school hours were spent). Furthermore, the air dose rate at the participants' household and school (see below) was also considered.
Air dose rate at home
Data were collected from the official website of the Ministry of Education, Culture, Sports, Science and Technology (MEXT). After the nuclear incident, MEXT has irregularly conducted airborne monitoring within an 80-km radius of the nuclear power plant. The monitoring was performed at 300 m above the ground and the track width was ∼1.85 km. The recorded data included the average of the measured values within circles with a diameter of ∼600 m at ground level. The data contains the air dose rate (μSv/h) at a height of 1 m above the ground measured in terms of the ambient dose equivalent (H*10) [ 17 ], which includes the natural radiation background only from the earth [ 20 ], and the latitude and longitude coordinates of their monitoring points. All monitored results are open to the public and available online.
The air dose rate at each participant's household was then calculated using the following approach. First, because the fourth Glass Badge measurement was conducted in the period between 1 September and 31 November 2012, while the MEXT monitoring took place twice in 2012 (28 June and 16 November [ 21 , 22 ], a time interpolation method was applied to estimate the air dose rate during the measurement periods. Second, the MEXT monitoring results were averaged by a 500-m 2 mesh on the basis of the Japan Profile for Geographical Information Standards (elevation and slope angle fourth mesh data) [ 23 ], which was developed and released by the Ministry of Land, Infrastructure and Transport, Japan, such that each participant's household belonged to a mesh area. This approach enabled estimation of the air dose rate at home for each participant's datasets during the Glass Badge measurements.
Air dose rate at school
The Fukushima prefecture carried out air contamination monitoring between 19 June and 11 July 2012 for each school in Minamisoma city. It was measured in terms of the ambient dose equivalent (H*10) [ 17 ], which included the natural radiation background from the earth. The data included the air dose rate [μSv/h] at a height of 1 m above ground at the school ground, main gate, and entrance/exit of the school. All results are open and available for public access [ 24 ].
Data analysis
Exploratory analysis
The 3-month Glass Badge measurements of the dose of the participants were compared by demographic characteristics. The Glass Badge measurements were expected to contain quantization errors; therefore, an accuracy of two significant digits might be appropriate to present the results. However, we accepted an accuracy of three significant digits because the participants' 3-month dose was not very large; hence, the potential difference in the doses between characteristics might not be confirmed if the doses were presented in two significant digits. A histogram of the doses was also constructed for easier understanding of the left-censoring effect of the Glass Badges.
The differences in the behavior survey results were investigated for three school levels because the behavioral patterns were expected to exhibit substantial difference with respect to the school level. To compare the proportions between groups, a Chi-squared test was used. The mean differences in two groups was evaluated by an unpaired t -test, and for multiple comparisons, a one-way ANOVA was applied, followed by a Scheffe's post hoc test. P -values < 0.05 were regarded as statistically significant.
Regression modeling
To evaluate the relationship between behavioral patterns among school children and radiation exposure, a Tobit regression analysis was conducted, which enabled estimation of their linear relationships, adjusting for the left-censoring effect of the Glass Badge [ 25 ]. The natural logarithm of the dose was applied to the dependent variable, given the potential outliers among the school children (i.e. those who showed relatively higher dose levels). Since the regression coefficients for each of the independent variables were computed on a logarithmic scale, we used the exponentiated forms of the coefficients in the regression results, which indicate the multiplicative change in the dose level for a per unit increase in the variables. In this analysis, the Tobit model was extended by regarding ‘school’ as a random variable, reflecting unobservable random differences between the populations in each school. Construction of the regression model was based on a backward-stepwise procedure with a P -to-remove value of 0.05. A backward-stepwise regression starts with all the candidate variables in the model, and then continues by removing the least significant variables until all the remaining variables are statistically significant. The partial F -test was used to verify the entry and removal of variables from the model. All statistical analyses were conducted using STATA/MP 13.
RESULTS
Characteristics of the subjects
A total of 1956 school children participated in the fourth screening program. After excluding those with missing data regarding the basic characteristics, such as their household addresses, and those who lived outside of Minamisoma city or in its adjacent areas, we were left with 1658 children. We also excluded individuals who did not adhere to the Glass Badge equipment instructions, including those who did not wear the Glass Badge while commuting to school or while they were outdoors (low-adherence group), leaving 520 children (high-adherence group) for the analyses. A significant difference between the low- and high-adherence groups was observed only in terms of the school level ( P = 0.001), showing that the high-adherence group had a slightly higher proportion of high school children than the low-adherence group. The 520 participants accounted for ∼13% of the total school children in the city during the measurement period. Demographic characteristics of the children are shown in Supplementary Data Appendix A . No significant differences in the characteristics were observed between the school levels.
Glass badge measurements of dose
Distribution of the dose measurements using the Glass Badges over a period of three months is shown in Fig. 1 ; it illustrates the left-censoring effect of the Glass Badge at 0.14 mSv. Table 1 presents the measurements of dose by characteristics. The mean value of the dose for 520 individuals was found to be 0.34 mSv, with a standard deviation (SD) of 0.14 mSv. High school children showed significantly higher doses than primary school children by 0.06 mSv ( P < 0.05) and secondary school children by 0.02 mSv ( P < 0.001). Differences for gender and dwelling areas (rural or urban) were not observed.
Fig. 1.
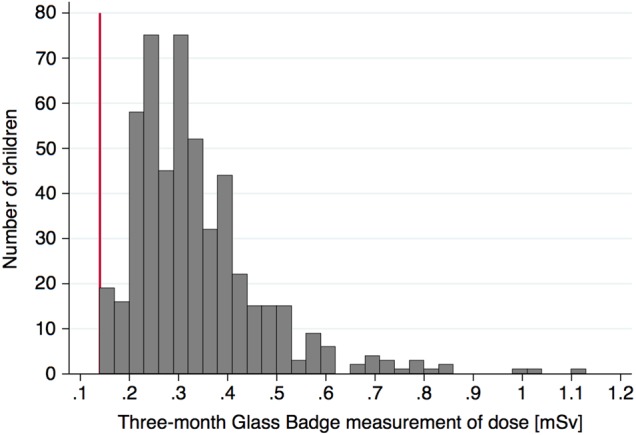
Histogram of the 3-month Glass Badge measurement of doses. The red line on the x -axis at x = 0.14 indicates the background dose and the left-censoring effect of the Glass Badge measurement.
Table 1.
Three-month measurements of doses a (mSV) expressed as mean (SD), using Glass Badges
| Gender | |
| Male | 0.34 (0.13) |
| Female | 0.34 (0.14) |
| Dwelling area | |
| Rural | 0.34 (0.14) |
| Urban | 0.33 (0.12) |
| School level** | |
| Primary | 0.32 (0.14) |
| Secondary | 0.36 (0.11) |
| High | 0.38 (0.12) |
a Includes doses from the universe and the earth. ** P < 0.001 by ANOVA: significant differences were observed between primary and secondary ( P < 0.05), and between primary and high ( P < 0.001) school students by Scheffé's test.
Behavioral survey results
Differences in behavioral patterns by school levels were explored ( Supplementary Data Appendix B: Parts 1–4 ). With regard to behaviors at home (Part 1), significant differences were observed only in terms of the room variable in which most of the daytime hours were spent ( P < 0.001). While 27% of the secondary and 38% of the high school children spent the daytime hours in their own rooms, 90% of the primary school children spent time in a living (family) room. Children also had different preferences or choices regarding a room for sleeping by school level ( P < 0.001). For behaviors while commuting to school (Part 2), both the commuting time and the commuting means differed by school level ( P < 0.001). Primary children were found to be more likely to use a car to go to school (80%), and the commute was <30 min for 91% of them. Secondary and high school children commuted to school by bicycles or walking (51% and 74%, respectively). For 46% of the high school children, it took more than 30 min to reach their school. For behaviors at school, a remarkable difference was observed in the places where most lunch breaks were spent ( P < 0.001). While about half of the primary school children spent their lunch-break time indoors (43%), only 5% of the secondary and 3% of the high school children had lunch indoors. For behaviors after school and on weekends, some of the children showed significant differences by school level; however, a substantial/meaningful difference was not observed.
Relationship of behavioral patterns to radiation exposure
Results of the multiple Tobit regression model, with a random effect for schools, are shown in Table 2 . Because of the small range of air dose rate at home (0.19–1.38 μSv/h) and on the school ground (0.06–0.22 μSv/h) between the participants, the results indicate a multiplicative change in the dose level for an increase per 0.1 and 0.01 μSv/h of the air dose rate, respectively. In this analysis, variables that were considered of public interest were incorporated into the final model, regardless of their statistical significance. Following which, the final model was evaluated using sensitivity analyses by omitting each variable one by one; the results of the evaluation showed similar outcomes (data not shown).
Table 2.
Multiple Tobit regression model with a random effect for schools
| Variable | Relative risk (95% CI) |
|---|---|
| Air contamination levels | |
| Air dose rate at home (0.1 μSv/h) | 1.10 (1.08–1.12)*** |
| Air dose rate in the school ground (0.01 μSv/h) | 1.02 (1.00–1.03)* |
| Basic demographic characteristics | |
| Age | 1.01 (0.99–1.03) |
| Gender | |
| Male | Ref. |
| Female | 1.03 (0.97–1.09) |
| Dwelling area | |
| Rural | Ref. |
| Urban | 1.04 (0.97–1.12) |
| School level | |
| Primary | Ref. |
| Secondary | 1.08 (0.94–1.25) |
| High | 1.06 (0.87–1.31) |
| Behavioral patterns at home | |
| Room where most daytime hours were spent at home | |
| Living (family) room | Ref. |
| Own room | 1.11 (0.99–1.23) |
| Floor of room where most daytime hours were spent at home | |
| 1st floor | Ref. |
| 2nd floor or above | 0.90 (0.82–1.00) |
| Place to sleep | |
| Living (family) room | Ref. |
| Own room | 1.00 (0.90–1.12) |
| Other | 1.11 (0.99–1.25) |
| Floor of place to sleep | |
| 1st floor | Ref. |
| 2nd floor or above | 1.01 (0.94–1.09) |
| Behavioral patterns during commute | |
| School commuting time (h) | |
| <0.5 | Ref. |
| ≥0.5 | 1.00 (0.90–1.11) |
| School commuting means | |
| Bicycle or walk | Ref. |
| Car | 0.97 (0.90–1.04) |
| Bus | 0.93 (0.79–1.10) |
| Behavioral patterns at school | |
| Seat position in the classroom | |
| Window area | Ref. |
| Center area | 0.90 (0.84–0.97)** |
| Passage area | 0.95 (0.87–1.03) |
| Not decided | 0.95 (0.85–1.07) |
| Number of times outdoor class exercise was done per week | |
| 0 | Ref. |
| 1 | 1.06 (0.96–1.16) |
| 2 | 1.01 (0.92–1.11) |
| More than three | 1.04 (0.94–1.14) |
| Outdoor sports club at school | |
| No | Ref. |
| Yes | 1.00 (0.91–1.11) |
| Behavioral patterns after school and on weekends | |
| Hours spent outdoors after school (h) | |
| <0.5 | Ref. |
| 0.5–1.0 | 1.03 (0.97–1.10) |
| >1.0 | 0.98 (0.89–1.09) |
| Hours spent outdoors on weekends (h) | |
| <0.5 | Ref. |
| 0.5–1.0 | 0.98 (0.91–1.06) |
| 1.0–2.0 | 1.04 (0.96–1.13) |
| >2.0 | 0.96 (0.87–1.07) |
* P < 0.05, ** P < 0.01, *** P < 0.001.
Our results indicate that behaviors related to outdoor activities, such as commuting hours and means, number of outdoor class exercises per week, outdoor sports club, and hours spent outdoors after school and on weekends, had no significant statistical relationship with the doses over the 3-month period (Table 2 ). Meanwhile, a 0.1 μSv/h increase in the air dose rate at home was associated with a 10% increase in the dose ( P < 0.001). A 2% increase in the dose for every 0.01 μSv/h increase in the air dose rate was observed for the school ground ( P = 0.01). In addition, after adjusting for covariates, the doses found in students sitting in the central areas in classrooms were lower than in those students using the window seats by 10% ( P < 0.01), indicating the seating position to be a significant factor affecting the dose.
Note that although a substantive significant difference was found in the mean dose between the three different school levels (Table 1 ), the statistical significance of this difference disappeared after adjusting for covariates in the regression analysis (Table 2 ). The regression analysis demonstrated that the air dose rate at home/school might affect the doses in children; therefore, we analyzed this relationship at the home/school and school level (Table 3 ). Large and statistically significant differences in air dose rates at home/school were observed by school level, with high-school children more likely to experience higher air dose rates at home/school. This result explains the higher dose in high-school children than that in the primary- and secondary-school children.
Table 3.
Air dose rate at a height of 1 m above ground at home and school (μSv/h)
| Primary | Secondary | High | Total | |
|---|---|---|---|---|
| Home* | 0.47 (0.17) | 0.54 (0.21) | 0.52 (0.25) | 0.49 (0.20) |
| School main gate** | 0.21 (0.06) | 0.22 (0.05) | 0.30 (0.07) | 0.22 (0.06) |
| School entrance/exit*** | 0.16 (0.05) | 0.17 (0.03) | 0.25 (0.10) | 0.17 (0.06) |
| School ground**** | 0.11 (0.03) | 0.11 (0.02) | 0.15 (0.04) | 0.11 (0.03) |
Results are presented as mean (SD). * P < 0.001 by ANOVA: significant differences were observed between primary and secondary ( P < 0.01) school students by Scheffé's test. ** P < 0.001 by ANOVA: significant differences were observed between primary and secondary ( P < 0.05), primary and high ( P < 0.001), and secondary and high ( P < 0.001) school students by Scheffé's test. *** P < 0.001 by ANOVA: significant differences were observed between primary and high ( P < 0.001), and secondary and high ( P < 0.001) school students by Scheffé's test. **** P < 0.001 by ANOVA: significant differences were observed between primary and high ( P < 0.001), and secondary and high ( P < 0.001) school students by Scheffé's test
These findings indicate that the air contamination levels at home and school, where children spend the majority of their time, are better for evaluating the risk of radiation exposure in children than considering the outdoor activities in a short period of time.
DISCUSSION
Following the 2011 Fukushima nuclear incident in Japan, a rigorous evaluation of the external exposure risk has been lacking due to a limited availability of information related to daily behaviors of individuals [ 2 ]. Monitoring the daily behavior of individuals is challenging, owing to the technical and practical difficulties, as well as barriers involving privacy issues that make people reluctant to agree to participate in monitoring exercises. The external radiation screening by the city of Minamisoma offered a unique and valuable opportunity to perform a retrospective study with a sufficient amount of quantitative behavioral data. This study involved the assessment of radiation exposure risk among school children. To date, this is the first assessment of the external radiation exposure at an individual level after the nuclear incident in Japan.
Our study showed that the mean value of the dose measured over the period of 18–20 months following the incident was 0.34 mSv in the participating school children in Minamisoma city; this dose amounted to a rough annual exposure of ∼1.36 mSv, including doses from natural sources such as the universe and the earth.
The results of this study indicated that, after adjusting for covariates, the factors that had a significant relationship to the dose were air dose rates at home and school (Table 2 ). In addition, a point estimate of the relative risk of spending time on the 2nd floor or above was 0.90 in relation to the 1st floor, though it was not statistically significant ( P = 0.06). This might reflect the fact that the air dose rates at higher altitudes were slightly lower than that on the ground level. The results related to the seating position in the school classroom explained the different air dose rates at different points inside the classroom. Although this difference might not be very large, due to the long periods of time spent by the children in the classroom every day, the effect of the differences in the air dose rate on the total doses was statistically significant, particularly with regard to the lower doses in the central area as opposed to the window area. However, the results obtained regarding variables such as room (and floor of the room) where most daytime hours were spent at home, indicated they were not significant. This was likely because the differences in the air dose rates between the different rooms/floors were not too large, or because the sleeping hours of the children were not long enough to result in a difference in the dose rate by floor.
In addition, the variables of time spent outdoors while commuting to school, after school, and on weekends were not statistically significant, as indicated by the doses measured over three months through the Glass Badge. Note that in this study, the majority of the participants did not spend much time outdoors: 84% spent <30 min while commuting to school, 88% spent <1 h after school, and 86% spent <2 h on weekends ( Supplementary Data Appendix B: Parts 2 and 4 ). These non-significant results indicate that the effects of outdoor activities over a short period of time on the total dose were marginal and could not be detected by the regression analyses. Other relevant outdoor activities, such as outdoor class exercise and sports club activities, also had no significant relationship to the dose for the same reason mentioned above.
These findings contrast with current concerns emerging from the public in the affected areas. In an attempt to reduce potential radiation exposure, many schools in the radiation-contaminated areas in the Fukushima prefecture have adopted countermeasures by placing restrictions on the number of weekly outdoor exercise classes, and other outdoor activities, including club activities after school. Another major concern was the potential presence of spots with exceptionally high contamination in the school commuting zones, which were referred to as ‘hot spots’. As a result, 80% of parents took their primary school children to school by car for protection against the radiation ( Supplementary Data Appendix B: Part 2 ). In addition, 40% of the participants who answered the survey believed that they were most exposed to radiation during the commuting hours (data not shown in tables). Contrary to these concerns, this study demonstrated that exposure risk during outdoor activities and school commuting over short periods of time might be marginal.
We identified a few limitations in this study. First, the external screening program was conducted on a voluntary basis, and the individuals with low adherence to the Glass Badge equipment instructions were excluded from the analyses, bringing the percentage of the school children participating in the study down to only 13% in Minamisoma city at the time of the dose measurement. However, no significant differences in the behavioral patterns were observed between the low- and high-adherence groups, except in terms of the school commuting time ( P < 0.05: Chi-squared test), which was not a significant variable in the regression analysis. This limitation did not, therefore, influence our conclusions. Second, the study comprised a population of school children whose daily behavioral patterns as well as living environment might differ from the population in other age groups; therefore, the results could not be generalized to the entire population.
This study indicates that air contamination levels at places where children spend most of the day can be the significant predictors of the dose, rather than an association with outdoor activities undertaken over short periods of time. These levels, therefore, are essential for evaluating exposure risk in children. This information is invaluable in helping parents, communities, health planners, and disaster coordinators, develop a well-optimized protection plan against radiation.
AUTHOR CONTRIBUTION
All authors were responsible for the study concept and design. MT, YK and TO acquired data, which was analyzed and interpreted by all authors. SN and MT drafted the manuscript, which was critically revised for important intellectual content by all authors. SN and TF performed the statistical analysis. YK and TO provided administrative, technical and material support. TF, RH, MK and TO served as the study supervisors. All authors have approved the final draft of the manuscript.
FUNDING
Funding to pay the Open Access publication charges for this article was provided by Minamisoma Municipal General Hospital.
Supplementary Material
ACKNOWLEDGEMENTS
We express our gratitude to the Minamisoma city employees and Minamisoma Municipal General Hospital staff for data collection and management. We are particularly grateful for the assistance given by Mr Kikugoro Sakaihara and Mr Masatsugu Tanaki from the Minamisoma Municipal General Hospital, in geocoding of the household addresses of the study participants. We also offer our special thanks to all the study participants as well as their parents and school teachers. Without their involvement, our study could not have reached its present form.
REFERENCES
- 1. World Health Organization . Preliminary dose estimation from the nuclear accident after the 2011 Great East Japan Earthquake and Tsunami . Technical report . Geneva: : World Health Organization, Geneva; , 2012. . [Google Scholar]
- 2. World Health Organization . Health risk assessment from the nuclear accident after the 2011 Great East Japan earthquake and tsunami, based on a preliminary dose estimation . Technical report . Geneva: : World Health Organization; , 2013. . [Google Scholar]
- 3. United Nations Scientific Committee on the Effects of Atomic Radiation . Annex D: Exposures from the Chernobyl accident . Technical report . New York: : United Nations Scientific Committee on the Effects of Atomic Radiation; , 1988. . [Google Scholar]
- 4. Tsubokura M, Gilmour S, Takahashi K, et al. Internal radiation exposure after the Fukushima nuclear power plant disaster . JAMA 2012. ; 308 : 669 – 70 . [DOI] [PubMed] [Google Scholar]
- 5. Tsubokura M, Kato S, Nihei M, et al. Limited internal radiation exposure associated with resettlements to a radiation-contaminated homeland after the Fukushima Daiichi nuclear disaster . PLoS One 2013. ; 8 : e81909 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Tsubokura M, Kato S, Nomura S, et al. Absence of internal radiation contamination by radioactive cesium among children affected by the Fukushima Daiichi nuclear power plant disaster . Health Phys 2015. ; 108 : 39 – 43 . [DOI] [PubMed] [Google Scholar]
- 7. Matsuda N, Kumagai A, Ohtsuru A, et al. Assessment of internal exposure doses in Fukushima by a whole body counter within one month after the nuclear power plant accident . Radiat Res 2013. ; 179 : 663 – 8 . [DOI] [PubMed] [Google Scholar]
- 8. Hamada N, Ogino H . Food safety regulations: what we learned from the Fukushima nuclear accident . J Environ Radioact 2012. ; 111 : 83 – 99 . [DOI] [PubMed] [Google Scholar]
- 9. Nagataki S, Takamura N, Kamiya K, et al. Measurements of individual radiation doses in residents living around the Fukushima Nuclear Power Plant . Radiat Res 2013. ; 180 : 439 – 47 . [DOI] [PubMed] [Google Scholar]
- 10. Harada KH, Niisoe T, Imanaka M, et al. Radiation dose rates now and in the future for residents neighboring restricted areas of the Fukushima Daiichi Nuclear Power Plant . Proc Natl Acad Sci U S A 2014. ; 111 : e914 – 23 . [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. United Nations Scientific Committee on the Effects of Atomic Radiation . Annex J: Exposures and effects of the Chernobyl accident . Technical report . New York: : United Nations Scientific Committee on the Effects of Atomic Radiation; , 2008. . [Google Scholar]
- 12. National Institute of Radiological Sciences; Japan Atomic Energy Agency . Researches on the characteristics of personal doses after the accident of TEPCO Fukushima Dai-ichi nuclear power plant . Technical report . Chiba: : National Institute of Radiological Sciences; Japan Atomic Energy Agency; , 2014. . [Google Scholar]
- 13. United Nations Scientific Committee on the Effects of Atomic Radiation . Annex A: Levels and effects of radiation exposure due to the nuclear accident after the 2011 great east-Japan earthquake and tsunami . Technical report . New York: : United Nations Scientific Committee on the Effects of Atomic Radiation; , 2014. . [Google Scholar]
- 14. Naito W, Uesaka M, Yamada C, et al. Evaluation of dose from external irradiation for individuals living in areas affected by the Fukushima Daiichi Nuclear Plant accident . Radiat Prot Dosimetry 2015. ; 163 : 353 – 61 . [DOI] [PubMed] [Google Scholar]
- 15. Nomura S, Tsubokura M, Hayano R, et al. Comparison between direct measurements and modeled estimates of external radiation exposure among school children 18 to 30 months after the Fukushima nuclear accident in Japan . Environ Sci Technol 2015. ; 49 : 1009 – 16 . [DOI] [PubMed] [Google Scholar]
- 16. Chiyoda Technol Corporation . The official homepage Tokyo . http://www.c-technol.co.jp/eng (5 June 2015, date last accessed).
- 17. International Commission on Radiological Protection . ICRP Publication 103: Recommendations of the ICRP . New York: : International Commission on Radiological Protection; , 2013. . [DOI] [PubMed] [Google Scholar]
- 18. Miyazaki M, Hayano R . Current individual radiation measurement in Fukushima . Isotope News 2014. ; 10 : 28 – 32(in Japanese) . [Google Scholar]
- 19. Hirayama H . An evaluation of personal dosimeter for widely distributed 134^Cs and 137^Cs by using EGS code . Radioisotopes 2013. ; 62 : 335 – 45 . [Google Scholar]
- 20. Nakamura T . Post accident radiation monitoring in the surrounding environment . Prog Nucl Sci Tech 2012. ; 10 : 30 – 5 . [Google Scholar]
- 21. Ministry of Education, Culture, Sports, Science and Technology . Results of the (i) fifth airborne monitoring survey and (ii) airborne monitoring survey outside 80 km from the Fukushima Dai-ichi NPP Tokyo . http://radioactivity.nsr.go.jp/en/contents/6000/5790/24/203_0928_14e.pdf (5 June 2015, date last accessed) . [Google Scholar]
- 22. Ministry of Education, Culture, Sports, Science and Technology . Results of the (i) sixth airborne monitoring and (ii) airborne monitoring out of the 80 km from the Fukushima Dai-ichi NPP Tokyo . http://radioactivity.nsr.go.jp/en/contents/7000/6099/24/203_e_0301_18.pdf (5 June 2015, date last accessed) . [Google Scholar]
- 23. Ministry of Land, Infrastructure and Transport . Japan Profile for Geographic Information Standards Tokyo . http://www.gsi.go.jp/ENGLISH/page_e30210.html (5 June 2015, date last accessed) . [Google Scholar]
- 24. Ministry of Education, Culture, Sports, Science and Technology . Results of the radiation monitoring. Measurement results of radiation monitoring action plan for supporting restoration of the former evacuation-prepared area in case of emergency (Minamisoma city, Tamura city, Kawauchi village) . http://radioactivity.nsr.go.jp/ja/contents/6000/5677/24/348_0706.pdf (5 June 2015, date last accessed) (in Japanese). [Google Scholar]
- 25. Sugimoto A, Gilmour S, Tsubokura M, et al. Assessment of the risk of medium-term internal contamination in Minamisoma City, Fukushima, Japan, after the Fukushima Dai-ichi nuclear accident . Environ Health Perspect 2014. ; 122 : 587 – 93 . [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.