

Abstract
Background
In our ageing society, valvular heart diseases (VHD) have become an increasing public health problem. However, the lack of studies describing the impact of these diseases on the outcome of very old subjects makes it difficult to appreciate their real clinical burden.
Methods
Prospective, observational, population-based cohort study in Belgium. Five hundred fifty six subjects aged 80 years and older were followed up for 5.1 ± 0.25 years for mortality and 3.0 ± 0.25 years for hospitalization. Echocardiograms were performed at baseline. The Cumulative Illness Rating Scale (CIRS) was calculated for each subject.
Results
The prevalence of moderate-to-severe VHD was 17 % (n = 97). Mitral stenosis was more prevalent in women and an age-dependent increase of the prevalence of severe aortic stenosis was seen. The overall disease burden was higher in participants with VHD (median CIRS 3 [IQR 3–5] vs 4 [IQR 3–6] (P = 0.008)). Moderate-to-severe VHD, and more specifically mitral stenosis and aortic stenosis, was found to be an independent predictor of both all-cause (HR 1.42 (95 % CI 1.04–1.95)) and cardiovascular mortality (HR 2.13 (95 % CI 1.38–3.29)). Moderate-to-severe VHD was also found to be an independent predictor of the need for a first unplanned hospitalization (HR 1.43 (95 % CI 1.06–1.94)).
Conclusions
A high prevalence of moderate-to-severe VHD was found in the very old. Moderate-to-severe VHD was identified as an independent risk factor for all-cause and cardiovascular mortality and as well for unplanned hospitalizations, independent of other structural cardiac abnormalities, ventricular function and major co-morbidities.
Keywords: Aged, 80 and over; Valvular heart disease; Mortality; Multimorbidity
Background
In the next several decades, the proportion of very old people living in industrialized countries will dramatically increase [1]. People aged 80 and older are indeed the fastest growing age segment in the Western World, and their numbers will peak by 2050 [2]. This forthcoming “grey epidemic” will lead to an explosion of chronic diseases and generate numerous complicated cases with multiple comorbid conditions.
In this ageing society, the burden of cardiac diseases is not only rising, but its very nature is also changing. Several population-based studies have indeed demonstrated that the prevalence of systolic dysfunction in the oldest old is steadily decreasing, whereas that of diastolic dysfunction and valvular heart diseases (VHDs) is increasing [3–6]. Survival effects and age-related changes in cardiac structure and function most likely explain this reverse epidemiology [6, 7]. Despite these observations, data on the clinical burden of VHDs in elderly subjects are scarce and mostly based on in-hospital series, which introduces an important selection bias. Although some observational studies have suggested that VHDs, and particularly aortic stenosis, negatively affect the physical capacity and mental performance of elderly patients [6], very few of these studies focused on their impact on patient’s outcome and quality of life. In the absence of relevant outcome data and evidence-based guidelines, the management of elderly patients with VHDs remains empirical and most often challenging [8]. Consequently, very old patients presenting with VHDs frequently refuse or are denied valve surgery, as the risk of cardiac surgery is often perceived to outweigh any possible clinical benefits [9–11]. Although with the advent of percutaneous treatments, these patients can nowadays be treated at a much a lower risk [8], the lack of studies describing the impact of VHDs on the outcome of very old subjects makes it difficult to appreciate the real benefits of these emerging treatments. In this context, the aim of the present study was to assess the prevalence, distribution patterns, and outcome consequences of significant (moderate-to-severe) left-sided VHDs in people aged 80 and older. Based on previous observations, we hypothesized that VHDs were not only highly prevalent but also beard significant and independent prognostic implications in very old subjects from the community.
Methods
Study population
The BELFRAIL study is a prospective, observational, population-based cohort study of subjects aged 80 years and older in three well-circumscribed areas of Belgium (Flanders, Brussels and Wallonia). All participants in the study gave informed consent, and the Biomedical Ethics Committee of the Université catholique de Louvain (UCL) in Brussels approved the study. The study design, methods and characteristics of the cohort were previously described in detail [12]. Briefly, 29 general practitioner (GP) centers were asked to include patients aged 80 and older. No other inclusion criteria were specified, and only three exclusion criteria were used: known severe dementia (mini-mental state examination < 15), palliative care, and medical emergency, such as acute onset heart failure or decompensated heart failure. The BELFRAIL cohort is representative in gender and age of the elderly living in Belgium [12].
Clinical evaluation
At study entrance, the GPs used a structured questionnaire to capture information on the patients’ medical history, cardiovascular risk factors, symptoms [13], and other current medical problems. These data were subsequently used to calculate the cumulative illness rating scale (CIRS) [14, 15], which was used as a multimorbidity index. The GPs were also asked to list the drugs the patients were taking on a regular basis or as needed. Drugs were classified according to the Anatomical, Therapeutic and Chemical (ATC) classification system (at level 5, which relates to the chemical substance). Data on relevant cardiovascular medications including diuretics, potassium-sparing agents, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, β-blockers and digitalis were also collected.
The subjects’ performance in basic activities of daily living (ADL) was assessed [12]. Cognitive functioning was measured by the Mini-Mental State Examination (MMSE). Depressive symptoms were measured in those with MMSE > 18 points by use of the 15-item Geriatric Depression Scale (GDS-15) [12].
Echocardiography
Echocardiographic data were obtained at the subject’s home using a commercially available portable system (CX50, Philips, Andover, Massachusetts, USA). All patients underwent a comprehensive examination, including M-mode and 2-dimensional echocardiography, as well as Doppler examinations, according to the recommendations of the American Society of Echocardiography and the European Association of Echocardiography (EAE) [16]. All tests were conducted by a certified cardiologist with level 3 competence in echocardiography.
The echocardiographic images were blindly analyzed by 1 or 2 observers with at least 2 years of experience in reading echocardiographic studies. All measurements were performed off-line using the XCelera software (Philips, Andover, Massachusetts, USA). In patients with poor quality images, all measurements were performed by the 2 observers and the averaged values were reported. In patients with good image quality, data were analyzed by only one single observer. To ensure adequate reproducibility, inter- and intra-observer variability was evaluated on a random sample of good quality echocardiograms. Intraclass correlation coefficients were always > 0.90.
LV volumes and LVEF were calculated by use of the biplane Simpson method, whereas LV mass was calculated according to Devereux et al [16]. Left atrial (LA) volume was measured using the biplane area-length formula. Systolic pulmonary artery pressure was considered to be equal to the systolic transtricuspid pressure gradient as calculated by use of the modified Bernoulli equation. No attempt was made to estimate right atrial pressure.
The function of the mitral, aortic and tricuspid valves was evaluated by use of standard continuous-wave, pulsed-wave and color Doppler echocardiograph, as recommended by the EAE [17–19]. In patients with aortic stenosis, stenosis severity was quantitated by use of the peak transaortic jet velocity, the mean transaortic gradient and the aortic valve area (continuity equation). In patients with mitral stenosis, stenosis severity was quantitated by use of the mean transmitral pressure gradient and the mitral valve area (direct planimetry or pressure half-time). The severity of aortic and mitral regurgitations was assessed semi-quantitatively on a scale of 1+ to 4+ by an integrated approach that included the size of the regurgitant jet in the receiving chamber, the proximal regurgitant jet width, the size of the proximal convergence zone and, when available, the regurgitant volume and the effective regurgitant orifice area. Mild, moderate and severe degrees of valve dysfunctions were graded as recommended by the EAE guidelines [18, 19].
Outcome measures
Two detailed follow-up questionnaires were filled in by the participating GPs after 1.4 ± 0.3 years and after 3.0 ± 0.3 years. The questionnaires included questions on mortality, cause of death and unplanned hospitalization. Mortality and cause of death were also recorded by the GPs 5.1 ± 0.3 years after baseline. The causes of death were divided into cardiovascular and non-cardiovascular causes, according to the GPs’ assessment and the subsequent review by 2 independent researchers blinded to all clinical data (BV and JD). The current study used all-cause mortality, cardiovascular mortality and first, all-cause, unplanned hospitalizations for > 24 h as outcome measures.
Data analysis
The data analysis was performed using SPSS 20.0 for Windows (SPSS Inc., Chicago, IL, USA). Continuous variables are reported as mean ± one standard deviation (SD) or median and inter-quartile range (IQR). Categorical variables are reported as numbers and frequencies. Comparisons between different categories of subjects were performed using a one-way ANOVA, the Mann-Whitney U test (nonparametric data) for unpaired data or the Jonckheere-Terpstra test (trend test), where appropriate.
Survival curves were computed using the Kaplan-Meier method and compared using the log-rank Chi square test. Determination of the factors independently associated with outcome was performed by use of a Cox's proportional-hazards survival analysis. For this purpose, all clinical, angiographic, and echocardiographic variables with p < 0.10 in the univariable analysis were proposed for inclusion into a multivariable Cox’s proportional-hazards survival model. In order to avoid multicollinearity, the correlation coefficients between all covariates were calculated. In case of multicollinearity (r-value >0.80), only one of the two covariables was considered in the multivariable model. Variable selection was performed using a stepwise, forward conditional selection procedure using the maximum partial likelihood ratio chi-square statistic (χ2 test) to enter (<0.05 level) or to remove (>0.05 level) a covariable into the model. Variables were entered until no F-to-enter statistics were significant at the 5 % level and until the mean squared error reached a minimum.
Results
Baseline clinical, hemodynamic and echocardiographic characteristics
Echocardiograms were obtained in 556 subjects (98 %), aged 84.7 ± 3.6 years, of whom 41 % were older than 85 and 9 % older than 90 years. The prevalence of moderate-to-severe VHD was found to be 17 %, and was similar in men (16 %) and women (18 %). Higher rates of MS were noted in women than in men (4.6 vs 1.5 %, p = 0.026). The prevalence of the other VHD was quite similar between men and women (13 vs 15 % for AS, 1.5 vs 1.7 % vs AR and 0.5 vs 0.9 % for MR). A significant trend in age-related prevalence was found for aortic stenosis, with a significantly increased prevalence of severe stenosis and a significantly decreased prevalence of mild stenosis in the very old (Table 1).
Table 1.
Prevalence of valvular heart disease
| 80–84 years | 85–89 years | ≥90 years | p for trenda | |
|---|---|---|---|---|
| Participants, n | 323 | 183 | 50 | |
| Male, n (%) | 125 (39 %) | 68 (37 %) | 13 (27 %) | |
| Mitral stenosis, n (%) | 10 (53 %) | 6 (3 %) | 3 (6 %) | |
| Mild, n (%) | 5 (2 %) | 3 (2 %) | 1 (2 %) | 0.85 |
| Moderate, n (%) | 4 (1 %) | 3 (2 %) | 2 (4 %) | 0.28 |
| Severe, n (%) | 1 (0.3 %) | 0 (0 %) | 0 (0 %) | 0.41 |
| Mitral regurgitation, n (%) | 236 (73 %) | 140 (77 %) | 39 (78 %) | |
| Mild, n (%) | 234 (72 %) | 138 (75 %) | 39 (78 %) | 0.32 |
| Moderate, n (%) | 2 (1 %) | 2 (1 %) | 0 (0 %) | 0.89 |
| Aortic stenosis, n (%) | 63 (20 %) | 45 (25 %) | 19 (38 %) | |
| Mild, n (%) | 27 (8 %) | 7 (4 %) | 1 (2 %) | 0.016 |
| Moderate, n (%) | 24 (7 %) | 15 (8 %) | 9 (18 %) | 0.10 |
| Severe, n (%) | 12 (4 %) | 11 (6 %) | 9 (18 %) | 0.002 |
| Aortic regurgitation, n (%) | 118 (37 %) | 72 (39 %) | 25 (50 %) | |
| Mild, n (%) | 113 (35.4) | 69 (37.9) | 24 (48.0) | 0.15 |
| Moderate, n (%) | 5 (1.6) | 3 (1.6) | 1 (2.0) | 0.85 |
aJonckheere-Terpstra Test
No significant differences in baseline characteristics were noted among subjects without any VHD and those with mild VHD. By contrast, higher rates of decompensated heart failure, stroke and chronic atrial fibrillation were noted in subjects with moderate-to-severe VHD as compared to those with no or mild VHD. The prevalence of heart failure related symptoms, such as dyspnea and peripheral edema were also higher among subjects with moderate-to-severe VHD than among those without (Table 2). Patients with moderate-to-severe VHD exhibited higher CIRS and GDS-15 scores, and lower ADL scores than those without. As shown in Table 3, patients with moderate-to-severe VHD exhibited larger LAs, LV masses, E/e’ ratios and E/A ratios, as well as shorter deceleration (DT) and isovolumic relaxation times than those without.
Table 2.
Clinical characteristics of the study population
| No VHD (n = 92) | Mild VHD (n = 367) | Moderate-to-severe VHD (n = 97) | p value | |
|---|---|---|---|---|
| Socio-demographic characteristics | ||||
| Male, n (%) | 38 (41 %) | 135 (37 %) | 33 (34 %) | <0.001 |
| Age, (years) | 84.1 ± 2.9 | 84.6 ± 3.6 | 86.3 ± 4.3 | 0.58 |
| Coronary risk factors and multimorbidity | ||||
| Smoking (current or ex), n (%) | 31 (34 %) | 122 (33 %) | 22 (23 %) | 0.11 |
| Hypertension, n (%) | 60 (66 %) | 258 (70 %) | 72 (74 %) | 0.46 |
| Dyslipidemia, n (%) | 40 (45 %) | 165 (46 %) | 37 (39 %) | 0.46 |
| Type 2 diabetes, n (%) | 21 (23 %) | 62 (17 %) | 19 (20 %) | 0.38 |
| CIRS, median (IQR) | 4 (3–5) | 3 (3–5) | 4 (3–6) | 0.008 |
| Prior history | ||||
| Myocardial infarction, n (%) | 17 (19 %) | 35 (10 %) | 8 (8 %) | 0.029 |
| TIA or stroke, n (%) | 15 (16 %) | 57 (16 %) | 29 (30 %) | 0.025 |
| COPD, n (%) | 13 (12 %) | 40 (11 %) | 10 (10 %) | 0.79 |
| Peripheral arterial disease, n (%) | 10 (11 %) | 29 (8 %) | 11 (11 %) | 0.45 |
| CABG, n (%) | 8 (9 %) | 20 (5 %) | 8 (8 %) | 0.39 |
| PCI, n (%) | 12 (13 %) | 30 (8 %) | 5 (5 %) | 0.13 |
| Valvular surgery, n (%) | 2 (2 %) | 15 (4 %) | 2 (2 %) | 0.48 |
| Heart failure, n (%) | 8 (9 %) | 36 (10 %) | 16 (16 %) | 0.14 |
| Chronic atrial fibrillation, n (%) | 4 (4 %) | 34 (9 %) | 19 (20 %) | 0.002 |
| Pacemaker, n (%) | 5 (6 %) | 21 (6 %) | 5 (5 %) | 0.97 |
| Symptoms | ||||
| Angina pectoris, n (%) | 11 (12 %) | 58 (16 %) | 21 (22 %) | 0.20 |
| Dyspnea ≥ 3a, n (%) | 22 (24 %) | 101 (28 %) | 42 (43 %) | 0.005 |
| Peripheral edema, n (%) | 31 (34 %) | 115 (31 %) | 42 (43 %) | 0.090 |
| Fatigue, n (%) | 17 (19 %) | 75 (21 %) | 22 (23 %) | 0.80 |
| Cardiac medications | ||||
| Diuretics, n (%) | 45 (49 %) | 162 (44 %) | 54 (56 %) | 0.12 |
| Potassium-sparing agents, n (%) | 17 (18 %) | 53 (14 %) | 17 (18 %) | 0.54 |
| ACE inhibitors, n (%) | 20 (22 %) | 123 (28 %) | 29 (30 %) | 0.39 |
| ARBs, n (%) | 18 (20 %) | 51 (14 %) | 17 (18 %) | 0.34 |
| ß-blockers, n (%) | 28 (30 %) | 161 (44 %) | 46 (47 %) | 0.035 |
| Digitalis, n (%) | 0 (0 %) | 11 (3 %) | 11 (11 %) | <0.001 |
| Physical activity and cognitive functioning | ||||
| ADL, median (IQR) | 25 (21–27) | 25 (21–28) | 23 (17–27) | <0.001 |
| MMSE, median (IQR) | 28 (26–29) | 28 (26–29) | 28 (25–29) | 0.36 |
| GDS-15, median (IQR) | 2 (1–4) | 2 (1–4) | 3 (2–5) | 0.033 |
aaccording to the Medical Research Council dyspnea scale. ACE angiotensin converting enzyme, ARB angiotensin receptor blocker, CABG coronary artery bypass graft surgery, CIRS cumulative illness rating scale, COPD chronic obstructive pulmonary disease, IQR interquartile range, PCI percutaneous coronary intervention, TIA transient ischemic attack
Table 3.
Echocardiographic characteristics of the study population
| No VHD (n = 92) | Mild VHD (n = 367) | Moderate-to-severe VHD (n = 97) | p value | |
|---|---|---|---|---|
| LV morphology and function | ||||
| LVEF (%) | 55 ± 3 | 55 ± 5 | 55 ± 3 | 0.60 |
| LVEF < 50 %, n (%) | 4 (4 %) | 26 (7 %) | 2 (2 %) | 0.14 |
| LV mass (g/m2) | 86 ± 21 | 92 ± 23 | 98 ± 27 | 0.002 |
| LVH, n (%) | 10 (11 %) | 57 (16 %) | 18 (19 %) | 0.33 |
| Indexed LAV (mL/m2) | 30 ± 9 | 32 ± 10 | 39 ± 12 | <0.001 |
| Indexed LAV > 34 mL/m2, n (%) | 23 (25 %) | 145 (40 %) | 62 (65 %) | <0.001 |
| Stroke volume (mL/beat) | 68 ± 19 | 70 ± 16 | 68 ± 14 | 0.48 |
| RWMA, n (%) | 13 (14 %) | 43 (12 %) | 7 (7 %) | 0.30 |
| LV diastolic filling | ||||
| E/A ratio | 0.87 ± 0.44 | 0.92 ± 0.48 | 1.07 ± 0.58 | 0.027 |
| E/A ratio ≥ 1.5, n (%) | 6 (7 %) | 31 (9 %) | 14 (19 %) | 0.013 |
| E/e’ ratio | 10.7 ± 3.1 | 11.6 ± 4.0 | 13.5 ± 4.2 | <0.001 |
| E/e’ ratio ≥ 13, n (%) | 23 (25 %) | 102 (28 %) | 41 (53 %) | <0.001 |
| Deceleration time (ms) | 178 ± 41 | 178 ± 44 | 174 ± 51 | 0.74 |
| Deceleration time < 160 ms, n (%) | 29 (32 %) | 115 (32 %) | 35 (48 %) | 0.028 |
| Vp (cm/s) | 58 ± 17 | 56 ± 16 | 52 ± 22 | 0.12 |
| Vp < 45 cm/s, n (%) | 23 (25 %) | 114 (32 %) | 35 (48 %) | 0.006 |
A atrial transmitral peak velocity, E early transmitral peak velocity, e’ early peak mitral annular velocity, LAV left atrial volume, LVEF left ventricular ejection fraction, LVH left ventricular hypertrophy (LV mass index >109 g/m2 in women and >132 g/m2 in men.), RWMA regional wall motion abnormalities, Vp velocity of inflow propagation
Clinical outcomes
Follow-up was 100 % complete. After an average follow-up time of 5.1 ± 0.3 years, there were 236 deaths (42 %), of which 102 (43 %) were of cardiovascular origin. Among the 97 subjects with moderate-to-severe VHD, 57 (59 %) died, of which 33 (58 %) died of cardiovascular causes. Among the subjects with VHD and systolic dysfunction, 19 (59 %) died, of whom 8 (42 %) from cardiovascular causes. As shown in Fig. 1, 5-year overall and cardiovascular survival was significantly lower in subjects with moderate-to-severe VHD than in those with no or mild VHD.
Fig. 1.
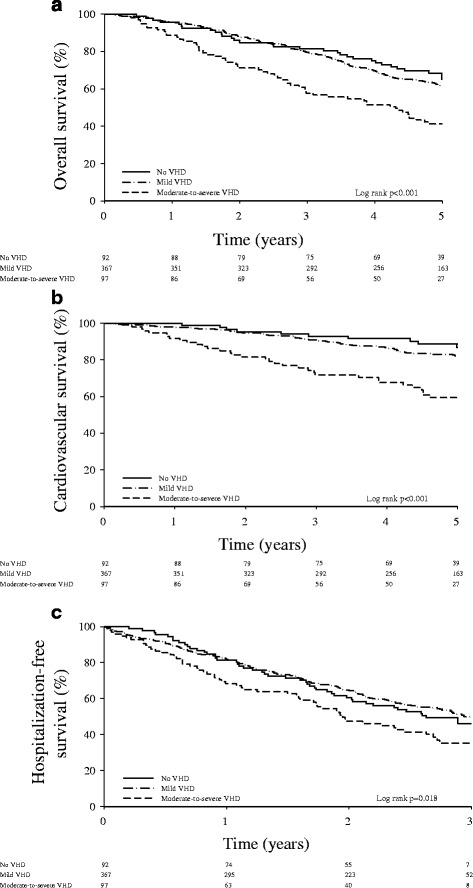
Kaplan Meier survival curves for overall survival (panel a), cardiovascular survival (panel b) and freedom from a first unplanned hospitalization (panel c) in patients with no (solid lines), mild (dotted-dashed lines) and moderate-to-severe (dashed lines), mild and without (solid lines) VHD. Risk of mortality and hospitalization based on the presence of valvular heart disease
After an average follow-up time of 3.0 ± 0.3 years, 278 participants (50 %) needed hospitalization. Hospitalization data were missing for only one participant. As shown in Fig. 1c, the freedom from a first unplanned hospitalization was better in patients with no or mild VHD than in those with moderate-to-severe VHD.
Predictors of all-cause and cardiovascular mortality
As show in Table 4, the multivariable Cox’s regression analysis identified age, moderate-to-severe VHD, CIRS, severe dyspnea, systolic dysfunction and LV hypertrophy as independent predictors of all-cause mortality. A dose-response effect was found for LV mass index (adjusted HR: 1.01, 95 %-CI [1.00–1.01], p = 0.003) but not for LV ejection fraction. No relation was found with parameters of diastolic dysfunction.
Table 4.
Uni- and multivariable predictors of outcome
| Univariable | Multivariable | |||||
|---|---|---|---|---|---|---|
| HR | 95 % CI | p value | HR | 95 % CI | p value | |
| All-cause mortality | ||||||
| Age (year) | 1.10 | 1.07–1.14 | <0.001 | 1.09 | 1.05–1.12 | <0.001 |
| Dyspnea ≥3 | 2.29 | 1.77–2.97 | <0.001 | 1.81 | 1.37–2.39 | <0.001 |
| CIRS (per point increase) | 1.21 | 1.12–1.30 | <0.001 | 1.11 | 1.03–1.21 | 0.007 |
| Moderate-to-severe VHD | 1.91 | 1.42–2.58 | <0.001 | 1.42 | 1.04–1.95 | 0.029 |
| Moderate-to-severe AS | 1.96 | 1.42–2.70 | <0.001 | |||
| LAVI ≥34 mL/m2 | 1.58 | 1.22–2.04 | 0.001 | |||
| LV hypertrophy | 1.01 | 1.00–1.01 | 0.004 | 1.01 | 1.00–1.01 | 0.020 |
| Moderate-to-severe MS | 2.30 | 1.08–4.88 | 0.030 | |||
| LVEF ≤50 % | 1.63 | 1.02–2.61 | 0.040 | 1.66 | 1.03–2.67 | 0.037 |
| Dyslipidemia | 0.78 | 0.60–1.01 | 0.063 | |||
| Cardiovascular mortality | ||||||
| Age (year) | 1.09 | 1.04–1.14 | <0.001 | 1.06 | 1.01–1.11 | 0.014 |
| CIRS (per point increase) | 1.23 | 1.10–1.37 | <0.001 | |||
| Dyspnea ≥3 | 3.06 | 2.07–4.53 | <0.001 | 2.68 | 1.80–3.98 | <0.001 |
| Moderate-to-severe VHD | 2.88 | 1.90–4.37 | <0.001 | 2.13 | 1.38–3.29 | 0.001 |
| Moderate-to-severe AS | 3.06 | 1.99–4.72 | <0.001 | |||
| Moderate-to-severe MS | 4.65 | 2.03–10.63 | <0.001 | |||
| LAVI ≥34 mL/m2 | 1.87 | 1.27–2.77 | 0.002 | |||
| LV hypertrophy | 1.01 | 1.00–1.02 | 0.029 | 1.01 | 1.00–1.01 | 0.087 |
| First unplanned Hospitalization | ||||||
| Smoker (current or ex) | 1.60 | 1.25–2.04 | <0.001 | 1.69 | 1.32–2.16 | <0.001 |
| CIRS (per point increase) | 1.20 | 1.13–1.29 | <0.001 | 1.15 | 1.07–1.23 | <0.001 |
| Dyspnea ≥3 | 1.81 | 1.42–2.31 | <0.001 | 1.50 | 1.16–1.94 | 0.002 |
| Moderate-to-severe AS | 1.71 | 1.25–2.33 | 0.001 | |||
| LAVI ≥34 mL/m2 | 1.37 | 1.08–1.74 | 0.009 | |||
| Moderate-to-severe VHD | 1.51 | 1.13–2.03 | 0.006 | 1.43 | 1.06–1.94 | 0.021 |
| Age (year) | 1.03 | 1.00–1.06 | 0.041 | |||
AS aortic stenosis, CI confidence interval, CIRS cumulative illness rating scale, HR hazard ratio, LAVI left atrial volume index, LVEF left ventricular ejection fraction, MS mitral stenosis, VHD valvular heart disease
Moderate-to-severe VHD was also identified as an independent predictor of cardiovascular mortality (adjusted HR: 2.13; 95 %-CI [1.38–3.29]), together with age, CIRS, LV hypertrophy and severe dyspnea (Table 4). A dose-response effect was found for both LV hypertrophy (adjusted HR: 1.01; 95 %-CI [1.00–1.02], p = 0.029). Diastolic parameters did not show any relationship with cardiovascular mortality.
Predictors of first unplanned hospitalizations
Moderate-to-severe VHD, together with the smoking status, CIRS, and severe dyspnea, was found to be independently associated with the need for a first unplanned hospitalization.
The relationships between moderate-to-severe VHD and all-cause mortality, cardiovascular mortality and the need for a first unplanned hospitalization did not change when echocardiographic parameters were entered as dichotomous or continuous variables, nor when the CIRS was replaced by individual morbidities.
Discussion
Studies investigating the prevalence of VHDs in elderly subjects are rather scarce and often based on in-hospital series [4, 20–22]. Studies describing the clinical impact and outcome consequences of VHDs in very old subjects are even fewer [22], making it difficult to appreciate their real burden in our ageing societies. The current study is the first to investigate the prevalence, clinical impact and outcome consequences of VHDs in a large population-based sample of subjects aged 80 and older. Our results can be summarized as follows:
The prevalence of moderate-to-severe VHD in very old subjects is around 17 %, and is similar in men and women.
There is a significant age-related increase in both the prevalence and the severity of aortic stenosis.
Higher rates of heart failure, atrial fibrillation and stroke were found in subjects with moderate-to-severe VHD than in those without. Accordingly, physical activity and cognitive functioning was negatively affected in patients with moderate-to-severe VHD.
The presence of moderate-to-severe VHD independently increases overall and cardiovascular mortality risks, as well as the need for unplanned hospitalizations.
Prevalence of VHD in very old subjects
The BELFRAIL study is one of the largest prospective observational studies performed so far on the prevalence of VHD in very old subjects. The salient finding of this study is that the prevalence of moderate-to-severe VHD in subjects aged 80 and older is quite high, in the range of 16−18 %. Moderate-to-severe AS was by far the most frequently encountered VHD (14 % of very old subjects), followed by moderate-to-severe degenerative MS (1.7 %), moderate AR (1.6 %) and finally moderate MR (0.7 %). MS was more prevalent in women and an age-dependent increase in the prevalence and severity of AS was observed.
Few previous studies have investigated the prevalence of VHD in elderly subjects. Although these studies demonstrated an age-dependent increase in the prevalence of VHD in the ageing population, very little data are available concerning VHD prevalence among very old subjects, i.e. those aged 80 years and older. By using data from 3 large north-American population-based studies [23–25] as well as from the Olmsted county community study, Nkomo et al. reported a prevalence of moderate-to-severe VHD in Americans aged 75 years and older of 11.7 to 13.2 % [4]. Interestingly, most of their patients presented with moderate-to-severe MR (9.3 % in the population-based studies, 7.1 % in the Olmsted County community study) whereas fewer patients presented with moderate-to-severe AS (2.8 % in the population-based studies, 4.6 % in in the Olmsted County community study). Although the results of our study are roughly in line with those of Nkomo’s study, they nonetheless differ with regard to the relative prevalence of MR and AS, MR being more prevalent in these earlier studies than in ours. Our results also differ from those of the Leyden 85+ study, in which the prevalence of moderate-to-severe VHD among subjects aged 90 and older was found to be close to 50 %, the majority of the subjects presenting with moderate to severe MR, and only 6 % with moderate-to-severe AS [22]. The reasons for these differences are unclear but may be related to the methods used to assess of MR severity. Most previous studies, including that from Nkomo et al., used the semi-quantitative method described by Helmcke et al [26] to make this assessment. While this approach works reasonably well in patients with central jets, it is notoriously inaccurate in those with impinging wall jets due to mitral valve prolapse [27]. In the present study, we used an integrated approach that included both qualitative and quantitative parameters, in order to minimize the natural tendency of echocardiographic methods to overestimate the true severity of MR [28].
Clinical burden of VHD in very old subjects
Another important objective of our study was to investigate the clinical and echocardiographic characteristics of very old subjects presenting with VHD. Our findings indicate that patients with moderate-to-severe VHD more often present with heart failure symptoms, such as dyspnea or peripheral edema; more frequently have a prior history of heart failure and stroke; and more frequently present with atrial fibrillation. This negatively affected their physical activity and cognitive functioning as measured by the ADL and GDS-15 scores. They were also more likely to exhibit increased LA volume and LV mass and to demonstrate echocardiographic features associated with altered LV diastolic properties and elevated filling pressures.
Our data also indicate that the VHD detected in our study were not simply benign imaging observations but had profound outcome consequences, as they were associated with a 40 % increase in adjusted overall mortality and a 2.1-fold excess in adjusted cardiovascular mortality. Patients with moderate-to-severe VHD were also hospitalized more frequently than patients without. Our observations confirm and extend those made by Nkomo et al. as they demonstrate that in elderly patients as well, moderate-to-severe VHDs are a major and independent determinant of outcome. Our results also concur with those of studies that specifically addressed the impact of aortic stenosis on the outcome of elderly patients [29, 30].
The excess risk associated with VHD stresses the importance of increasing the awareness of the medical community on the dismal outcome consequences of VHDs and on the need to detect them early. Early detection of VHD, before the onset of symptoms and at a time when patients are still sufficiently fit to be proposed surgical valve replacement is probably key to improving their prognosis. Nkomo et al. have indeed shown that in the community, VHDs are frequently underdiagnosed, owing probably to the need for echocardiography to be clinically indicated before diagnosis is made [4]. Whereas delaying diagnosis likely has little impact on outcome in younger individuals, it exposes elderly patients to be denied appropriate treatment because of their advanced age. The EuroHeart survey has indeed clearly demonstrated that old patients are frequently denied interventions despite unequivocal guideline-based indications, because of their advanced age [10, 11].
Study limitations
This study has limitations that should be acknowledged. First, although many factors potentially associated with VHDs were considered, we cannot exclude the possibility that some yet unknown confounders contributed to our results. Second, comorbidities may have been underdiagnosed, as their identification relied only on the information gathered by the general practitioner.
Conclusions
In this large representative population-based sample of subjects aged 80 and older a high prevalence of VHD was found. Patients with VHD more frequently presented with heart failure symptoms, atrial fibrillation and stroke than those without. They were also found to be at higher risk for all-cause and cardiovascular mortality as well as unplanned hospitalizations.
Acknowledgements
This study was made possible by the participating GPs.
The authors would also like to thank Pauline Boeckxstaens and Olivia Dalleur for encoding the problem lists of the BELFRAIL participants.
Funding
The BELFRAIL study [B40320084685] was supported by an unconditional grant from the Fondation Louvain. The Fondation Louvain is the support unit of the Université Catholique de Louvain, which is in charge of developing education and research projects at the university by collecting gifts from corporation, foundations and alumni.
Footnotes
Competing interests
The authors declare they have no competing interests.
Authors’ contributions
JD and BV designed the BELFRAIL study. NR, BV, CdM and JLV analysed the data and drafted the first version of the manuscript. NR, BV, JD, GV, CM, WA and AP collected the data and commented the manuscript. All authors read and approved the final manuscript.
Contributor Information
Nawel Rezzoug, Email: reznawel@yahoo.fr.
Bert Vaes, Email: bert.vaes@med.kuleuven.be.
Christophe de Meester, Email: christophe.demeester@uclouvain.be.
Jan Degryse, Email: Jan.Degryse@med.kuleuven.be.
Gijs Van Pottelbergh, Email: Gijs.VanPottelbergh@med.kuleuven.be.
Catharina Mathei, Email: Catharina.Mathei@med.kuleuven.be.
Wim Adriaensen, Email: Wim.Adriaensen@med.kuleuven.be.
Agnes Pasquet, Email: Agnes.Pasquet@uclouvain.be.
Jean-Louis Vanoverschelde, Email: Jean-Louis.Vanoverschelde@uclouvain.be.
References
- 1.European Commission Eurostat. Europe in figures. 2009. Report No.: Eurostat yearbook.
- 2.United Nations.Department of Economic and Social Affairs Pd. World Population Prospects: The 2008 Revision, highlights. New York; 2009. Report No.: Working Paper no ESE/P/WP202.
- 3.Abhayaratna WP, Smith WT, Becker NG, Marwick TH, Jeffery IM, McGill DA. Prevalence of heart failure and systolic ventricular dysfunction in older Australians: the Canberra Heart Study. Med J Aust. 2006;184:151–4. doi: 10.5694/j.1326-5377.2006.tb00173.x. [DOI] [PubMed] [Google Scholar]
- 4.Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368:1005–11. doi: 10.1016/S0140-6736(06)69208-8. [DOI] [PubMed] [Google Scholar]
- 5.Redfield MM, Jacobsen SJ, Burnett JC, Jr, Mahoney DW, Bailey KR, Rodeheffer RJ. Burden of systolic and diastolic ventricular dysfunction in the community: appreciating the scope of the heart failure epidemic. JAMA. 2003;289:194–202. doi: 10.1001/jama.289.2.194. [DOI] [PubMed] [Google Scholar]
- 6.Vaes B, Rezzoug N, Pasquet A, Wallemacq P, Van Pottelbergh G, Mathei C, et al. The prevalence of cardiac dysfunction and the correlation with poor functioning among the very elderly. Int J Cardiol. 2012;155:134–43. doi: 10.1016/j.ijcard.2011.07.024. [DOI] [PubMed] [Google Scholar]
- 7.Gerstenblith G, Frederiksen J, Yin FC, Fortuin NJ, Lakatta EG, Weisfeldt ML. Echocardiographic assessment of a normal adult aging population. Circulation. 1977;56:273–8. doi: 10.1161/01.CIR.56.2.273. [DOI] [PubMed] [Google Scholar]
- 8.Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, Guyton RA, et al. 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63:e57–185. doi: 10.1016/j.jacc.2014.02.536. [DOI] [PubMed] [Google Scholar]
- 9.Iung B, Cachier A, Baron G, Messika-Zeitoun D, Delahaye F, Tornos P, et al. Decision-making in elderly patients with severe aortic stenosis: why are so many denied surgery? Eur Heart J. 2005;26:2714–20. doi: 10.1093/eurheartj/ehi471. [DOI] [PubMed] [Google Scholar]
- 10.Mirabel M, Iung B, Baron G, Messika-Zeitoun D, Detaint D, Vanoverschelde J-L, et al. What are the characteristics of patients with severe, symptomatic, mitral regurgitation who are denied surgery? Eur Heart J. 2007;28:1358–65. doi: 10.1093/eurheartj/ehm001. [DOI] [PubMed] [Google Scholar]
- 11.Piérard S, de Meester C, Seldrum S, Pasquet A, Gerber B, Vancraeynest D, et al. Impact of preoperative symptoms on postoperative survival in severe aortic stenosis: Implications for the timing of surgery. Ann Thorac Surg. 2014;97:803–9. doi: 10.1016/j.athoracsur.2013.08.059. [DOI] [PubMed] [Google Scholar]
- 12.Vaes B, Pasquet A, Wallemacq P, Rezzoug N, Mekouar H, Olivier PA, et al. The BELFRAIL (BFC80+) study: a population-based prospective cohort study of the very elderly in Belgium. BMC Geriatr. 2010;10:39. doi: 10.1186/1471-2318-10-39. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Fletcher CM. Standardised questionnaire on respiratory symptoms: a statement prepared and approved by the MRC Committee on the Aetiology of Chronic Bronchitis (MRC breathlessness score) BMJ. 1960;2:1665. [Google Scholar]
- 14.Hudon C, Fortin M, Soubhi H. Abbreviated guidelines for scoring the cumulative illness rating scale (CIRS) in family practice. J Clin Epidemiol. 2007;60:212e1–4. doi: 10.1016/j.jclinepi.2005.12.021. [DOI] [PubMed] [Google Scholar]
- 15.Boeckxstaens P, Vaes B, Legrand D, Dalleur O, De Sutter A, Degryse J. The relationship of multimorbidity with disability and frailty in the oldest patients: A cross-sectional analysis of three measures of multimorbidity in the BELFRAIL cohort. Eur J Gen Pract. 2015;21:39–44. doi: 10.3109/13814788.2014.914167. [DOI] [PubMed] [Google Scholar]
- 16.Lang RM, Bierig M, Devereux RB, Flachskampf FA, Foster E, Pellikka PA, et al. Recommendations for chamber quantification. J Am Soc Echocardiogr. 2008;21:1179–201. doi: 10.1016/j.echo.2008.09.009. [DOI] [PubMed] [Google Scholar]
- 17.Baumgartner H, Hung J, Bermejo J, Chambers JB, Evangelista A, Griffin BP, et al. Echocardiographic assessment of valve stenosis: EAE/ASE recommendations for clinical practice. Eur J Echocardiogr. 2009;10:1–25. doi: 10.1093/ejechocard/jen303. [DOI] [PubMed] [Google Scholar]
- 18.Lancellotti P, Tribouilloy C, Hagendorff A, Moura L, Popescu BA, Agricola E, et al. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 1: aortic and pulmonary regurgitation (native valve disease) Eur J Echocardiogr. 2010;11:223–44. doi: 10.1093/ejechocard/jeq030. [DOI] [PubMed] [Google Scholar]
- 19.Lancellotti P, Moura L, Pierard L, Agricola E, Popescu BA, Tribouilloy C, et al. European Association of Echocardiography recommendations for the assessment of valvular regurgitation. Part 2: mitral and tricuspid regurgitation (native valve disease) Eur J Echocardiogr. 2010;11:307–32. doi: 10.1093/ejechocard/jeq031. [DOI] [PubMed] [Google Scholar]
- 20.Iung B, Baron G, Butchaet EG, Delahaye F, Gohlke-Bärwolf C, Levan OW, et al. A prospective survey of patients with valvular heart disease in Europe: the Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003;24:1231–43. doi: 10.1016/S0195-668X(03)00201-X. [DOI] [PubMed] [Google Scholar]
- 21.Lindroos M, Kupari M, Heikkila J, Tilvis R. Prevalence of aortic valve abnormalities in the elderly: an echocardiographic study of a random population sample. J Am Coll Cardiol. 1993;21:1220–5. doi: 10.1016/0735-1097(93)90249-Z. [DOI] [PubMed] [Google Scholar]
- 22.van Bemmel T, Delgado V, Bax JJ, Gussekloo J, Blauw GJ, Westendorp RG, et al. Impact of valvular heart disease on activities of daily living of nonagenarians: the Leiden 85-plus study a population based study. BMC Geriatr. 2010;10:17. doi: 10.1186/1471-2318-10-17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Fox ER, Wilson RS, Penman AD, King JJ, Towery JG, Butler KR, et al. Epidemiology of pure valvular regurgitation in the large middle-aged African American cohort of the Atherosclerosis Risk in Communities study. Am Heart J. 2007;154:1229–34. doi: 10.1016/j.ahj.2007.07.030. [DOI] [PubMed] [Google Scholar]
- 24.Reid CL, Anton-Culver H, Yunis C, Gardin JM. Prevalence and clinical correlates of isolated mitral, isolated aortic regurgitation, and both in adults aged 21 to 35 years (from the CARDIA study) Am J Cardiol. 2007;99:830–4. doi: 10.1016/j.amjcard.2006.10.048. [DOI] [PubMed] [Google Scholar]
- 25.Fried LP, Borhani NO, Enright P, Furberg C, Gardin JM, Kronmal R, et al. The Cardiovascular Health Study: design and rationale. Ann Epidemiol. 1991;1:263–76. doi: 10.1016/1047-2797(91)90005-W. [DOI] [PubMed] [Google Scholar]
- 26.Helmcke F, Nanda NC, Hsiung MC, Soto B, Adey CK, Goyal RG, et al. Color Doppler assessment of mitral regurgitation with orthogonal planes. Circulation. 1987;75:175–83. doi: 10.1161/01.CIR.75.1.175. [DOI] [PubMed] [Google Scholar]
- 27.Chen C, Thomas JD, Anconina J, Harrigan P, Mueller L, Picard MH, et al. Impact of impinging wall jet on color Doppler quantification of mitral regurgitation. Circulation. 1991;84:712–20. doi: 10.1161/01.CIR.84.2.712. [DOI] [PubMed] [Google Scholar]
- 28.Topilsky Y, Michelena H, Bichara V, Maalouf J, Mahoney DW, Enriquez-Sarano M. Mitral valve prolapse with mid-late systolic mitral regurgitation: pitfalls of evaluation and clinical outcome compared with holosystolic regurgitation. Circulation. 2012;125:1643–51. doi: 10.1161/CIRCULATIONAHA.111.055111. [DOI] [PubMed] [Google Scholar]
- 29.Leibowitz D, Stessman J, Jacobs JM, Stessman-Lande I, Gilon D. Prevalence and prognosis of aortic valve disease in subjects older than 85 years of age. Am J Cardiol. 2013;112:395–9. doi: 10.1016/j.amjcard.2013.03.044. [DOI] [PubMed] [Google Scholar]
- 30.Otto CM, Lind BK, Kitzman DW, Gersh BJ, Siscovick DS. Association of aortic-valve sclerosis with cardiovascular mortality and morbidity in the elderly. N Engl J Med. 1999;341:142–7. doi: 10.1056/NEJM199907153410302. [DOI] [PubMed] [Google Scholar]