

Abstract
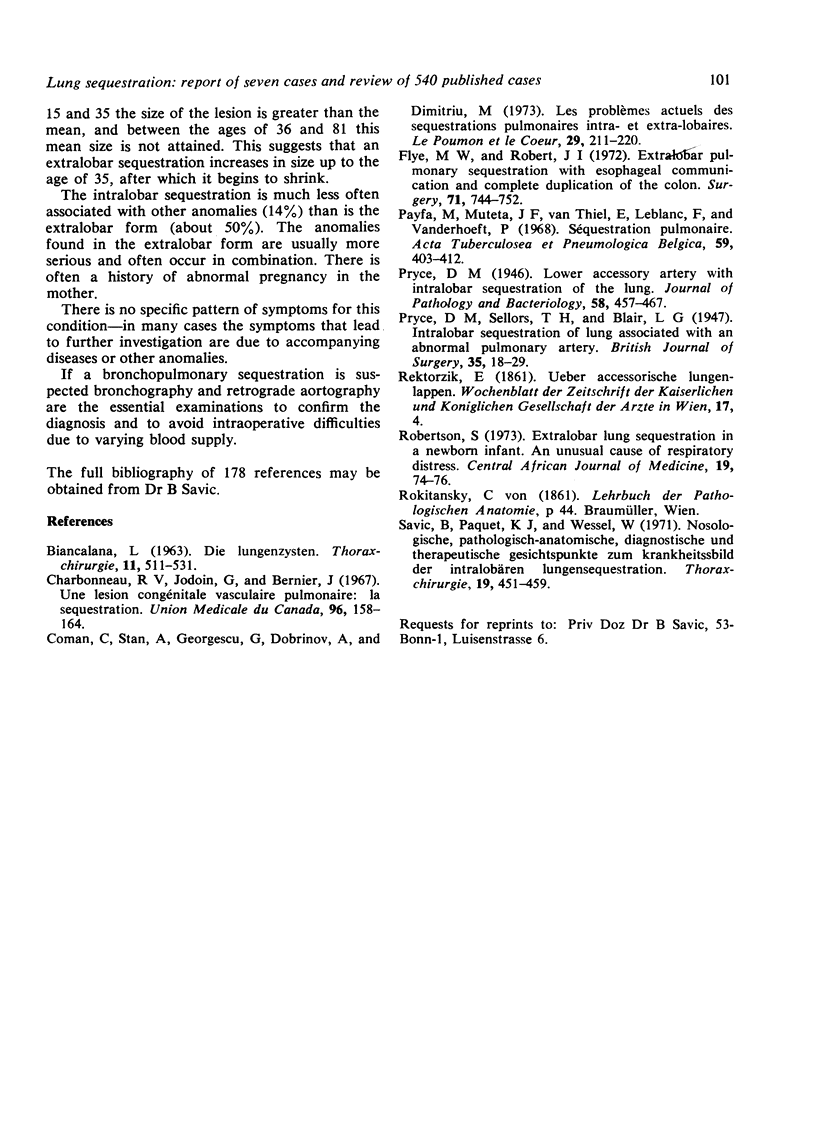
We present an analysis of 400 intralobar and 133 extralobar sequestrations, six cases presenting intra- and extralobar sequestration simultaneously, five sequestrations of one whole lung, and two bilateral intralobar sequestrations.
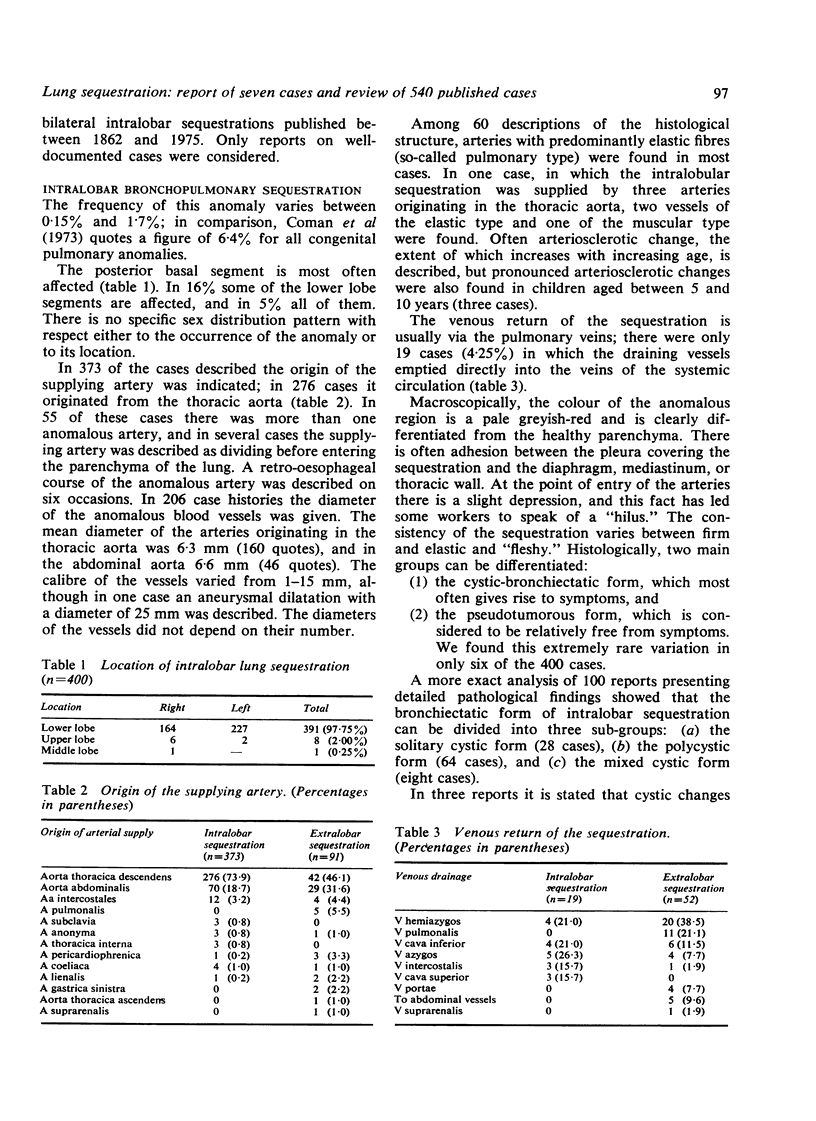
This anomaly comprises 0·15-6·4% of all congenital pulmonary malformations. Usually the posterior basal segment is affected.
The aberrant artery in intralobar sequestration originated in 74% of all cases from the thoracic aorta, and in 14·8% there was more than one anomalous artery. The mean diameter of the aberrant arteries was 6·3-6·6 mm. Usually arteries with predominantly elastic fibres were found. Arteriosclerotic changes were common, even in children.
The venous return of the intralobar sequestration is, in 95·7% of all cases, via the pulmonary veins.
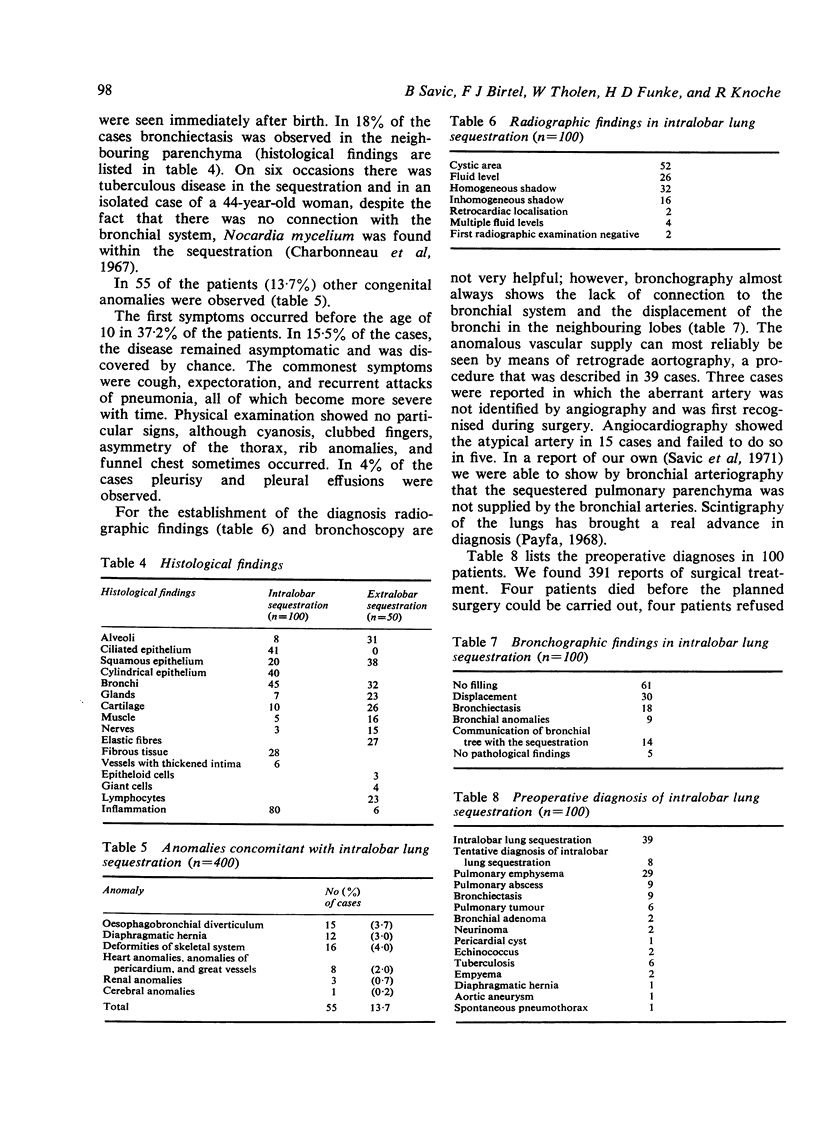
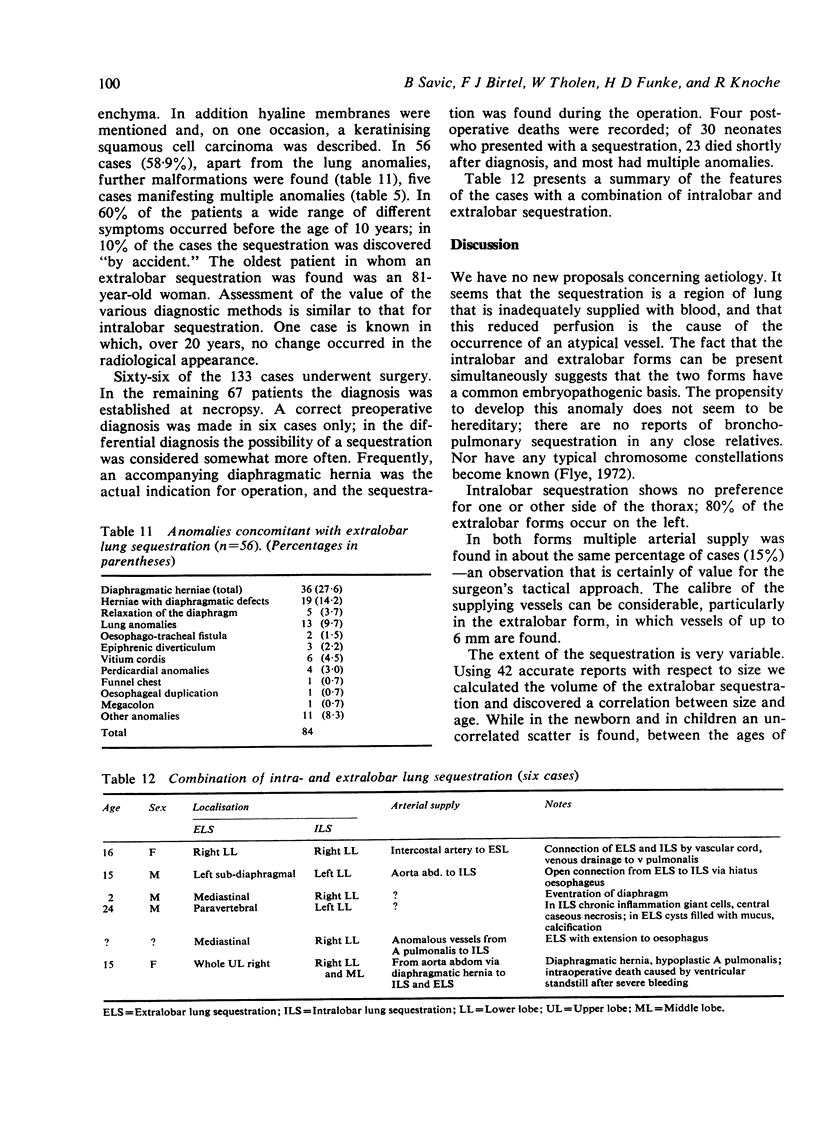
In 13·7% of all cases other congenital malformations were observed. Symptoms arose within the first decade of life in 37·2%
Bronchography and retrograde arteriography are the mainstay of diagnosis. Sequestrations are not supplied by a bronchial artery.
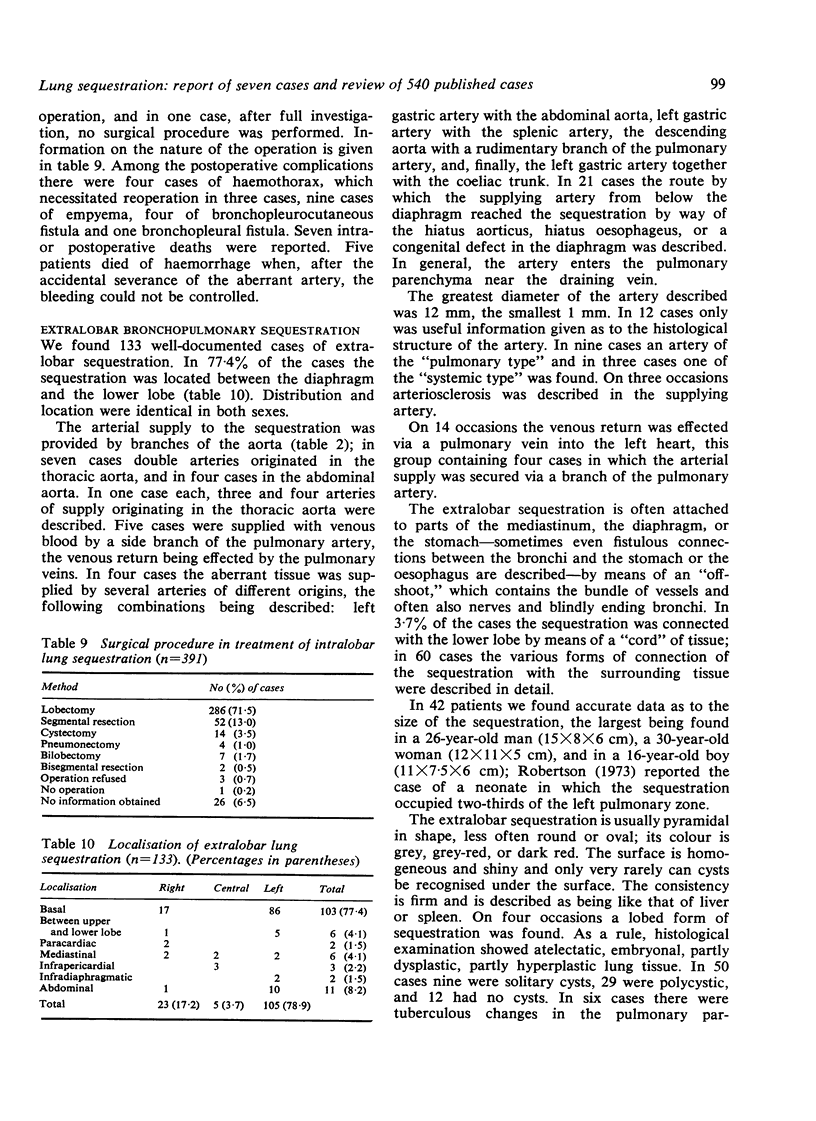
Treatment of choice is operation as early as possible. Altogether seven operative deaths were reported, five of which were due to haemorrhage during operation.
Of the 133 extralobar sequestrations, 77·4% were located between diaphragm and lower lobe. The arterial supply was provided by branches of the aorta. Some cases were supplied with venous blood by branches of the pulmonary artery. In six cases secondary changes, such as tuberculosis or carcinoma were found. In 60% of all the patients symptoms occurred within the first decade of life. Preoperative diagnosis was correct in only six cases. There were four postoperative deaths.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BIANCALANA L. DIE LUNGENZYSTEN. Thoraxchir Vask Chir. 1964 Apr;11:511–531. [PubMed] [Google Scholar]
- Charbonneau R., Jodoin G., Bernier J. Une lésion congénitale vasculaire pulmonaire: la séquestration. Observation d'un cas typique. Union Med Can. 1967 Feb;96(2):158–164. [PubMed] [Google Scholar]
- Coman C., Stan A., Georgescu G., Dobrinov H., Dimitriu M. Les problemes actuels des sequestrations pulmonaires intra et extra-lobaires. Poumon Coeur. 1973 Feb;29(2):211–220. [PubMed] [Google Scholar]
- Flye M. W., Izant R. J. Extralobar pulmonary sequestration with esophageal communication and complete duplication of the colon. Surgery. 1972 May;71(5):744–752. [PubMed] [Google Scholar]
- Payfa M., Muteta I. F., Van Thiel E., Leblanc G., Vanderhoeft P. Séquestration pulmonarie. Acta Tuberc Pneumol Belg. 1968 Mar-Jun;59(2):403–412. [PubMed] [Google Scholar]
- Robertson S. Extralobar lung sequestration in a newborn infant. An unusual cause of respiratory distress. Cent Afr J Med. 1973 Apr;19(4):74–76. [PubMed] [Google Scholar]
- Savic B., Paquet K. J., Wessel W. Nosologische, pathologische-anatomische, diagnostische und therapeutische Gesichtspunkte zum Krankheitsbild der intralobären Lungensequestration. Thoraxchir Vask Chir. 1971 Dec;19(6):451–459. [PubMed] [Google Scholar]