

Abstract
Alterations in resting autonomic tone can be pathogenic in many cardiovascular disease states, such as heart failure and hypertension. Indeed, autonomic modulation by way of beta-blockade is a standard treatment of these conditions. There is a significant interest in developing non-pharmacological methods of autonomic modulation as well. For instance, clinical trials of vagal stimulation and spinal cord stimulation in the treatment of heart failure are currently underway, and renal denervation has been studied recently in the treatment of resistant hypertension. Notably, autonomic stimulation is also a potent modulator of cardiac electrophysiology. Manipulating the autonomic nervous system in studies designed to treat heart failure and hypertension have revealed that autonomic modulation may have a role in the treatment of common atrial and ventricular arrhythmias as well. Experimental data on vagal nerve and spinal cord stimulation suggest that each technique may reduce ventricular arrhythmias. Similarly, renal denervation may play a role in the treatment of atrial fibrillation, as well as in controlling refractory ventricular arrhythmias. In this review, we present the current experimental and clinical data on the effect of these therapeutic modalities on cardiac electrophysiology and their potential role in arrhythmia management.
Keywords: Autonomic stimulation, spinal cord stimulation, renal denervation, vagal stimulation, arrhythmias
The interplay between the central nervous system and cardiac electrophysiology is fundamental, and becomes obvious each time one’s pulse quickens in response to stress. Normally, cardiac neurohormonal regulation is accomplished through the balanced effects of sympathetic and parasympathetic autonomic stimulation, along with the hormonal regulation of the renin-angiotensin-aldosterone system (RAAS). Autonomic and hormonal input modulate multiple facets of cellular electrophysiology – action potential duration, ion channel kinetics and intracellular calcium dynamics (just to name a few) – which translate into macroscopic manifestations of autonomic modulation such as heart rate variability, atrioventricular (AV) conduction time and QT interval variability.1 Therefore, it is no surprise that neurohormonal regulation of cardiac electrophysiology is an area of active investigation for its potential antiarrhythmic effects. Recent reviews have focused on the efficacy of neurohormonal modulation, via non-pharmacological methods, to enhance heart failure treatment.2,3
This review will attempt to provide a state-of-the-art on the potential antiarrhythmic efficacy of renal artery denervation, spinal cord stimulation and direct vagal stimulation.
Neurohormonal Control in the Normal and Failing Heart
Autonomic control of cardiac physiology is often conceptualised as parasympathetic (cholinergic) and sympathetic (adrenergic) innervation existing in a ‘yin and yang’ balance under normal circumstances; however, this concept may be over-simplified.4 In reality, the intrinsic cardiac nervous system, composed of several ganglia located primarily posterior to the atria, likely acts as a ‘little brain’ of the heart – it provides efferent input to the myocardium, collects afferent signals on a beat-to-beat basis and performs some integrative functions on its own, all under the tonic modulation of extrinsic sympathetic and parasympathetic input (see Figure 1).4–8
Figure 1: Schematic of Cardiovascular Autonomic Control.
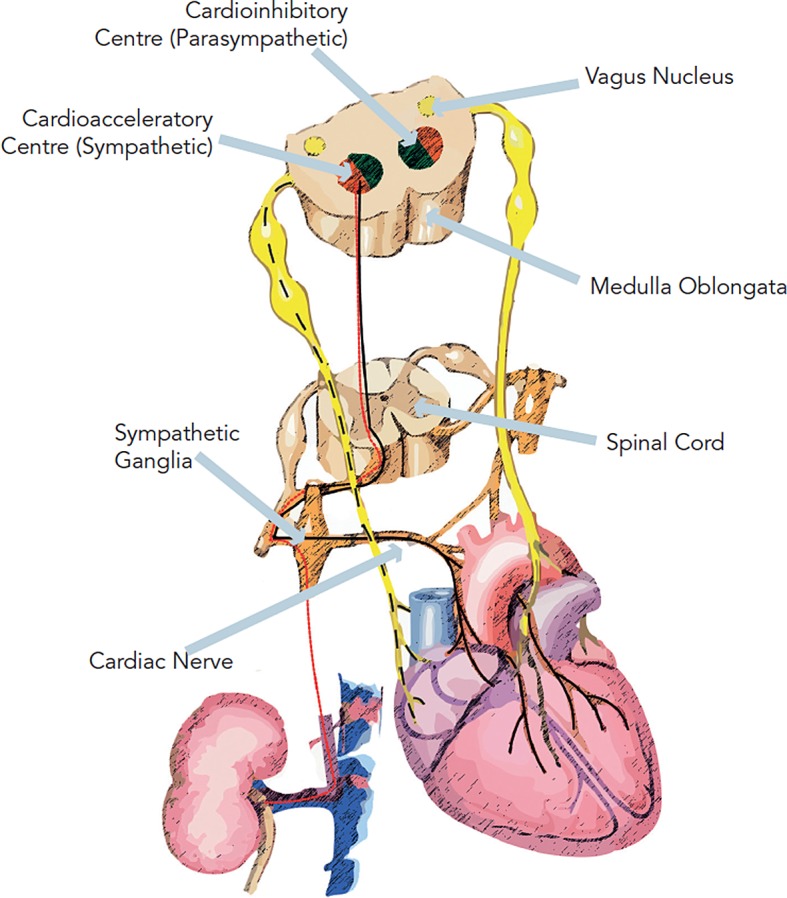
Parasympathetic innervation exits the medullary centres via the vagus nerve, which then synapses with the intracardiac nervous system before providing post-ganglionic fibres to the myocardium. Sympathetic innervation exits the medulla and enters the spinal cord before exiting and traveling to the ganglia within the sympathetic chain. Post-ganglionic fibres travel along the major vessels prior to entering the myocardium. Sympathetic innervation also continues along the major vessels to the kidneys, supplying renal sympathetic innervation.
The ganglia are predominantly composed of cholinergic neurons; however, sympathetic efferent neurons are also present. Due to the complex interconnectivity between the ganglia, afferent mechanosensory, nociceptive and chemosensory signals from all four chambers of the heart may be processed within a single ganglion.4 Such interconnectivity implies that predicting the effect of stimulation or ablation of a particular ganglion may be difficult, because each ganglion performs multiple functions.7,9
The intrinsic cardiac nervous system is constantly modulated by central autonomic tone via the extrinsic cardiac nervous system.10 Cardiac sympathetic innervation arises from the superior cervical ganglion, stellate ganglion and thoracic ganglia, which communicate with C1–3, C7–T2 and T1–T5, respectively.4,11,12 Preganglionic parasympathetic innervation exits the medulla via the vagus nerve, which then provides several small branches to the intrinsic cardiac nervous system. Parasympathetic innervation is concentrated around the sinoatrial (SA) and AV nodes, with greater vagal innervation of the atria than the ventricles.
In heart failure, the balance of cardiac parasympathetic and sympathetic tone is significantly altered leading to sympathetic hyperactivity.13 Decreased cardiac output and myocardial ischaemia stimulate the arterial baroreflex, arterial chemoreflex and the cardiac sympathetic afferent reflex while attenuating afferent cardiac vagal reflexes leading to an overall increased sympathetic tone, peripheral vasoconstriction and sodium retention.14–18 Over time, chronic sympathetic hyperactivity is maladaptive in the heart, leading to decreased contractility through beta-receptor downregulation, increased cardiomyocyte apoptosis and myocardial fibrosis.14 Current cornerstones of pharmacological heart failure management are based on neurohormonal blockade, with a mortality benefit conveyed by beta-blockers,19–21 angiotensin-converting enzyme (ACE) inhibitors22 and aldosterone antagonists.23
Due to the growing need to improve heart failure therapies, there are now non-pharmacological approaches to re-establish autonomic balance that are currently under investigation, such as vagal stimulation and spinal cord stimulation.3 Similarly, renal denervation is an emerging technique to treat resistant hypertension, and may have a role in treating heart failure as well. Arrhythmias are common co-morbidities in patients with heart failure and resistant hypertension, therefore trials designed to investigate non-pharmacological autonomic modulation in these populations will likely provide significant insight into the possibility of employing autonomic modulation as an antiarrhythmic strategy.
Device-Based Approaches to Modulate the Autonomic Nervous System
Renal Denervation
Renal Denervation and Atrial Electrophysiology
Recently, renal denervation (RDN) has become an increasingly studied method to control resistant hypertension.24 RDN is performed through endovascular ablation of several locations within the renal arteries, disrupting sympathetic renal efferent innervation. Reducing renal efferent input also decreases renal afferent output and is associated with reduced serum norepinephrine levels25–27 and decreased central sympathetic tone.28 Therefore, RDN is likely to influence cardiac electrophysiology through modulation of central adrenergic tone, and may have a role in antiarrhythmic therapy.29,30
Preclinical work in dogs and pigs have indicated that RDN affects heart rate variability,26 resting heart rate, heart rate during atrial fibrillation (AF), AV conduction time, and decreases AF incidence in a model of obstructive sleep apnoea.31,32 RDN does not appear to effect the atrial refractory period.33 RDN has also been shown to prevent structural and electrical remodeling in a canine model of chronic rapid atrial pacing.34
In humans, resting heart rate was decreased, and the PR interval was increased following RDN;35 indicating that RDN can affect autonomic modulation of cardiac conduction in patients. The direct effect of RDN on atrial arrhythmias was recently investigated in a small trial of patients with a history of drug resistant hypertension and paroxysmal AF that were randomised to either pulmonary vein isolation (PVI) or PVI with RDN.36 In the RDN group, both the systolic and diastolic blood pressures were significantly decreased as compared with the PVI group. Echocardiographic data also revealed a decrease in left ventricular (LV) thickness – substantiated in other studies as well.37,38 In this setting, the freedom from AF was 69 % at one-year in the RDN group, versus 29 % in the PVI only group.36 However, because there was also a substantial decrease in blood pressure in the denervation group, these results beg the question: did blood pressure control alone account for the decrease in AF, or was it also influenced by decreased afferent renal sympathetic output?
Hypertension alone has been shown to cause atrial remodeling and is a significant reversible risk factor for AF.39 Therefore, removing the hypertensive stimulus for remodeling may be responsible for the decrease in AF, and not necessarily autonomic modulation. However, if it were solely the effect of hypertension, similar improvement in AF rates would have presumably been seen in prior large trials of hypertension treatment.40 While the blood pressure decrease seen in recent RDN trials has been larger than seen previously in trials of drug therapy for hypertension (which may potentiate its effect on AF), the true efficacy of RDN for hypertension management has been brought into question with the recent announcement that the Renal Denervation in Patients With Uncontrolled Hypertension (Symplicity HTN-3) trial (clinicaltrials. gov; Identifier: NCT01418261) did not meet its primary efficacy endpoint. Once published, the data from this trial will have to be examined carefully to determine if RDN affected the rates of atrial arrhythmias in the absence of a significant decrease in blood pressure.
Renal Denervation and Ventricular Electrophysiology
Thus far, less is known about the impact of RDN on ventricular arrhythmias. Adrenergic stimulation is arrhythmogenic in the ventricles, with cardiac sympathetic denervation used as a possible treatment for refractory ventricular arrhythmias.41 RDN has been shown to decrease serum norepinephrine, aldosterone and central sympathetic tone.28 Therefore it is certainly possible that RDN may also reduce ventricular ectopy and arrhythmias through its ability to decrease central sympathetic tone. Recently a small study of RDN coupled with myocardial ischaemia demonstrated that RDN in pigs reduced premature ventricular contraction (PVC) burden and ventricular fibrillation (VF) induced by ischaemia.42
In humans, case reports of RDN used in patients with ventricular tachycardia (VT) storm, demonstrated a decrease in ventricular arrhythmias.43–45 Presumably, the mechanism is via decreased sympathetic tone; however, the true mechanisms will have to be elucidated in larger studies. Importantly, large clinical trials have demonstrated that aldosterone blockade is associated with decreased rates of sudden cardiac death after myocardial infarction (MI).23,46 Therefore, it may be that decreased renin and aldosterone secretion after RDN34,47 may influence its antiarrhythmic effect instead of (or in addition to) any change it causes in adrenergic activation.
Potential Adverse Effects of Renal Denervation
The number of studies investigating RDN is increasing significantly. Thus far, there have not been significant complications reported. In a three-year follow-up of the Renal Denervation in Patients with Refractory Hypertension (Symplicity HTN-1) trial, one patient was noted to develop renal artery stenosis.48 At one-year, patients in the Renal Denervation in Patients With Uncontrolled Hypertension (Symplicity HTN-2) trial had stable renal function and only one renal artery dissection was reported at the time of denervation.49 There has also been concern about the possibility of RDN causing orthostatic hypotension. This was investigated in a small study of 36 patients who had undergone RDN, where no increase in orthostasis or syncope was found with tilt table testing.50 Recently, announcements regarding the Symplicity HTN-3 trial indicated that the trial met its safety endpoint and did not raise any significant safety concerns.
Spinal Cord Stimulation
Spinal Cord Stimulation and Atrial Electrophysiology
Spinal cord stimulation (SCS) has been used for decades in the treatment of refractory angina, epilepsy and for chronic pain.51 The precise mechanism underlying its beneficial effect in angina is debated; however, experimental studies suggest that spinal cord stimulation likely modulates preganglionic sympathetic input to the intrinsic cardiac nervous system, decreases afferent sensory output from intrinsic cardiac nerves during ischaemia, and stabilises the activity of the intrinsic cardiac nervous system during an ischaemic challenge.3,4,52,53
SCS may have an antiarrhythmic role as well. SCS in dogs applied at the T1–T2 level prolonged sinus cycle length and increased AH interval conduction time, which was abolished by vagotomy, suggesting that SCS at T1–T2 has a predominantly vagal effect.54 However, a recent study by Bernstein et al.55 applied SCS to a canine model of AF induced by rapid atrial pacing, and showed that SCS prolonged the atrial effective refractory periods in both atria and reduced AF inducibility if SCS was applied at the time that rapid atrial pacing began. These changes would suggest a predominantly sympathetic effect of SCS in the atria. However, one important difference in this study as compared with the Olgin et al.54 study is that Bernstein et al.55 applied SCS from T1–T5 whereas Olgin et al. applied SCS to T1–T2. Therefore, it is possible that different populations of nerves were recruited with SCS in the two studies, which could have influenced the net effect of SCS stimulation. Nevertheless, their results suggest that spinal cord stimulation reduced the burden of AF and may be a useful strategy in the treatment of AF. Similarly, Cardinal et al.56 demonstrated that brady-and tachy-arrhythmias that were induced by excessive activation of the intrinsic cardiac nervous system were reduced by SCS.
Spinal Cord Stimulation and Ventricular Electrophysiology
The beneficial effect of SCS on refractory angina and its predominantly sympatholytic effect54 suggests the possibility that SCS may decrease ventricular arrhythmias as well.57 Issa et al.58 observed a significant decrease in VT and VF in a canine heart failure model that was exposed to transient ischaemia. In this model, SCS reduced VT/VF incidence from 59 % to 23 % in the setting of acute ischaemia. Similarly, in a pig model of acute ischaemia, Odenstedt et al.59 observed a significant decrease in sustained and non-sustained VT in pigs receiving SCS. This study also demonstrated a reduction in spatial repolarization gradients with SCS. Similar effects were observed following chronic SCS by Lopshire et al.,60 in which case chronic SCS not only improved LV function in a canine model of ischaemic cardiomyopathy, but also decreased ventricular tachyarrhythmias, over and above the effect seen from standard medical therapy for heart failure.
The mechanism behind the antiarrhythmic effect of SCS is not completely understood and is likely multifactorial, involving modulation of the activity within the intrinsic cardiac nervous system, as well as altering the sympathetic and vagal efferents to the heart.53,60 In addition, inhibition of the cardiocardiac reflex may also contribute to the antiarrhythmic effect of SCS. In the setting of ischaemia, Foreman et al.53 demonstrated that SCS decreased afferent output from the intrinsic cardiac nervous system. In rats, disrupting the T1–T5 dorsal root ganglia to interrupt this reflex arc decreased the time to onset of ventricular arrhythmias.61 Clinically, disrupting cardiac sympathetic innervation either through epidural anaesthesia or through cardiac sympathetic denervation has been used to treat patients with refractory ventricular arrhythmias.62
Myocardial infarction interrupts autonomic innervation in the area of the infarct, with the subsequent development of sympathetic hypersensitivity, nerve sprouting and heterogeneous gradients of sympathetic innervation around the infarct.57,63 Interestingly, Zhou et al.64 demonstrated that in ambulatory dogs with ischaemic cardiomyopathy, ventricular tachyarrhythmias were predominantly preceded by bursts of sympathetic nerve activity in the stellate ganglia. Therefore, it is plausible that sympathetic input enhances the heterogeneity of conduction in the diseased myocardium due to gradients in sympathetic innervation creating a ventricular substrate that is more arrhythmogenic. SCS may mitigate this effect by decreasing sympathetic efferent signaling to the myocardium, thereby preventing the enhancement of heterogeneous conduction and decreasing the likelihood for a ventricular arrhythmia to arise. In support of this hypothesis, a report of three patients that received an implantable cardioverter defibrillator (ICD) and a spinal stimulator demonstrated a reduction in T-wave alternans when SCS was active, suggesting that SCS may reduce temporal repolarization gradients and stabilise the ventricular electrical substrate.65
Based largely on the data from dog models, there are clinical trials now enrolling patients to investigate the possible role of SCS in heart failure. The Determining the Feasibility of Spinal Cord Neuromodulation for the Treatment of Chronic Heart Failure (DEFEAT HF) trial, sponsored by Medtronic Inc., hopes to enrol 250 patients in a phase II study designed to measure changes in LV volume and exercise capacity in a population with systolic heart failure (ClinicalTrials.gov; Identifier: NCT01112579). Similarly, the Spinal Cord Stimulation For Heart Failure (SCS HEART) study is a small phase II study sponsored by St. Jude Medical that aims to enrol 20 patients in a trial designed to assess safety and develop efficacy parameters of spinal cord stimulation in patients with systolic heart failure (ClinicalTrials.gov; Identifier: NCT01362725). Neither of these trials have mentioned investigating arrhythmias in this population; however, it will be intriguing to see if there is any observed decrease in ventricular arrhythmias in this population, which is clearly at risk.
Potential Adverse Effects of Spinal Cord Stimulation
The safety of SCS has been evaluated in trials using SCS for the treatment of angina. Large trials are lacking in this field; however, most studies indicate that the procedure is safe, with device-related infections and catheter dislodgements as the most common complications of the procedure.51 There was concern in the angina trials that SCS may mask a true MI; however, evaluation of patients with electrocardiogram (ECG) evidence of an MI occurring after implantation of the spinal cord stimulator demonstrated that they were aware when their MI occurred.66 Therefore, use of SCS for either heart failure treatment or possibly for arrhythmia control is unlikely to mask significant ischaemic pain. More safety information about the procedure will be obtained in the trials that are currently enrolling patients.
Vagal Stimulation
Vagal Stimulation and Atrial Electrophysiology
In the atria, parasympathetic stimulation can be proarrhythmic. It shortens atrial myocyte action potential duration (APD) and reduces atrial effective refractory period (ERP),67 thereby shortening the atrial re-entrant wavelength (the product of ERP and conduction velocity) enhancing the possibility of re-entry.68,69 It also depresses intra-atrial conduction, and can induce re-entrant atrial arrhythmias.70 In addition, cholinergic stimulation produces atrial ERP heterogeneity, likely due to heterogeneous distribution of vagal innervation.71 There is a direct relationship between the intensity of parasympathetic stimulation, the spatial disparity of refractory periods and AF inducibility.72
As a result of its profound effect on atrial conduction, intracardiac vagal stimulation and ablation of intracardiac ganglia (predominantly cholinergic neurons) has been considered in the diagnosis and treatment of atrial arrhythmias. However, the results of this strategy have been mixed.73–79 Choi et al. recently demonstrated that in ambulatory dogs, all episodes of atrial tachyarrhythmias were preceded by bursts of autonomic activity (both parasympathetic and sympathetic),6 suggesting that vagal activity alone may not explain arrhythmogenesis in the atria. Additionally, intracardiac ganglia not only provide some parasympathetic and sympathetic efferent innervation of the atria, they also process afferent information as well.4 Therefore, predicting the outcome of ganglion ablation may be difficult and unpredictable because it may tip the balance of parasympathetic and sympathetic innervation in one direction or another, producing contradictory results among patients.
Extrinsic to the heart, vagal nerve stimulation (VNS) may also have a role in atrial arrhythmia management. Despite the fact that vagal stimulation has been used for years as a method to induce AF, recent experimental studies in dogs have demonstrated that low level VNS (below the threshold needed to reduce heart rate) may be antiarrhythmic in the atrium. Shen et al.80 demonstrated that left-sided low-level vagal stimulation decreased left-sided stellate ganglion activity, decreased the incidence of AF and atrial tachycardia, and decreased sympathetic innervation within the stellate ganglion.80 Similarly, Sha et al.,81 in a study of acute, right-sided, low-level vagal stimulation, found that the threshold to induce AF was higher in the VNS group, and the response of heart rate to direct sympathetic and parasympathetic stimulation was blunted in the setting of low level vagal stimulation. In addition, neural activity in a ganglion of the intrinsic cardiac nervous system was reduced with low level VNS, which may be the basis for its antiarrhythmic effect.80 Clearly more studies are needed to further explore the possibilities of low level VNS for arrhythmia management; however, these experimental results are intriguing.12
Vagal Stimulation and Ventricular Electrophysiology
In the ventricle, parasympathetic stimulation is thought to be cardioprotective as decreased vagal activity after myocardial infarction is associated with a higher risk of ventricular arrhythmias.1,6,82,83 It is generally accepted that VNS and cholinergic agonists prolong the ventricular effective refractory period in vivo, in animals.84–86 In patients, reflex vagal stimulation causes a small but significant prolongation of right ventricular refractoriness. Finally, VNS can influence the vulnerability to VF. In contrast to sympathetic stimulation, VNS decreased the maximum slope of APD restitution, attenuated electrical alternans, and increased ventricular ERP and VF thresholds.87
Waxman et al. provided early clinical evidence, which demonstrated that VTs could respond to vagal activation, contrary to traditional belief,88,89 and that ventricular automaticity was decreased by vagal activity.90 Subsequently, experimental animal data in conscious dogs clearly demonstrated that increasing vagal tone by means of right vagus nerve stimulation can prevent ventricular tachyarrhythmias in a model with healed myocardial infarction, evaluated with exercise testing and intermittent ischaemia.91 Interestingly, the observed antifibrillatory effect was independent from heart rate reduction. In the setting of heart failure, the Autonomic Tone and Reflexes After Myocardial Infarction (ATRAMI) study92 and the Cardiac Insufficiency Bisoprolol Study II (CIBIS II)93 demonstrated that diminished cardiac vagal activity and increased heart rate were powerful predictors of increased mortality in heart failure. Therefore, significant clinical evidence exists that vagal tone may be cardioprotective.
More recent investigations have focused on the possibility that vagal stimulation may be a treatment modality for heart failure. De Ferrari et al.94 reported the first proof of concept trial using VNS in patients with class II–IV heart failure (n=32 patients), which demonstrated significant improvement in functional ability and ejection fraction with VNS. From the arrhythmia perspective, three patients developed AF during the study, and two patients were reported to receive multiple ICD shocks, which resolved with medication changes and diuresis. The episodes of AF were thought to possibly be due to the intervention; however, the cases of ICD shocks were unlikely related to VNS. Importantly, no difference was found in VT rates observed on Holter monitors performed during the study.
The improvement in heart failure that was documented in this study has led to larger, randomised trials – the Increase of Vagal Tone in Chronic Heart Failure (INOVATE HF) and Neural Cardiac Therapy for Heart Failure (NECTAR-HF) study are currently ongoing. Both of these trials have endpoints centred around mortality and heart failure admissions, as well as measures of left ventricular function. However, analysing the data on arrhythmias from these studies (both atrial and ventricular) will provide significant insight into the potential use of VNS as an antiarrhythmic in the near future.
Potential Adverse Effects of Vagal Stimulation
Parasympathetic nerve stimulation has been used historically to promote atrial arrhythmias and therefore it certainly has this potential. VNS also may influence the vulnerability to VF by increasing the VF threshold;87 however, others have reported that vagal effects are indirect and depend on concomitant sympathetic activity.95 Thus, VNS-induced elevation of the VF thresholds may require the presence of heightened adrenergic tone. Also in some cases of idiopathic VT, enhanced vagal tone has been suggested to be profibrillatory.96,97 Less serious but important common side effects that have been reported from VNS include a cough, neck pain, swallowing difficulty or change in voice. In addition, procedural complications are certainly possible. However, as the technique improves and the clinical experience grows, VNS may emerge as a potential treatment strategy for atrial and ventricular arrhythmias.
Conclusions
As our understanding of the autonomic nervous system and its role in pathophysiology of disease states grows, the potential applications of autonomic modulation will continue to expand significantly. The techniques of renal denervation, SCS and direct vagal stimulation are all emerging as possible treatments for hypertension and heart failure, respectively, and may in turn serve as non-pharmacological antiarrhythmic strategies for atrial and ventricular arrhythmias. As the results of larger clinical trials using these techniques become available, a careful analysis of the data will be crucial to determine if an antiarrhythmic effect truly emerges. The current state of preclinical and small clinical trials provides cautious optimism that RDN, SCS and direct vagal stimulation may all play a role in arrhythmia management in the near future.
Acknowledgment
The work was supported by NIA grant 1R21AG035128.
References
- 1.Zipes DP, Rubart M. neural modulation of cardiac arrhythmias and sudden cardiac death. Heart Rhythm. 2006;3(1):108–13. doi: 10.1016/j.hrthm.2005.09.021. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lopshire JC, Zipes DP. Device therapy to modulate the autonomic nervous system to treat heart failure. CurrCardiol Rep. 2012;14(5):593–600. doi: 10.1007/s11886-012-0292-8. [DOI] [PubMed] [Google Scholar]
- 3.Singh JP, Kandala J, John C, amm A. Non-pharmacological modulation of the autonomic tone to treat heart failure. Eur Heart J. 2014;35(2):77–85. doi: 10.1093/eurheartj/eht436. [DOI] [PubMed] [Google Scholar]
- 4.Armour JA. Potential clinical relevance of the ‘little brain’ on the mammalian heart. Exp Physiol. 2008;93(2):165–76. doi: 10.1113/expphysiol.2007.041178. [DOI] [PubMed] [Google Scholar]
- 5.Armour JA, Murphy DA, Yuan BX et al. Gross and microscopic anatomy of the human intrinsic cardiac nervous system. Anat Rec. 1997;247(2):289–98. doi: 10.1002/(SICI)1097-0185(199702)247:2<289::AID-AR15>3.0.CO;2-L. [DOI] [PubMed] [Google Scholar]
- 6.Choi EK, Shen MJ, Han S et al. Intrinsic cardiac nerve activity and paroxysmal atrial tachyarrhythmia in ambulatory dogs. Circulation. 2010;121(24):2615–23. doi: 10.1161/CIRCULATIONAHA.109.919829. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.He B, Scherlag BJ, Nakagawa H et al. The intrinsic autonomic nervous system in atrial fibrillation: a review. ISRNCardiol. 2012;2012:490674. doi: 10.5402/2012/490674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Randall DC, Brown DR, McGuirt AS et al. Interactions within the intrinsic cardiac nervous system contribute to chronotropic regulation. Am J Physiol Regul Integr Comp Physiol. 2003;285((5)):R1066–75. doi: 10.1152/ajpregu.00167.2003. [DOI] [PubMed] [Google Scholar]
- 9.Oh S, Zhang Y, Bibevski S et al. Vagal denervation and atrial fibrillation inducibility: epicardial fat pad ablation does not have long-term effects. Heart Rhythm. 2006;3(6):701–8. doi: 10.1016/j.hrthm.2006.02.020. [DOI] [PubMed] [Google Scholar]
- 10.Shen MJ, Zipes DP. Role of the autonomic nervous system in modulating cardiac arrhythmias. Circ Res. 2014;114(6):1004–21. doi: 10.1161/CIRCRESAHA.113.302549. [DOI] [PubMed] [Google Scholar]
- 11.Kawashima T. The autonomic nervous system of the human heart with special reference to its origin, course, and peripheral distribution. Anat Embryol (Berl) 2005;209(6):425–38. doi: 10.1007/s00429-005-0462-1. [DOI] [PubMed] [Google Scholar]
- 12.Shen MJ, Choi EK, Tan AY et al. Neural mechanisms of atrial arrhythmias. Nat Rev Cardiol. 2012;9(1):30–9. doi: 10.1038/nrcardio.2011.139. [DOI] [PubMed] [Google Scholar]
- 13.Parati G, Esler M. The human sympathetic nervous system: its relevance in hypertension and heart failure. EurHeart J. 2012;33(9):1058–66. doi: 10.1093/eurheartj/ehs041. [DOI] [PubMed] [Google Scholar]
- 14.Sousa-Pinto B, Ferreira-Pinto MJ, Santos M, Leite-Moreira AF. Central nervous system circuits modified in heart failure: pathophysiology and therapeutic implications. Heart Fail Rev. 2014. [Epub ahead of print]. [DOI] [PubMed]
- 15.Triposkiadis F, Karayannis G, Giamouzis G et al. The sympathetic nervous system in heart failure physiology, pathophysiology, and clinical implications. J Am Coll Cardiol. 2009;54(19):1747–62. doi: 10.1016/j.jacc.2009.05.015. [DOI] [PubMed] [Google Scholar]
- 16.Meredith IT, Broughton A, Jennings GL, Esler MD. Evidence of a selective increase in cardiac sympathetic activity in patients with sustained ventricular arrhythmias. NEngl J Med. 1991;325(9):618–24. doi: 10.1056/NEJM199108293250905. [DOI] [PubMed] [Google Scholar]
- 17.Azevedo ER, Parker JD. Parasympathetic control of cardiac sympathetic activity: normal ventricular function versus congestive heart failure. Circulation. 1999;100(3):274–9. doi: 10.1161/01.cir.100.3.274. [DOI] [PubMed] [Google Scholar]
- 18.Olshansky B, Sabbah HN, Hauptman PJ, Colucci WS. Parasympathetic nervous system and heart failure: pathophysiology and potential implications for therapy. Circulation. 2008;118(8):863–71. doi: 10.1161/CIRCULATIONAHA.107.760405. [DOI] [PubMed] [Google Scholar]
- 19.Gottlieb SS, McCarter RJ, Vogel RA. Effect of beta-blockade on mortality among high-risk and low-risk patients after myocardial infarction. N Engl J Med. 1998;339(8):489–97. doi: 10.1056/NEJM199808203390801. [DOI] [PubMed] [Google Scholar]
- 20.Packer M, Bristow MR, Cohn JN et al. The effect of carvedilol on morbidity and mortality in patients with chronic heart failure. U.S. Carvedilol Heart Failure Study Group. N Engl J Med. 1996;334(21):1349–55. doi: 10.1056/NEJM199605233342101. [DOI] [PubMed] [Google Scholar]
- 21.Ryden L, Ariniego R, Arnman K et al. A Double-Blind Trial of Metoprolol in Acute Myocardial Infarction. N Engl J Med. 1983;308(11):614–8. doi: 10.1056/NEJM198303173081102. [DOI] [PubMed] [Google Scholar]
- 22.Pfeffer MA, Braunwald E, Moyé LA et al. Effect of captopril on mortality and morbidity in patients with left ventricular dysfunction after myocardial infarction. Results of the survival and ventricular enlargement trial. The SAVE Investigators. N Engl J Med. 1992;327(10):669–77. doi: 10.1056/NEJM199209033271001. [DOI] [PubMed] [Google Scholar]
- 23.Pitt B, Remme W, Zannad F et al. Eplerenone, a selective aldosterone blocker, in patients with left ventricular dysfunction after myocardial infarction. N Engl J Med. 2003;348(14):1309–21. doi: 10.1056/NEJMoa030207. [DOI] [PubMed] [Google Scholar]
- 24.Böhm M, Linz D, Urban D et al. Renal sympathetic denervation: applications in hypertension and beyond. Nat Rev Cardiol. 2013;10(8):465–76. doi: 10.1038/nrcardio.2013.89. [DOI] [PubMed] [Google Scholar]
- 25.Schlaich MP, Sobotka PA, Krum H et al. Renal sympathetic- nerve ablation for uncontrolled hypertension. N Engl J Med. 2009;361(9):932–4. doi: 10.1056/NEJMc0904179. [DOI] [PubMed] [Google Scholar]
- 26.Chinushi M, Izumi D, Iijima K et al. Blood pressure and autonomic responses to electrical stimulation of the renal arterial nerves before and after ablation of the renal artery. Hypertension. 2013;61(2):450–6. doi: 10.1161/HYPERTENSIONAHA.111.00095. [DOI] [PubMed] [Google Scholar]
- 27.Krum H, Schlaich M, Whitbourn R et al. Catheter-based renal sympathetic denervation for resistant hypertension: a multicentre safety and proof-of-principle cohort study. Lancet. 2009;373(9671):1275–81. doi: 10.1016/S0140-6736(09)60566-3. [DOI] [PubMed] [Google Scholar]
- 28.Sobotka PA, Mahfoud F, Schlaich MP et al. Sympatho-renal axis in chronic disease. ClinRes Cardiol. 2011;100(12):1049–57. doi: 10.1007/s00392-011-0335-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Steinberg JS, Pokushalov E, Mittal S. Renal denervation for arrhythmias: hope or hype? CurrCardiol Rep. 2013;15((9)):392. doi: 10.1007/s11886-013-0392-0. [DOI] [PubMed] [Google Scholar]
- 30.Ukena C, Mahfoud F, Linz D et al. Potential role of renal sympathetic denervation for the treatment of cardiac arrhythmias. EuroIntervention. 2013;9(Suppl R):R110–6. doi: 10.4244/EIJV9SRA19. [DOI] [PubMed] [Google Scholar]
- 31.Linz D, Hohl M, Nickel A et al. Effect of renal denervation on neurohumoral activation triggering atrial fibrillation in obstructive sleep apnea. Hypertension. 2013;62(4):767–74. doi: 10.1161/HYPERTENSIONAHA.113.01728. [DOI] [PubMed] [Google Scholar]
- 32.Linz D, Mahfoud F, Schotten U et al. Renal sympathetic denervation suppresses postapneic blood pressure rises and atrial fibrillation in a model for sleep apnea. Hypertension. 2012;60(1):172–8. doi: 10.1161/HYPERTENSIONAHA.112.191965. [DOI] [PubMed] [Google Scholar]
- 33.Linz D, Mahfoud F, Schotten U et al. Renal sympathetic denervation provides ventricular rate control but does not prevent atrial electrical remodeling during atrial fibrillation. Hypertension. 2013;61(1):225–31. doi: 10.1161/HYPERTENSIONAHA.111.00182. [DOI] [PubMed] [Google Scholar]
- 34.Wang X, Zhao Q, Huang H et al. Effect of Renal Sympathetic Denervation on Atrial Substrate Remodeling in Ambulatory Canines with Prolonged Atrial Pacing. PLoSOne. 2013;8((5)):e64611. doi: 10.1371/journal.pone.0064611. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Ukena C, Mahfoud F, Spies A et al. Effects of renal sympathetic denervation on heart rate and atrioventricular conduction in patients with resistant hypertension. Int J Cardiol. 2013;167(6):2846–51. doi: 10.1016/j.ijcard.2012.07.027. [DOI] [PubMed] [Google Scholar]
- 36.Pokushalov E, Romanov A, Corbucci G et al. A randomized comparison of pulmonary vein isolation with versus without concomitant renal artery denervation in patients with refractory symptomatic atrial fibrillation and resistant hypertension. J Am Coll Cardiol. 2012;60(13):1163–70. doi: 10.1016/j.jacc.2012.05.036. [DOI] [PubMed] [Google Scholar]
- 37.Brandt MC, Mahfoud F, Reda S et al. Renal sympathetic denervation reduces left ventricular hypertrophy and improves cardiac function in patients with resistant hypertension. J Am Coll Cardiol. 2012;59(10):901–9. doi: 10.1016/j.jacc.2011.11.034. [DOI] [PubMed] [Google Scholar]
- 38.Schirmer SH, Sayed MM, Reil JC et al. Improvements of left-ventricular hypertrophy and diastolic function following renal denervation - Effects beyond blood pressure and heart rate reduction. J Am Coll Cardiol. 2013;pii:S0735–1097. doi: 10.1016/j.jacc.2013.10.073. (13)06233–5. [DOI] [PubMed] [Google Scholar]
- 39.Kumar S, Teh AW, Medi C et al. Atrial remodeling in varying clinical substrates within beating human hearts: relevance to atrial fibrillation. Prog Biophys Mol Biol. 2012;;110((2–3)):278–94. doi: 10.1016/j.pbiomolbio.2012.07.011. [DOI] [PubMed] [Google Scholar]
- 40.Yusuf S, Healey JS, Pogue J et al. Irbesartan in patients with atrial fibrillation. N Engl J Med. 2011;364(10):928–38. doi: 10.1056/NEJMoa1008816. [DOI] [PubMed] [Google Scholar]
- 41.Vaseghi M, Gima J, Kanaan C et al. Cardiac sympathetic denervation in patients with refractory ventricular arrhythmias or electrical storm: Intermediate and long-term follow-up. Heart Rhythm. 2014;11(3):360–6. doi: 10.1016/j.hrthm.2013.11.028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Linz D, Wirth K, Ukena C et al. Renal denervation suppresses ventricular arrhythmias during acute ventricular ischemia in pigs. Heart Rhythm. 2013;10(10):1525–30. doi: 10.1016/j.hrthm.2013.07.015. [DOI] [PubMed] [Google Scholar]
- 43.Hoffmann BA, Steven D, Willems S, Sydow K. Renal Sympathetic Denervation as an Adjunct to Catheter Ablation for the Treatment of Ventricular Electrical Storm in the Setting of Acute Myocardial Infarction. J Cardiovasc Electrophysiol. 2013. [Epub ahead of print] [DOI] [PubMed]
- 44.Remo BF, Preminger M, Bradfield J et al. Safety and efficacy of renal denervation as a novel treatment for ventricular tachycardia storm in patients with cardiomyopathy. Heart Rhythm. 2014;11(4):541–6. doi: 10.1016/j.hrthm.2013.12.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Ukena C, Bauer A, Mahfoud F et al. Renal sympathetic denervation for treatment of electrical storm: first-in-man experience. ClinRes Cardiol. 2012;101(1):63–7. doi: 10.1007/s00392-011-0365-5. [DOI] [PubMed] [Google Scholar]
- 46.Pitt B, White H, Nicolau J et al. Eplerenone reduces mortality 30 days after randomization following acute myocardial infarction in patients with left ventricular systolic dysfunction and heart failure. J Am Coll Cardiol. 2005;46(3):425–31. doi: 10.1016/j.jacc.2005.04.038. [DOI] [PubMed] [Google Scholar]
- 47.Zhao Q, Yu S, Zou M et al. Effect of renal sympathetic denervation on the inducibility of atrial fibrillation during rapid atrial pacing. J Interv Card Electrophysiol. 2012;35(2):119–25. doi: 10.1007/s10840-012-9717-y. [DOI] [PubMed] [Google Scholar]
- 48.Krum H, Schlaich MP, Sobotka PA et al. Percutaneous renal denervation in patients with treatment-resistant hypertension: final 3-year report of the Symplicity HTN-1 study. Lancet. 2014;383(9917):622–9. doi: 10.1016/S0140-6736(13)62192-3. [DOI] [PubMed] [Google Scholar]
- 49.Esler MD, Krum H, Schlaich M et al. Renal sympathetic denervation for treatment of drug-resistant hypertension: one-year results from the Symplicity HTN-2 randomized, controlled trial. Circulation. 2012;126(25):2976–82. doi: 10.1161/CIRCULATIONAHA.112.130880. [DOI] [PubMed] [Google Scholar]
- 50.Lenski M, Mahfoud F, Razouk A et al. Orthostatic function after renal sympathetic denervation in patients with resistant hypertension. Int J Cardiol. 2013;169(6):418–24. doi: 10.1016/j.ijcard.2013.10.017. [DOI] [PubMed] [Google Scholar]
- 51.Lanza GA, Barone L, Di M, onaco A. Effect of spinal cord stimulation in patients with refractory angina: evidence from observational studies. Neuromodulation. 2012;15((6)):542–9. doi: 10.1111/j.1525-1403.2012.00430.x. discussion 549. [DOI] [PubMed] [Google Scholar]
- 52.Foreman RD, Linderoth B. Neural mechanisms of spinal cord stimulation. IntRev Neurobiol. 2012;107:87–119. doi: 10.1016/B978-0-12-404706-8.00006-1. [DOI] [PubMed] [Google Scholar]
- 53.Foreman RD, Linderoth B, Ardell JL et al. Modulation of intrinsic cardiac neurons by spinal cord stimulation: implications for its therapeutic use in angina pectoris. Cardiovasc Res. 2000;47(2):367–75. doi: 10.1016/s0008-6363(00)00095-x. [DOI] [PubMed] [Google Scholar]
- 54.Olgin JE, Takahashi T, Wilson E et al. Effects of thoracic spinal cord stimulation on cardiac autonomic regulation of the sinus and atrioventricular nodes. JCardiovasc Electrophysiol. 2002;13(5):475–81. doi: 10.1046/j.1540-8167.2002.00475.x. [DOI] [PubMed] [Google Scholar]
- 55.Bernstein SA, Wong B, Vasquez C et al. Spinal cord stimulation protects against atrial fibrillation induced by tachypacing. Heart Rhythm. 2012;9(9):1426–33. doi: 10.1016/j.hrthm.2012.04.038. e3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Cardinal R, Pagé P, Vermeulen M et al. Spinal cord stimulation suppresses bradycardias and atrial tachyarrhythmias induced by mediastinal nerve stimulation in dogs. Am J Physiol Regul Integr Comp Physiol. 2006;291((5)):R1369–75. doi: 10.1152/ajpregu.00056.2006. [DOI] [PubMed] [Google Scholar]
- 57.Zipes DP. Heart-brain interactions in cardiac arrhythmias: role of the autonomic nervous system. Cleve Clin J Med. 2008;75(Suppl 2):S94–6. doi: 10.3949/ccjm.75.suppl_2.s94. [DOI] [PubMed] [Google Scholar]
- 58.Issa ZF, Zhou X, Ujhelyi MR et al. Thoracic spinal cord stimulation reduces the risk of ischemic ventricular arrhythmias in a postinfarction heart failure canine model. Circulation. 2005;111(24):3217–20. doi: 10.1161/CIRCULATIONAHA.104.507897. [DOI] [PubMed] [Google Scholar]
- 59.Odenstedt J, Linderoth B, Bergfeldt L et al. Spinal cord stimulation effects on myocardial ischemia, infarct size, ventricular arrhythmia, and noninvasive electrophysiology in a porcine ischemia-reperfusion model. Heart Rhythm. 2011;8(6):892–8. doi: 10.1016/j.hrthm.2011.01.029. [DOI] [PubMed] [Google Scholar]
- 60.Lopshire JC, Zhou X, Dusa C et al. Spinal cord stimulation improves ventricular function and reduces ventricular arrhythmias in a canine postinfarction heart failure model. Circulation. 2009;120(4):286–94. doi: 10.1161/CIRCULATIONAHA.108.812412. [DOI] [PubMed] [Google Scholar]
- 61.Lujan HL, Krishnan S, Dicarlo SE. Cardiac spinal deafferentation reduces the susceptibility to sustained ventricular tachycardia in conscious rats. Am J Physiol Regul Integr Comp Physiol. 2011;301((3)):R775–82. doi: 10.1152/ajpregu.00140.2011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Bourke T, Vaseghi M, Michowitz Y et al. Neuraxial modulation for refractory ventricular arrhythmias: value of thoracic epidural anesthesia and surgical left cardiac sympathetic denervation. Circulation. 2010;121(21):2255–62. doi: 10.1161/CIRCULATIONAHA.109.929703. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Cao JM, Fishbein MC, Han JB et al. Relationship between regional cardiac hyperinnervation and ventricular arrhythmia. Circulation. 2000;101(16):1960–9. doi: 10.1161/01.cir.101.16.1960. [DOI] [PubMed] [Google Scholar]
- 64.Zhou S, Jung BC, Tan AY et al. Spontaneous stellate ganglion nerve activity and ventricular arrhythmia in a canine model of sudden death. Heart Rhythm. 2008;5(1):131–9. doi: 10.1016/j.hrthm.2007.09.007. [DOI] [PubMed] [Google Scholar]
- 65.Ferrero P, Castagno D, Massa R et al. Spinal cord stimulation affects T-wave alternans in patients with ischaemic cardiomyopathy: a pilot study. Europace. 2008;10(4):506–8. doi: 10.1093/europace/eun052. [DOI] [PubMed] [Google Scholar]
- 66.Andersen C, Hole P, Oxhøj H. Does pain relief with spinal cord stimulation for angina conceal myocardial infarction? Br Heart J. 1994;71(5):419–21. doi: 10.1136/hrt.71.5.419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Prystowsky EN, Naccarelli GV, Jackman WM et al. Enhanced parasympathetic tone shortens atrial refractoriness in man. Am J Cardiol. 1983;51(1):96–100. doi: 10.1016/s0002-9149(83)80018-6. [DOI] [PubMed] [Google Scholar]
- 68.Liu L, Nattel S. Differing sympathetic and vagal effects on atrial fibrillation in dogs: role of refractoriness heterogeneity. Am J Physiol. 1997;273((2 Pt 2)):H805–16. doi: 10.1152/ajpheart.1997.273.2.H805. [DOI] [PubMed] [Google Scholar]
- 69.Smeets JL, Allessie MA, Lammers WJ et al. The wavelength of the cardiac impulse and reentrant arrhythmias in isolated rabbit atrium. The role of heart rate, autonomic transmitters, temperature, and potassium. Circ Res. 1986;58(1):96–108. doi: 10.1161/01.res.58.1.96. [DOI] [PubMed] [Google Scholar]
- 70.Rosenshtraukh LV, Zaitsev AV, Fast VG et al. Vagally induced depression of impulse propagation as a cause of atrial tachycardia. J Mol Cell Cardiol. 1991;23(Suppl 1):3–9. doi: 10.1016/0022-2828(91)90018-h. [DOI] [PubMed] [Google Scholar]
- 71.Arora R, Ulphani JS, Villuendas R et al. Neural substrate for atrial fibrillation: implications for targeted parasympathetic blockade in the posterior left atrium. Am J Physiol Heart Circ Physiol. 2008;294((1)):H134–44. doi: 10.1152/ajpheart.00732.2007. [DOI] [PubMed] [Google Scholar]
- 72.Wang J, Liu L, Feng J, Nattel S. Regional and functional factors determining induction and maintenance of atrial fibrillation in dogs. Am J Physiol. 1996;271((1 Pt 2)):H148–58. doi: 10.1152/ajpheart.1996.271.1.H148. [DOI] [PubMed] [Google Scholar]
- 73.Schauerte P, Scherlag BJ, Pitha J et al. Catheter ablation of cardiac autonomic nerves for prevention of vagal atrial fibrillation. Circulation. 2000;102(22):2774–80. doi: 10.1161/01.cir.102.22.2774. [DOI] [PubMed] [Google Scholar]
- 74.Lemola K, Chartier D, Yeh YH et al. Pulmonary vein region ablation in experimental vagal atrial fibrillation: role of pulmonary veins versus autonomic ganglia. Circulation. 2008;117(4):470–7. doi: 10.1161/CIRCULATIONAHA.107.737023. [DOI] [PubMed] [Google Scholar]
- 75.Chiou CW, Eble JN, Zipes DP et al. Efferent vagal innervation of the canine atria and sinus and atrioventricular nodes. The third fat pad. Circulation. 1997;95(11):2573–84. doi: 10.1161/01.cir.95.11.2573. [DOI] [PubMed] [Google Scholar]
- 76.Pokushalov E, Romanov A, Shugayev P et al. Selective ganglionated plexi ablation for paroxysmal atrial fibrillation. Heart Rhythm. 2009;6(9):1257–64. doi: 10.1016/j.hrthm.2009.05.018. [DOI] [PubMed] [Google Scholar]
- 77.Katritsis D, Giazitzoglou E, Sougiannis D et al. Anatomic approach for ganglionic plexi ablation in patients with paroxysmal atrial fibrillation. Am J Cardiol. 2008;102(3):330–4. doi: 10.1016/j.amjcard.2008.03.062. [DOI] [PubMed] [Google Scholar]
- 78.Danik S, Neuzil P, d’Avila A et al. Evaluation of catheter ablation of periatrial ganglionic plexi in patients with atrial fibrillation. Am J Cardiol. 2008;102(5):578–83. doi: 10.1016/j.amjcard.2008.04.064. [DOI] [PubMed] [Google Scholar]
- 79.Verma A, Saliba WI, Lakkireddy D et al. Vagal responses induced by endocardial left atrial autonomic ganglion stimulation before and after pulmonary vein antrum isolation for atrial fibrillation. Heart Rhythm. 2007;4(9):1177–82. doi: 10.1016/j.hrthm.2007.04.023. [DOI] [PubMed] [Google Scholar]
- 80.Shen MJ, Shinohara T, Park HW et al. Continuous low- level vagus nerve stimulation reduces stellate ganglion nerve activity and paroxysmal atrial tachyarrhythmias in ambulatory canines. Circulation. 2011;123(20):2204–12. doi: 10.1161/CIRCULATIONAHA.111.018028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Sha Y, Scherlag BJ, Yu L et al. Low-level right vagal stimulation: anticholinergic and antiadrenergic effects. J Cardiovasc Electrophysiol. 2011;22(10):1147–53. doi: 10.1111/j.1540-8167.2011.02070.x. [DOI] [PubMed] [Google Scholar]
- 82.Schwartz PJ, Billman GE, Stone HL. Autonomic mechanisms in ventricular fibrillation induced by myocardial ischemia during exercise in dogs with healed myocardial infarction. An experimental preparation for sudden cardiac death. Circulation. 1984;69(4):790–800. doi: 10.1161/01.cir.69.4.790. [DOI] [PubMed] [Google Scholar]
- 83.Schwartz PJ, Vanoli E, Stramba-Badiale M et al. Autonomic mechanisms and sudden death. New insights from analysis of baroreceptor reflexes in conscious dogs with and without a myocardial infarction. Circulation. 1988;78(4):969–79. doi: 10.1161/01.cir.78.4.969. [DOI] [PubMed] [Google Scholar]
- 84.Litovsky SH, Antzelevitch C. Differences in the electrophysiological response of canine ventricular subendocardium and subepicardium to acetylcholine and isoproterenol. A direct effect of acetylcholine in ventricular myocardium. Circ Res. 1990;67(3):615–27. doi: 10.1161/01.res.67.3.615. [DOI] [PubMed] [Google Scholar]
- 85.Martins JB, Zipes DP, Lund DD. Distribution of local repolarization changes produced by efferent vagal stimulation in the canine ventricles. J Am Coll Cardiol. 1983;2(6):1191–9. doi: 10.1016/s0735-1097(83)80350-7. [DOI] [PubMed] [Google Scholar]
- 86.Pickoff AS, Stolfi A. Modulation of electrophysiological properties of neonatal canine heart by tonic parasympathetic stimulation. Am J Physiol. 1990;258((1 Pt 2)):H38–44. doi: 10.1152/ajpheart.1990.258.1.H38. [DOI] [PubMed] [Google Scholar]
- 87.Ng GA, Brack KE, Patel VH, Coote JH. Autonomic modulation of electrical restitution, alternans and ventricular fibrillation initiation in the isolated heart. Cardiovasc Res. 2007;73(4):750–60. doi: 10.1016/j.cardiores.2006.12.001. [DOI] [PubMed] [Google Scholar]
- 88.Waxman MB, Downar E, Berman ND, Felderhof CH. Phenylephrine (Neo-synephrine) terminated ventricular tachycardia. Circulation. 1974;50(4):656–64. doi: 10.1161/01.cir.50.4.656. [DOI] [PubMed] [Google Scholar]
- 89.Waxman MB, Wald RW. Termination of ventricular tachycardia by an increase in cardiac vagal drive. Circulation. 1977;56(3):385–91. doi: 10.1161/01.cir.56.3.385. [DOI] [PubMed] [Google Scholar]
- 90.Waxman MB, Cupps CL, Cameron DA. Modulation of an idioventricular rhythm by vagal tone. JAm Coll Cardiol. 1988;11(5):1052–60. doi: 10.1016/s0735-1097(98)90065-1. [DOI] [PubMed] [Google Scholar]
- 91.Vanoli E, De F, errari GM, Stramba-Badiale M et al. Vagal stimulation and prevention of sudden death in conscious dogs with a healed myocardial infarction. Circ Res. 1991;68(5):1471–81. doi: 10.1161/01.res.68.5.1471. [DOI] [PubMed] [Google Scholar]
- 92.La R, overe MT, Bigger JT, Jr, Marcus FI et al. Baroreflex sensitivity and heart-rate variability in prediction of total cardiac mortality after myocardial infarction. ATRAMI (Autonomic Tone and Reflexes After Myocardial Infarction) Investigators. Lancet. 1998;351(9101):478–84. doi: 10.1016/s0140-6736(97)11144-8. [DOI] [PubMed] [Google Scholar]
- 93.Lechat P, Hulot JS, Escolano S et al. Heart rate and cardiac rhythm relationships with bisoprolol benefit in chronic heart failure in CIBIS II Trial. Circulation. 2001;103(10):1428–33. doi: 10.1161/01.cir.103.10.1428. [DOI] [PubMed] [Google Scholar]
- 94.De Ferrari GM, Crijns HJ, Borggrefe M et al. Chronic vagus nerve stimulation: a new and promising therapeutic approach for chronic heart failure. Eur Heart J. 2011;32(7):847–55. doi: 10.1093/eurheartj/ehq391. [DOI] [PubMed] [Google Scholar]
- 95.Kolman BS, Verrier RL, Lown B. The effect of vagus nerve stimulation upon vulnerability of the canine ventricle: role of sympathetic-parasympathetic interactions. Circulation. 1975;52(4):578–85. doi: 10.1161/01.cir.52.4.578. [DOI] [PubMed] [Google Scholar]
- 96.Kasanuki H, Ohnishi S, Ohtuka M et al. Idiopathic ventricular fibrillation induced with vagal activity in patients without obvious heart disease. Circulation. 1997;95(9):2277–85. doi: 10.1161/01.cir.95.9.2277. [DOI] [PubMed] [Google Scholar]
- 97.Luu M, Stevenson WG, Stevenson LW et al. Diverse mechanisms of unexpected cardiac arrest in advanced heart failure. Circulation. 1989;80(6):1675–80. doi: 10.1161/01.cir.80.6.1675. [DOI] [PubMed] [Google Scholar]