

Abstract
Arrhythmias in adults with congenital heart disease, most commonly related to previous surgical procedures, are a frequent comorbidity in this growing population thanks to the improved outcome of surgical techniques. Re-entrant circuits around areas of scarring and natural barriers, combined with abnormal haemodynamics and the underlying anatomy, are the most common cause for these arrhythmias. They are often poorly tolerated and medical treatment is frequently inadequate. In recent years, catheter ablation has emerged as a successful therapeutic option. New advanced techniques such as the use of modern three-dimensional (3D) navigation systems have contributed to better understanding of the arrhythmia mechanisms and higher success rates of the ablation procedures. In this article we briefly summarise the characteristics of the most common arrhythmias in this patient population and some key aspects in their treatment by catheter ablation.
Keywords: Congenital heart disease, catheter ablation, Mustard, Senning, Fontan, Ebstein, Fallot
Around 0.8 % of live births are affected by some type of congenital heart disease; 30–50 % of whom will need one or more surgical interventions, generally during early childhood, involving in some cases complex corrections with patches, baffles or extracardiac circuits.1,2
As a result of advances in surgical interventions, the life expectancy of patients with congenital heart disease has significantly improved. Consequently, a greater proportion of these patients reach adulthood where they face significant morbidities, among which cardiac arrhythmias have a considerable impact not only on their quality of life but also on their survival.3
The mechanisms responsible for the appearance of these cardiac arrhythmias vary depending on both the nature of the underlying defects and the type of surgical correction. These determine the electrophysiological substrate through a complex interplay between gross cardiac anatomy, chamber enlargement from increased pressure and volume loads, cellular injury from hypoxia and cardiopulmonary bypass, fibrosis at sites of suture lines and patches, and direct trauma to the specialised conduction tissues.2
Most surgical corrections involve manipulation of atrial chambers. It is therefore not surprising that many of the arrhythmias seen in this patient population are atrial in origin, usually involving macro re-entrant circuits around areas of scarring and natural barriers.4
It is important to be aware that in patients with complex congenital heart disease and poor haemodynamic reserves these arrhythmias can be poorly tolerated and easily lead to haemodynamic collapse (e.g. in patients with previous Fontan correction) requiring urgent electrical cardioversion to restoration of haemodynamic stability.5 Antiarrhythmic medication including type Ic and III drugs often fail to prevent arrhythmic events and are associated with the development of severe side-effects, including thyroid dysfunction and pulmonary fibrosis, which may limit their use.6 Catheter ablation has emerged as a highly successful alternative therapeutic option in most cases, either alone or in combination with ongoing drug treatment.7,8 New technological advances in catheters and energy sources, three-dimensional (3D) navigation mapping systems and the development of magnetic navigation have improved the outcome of ablation procedures to a great extent.9
In recent years better knowledge of the circuits responsible for these arrhythmias has contributed to the modification of surgical techniques, which may also lead to a reduction in the incidence of cardiac arrhythmias.10,11
Macro Re-entrant Atrial Tachycardias and Atrial Flutter
These are the most common arrhythmias in patients with CHD, usually secondary to a re-entrant circuit around scarred tissues due to patches, atriotomies or other natural or surgically created barriers to electrical conduction.4 Risk factors, in addition to the type of surgery, include concomitant sinus node dysfunction (tachy-brady syndrome), older age at operation and longer follow-up.12,13
In relatively simple CHD, such as lone atrial septal defect (ASD) or ventricular septal defect (VSD), the most common atrial substrate is a combination of typical atrial flutter around the cavotricuspid isthmus (CTI) and flutter around atriotomy scars.14 In these cases, typical atrial flutter may switch to flutter around the atriotomy during the ablation procedure as the cavotricuspid isthmus blocks with only a small change in cycle length.15 Following termination of the flutter by ablation it is essential to ensure not only that the cavotricuspid isthmus is blocked but also that the atriotomy scar is extended to the inferior vena cava. Block across this line can be confirmed by pacing the low right atrium posterior to the line and demonstrating high to low activation of the anterolateral right atrium. Other circuits may also be seen, particularly on the septum around the ASD repair itself.16
New atrial fibrillation is also frequently seen in patients with ASD even after a successful correction/closure. In these circumstances, left atrial access for pulmonary vein isolation may be difficult. It is usually straightforward to perform a transseptal puncture in post-surgical repairs particularly with echo guidance. It is more challenging in those patients with a previous percutaneous ASD closure. However, in the majority of cases transseptal puncture can be safely performed alongside or occasionally through the device under transoesophageal or intracardiac echo guidance (see Figure 1).17,18 Retrograde transaortic approach with the support of magnetic navigation is an alternative route when transseptal puncture is not possible.19
Figure 1: Transoesophageal Echocardiography-guided Transseptal Puncture Before Atrial Fibrillation Ablation in a Patient with a Previous Percutaneous Atrial Septal Defect Closure and a Dual Chamber Pacemaker Due to Sinus Dysfunction.
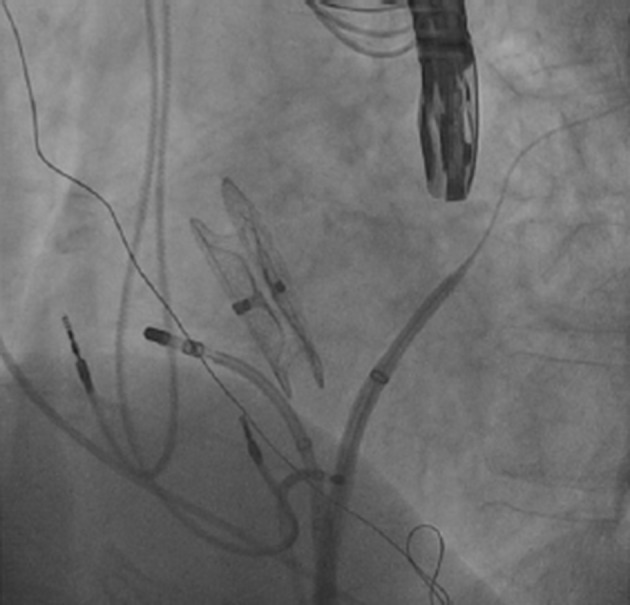
The transseptal puncture could be performed safely away from the atrial septal defect closure device. Both ablation catheter and Lasso could be advanced into the left atrium and the ablation procedure was carried out normally. The image corresponds to a left anterior oblique projection.
As the original disease and its surgical correction get more complex, the likelihood of a more complex intra-atrial re-entrant tachycardia (IART) increases.20 These circuits are often associated with slower cycle length than in typical atrial flutter (270–450 ms) allowing in some cases a 1:1 atrioventricular (AV) conduction, occasionally with poor haemodynamic tolerance needing urgent electrical cardioversion.4,5 In extreme cases the cycle length may be so long that they are mistaken for sinus rhythm and are only easily differentiated by a lack of heart rate variability.
A group of patients that deserve special consideration are those who have had a Mustard or Senning correction for dextro-transposition of the great arteries (d-TGA). At least 30 % of them will also develop some type of IART.4 Most commonly these IART are CTI-dependent flutters.21 In our experience, even when no arrhythmia can be induced in the lab, performance of empiric CTI line ablation will often lead to a good outcome. This requires ablation at both sides of the baffle suture line, which can be achieved by either a retrograde approach or a trans-baffle puncture (see Figure 2).22,23
Figure 2: Cavotricuspid Isthmus Ablation at Both Sides of the Baffle in a Patient with Previous Senning Intervention.
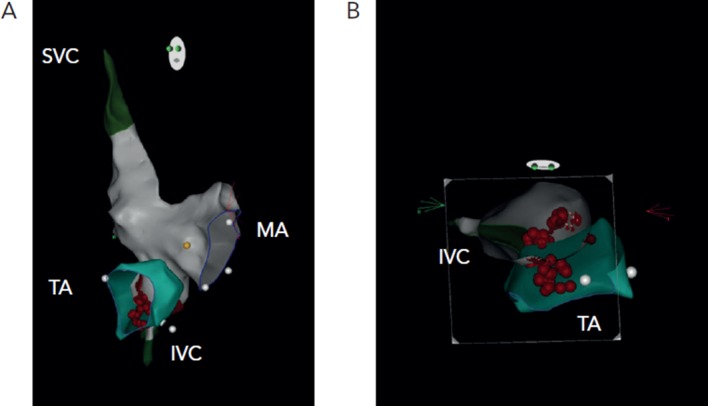
Images in left anterior oblique view (A) and clipped superior view (B). IVC = inferior vena cava; MA = mitral annulus; SVC = superior vena cava; TA = tricuspid annulus.
A careful analysis of the surgical procedure is necessary before attempting any type of electrophysiological study, as is confirmation of patency of venous access to the heart, as unilateral or even bilateral ileofemoral vein occlusion is not uncommon as a result of frequent history of balloon atrial septostomy as newborns and multiple catheterisations.24
Other types of supraventricular tachycardia, particularly atrioventricular nodal re-entry tachycardias (AVNRT), are seen in this group of patients, and they should be ruled out during the electrophysiological study. AVNRT can be treated by a standard AV nodal slow pathway modification, although this usually has to be approached retrogradely (see Figure 3).25 Focal atrial tachycardias usually arising from areas of abnormal atrial tissue are not uncommon either and can be equally targeted for ablation with good results.26
Figure 3: Atrioventricular Nodal Slow Pathway Modification for Atrioventricular Nodal Re-entrant Tachycardia in Patient with Previous Senning Surgical Procedure and Dual Chamber Pacemaker Due to Sinus Dysfunction.
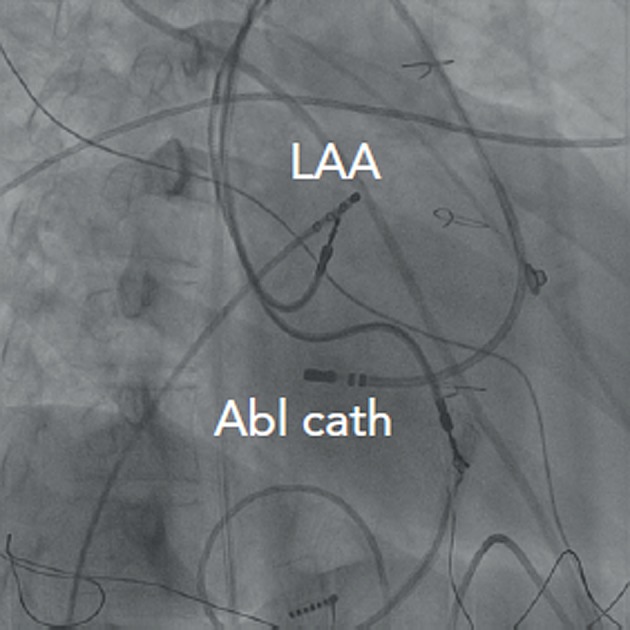
The ablation was targeted retrogradely through the aortic root. The image corresponds to a right anterior oblique projection. Abl cath = ablation catheter; LAA = left atrial appendage.
In patients with a single ventricle following a classic right atrial–right ventricular or atriopulmonary Fontan connection, complex IART can be observed in up to 50 % within a decade of the surgery.4 The electrophysiological procedures in these patients are particularly challenging due to the usually severely dilatation of the right atrium, thickness of atrial wall that may hinder or preclude transmural lesion formation and the frequent existence of more than one re-entrant circuit. The vast majority of the re-entrant circuits are located in the right atrium, mainly associated with the atriotomy scar (usually in low anterolateral area) and the CTI, and less frequently around caval orifices, crista terminalis or the atrial appendage.24 Prior to the electrophysiological procedure intra-atrial thrombus must be excluded.27 It is usual for multiple IARTs to be induced in a single patient, each requiring individual mapping and ablation. Empiric cavotricuspid and intercaval ablation may be useful particularly in patients with multiple tachycardias or more irregular tachycardias, or where the tachycardia is non-inducible or not haemodynamically tolerated. 3D mapping is essential but the use of arrays is limited by the large size of the Fontan chamber. Access to the atrial tissue can be difficult in patients with more modern surgical approaches such as the lateral tunnel and extracardiac total cavopulmonary connection, but can be achieved by collaboration with the congenital heart teams.28 Alternatively, remote magnetic navigation via a retrograde approach is particularly useful in these patient groups, allowing easy retrograde access to the atrial chambers without the need for more invasive interventional procedures.9
Accessory Atrioventricular Pathways
The incidence of accessory atrioventricular pathways is similar to that of normal population with the clear exceptions of Ebstein’s anomaly and congenitally corrected levo-transposition of the great arteries (L-TGA). Indeed in Ebstein’s anomaly around 20 % of patients will show the presence of accessory atrioventricular connections (typically along the posterior and septal portion of the tricuspid ring), and 50 % of them will be affected by multiple accessory pathways.20,29 Accessory pathways are present in 2–5 % of patients with l-TGA with an Ebsteinoid malformation of their left-sided (systemic) tricuspid valve.24
Ablation of the accessory pathways in Ebstein’s anomaly or l-TGA can be challenging due to the displacement of the AV valves in relation to the real AV grooves, which is the optimal level for ablation of pathways. Their location is generally parallel to the course of right coronary artery or the coronary sinus. Therefore a selective angiography or placement of catheters inside these vessels can be useful to facilitate the ablation procedure.30 Ablation is acutely successful in 80 % of patients, with a recurrence rate of 25–40 %. This worse outcome after the ablation of accessory pathways is due to several factors, including the presence of frequent multiple accessory pathways, power limitation because of the proximity of coronary arteries or the AV node in a particularly thin right atrium as is usually the case in Ebstein’s anomaly.31,32 The use of 3D mapping, steerable sheaths and multipolar mapping catheters can be of particular use in this subgroup of patients.
A special situation is the case of patients with heterotaxy syndrome that can have the so-called ‘twin AV nodes’ consisting of two separate AV nodes and a diverse combination of possible re-entrant circuits. The ablation of the AV node with poorer anterograde conduction properties, which generally constitutes the retrograde limb of the re-entrant tachycardia, has shown to be effective in this setting.33
Ventricular Tachycardias
Two main mechanisms are involved in the development of ventricular tachycardias (VTs) in CHD patients. Firstly, the presence of surgical ventricular scars (ventriculotomy) or patching material may determine the appearance of macro re-entrant VT. This mechanism has been described particularly in patients following correction of tetralogy of Fallot who have a prevalence of VT of 3–14 %, and an incidence of sudden cardiac death of 2 % per decade with increasing risk for older patients.34,35 Four main macro re-entrant routes have been described involving specific anatomical isthmuses:
between the right ventricular outflow tract/adjacent right ventricular scar and tricuspid annulus;
between the right ventricular scar and pulmonary valve;
between the pulmonary valve and septal scar; and
between the septal scar and the tricuspid annulus.
These can be targeted by ablation with a high degree of success.36
Secondly, progressive degrees of ventricular dysfunction or hypertrophy due to altered haemodynamic state as seen in aortic valve disease, right ventricular dysfunction after Senning or Mustard procedures for d-TGA, or in failing single ventricles can also increase the risk for ventricular arrhythmias independently of the presence or not of surgery-related scars.
Risk factors for VT include: older age at surgery, older age at follow-up, prior palliative shunts, high density of ventricular ectope on non-invasive monitoring, inducible VT at electrophysiological study, poor right ventricular haemodynamics, depressed left ventricular function, markedly prolonged QRS duration (>180 ms) and previous symptoms of rapid palpitations, dizziness or syncope.2,4,34
Due to the high incidence of sudden cardiac death there is a low threshold for ICD implantation to treat VT in CHD, with ablation often reserved to reduce the number of shocks rather than as a first-line treatment, particularly in patients with impaired systemic ventricle. New surgical procedures to improve the cardiac haemodynamics or antiarrhythmic medication may reduce the risk for VT and sudden cardiac death in the future.
Conclusions
Adult patients affected by congenital heart disease are a growing population thanks to the development of advanced techniques for surgical repair. These patients are at lifelong risk of complications, including a high incidence of arrhythmias that are generally sustained by complex macro re-entrant circuits. Although technically challenging, catheter ablation continues to be the best therapeutic option for these arrhythmias after a thorough analysis of the specific cardiac anomaly and its surgical correction. A better understanding of the electrophysiological substrates has led to improved outcome of ablation procedures, and has contributed to the modification of surgical techniques producing a significant reduction of the arrhythmic burden in younger generations.
References
- 1.Gatzoulis MA, Webb GD. Adults with congenital heart disease: a growing population. In: Gatzoulis MA, Webb GD, Daubeney PEF, editors. Diagnosis and management of adult congenital heart disease 2nd ed. Philadelphia US: Elsevier Saunders; 2011. p. 2. [Google Scholar]
- 2.Walsh EP. Interventional electrophysiology in patients with congenital heart disease. Circulation. 2007;115:3224–34. doi: 10.1161/CIRCULATIONAHA.106.655753. [DOI] [PubMed] [Google Scholar]
- 3.Somerville J. Management of adults with congenital heart disease: an increasing problem. Annu Rev Med. 1997;48:283–93. doi: 10.1146/annurev.med.48.1.283. [DOI] [PubMed] [Google Scholar]
- 4.Walsh EP. Arrhythmias in patients with congenital heart disease. Card Electrophysiol Rev. 2002;6:422–30. doi: 10.1023/a:1021192526642. [DOI] [PubMed] [Google Scholar]
- 5.Garson A, Jr, Bink-Boelkens M, Hesslein PS et al. Atrial flutter in the young: a collaborative study of 380 cases. J Am Coll Cardiol. 1985;6:871–8. doi: 10.1016/s0735-1097(85)80497-6. [DOI] [PubMed] [Google Scholar]
- 6.Thorne SA, Barnes I, Cullinan P, Somerville J. Amiodarone- associated thyroid dysfunction: risk factors in adults with congenital heart disease. Circulation. 1999;100:149–54. doi: 10.1161/01.cir.100.2.149. [DOI] [PubMed] [Google Scholar]
- 7.van Hare GF. Radiofrequency ablation of accessory pathways associated with congenital heart disease. Pacing Clin Electrophysiol. 1997;20:2077–81. doi: 10.1111/j.1540-8159.1997.tb03632.x. [DOI] [PubMed] [Google Scholar]
- 8.Tanner H, Lukac P, Schwick N et al. Irrigated-tip catheter ablation of intraatrial reentrant tachycardia in patients late after surgery of congenital heart disease. Heart Rhythm. 2004;1:268–75. doi: 10.1016/j.hrthm.2004.04.020. [DOI] [PubMed] [Google Scholar]
- 9.Ueda A, Suman-Horduna I, Mantziari L et al. Contemporary otuomes of supraventricular tachycardia ablation in congenital heart disease. A singe-centre experience in 116 patients. Circ Arrhythm Electrophysiol. 2013;6:606–13. doi: 10.1161/CIRCEP.113.000415. [DOI] [PubMed] [Google Scholar]
- 10.Rhodes LA, Wernovsky G, Keane JF et al. Arrhythmias and intracardiac conduction after the arterial switch operation. J Thorac Cardiovasc Surg. 1995;109:303–10. doi: 10.1016/S0022-5223(95)70392-6. [DOI] [PubMed] [Google Scholar]
- 11.Stamm C, Friehs I, Mayer JE, Jr et al. Long-term results of the lateral tunnel Fontan operation. J Thorac Cardiovasc Surg. 2001;121:28–41. doi: 10.1067/mtc.2001.111422. [DOI] [PubMed] [Google Scholar]
- 12.Fishberger SB, Wernovsky G, Gentles TL et al. Factors that influence the development of atrial flutter after the Fontan operation. J Thorac Cadiovas Surg. 1997;113:80–6. doi: 10.1016/s0022-5223(97)70402-1. [DOI] [PubMed] [Google Scholar]
- 13.Durongpisitkul K, Porter CJ, Cetta F et al. Predictors of early- and late-onset supraventricular tachyarrhythmias after Fontan operation. Circulation. 1998;98:1099–107. doi: 10.1161/01.cir.98.11.1099. [DOI] [PubMed] [Google Scholar]
- 14.Wasmer K, Köbe J, Dechering DG et al. Isthmus-dependent right atrial flutter as the leading cause of atrial tachycardias after surgical atrial septal defect repair. Int J Cardiol. 2013;168:2447–52. doi: 10.1016/j.ijcard.2013.03.012. [DOI] [PubMed] [Google Scholar]
- 15.Uhm JS, Mun HS, Wi J et al. Importance of tachycardia cycle length for differentiating typical atrial flutter from scar-related in adult congenital heart disease. Pacing Clin Electrophysiol. 2012;35:1338–47. doi: 10.1111/j.1540-8159.2012.03494.x. [DOI] [PubMed] [Google Scholar]
- 16.Love BA, Collins KK, Walsh EP, Triedman JK. Electroanatomic characterization of conduction barriers in sinus/atrial paced rhythm and association with intra-atrial reentrant tachycardia circuits following congenital heart disease surgery. J Cardiovasc Electrophysiol. 2001;12:17–25. doi: 10.1046/j.1540-8167.2001.00017.x. [DOI] [PubMed] [Google Scholar]
- 17.Lakkireddy D, Rangisetty U, Prasad S et al. Intracardiac echo- guided radiofrequency catheter ablation of atrial fibrillation in patients with atrial septal defect or patent foramen ovale repair: a feasibility, safety, and efficacy study. J Cardiovasc Electrophysiol. 2008;19:1137–42. doi: 10.1111/j.1540-8167.2008.01249.x. [DOI] [PubMed] [Google Scholar]
- 18.Santangeli P, DiBiase L, Burkhardt D et al. Transseptal access and atrial fibrillation ablation guided by intracardiac echocardiography in patients with atrial septal closure devices. Heart Rhythm. 2011;8:1669–75. doi: 10.1016/j.hrthm.2011.06.023. [DOI] [PubMed] [Google Scholar]
- 19.Miyazaki S, Nault I, Haïssaguerre M, Hocini M. Atrial fibrillation ablation by aortic retrograde approach usiing a magnetic navigation system. J Cardiovasc Electrophysiol. 2010;21:455–7. doi: 10.1111/j.1540-8167.2009.01666.x. [DOI] [PubMed] [Google Scholar]
- 20.Triedman JK, Jenkins KJ, Colan SD et al. Intra-atrial reentrant tachycardia after palliation of congenital heart disease: characterization of multiple macroreentrant circuits using fluoroscopically based three-dimensional endocardial mapping. J Cardiovasc Electrophysiol. 1997;8(3):259–70. doi: 10.1111/j.1540-8167.1997.tb00789.x. [DOI] [PubMed] [Google Scholar]
- 21.Lukac P, Pedersen A, Mortensen PT et al. Ablation of atrial tachycardia after surgery for congenital and acquired heart disease using an electroanatomic mapping system: Which circuits to expect in which substrate? Heart Rhythm. 2005;2:64–72. doi: 10.1016/j.hrthm.2004.10.034. [DOI] [PubMed] [Google Scholar]
- 22.Kanter RJ, Papagiannis J, Carboni MP et al. Radiofrequency catheter ablation of supraventricular tachycardia substrates after Mustard and Senning operations for d-transposition of the great arteries. J Am Coll Cardiol. 2000;35:428–41. doi: 10.1016/s0735-1097(99)00557-4. [DOI] [PubMed] [Google Scholar]
- 23.Jones DG, Jarman JW, Lyne JC et al. The safety and efficacy of trans-baffle puncture to enable catheter ablation of atrial tachycardias following the Mustard procedure: a single centre experience and literature review. Int J Cardiol. 2013;168(2):1115–20. doi: 10.1016/j.ijcard.2012.11.047. [DOI] [PubMed] [Google Scholar]
- 24.Kanter RJ. Pearls for ablation in congenital heart disease. J Cardiovasc Electrophysiol. 2010;21:223–30. doi: 10.1111/j.1540-8167.2009.01685.x. [DOI] [PubMed] [Google Scholar]
- 25.Wu J, Deisenhofer I, Ammar S et al. Acute and long-term outcome after catheter ablation of supraventricular tachycardia in patients after the Mustard or Senning operation for D-transposition of the great arteries. Europace. 2013;15:886–91. doi: 10.1093/europace/eus402. [DOI] [PubMed] [Google Scholar]
- 26.de G, root NM, Zeppenfeld K, Wijffels MC et al. Ablation of focal atrial arrhythmia in patients with congenital heart defects after surgery: role of circumscribed areas with heterogeneous conduction. Heart Rhythm. 2006;3:526–35. doi: 10.1016/j.hrthm.2006.01.011. [DOI] [PubMed] [Google Scholar]
- 27.Grewal J, Al Hussein M, Feldstein J et al. Evaluation of silent thrombus after the Fontan operation. Congenit Heart Dis. 2013;8:40–7. doi: 10.1111/j.1747-0803.2012.00699.x. [DOI] [PubMed] [Google Scholar]
- 28.Dave AS, Aboulhosn J, Child JS, Shivkumar K. Transconduit puncture for catheter ablation of atrial tachycardia in a patient with extracardiac Fontan palliation. Heart Rhythm. 2010;7:413–6. doi: 10.1016/j.hrthm.2009.10.037. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Attenhofer Jost CH, Connolly HM, Edwards WD et al. Ebstein’s anomaly - review of a multifaceted congenital cardiac condition. Swiss Med Wkly. 2005;135:269–81. doi: 10.4414/smw.2005.10985. [DOI] [PubMed] [Google Scholar]
- 30.Shah MJ, Jones TK, Cecchin F. Improved localization of right- sided accessory pathways with microcatheter-assisted right coronary artery mapping in children. J Cardiovasc Electrophysiol. 2004;15:1238–43. doi: 10.1046/j.1540-8167.2004.04100.x. [DOI] [PubMed] [Google Scholar]
- 31.Cappato R, Schlüter M, Weiss C et al. Radiofrequency current catheter ablation of accessory atrioventricular pathways in Ebstein’s anomaly. Circulation. 1996;94:376–83. doi: 10.1161/01.cir.94.3.376. [DOI] [PubMed] [Google Scholar]
- 32.Roten L, Lukac P, DE Groot N et al. Catheter ablation of arrhythmias in Ebstein’s anomaly: a multicenter study. J Cardiovasc Electrophysiol. 2011;22:1391–6. doi: 10.1111/j.1540-8167.2011.02161.x. [DOI] [PubMed] [Google Scholar]
- 33.Wu MH, Wang JK, Lin JL et al. Long-term outcome of twin atrioventricular node and supraventricular tachycardia in patients with right isomerism of the atrial appendage. Heart Rhythm. 2008;5:224–9. doi: 10.1016/j.hrthm.2007.10.010. [DOI] [PubMed] [Google Scholar]
- 34.Gatzoulis MA, Balaji S, Webber SA et al. Risk factors for arrhythmia and sudden cardiac death late after repair of tetralogy of Fallot: a multicentre study. Lancet. 2000;356:975–81. doi: 10.1016/S0140-6736(00)02714-8. [DOI] [PubMed] [Google Scholar]
- 35.Silka MJ, Hardy BG, Menashe VD, Morris CD. A population- based prospective evaluation of risk of sudden cardiac death after operation for common congenital heart defects. J Am Coll Cardiol. 1998;32:245–51. doi: 10.1016/s0735-1097(98)00187-9. [DOI] [PubMed] [Google Scholar]
- 36.Zeppenfeld K, Schalij MJ, Bartelings MM et al. Catheter ablation of ventricular tachycardia after repair of congenital heart disease: electroanatomic identification of the critical right ventricular isthmus. Circulation. 2007;116:2241–52. doi: 10.1161/CIRCULATIONAHA.107.723551. [DOI] [PubMed] [Google Scholar]