

Abstract
We conducted a prospective study to analyze whether ERCC1 rs11615 and rs3212986 and ERCC2 rs13181 and rs1799793 gene polymorphisms could serve as potential biomarkers for the prognosis of gastric cancer. A total of 228 patients with pathologically proven gastric cancer and receiving platinum-based chemotherapy were recruited from our hospital between October 2009 and October 2011. The ERCC1 rs11615 and rs3212986 and ERCC2 rs13181 and rs1799793 polymorphisms were genotyped using the polymerase chain reaction restriction fragment length polymorphism (PCR-RFLP) assay. Conditional logistic regression analysis revealed that patients carrying the CA and AA genotypes of ERCC1 rs3212986 polymorphism showed a poorer response to chemotherapy compared to the CC genotype (CA vs. CC: OR = 0.28, 95% CI = 0.06-0.98, P = 0.04; AA vs. CC: OR = 0.49, 95% CI = 0.06-0.98, P = 0.01). Moreover, the CA+AA genotype of ERCC1 rs3212986 polymorphism showed a significantly poorer response to chemotherapy (CA+AA vs. CC: OR = 0.49, 95% CI = 0.27-0.90). Patients with the AA genotype of ERCC1 rs3212986 polymorphism had a longer overall survival time when compared with the CC genotype (34.91 months vs. 51.19 months, log-rank P = 0.003). The AA genotype of ERCC1 rs3212986 polymorphism in gastric cancer patients was correlated with a higher risk of death from varying causes by the Cox proportional hazards model, compared to the CC genotype (HR = 6.19, 95% CI = 1.42-30.60). In conclusion, the ERCC1 rs3212986 polymorphism was found to influence the response to chemotherapy and overall survival of gastric cancer patients.
Keywords: ERCC1, ERCC2, polymorphism, gastric cancer, treatment outcome
Introduction
Almost one million new cases of gastric cancer were estimated to have occurred in 2012 (952,000 cases, 6.8% of the total), making it the fifth most common malignancy in the world, after cancers of the lung, breast, colorectum and prostate [1]. This represents a substantive change since the very first estimates in 1975 when gastric cancer was the most common neoplasm. More than 70% of cases (677,000 cases) occur in developing countries (456,000 in men, 221,000 in women), and half the world total occurs in Eastern Asia (mainly in China) [1]. Gastric cancer can be successfully treated if tumors are discovered early and removed surgically; however, most patients are diagnosed at a later stage. The development of valid therapies for advanced gastric cancer is fairly slow [2]. Systemic chemotherapy is the primary treatment for advanced gastric cancer, but generating resistance is a main cause of chemotherapy failure. Tumor-node-metastasis (TNM) stage and patients’ age is the most important prognostic factor for gastric cancer [3]. However, patients with similar TNM stage and patients’ age show different prognosis of gastric cancer, which suggest that genetic biomarkers may have a role in the prognosis of gastric cancer patients. Therefore, identification of genetic biomarkers could be helpful in designing individualized therapy, post-operational treatment and follow-up strategies.
NER plays an important role in the repair of various distorting helix-distorting lesions [4]. Excision repair cross complementation group 1 (ERCC1) and ERCC2 are two DNA repair genes, whose products are important in NER lie on chromosome 19q13.3. These two enzymes of this pathway are correlated with resistance to cisplatin chemotherapy, and the two gene polymorphisms are a part of an endonuclease complex. ERCC1 plays an important role in the DNA damage incision, and ERCC2 is involved in the damage unwinding process [5,6]. Alteration of NER capacity may influence the sensitivity to chemotherapy, and contribute to the individualized treatment outcome of several kinds of cancers, such as nasopharyngeal cancer, non-small cell lung cancer and ovarian cancer [7-9]. Several previous studies have reported the association between ERCC1 and ERCC2 gene polymorphisms and development of gastric cancer, but the results are inconsistent [7-10]. Therefore, we conducted a prospective study to analyze whether ERCC1 rs11615 and rs3212986 and ERCC2 rs13181 and rs1799793 gene polymorphisms could serve as potential biomarkers for prognosis of gastric cancer receiving platinum-based chemotherapy.
Materials and methods
Study population
A total of 266 patients with pathologically proven gastric cancer and receiving platinum-based chemotherapy were recruited from our hospital between October 2009 and October 2011. Patients who had primary tumors other than gastric cancer, tumors of an unknown origin or any histopathological diagnosis other than gastric cancer were excluded. Patients who had received preoperative radiotherapy or chemotherapy and had distant metastasis before participating into this study were excluded from the study group. Among these patients, 228 patients with gastric cancer agreed to participate in this study (participation rate = 85.71%). The signed informed consent forms were gained from all gastric cancer patients.
The demographic and clinical characteristics of the enrolled patients, including sex, age, histological classification, TNM stage, and lymphatic metastasis, were collected from the patient medical records.
The tumors were histopathologically classified based on Lauren’s classification. The TNM stage of gastric cancer was defined according to the 7th edition of the TNM staging system of the International Union Against Cancer (UICC)/American Joint Committee on Cancer (AJCC). The project was approved by the ethics committee of our hospital.
Assessment of clinical outcome
All 228 gastric cancer patients were treated with platinum-based chemotherapy, and the gastric cancer patients received chemotherapy treatment evaluation based on the RECIST criteria [11]. Gastric cancer patients who showed complete response (CR) or partial response (PR) to chemotherapy were considered as response to chemotherapy, while patients who showed stable disease (SD) or progressive disease (PD) were considered as non-response to chemotherapy. Gastric cancer patients were subjected to chemotherapy intervals of three weeks for up to six cycles, unless unacceptable toxicity levels were reached, or in case of disease progression. The event of our study was death from varying causes, and overall survival (OS) was used to describe the outcome variable. The OS was defined as the time from the beginning of study (January 2010) to death or the end of follow-up (October 2014).
Genotyping
Two milliliters of peripheral blood was collected from the patients prior to their treatment in EDTA-anticoagulant tubes. Genomic DNA was extracted from the blood, using the QIAamp DNA MAX Kit (Qiagen, Hilden, Germany). The ERCC1 rs11615 and rs3212986 and ERCC2 rs13181 and rs1799793 polymorphisms were assessed using the polymerase chain reaction restriction fragment length polymorphism (PCR-RFLP) assay. The following forward and reverse primers were used in this assay: rs11615: 5’-GCTGTGCACTCCAGTGGTTC-3’ and 5’-GTGGAGCTTGTTGAGGAGGT-3’; rs3212986: 5’-CAGAGACAGTGCCCCAAGAG-3’ and 5’-GGGCACCTTCAGCTTTCTTT-3’; rs13181: 5’-CCGTTCTGACTCCTGTCACC-3’ and 5’-CCCTCTCCCTTTCCTCTGTT-3’; rs1799793: 5’-CAGCTCATCTCTGCAGGATCAA-3’ and 5’-GTCTCAGGGTGCAGCACAAGGA-3’. The restriction enzymes for rs11615, rs3212986, rs13181 and rs1799793 were Tai I, Pvu II, Mbo II and Eco130I, respectively. The PCR conditions were set as follows: initial denaturation at 94°C for 8 minutes, followed by 30 cycles of denaturation at 94°C for 30 seconds, annealing at 60°C for 30 seconds, and extension at 72°C for 1 minute. The DNA fragments were confirmed via electrophoresis on a 3.5% agarose gel, which was subsequently visualized under UV light after staining with ethidium bromide.
Statistical analysis
The demographic and clinical data were expressed as number (N) and percentage (%). Conditional logistic regression analysis was used to evaluate the association between rs11615, rs3212986, rs13181 and rs1799793 polymorphisms and response to chemotherapy, and the results were shown as odds ratio (ORs) and corresponding 95% confidence intervals (95% CI). Cox proportional hazards model was taken to analyze the association between rs11615, rs3212986, rs13181 and rs1799793 polymorphisms and overall survival of gastric cancer patients, and the association was shown as the hazard ratio (HR) with a 95% CI. Survival curves were analyzed by the Kaplan-Meier method. Two-sided P values < 0.05 were considered to be statistically significant. Statistical analyses were performed on a statistical package SPSS 16.0 software platform (version 16.0, SPSS Inc., Chicago, IL, USA).
Results
The clinical and demographic characteristics of 228 patients with gastric cancer are summarized in Table 1. The mean age of the patients with gastric cancer was 56.65±11.52 years. There were 120 females (52.63%) and 108 males (47.37%) in our study. Of 228 patients with gastric cancer, 109 subjects (47.81%) had a tobacco smoking habit, 97 (42.54%) had alcohol drinking habit, 84 (36.84%) were intestinal type, 144 (63.16%) were diffuse type, 49 (21.49%) were at stage I-II and 179 (78.51%) were at stages III-IV. One hundred and fifty three patients (67.11%) showed CR+PR to chemotherapy, while 75 (32.89%) showed SD+PD to chemotherapy (Table 1).
Table 1.
Characteristics of patients with gastric cancer
| Characteristics | Patients with gastric cancer | % |
|---|---|---|
| Age, years | 56.65±11.52 | |
| <55 | 99 | 43.42 |
| ≥55 | 129 | 56.58 |
| Gender | ||
| Female | 120 | 52.63 |
| Male | 108 | 47.37 |
| Tobacco smoking | ||
| Never | 119 | 52.19 |
| Ever | 109 | 47.81 |
| Alcohol drinking | ||
| Never | 131 | 57.46 |
| Ever | 97 | 42.54 |
| Lauren’s classification | ||
| Intestinal | 84 | 36.84 |
| Diffuse | 144 | 63.16 |
| TNM stage | ||
| I-II | 49 | 21.49 |
| III-IV | 179 | 78.51 |
| Response to chemotherapy | ||
| CR+PR | 153 | 67.11 |
| SD+PD | 75 | 32.89 |
Association between ERCC1 rs11615 and rs3212986 and ERCC2 rs13181 and rs1799793 polymorphisms and response to chemotherapy in gastric cancer patients were shown in Table 2. Conditional logistic regression analysis revealed that patients carrying the CA and AA genotypes of ERCC1 rs3212986 polymorphism showed a poorer response to chemotherapy compared to the CC genotype (CA vs. CC: OR = 0.28, 95% CI = 0.06-0.98, P = 0.04; AA vs. CC: OR = 0.49, 95% CI = 0.06-0.98, P = 0.01). Moreover, the CA+AA genotype of the ERCC1 rs3212986 polymorphism showed a significantly poorer response to chemotherapy when compared with the CC genotype (CA+AA vs. CC: OR = 0.49, 95% CI = 0.27-0.90). However, we observed no significant association between the ERCC1 rs11615, ERCC2 rs13181 and rs1799793 polymorphisms and response to chemotherapy in patients with gastric cancer.
Table 2.
Association between ERCC1 and ERCC2 gene polymorphisms and response to chemotherapy
| SNPs | Patients | % | CR+PR | % | SD+PD | % | OR (95% CI)1 | P value |
|---|---|---|---|---|---|---|---|---|
| rs11615 | ||||||||
| TT | 106 | 46.49 | 75 | 49.02 | 31 | 41.33 | 1.0 (Ref.) | - |
| TC | 100 | 43.86 | 64 | 41.83 | 36 | 48.00 | 0.73 (0.39-1.37) | 0.3 |
| CC | 22 | 9.65 | 14 | 9.15 | 8 | 10.67 | 0.72 (0.25-2.21) | 0.51 |
| TC+CC | 122 | 53.51 | 78 | 50.98 | 44 | 58.67 | 0.73 (0.40-1.33) | 0.27 |
| rs3212986 | 0.00 | |||||||
| CC | 118 | 51.75 | 88 | 57.52 | 30 | 40.00 | 1.0 (Ref.) | - |
| CA | 99 | 43.42 | 60 | 39.22 | 39 | 52.00 | 0.52 (0.28-0.97) | 0.03 |
| AA | 11 | 4.82 | 5 | 3.27 | 6 | 8.00 | 0.28 (0.06-0.98) | 0.04 |
| CA+AA | 110 | 48.25 | 65 | 42.48 | 45 | 60.00 | 0.49 (0.27-0.90) | 0.01 |
| rs13181 | 0.00 | |||||||
| AA | 116 | 50.88 | 82 | 53.59 | 34 | 45.33 | 1.0 (Ref.) | - |
| AC | 83 | 36.40 | 54 | 35.29 | 29 | 38.67 | 0.59 (0.24-1.51) | 0.21 |
| CC | 29 | 12.72 | 17 | 11.11 | 12 | 16.00 | 0.59 (0.24-1.51) | 0.21 |
| AC+CC | 112 | 49.12 | 71 | 46.41 | 41 | 54.67 | 0.72 (0.40-1.30) | 0.24 |
| rs1799793 | 0.00 | |||||||
| GG | 125 | 54.82 | 87 | 56.86 | 38 | 50.67 | 1.0 (Ref.) | - |
| GA | 85 | 37.28 | 56 | 36.60 | 29 | 38.67 | 0.84 (0.45-1.59) | 0.57 |
| AA | 18 | 7.89 | 10 | 6.54 | 8 | 10.67 | 0.55 (0.18-1.73) | 0.23 |
| GA+AA | 103 | 45.18 | 66 | 43.14 | 37 | 49.33 | 0.78 (0.43-1.41) | 0.38 |
Adjusted for age, gender, Lauren’s classification, TNM stage and lymphatic metastasis.
At the end of the follow-up period, sixty one patients died from varying causes, and the five year survival rate of gastric cancer patients is calculated to be 73.25%. Patients with the AA genotype of ERCC1 rs3212986 polymorphism had a longer overall survival time when compared with the CC genotype (34.91 months vs. 51.19 months, log-rank P = 0.003) (Figure 1). The AA genotype of ERCC1 rs3212986 polymorphism in gastric cancer patients was correlated with a higher risk of death from varying causes by the Cox proportional hazards model, compared to the CC genotype (Table 3). The adjusted HR (95% CI) for the AA genotype versus the CC genotype of rs3212986 polymorphism was 6.19 (1.42-30.60) (P = 0.0025).
Figure 1.
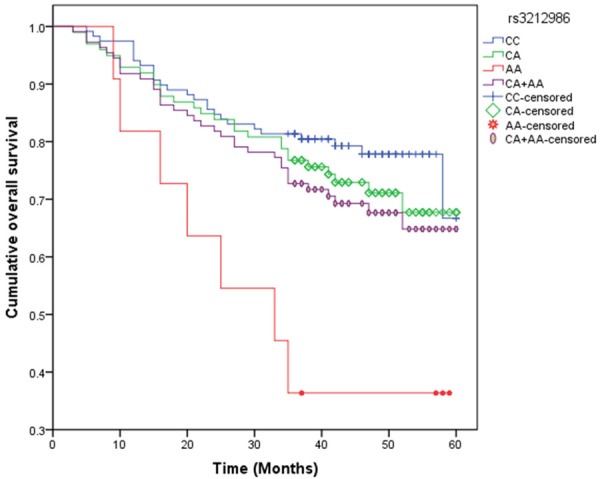
Kaplan-Meier survival curves by ERCC1 rs3212986 polymorphisms in gastric cancer patients.
Table 3.
Association between ERCC1 and ERCC2 gene polymorphisms and overall survival of gastric cancer
| SNPs | Mean survival, months | P value (log-rank) | Patients | % | Succumbed | % | Survived | % | HR (95% CI)1 | P value |
|---|---|---|---|---|---|---|---|---|---|---|
| rs11615 | 61 | 167 | ||||||||
| TT | 47.92 | 106 | 46.49 | 28 | 45.90 | 78 | 46.71 | 1.0 (Ref.) | - | |
| TC | 46.92 | 100 | 43.86 | 27 | 44.26 | 73 | 43.71 | 1.03 (0.53-2.00) | 0.92 | |
| CC | 45.71 | 22 | 9.65 | 6 | 9.84 | 16 | 9.58 | 1.05 (0.30-3.17) | 0.93 | |
| TC+CC | 46.11 | 0.42 | 122 | 53.51 | 33 | 54.10 | 89 | 53.29 | 1.03 (0.55-1.94) | 0.91 |
| rs3212986 | ||||||||||
| CC | 51.19 | 118 | 51.75 | 26 | 42.62 | 92 | 55.09 | 1.0 (Ref.) | - | |
| CA | 47.13 | 99 | 43.42 | 28 | 45.90 | 71 | 42.51 | 1.40 (0.72-2.71) | 0.29 | |
| AA | 34.91 | 11 | 4.82 | 7 | 11.48 | 4 | 2.40 | 6.19 (1.42-30.60) | 0.0025 | |
| CA+AA | 45.77 | 0.003 | 110 | 48.24 | 35 | 57.38 | 75 | 44.91 | 1.65 (0.87-3.12) | 0.09 |
| rs13181 | ||||||||||
| AA | 48.40 | 116 | 50.88 | 29 | 47.54 | 87 | 52.10 | 1.0 (Ref.) | - | |
| AC | 47.12 | 83 | 36.40 | 23 | 37.70 | 60 | 35.93 | 1.14 (0.58-2.28) | 0.67 | |
| CC | 45.93 | 29 | 12.72 | 9 | 14.75 | 20 | 11.98 | 1.35 (0.48-3.53) | 0.51 | |
| AC+CC | 46.64 | 0.39 | 112 | 49.12 | 32 | 52.46 | 80 | 47.90 | 1.20 (0.64-2.25) | 0.54 |
| rs1799793 | ||||||||||
| GG | 48.42 | 125 | 54.82 | 31 | 50.82 | 94 | 56.29 | 1.0 (Ref.) | - | |
| GA | 46.10 | 85 | 37.28 | 23 | 37.70 | 62 | 37.13 | 1.12 (0.57-2.20) | 0.71 | |
| AA | 44.54 | 18 | 7.89 | 7 | 11.48 | 11 | 6.59 | 1.93 (0.58-6.00) | 0.21 | |
| GA+AA | 45.20 | 0.07 | 103 | 45.17 | 30 | 49.18 | 73 | 43.71 | 1.25 (0.66-2.34) | 0.46 |
Adjusted for age, gender, Lauren’s classification, TNM stage and lymphatic metastasis.
Discussion
In the present study, we investigated the influence of ERCC1 and ERCC2 polymorphisms in DNA repair mechanisms on the treatment response and survival in gastric cancer patients treated with platinum-based chemotherapy. We found that the CA and AA genotypes of ERCC1 rs3212986 polymorphism were associated with response to chemotherapy, while the AA genotype of the ERCC1 rs3212986 polymorphism influenced both EFS and OS of gastric cancer patients.
The ERCC1 protein is a major component of the NER complex, acting as the rate-limiting enzyme in the NER pathway [12,13]. High expression of ERCC1 has been demonstrated to be correlated with poor response to chemotherapy because the ERCC1 protein influences the repair of platinum-induced DNA damage [14-17]. Platinum-based chemotherapy is a commonly used chemotherapeutic agent that exerts its cytotoxic effect mainly through formation of different kinds of DNA lesions, which could induce inter-strand and intra-strand cross-link generation, as well as DNA-protein cross-links, resulting in inhibition of cell growth and apoptosis of targeted cells unless repair [18]. DNA repair mechanisms may therefore play a very important role in response to platinum-based chemotherapy. Particularly NER enzymes are among the most important factors that can modify susceptibility to platinum-based chemotherapy, and contribute to interindividual differences in response between patients.
It is reported that ERCC1 enzyme involved in recognizing and removing platinum-induced intra-strand adducts in DNA, and this gene polymorphism was associated with resistant to platinum-based chemotherapy in various cancer, such as non-small cell lung cancer, gastric cancer, breast cancer, colorectal cancer and ovarian cancer as well as esophageal squamous cell carcinoma [19-25]. Kalikaki et al. have conducted a study in a Greek population, and they found that ERCC1 rs3212986 polymorphism contributed to the response to chemotherapy [19]. Zhou et al. conducted a study in a Chinese population, and they reported that ERCC1 rs3212986 polymorphism influenced the response to chemotherapy and overall survival of gastric cancer [20]. Palomba et al. reported that ERCC1 rs3212986 polymorphism may predict favorable prognosis in breast cancer patients undergoing a platinum-based treatment [22]. Chen et al. reported that ERCC1 rs3212986 polymorphism was significantly associated with survival of esophageal squamous cell carcinoma in a Chinese population [25]. However, some studies reported inconsistent results. Park et al. conducted a study in American population, and they reported that ERCC1 rs3212986 polymorphism could not predict the clinical outcome in advanced colorectal cancer patients [23]. Qi et al. conducted a study in a Chinese population, and reported that ERCC1 rs3212986 polymorphism did not contribute to the development of ovarian cancer patients treated with platinum-based chemotherapy [24]. The inconsistency results might be due to differences in ethnicities, source of patients, sample size, and by chance.
Two previous studies have reported the association between ERCC1 rs3212986 gene polymorphisms and treatment outcome of gastric cancer received platinum-based chemotherapy [26-28]. Xue et al. have reported that ERCC1 rs11615 and rs3212986 polymorphisms could affect the clinical outcome of patients with gastric cancer [26]. Another study in Chinese population found that the ERCC1 rs3212986 did not contribute to the response to chemotherapy and clinical outcome of patients with gastric cancer [27]. In our study, we suggested that the AA genotype of ERCC1 rs3212986 could influence the response to platinum-based chemotherapy and overall survival of gastric cancer patients, which is inconsistent with previous results. Further large sample studies are greatly needed to confirm our findings.
We identified three limitations in this study. First, patients were selected from one hospital, which suggests that the sample used by this study would not likely be representative of other populations. Therefore, selective bias may exist in this hospital. Second, the sample size of patients with gastric cancer was relatively small, which might limit the statistical power to find an association between groups. Third, the risk of gastric cancer might be modified by many other DNA repaired genes in addition to the ERCC1 and ERCC2 genes. Further studies with large sample size are greatly needed to verify the results of our study.
In conclusion, the ERCC1 rs3212986 polymorphism was found to influence the response to chemotherapy and overall survival of gastric cancer patients. These findings may be useful in predicting the clinical outcome of patients with gastric cancer. Further studies are required to confirm the clinical significance of these results.
Disclosure of conflict of interest
None.
References
- 1.International Agency for Research on Cancer. Stomach Cancer. Estimated Incidence, Mortality and Prevalence Worldwide in 2012. http://globocan.iarc.fr/Pages/fact_sheets_cancer.aspx.
- 2.Ohtsu A. Chemotherapy for metastatic gastric cancer: past, present, and future. J Gastroenterol. 2008;43:256–64. doi: 10.1007/s00535-008-2177-6. [DOI] [PubMed] [Google Scholar]
- 3.Washington K. 7th edition of the AJCC cancer staging manual: stomach. Ann Surg Oncol. 2010;17:3077–9. doi: 10.1245/s10434-010-1362-z. [DOI] [PubMed] [Google Scholar]
- 4.Costa RM, Chiganças V, Galhardo Rda S, Carvalho H, Menck CF. The eukaryotic nucleotide excision repair pathway. Biochimie. 2003;85:1083–99. doi: 10.1016/j.biochi.2003.10.017. [DOI] [PubMed] [Google Scholar]
- 5.Coin F, Oksenych V, Egly JM. Distinct roles for the XPB/p52 and XPD/p44 subcomplexes of TFIIH in damaged DNA opening during nucleotide excision repair. Mol Cell. 2007;26:245–56. doi: 10.1016/j.molcel.2007.03.009. [DOI] [PubMed] [Google Scholar]
- 6.Enzlin JH, Schärer OD. The active site of the DNA repair endonuclease XPF-ERCC1 forms a highly conserved nuclease motif. EMBO J. 2002;21:2045–53. doi: 10.1093/emboj/21.8.2045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Liang R, Lin Y, Liu ZH, Liao XL, Yuan CL, Liao SN, Li YQ. Correlation between ERCC1 expression and concurrent chemotherapy and radiotherapy in patients with locally advanced nasopharyngeal cancer. Genet Mol Res. 2015;14:5804–11. doi: 10.4238/2015.May.29.12. [DOI] [PubMed] [Google Scholar]
- 8.Shi ZH, Shi GY, Liu LG. Polymorphisms in ERCC1 and XPF gene and response to chemotherapy and overall survival of non-small cell lung cancer. Int J Clin Exp Pathol. 2015;8:3132–7. [PMC free article] [PubMed] [Google Scholar]
- 9.Xu Q, Ding YY, Song LX, Xu JF. Correlation of UGT1A1 and ERCC1 gene polymorphisms with the outcome of combined irinotecan plus cisplatin treatment in recurrent ovarian cancer. Genet Mol Res. 2015;14:7241–7. doi: 10.4238/2015.June.29.17. [DOI] [PubMed] [Google Scholar]
- 10.Xue MH, Li GY, Wu XJ, Zhang CX, Zhang CF, Zhu KX. Genetic variability of genes in NER pathway influences the treatment outcome of gastric cancer. Int J Clin Exp Pathol. 2015;8:5563–9. [PMC free article] [PubMed] [Google Scholar]
- 11.Duffaud F, Therasse P. New guidelines to evaluate the response to treatment in solid tumors. Bull Cancer. 2000;87:881–6. [PubMed] [Google Scholar]
- 12.Olaussen KA, Dunant A, Fouret P, Brambilla E, André F, Haddad V, Taranchon E, Filipits M, Pirker R, Popper HH, Stahel R, Sabatier L, Pignon JP, Tursz T, Le Chevalier T, Soria JC IALT Bio Investigators. DNA repair by ERCC1 in nonsmall- cell lung cancer and cisplatin-based adjuvant chemotherapy. N Engl J Med. 2006;355:983–91. doi: 10.1056/NEJMoa060570. [DOI] [PubMed] [Google Scholar]
- 13.Mamenta EL, Poma EE, Kaufmann WK, Delmastro DA, Grady HL, Chaney SG. Enhanced replicative bypass of platinum-DNA adducts in cisplatin-resistant human ovarian carcinoma cell lines. Cancer Res. 1994;54:3500–5. [PubMed] [Google Scholar]
- 14.Qiao H, Huang X, Guo H, Liu Y, Yue C. ERCC1, RRM1 and TUBB3 mRNA expression on the tumor response and overall survival of non-small cell lung cancer treated with platinum-based chemotherapy. Pak J Med Sci. 2014;30:1403–8. doi: 10.12669/pjms.306.5768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Zhang H, Li J, Zhang Y, Sun M, Zhao P, Zhang G, Jin C, Sun L, He M, Wang B, Zhang X. ERCC1 mRNA expression is associated with the clinical outcome of non-small cell lung cancer treated with platinum-based chemotherapy. Genet Mol Res. 2014;13:10215–22. doi: 10.4238/2014.December.4.16. [DOI] [PubMed] [Google Scholar]
- 16.Bonneau C, Rouzier R, Geyl C, Cortez A, Castela M, Lis R, Daraï E, Touboul C. Predictive markers of chemoresistance in advanced stages epithelial ovarian carcinoma. Gynecol Oncol. 2015;136:112–20. doi: 10.1016/j.ygyno.2014.10.024. [DOI] [PubMed] [Google Scholar]
- 17.Wang J, Zhou XQ, Li JY, Cheng JF, Zeng XN, Li X, Liu P. Prognostic significance of ERCC1 expression in postoperative patients with gastric cancer. Chin J Cancer Res. 2014;26:323–30. doi: 10.3978/j.issn.1000-9604.2014.06.07. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Rezaee M, Alizadeh E, Cloutier P, Hunting DJ, Sanche L. A single subexcitation-energy electron can induce a double-strand break in DNA modified by platinum chemotherapeutic drugs. ChemMedChem. 2014;9:1145–9. doi: 10.1002/cmdc.201300462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kalikaki A, Voutsina A, Koutsopoulos A, Papadaki C, Sfakianaki M, Yachnakis E, Xyrafas A, Kotsakis A, Agelaki S, Souglakos J, Mavroudis D, Georgoulias V. ERCC1 SNPs as Potential Predictive Biomarkers in Non-Small Cell Lung Cancer Patients Treated With Platinum-Based Chemotherapy. Cancer Invest. 2015;33:107–13. doi: 10.3109/07357907.2014.1001897. [DOI] [PubMed] [Google Scholar]
- 20.Zhou J, Liu ZY, Li CB, Gao S, Ding LH, Wu XL, Wang ZY. Genetic polymorphisms of DNA repair pathways influence the response to chemotherapy and overall survival of gastric cancer. Tumour Biol. 2015;36:3017–23. doi: 10.1007/s13277-014-2936-3. [DOI] [PubMed] [Google Scholar]
- 21.Yang Y, Luo X, Yang N, Feng R, Xian L. The prognostic value of excision repair cross-complementation group 1 (ERCC1) in patients with small cell lung cancer (SCLC) receiving platinum-based chemotherapy: evidence from meta-analysis. PLoS One. 2014;9:e111651. doi: 10.1371/journal.pone.0111651. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Palomba G, Atzori F, Budroni M, Ombra M, Cossu A, Sini M, Pusceddu V, Massidda B, Frau B, Notari F, Ionta M, Palmieri G. ERCC1 polymorphisms as prognostic markers in T4 breast cancer patients treated with platinum-based chemotherapy. J Transl Med. 2014;12:272. doi: 10.1186/s12967-014-0272-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Park DJ, Zhang W, Stoehlmacher J, Tsao-Wei D, Groshen S, Gil J, Yun J, Sones E, Mallik N, Lenz HJ. ERCC1 gene polymorphism as a predictor for clinical outcome in advanced colorectal cancer patients treated with platinum-based chemotherapy. Clin Adv Hematol Oncol. 2003;1:162–6. [PubMed] [Google Scholar]
- 24.Qi BL, Li Y, Wang N, Zhou RM, Hu P, Kang S. Polymorphisms of ERCC1 gene and outcomes in epithelial ovarian cancer patients with platinum-based chemotherapy. Zhonghua Fu Chan Ke Za Zhi. 2013;48:847–52. [PubMed] [Google Scholar]
- 25.Chen WH, Xin PL, Pan QX, Chen YY, Wang CR, Zhang ZS, Chen YF, Zhang CY, Cai WJ. ERCC1 single nucleotide polymorphism C8092A, but not its expression is associated with survival of esophageal squamous cell carcinoma patients from Fujian province, China. PLoS One. 2014;9:e106600. doi: 10.1371/journal.pone.0106600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Xue MH, Li GY, Wu XJ, Zhang CX, Zhang CF, Zhu KX. Genetic variability of genes in NER pathway influences the treatment outcome of gastric cancer. Int J Clin Exp Pathol. 2015;8:5563–5569. [PMC free article] [PubMed] [Google Scholar]
- 27.Yu H, Wu X, Zhang Y, Jin Z, Li G, Zhao H. Genetic variability of DNA repair mechanisms influences chemotherapy outcome of gastric cancer. Int J Clin Exp Pathol. 2015;8:4106–12. [PMC free article] [PubMed] [Google Scholar]
- 28.Yao A, Wang Y, Peng X, Ye R, Wang Q, Qi Y, Zhou F. Predictive value of excision repair crosscomplementation group 1 expression for platinum-based chemotherapy and survival in gastric cancer: a meta-analysis. J Cancer Res Clin Oncol. 2014;140:2107–2117. doi: 10.1007/s00432-014-1758-4. [DOI] [PMC free article] [PubMed] [Google Scholar]