

Abstract
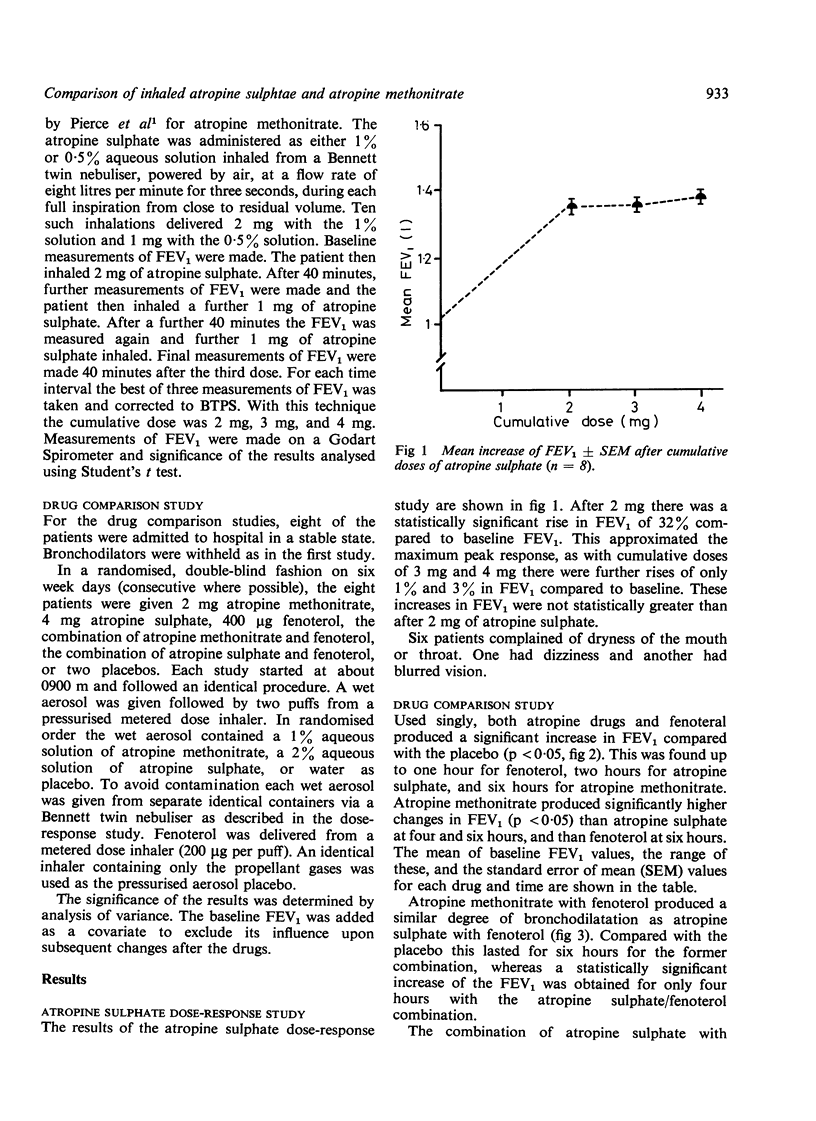
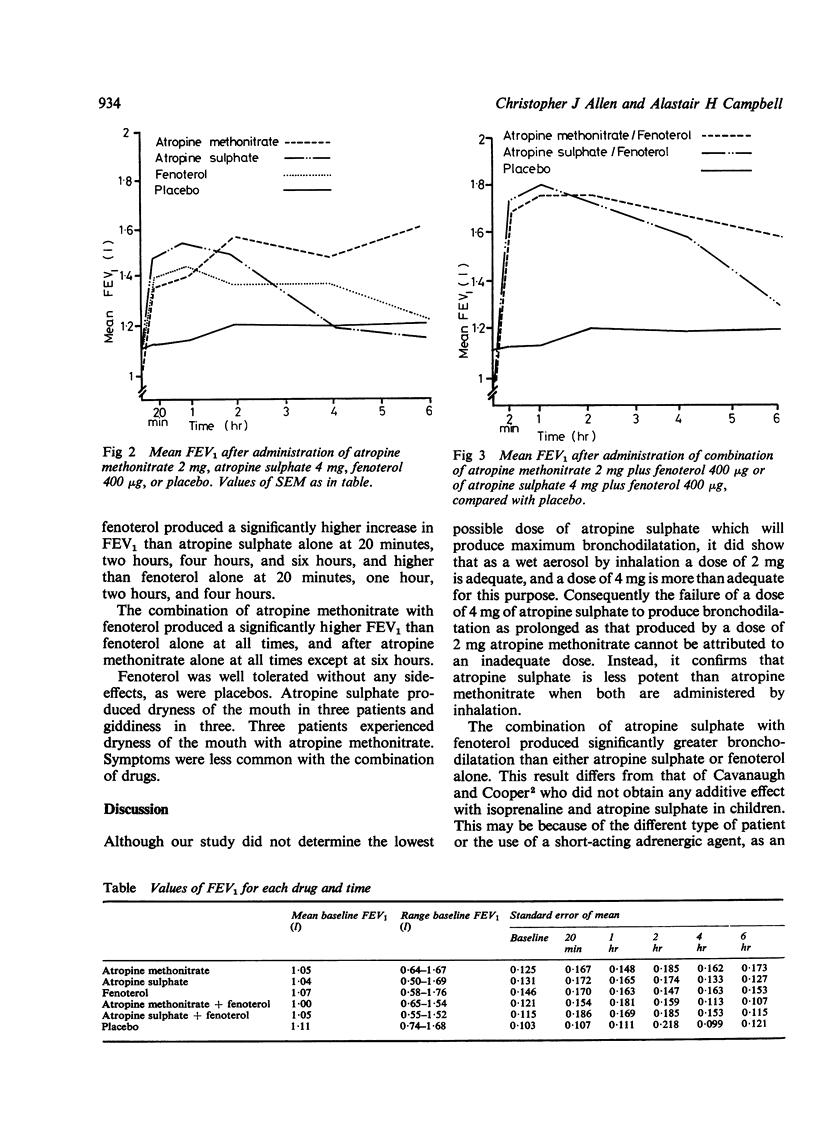
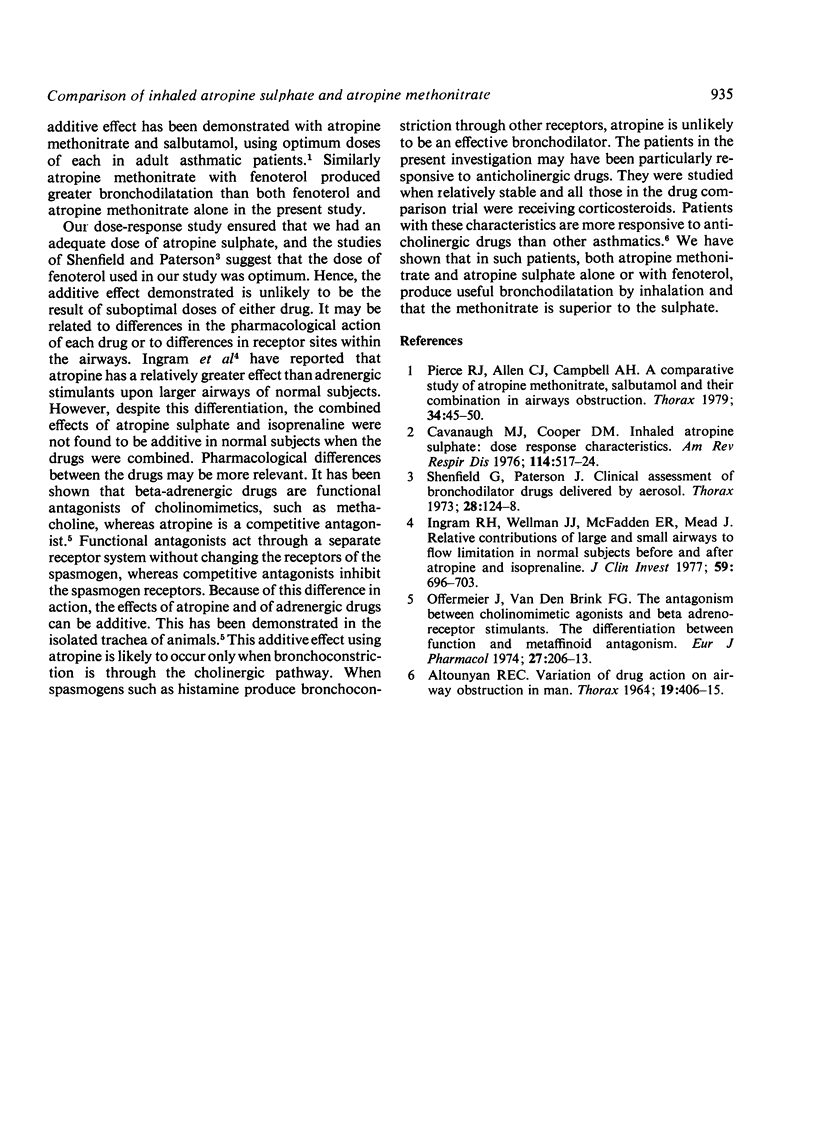
The bronchodilator potencies of inhaled atropine sulphate and atropine methonitrate have been compared either alone or in combination with fenoterol in a group of adult asthmatic patients. A cumulative dose response study showed that 2 mg of atropine sulphate produced near maximum bronchodilatation. A larger dose of 4 mg was used in comparing the potency of this drug with 2 mg of atropine methonitrate, a dose previously shown to produce optimum bronchodilatation. In a randomised double-blind fashion atropine methonitrate (2 mg), atropine sulphate (4 mg), fenoterol (400 μg), a combination of atropine methonitrate with fenoterol, a combination of atropine sulphate with fenoterol, and two placebos were administered by inhalation on separate days to eight stable adult asthmatics. Measurements of FEV1 were made before administration of the drugs and at 20 minutes, one, two, four, and six hours afterwards. The two atropine drugs produced a similar peak effect but the bronchodilatation after atropine methonitrate was more prolonged. In combination the bronchodilatation achieved with both atropine drugs and fenoterol was greater than with either atropine or fenoterol alone, confirming that atropine and an adrenergic drug can have an additive effect. The response with atropine methonitrate and fenoterol showed a significant increase in the FEV1 for six hours whereas with atropine sulphate and fenoterol the increase of FEV1 was significantly greater than the placebo for only four hours. It was concluded that the atropine drugs produce useful bronchodilatation either alone or in combination with an adrenergic agent. Of the two atropine drugs, the methonitrate appears to be superior to the sulphate as an inhaled bronchodilator in adult asthmatics.
Full text
PDF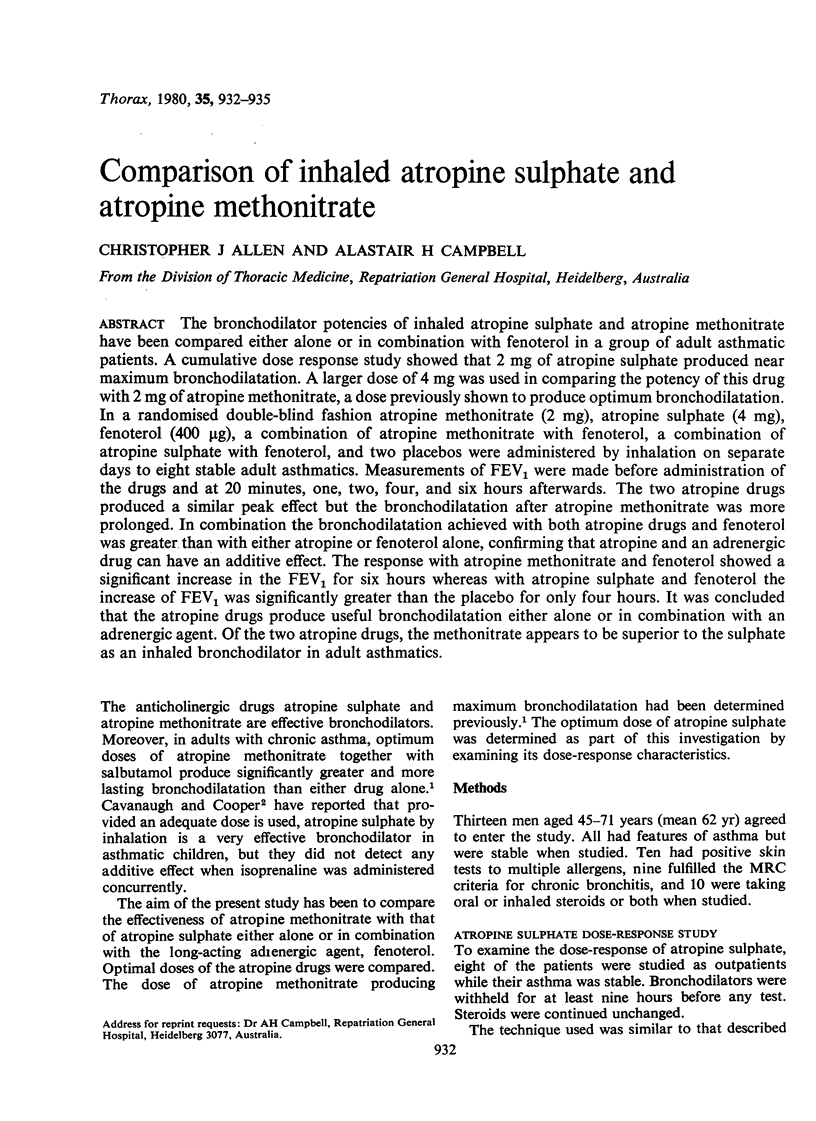
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- ALTOUNYAN R. E. VARIATION OF DRUG ACTION ON AIRWAY OBSTRUCTION IN MAN. Thorax. 1964 Sep;19:406–415. doi: 10.1136/thx.19.5.406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cavanaugh M. J., Cooper D. M. Inhaled atropine sulfate: dose response characteristics. Am Rev Respir Dis. 1976 Sep;114(3):517–524. doi: 10.1164/arrd.1976.114.3.517. [DOI] [PubMed] [Google Scholar]
- Ingram R. H., Jr, Wellman J. J., McFadden E. R., Jr, Mead J. Relative contributions of large and small airways to flow limitation in normal subjects before and after atropine and isoproterenol. J Clin Invest. 1977 Apr;59(4):696–703. doi: 10.1172/JCI108688. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Offermeier J., van den Brink F. G. The antagonism between cholinomimetic agonists and beta-adrenoceptor stimulants. The differentiation between functional and metaffinoid antagonism. Eur J Pharmacol. 1974 Jul;27(2):206–213. doi: 10.1016/0014-2999(74)90147-2. [DOI] [PubMed] [Google Scholar]
- Pierce R. J., Allen C. J., Campbell A. H. A comparative study of atropine methonitrate, salbutamol, and their combination in airways obstruction. Thorax. 1979 Feb;34(1):45–50. doi: 10.1136/thx.34.1.45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Shenfield G. M., Paterson J. W. Clinical assessment of bronchodilator drugs delivered by aerosol. Thorax. 1973 Mar;28(2):124–128. doi: 10.1136/thx.28.2.124. [DOI] [PMC free article] [PubMed] [Google Scholar]