

Abstract
We report an unusual case of benign tumor mimicking tumor recurrence following radical cystectomy and bladder replacement for high grade urothelial carcinoma.
Keywords: Mesenteric fibromatosis, Cystectomy, Urothelial carcinoma
Introduction
Following radical cystectomy, growing abdominal mass is usually suspected as tumor recurrence and should be accordingly approached. Nevertheless, benign abdominal tumors are still rarely encountered among which only one case of mesenteric fibromatosis following salvage cystectomy has been previously reported.1
In this report we present an unusual case of mesenteric fibromatosis mimicking tumor recurrence following radical cystectomy and bladder replacement for invasive urothelial carcinoma.
Case report
A 69 yr old gentleman was presented with high grade invasive urothelial carcinoma of the bladder.
He underwent radical cysto-prostatectomy followed by bladder replacement according to Mainz I technique with an appendiceal cutaneous stoma.
Pathological stage was PT2N0M0.
Operative and post-operative course were uneventful.
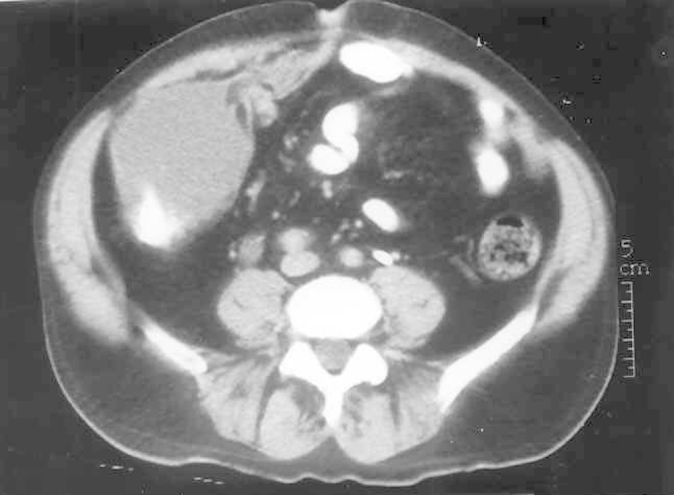
The patient was followed regularly at 6 months intervals with no evidence of recurrence. An abdominal CT scan performed 5 years postoperatively demonstrated left lower quadrant abdominal mass, located anterior to the reconstructed bladder, but without any linkage to it (Figure 1, Figure 2). Needle biopsy of the mass revealed a pseudosarcomatous fibromyxoid tumor. The mass appeared to grow significantly in repeat CT scan 3 months later and surgical exploration was suggested. At laparotomy a 15 cm in diameter mass was found, originating from the small bowel mesenterial root and involving a couple of terminal ileum loops at a total length of 50 cm. Complete removal was achieved. The neobladder and the cutaneous stoma were successfully preserved.
Figure 1.
A reconstructed urinary bladder according to Mainz I technique with an appendiceal stoma.
Figure 2.

An abdominal mass (denoted by arrow) that has no linkage to the reconstructed bladder.
No enlarged lymph nodes were found and neither peritoneal spread nor parenchymal involvement were seen. The histopathological findings were consistent with mesenteric fibromatosis. Surgical margins were free. No recurrence was noted within a period of 5 years follow up.
Discussion
Mesenteric fibromatosis, a rare benign tumor, is a member of the fibromatoses family, which accounts for 2–4:100,000 cases per year.2
Fibromatoses, referred also as Desmoid tumors, tend to recur locally though it seldom metastasizes.1, 2, 3 Whenever intra-abdominal, fibromatoses are usually solitary and can be found in the small bowel mesentery (most commonly), gastro-hepatic ligament, transverse mesocolon and omentum.1, 4
Macroscopically they are solitary lesions, but can be multi-centric.1
Their cut surface is glistening pinky-white and whorled. Microscopically the tumors consist of well differentiated fibroblasts of uniform size with no evidence of mitotic activity. Inflammatory infiltration is absent. Cellularity and collagen content are variable (Fig. 3).2
Figure 3.
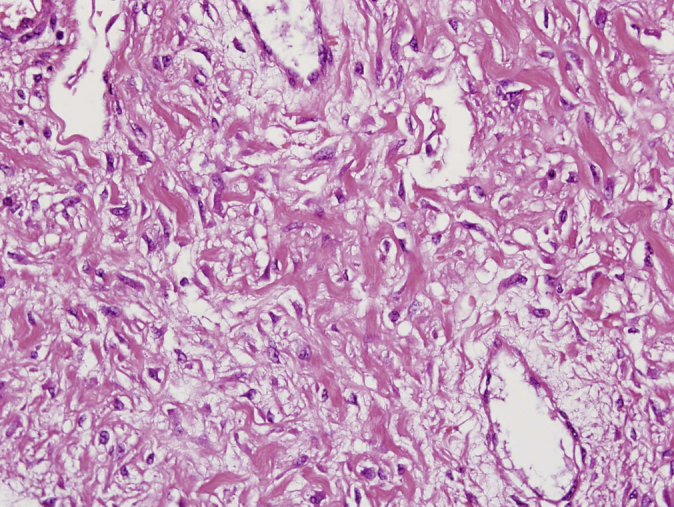
Mesenteric fibromatosis – hematoxylin and eosin stain.
Clinical symptoms vary from asymptomatic abdominal mass, vague abdominal discomfort or abdominal pain with or without weight loss.3, 4
Complications of fibromatoses include bowel obstruction and bowel perforation.2, 3
Ureteric compression and hydronephrosis, as a complication of an isolated mesenteric fibromatosis were also reported.5
The exact etiology is unknown. Conditions that were found to be in association with high incidence of mesenteric fibromatosis include Gardner's syndrome, especially following colectomies; pregnancy and surgical trauma.1, 2, 3
Surgical removal is the definitive treatment for mesenteric fibromatosis.1, 3
In case of surgical failure or non-resectable tumors, pharmacological treatment has been proposed using NSAIDs or an anti-estrogen receptors agents.2, 3
Radiotherapy or multidrug chemotherapeutic regimens such as Actinomycin D, Doxorubicine, Vincristine and Cyclophosphamide were also suggested,1, 3 however only partial success was gained in reducing or eradicating the tumoral mass.
Although benign in nature, mesenteric fibromatosis tends to recur, thus careful attention and a long term follow up are required.
Conclusion
Abdominal mass following radical cystectomy for invasive urothelial carcinoma should always be suspected for tumor recurrence, yet the differential diagnosis also consists of benign conditions mimicking recurrence but are not life threatening.
Conflict of interest
None declared.
References
- 1.Pasciak R.M., Kozlowski J.M. Mesenteric desmoid tumor presenting as an abdominal mass following salvage cystectomy for invasive bladder cancer. J Urol. 1987;138:145–146. doi: 10.1016/s0022-5347(17)43026-6. [DOI] [PubMed] [Google Scholar]
- 2.Suarez V., Hall C. Mesenteric fibromatosis. Br J Surg. 1985;72:976–978. doi: 10.1002/bjs.1800721214. [DOI] [PubMed] [Google Scholar]
- 3.Al-Jadaan S.A., Al Rabeeah A. Mesenteric fibromatisis: case report and literature review. J Pediatr Surg. 1999;34:1130–1132. doi: 10.1016/s0022-3468(99)90583-3. [DOI] [PubMed] [Google Scholar]
- 4.Forte M.D., Brant W.F. Spontaneous isolated mesenteric fibromatosis. Dis Colon Rectum. 1988;31:315–317. doi: 10.1007/BF02554369. [DOI] [PubMed] [Google Scholar]
- 5.Hailemariam S., Jaeger P., Goebel N., Grant J.W. Mesenteric fibromatisis with ureteric stenosis. Postgrad Med J. 1988;64:79–81. doi: 10.1136/pgmj.64.747.79. [DOI] [PMC free article] [PubMed] [Google Scholar]