

Abstract
Background:
Establishing individual identification of a decedent only by dental means is a mammoth task in forensic odontology. Palatal rugae's uniqueness, its resistance to heat, and stability throughout life have been proved by its use as an alternative aid in individual identification where comparison of fingerprints and other records is difficult.
Aims and Objectives:
The aim of the present study was to analyze the role of palatal rugoscopy in personal identification and sex determination of Nalgonda pediatric population.
Materials and Methods:
The study group consisted of 100 children having mixed dentition within the age range of 8–11 years, residing in Nalgonda district. Palatal rugae pattern, shape of the incisive papillae, length of the median palatal raphae, and shape of the dental arches were analyzed using Chi-square and Mann-Whitney tests between males and females.
Results:
Wavy and curved patterns appeared to be most prevalent in both males and females but with no significant difference. The number of primary rugae in females and secondary rugae in males, on left side of the palate, was significantly more than their counterparts (P < 0.05). When rugae unification was observed, diverging type was significantly more in males than in females. Parabolic dental arch form, elliptical type of incisive papilla, and medium length of median palatal raphae was observed in majority of the subjects.
Conclusion:
The present study hypothesizes the uniqueness of the rugae in personal identification as no two palates showed similar type of rugae in either of the genders. The rugae pattern also contributes minimally towards sex determination as there was no significant difference observed between the two variables.
Keywords: Human identification, palatal rugoscopy, pediatric population, sex determination
Introduction
Human identification in postmortem scenarios is fundamental and achieving it by dental or any other means is one of the most challenging task. Forensic odontology is a unique discipline dealing with evidence related to dental and oral structures. Although the literature is replete with the use of teeth in forensic investigations, use of other methods such as palatal rugae patterns, lip prints, and bite marks were also reported. Palatal rugae are considered to be equipotent with fingerprints and bite marks, for individual identification in medico-legal investigations.
Palatal rugae or transverse palatine folds are asymmetrical and irregular elevations of the mucosa located in the anterior third of the palate, arranged in transverse direction from palatine raphae located in midsagittal plane. Rugae are protected from trauma by their internal position in the head, and they are insulated from heat by the tongue and the buccal fat pads.[1] Palatal rugoscopy, the study of palatal rugae, can be used with expediency in cases like decomposed and burned bodies where fingerprints are unavailable.[2]
Sassouni stated that no two palates are alike and are constant even during growth.[3] The abiding nature of palatal rugae and its uniqueness[1,4,5] has led us to undertake the following study with the principal objective of evaluating its role in establishing individual identity and sex determination among Nalgonda pediatric population, since such studies have seldom been carried out in children.
Materials and Methods
A total of 100 children (50 males and 50 females), within the age-group of 8–11 years were randomly selected and included in the present study after complete oral examination in the Department of Pedodontics and Preventive Dentistry, Kamineni Institute of Dental Sciences, Narketpally, Nalgonda. Children having mixed dentition and absence of proximal carious lesions on teeth were included. Subjects with congenital abnormalities, bony and soft tissue protuberances, active lesions, scars, trauma to the palate, and those undergoing interceptive orthodontic procedures were excluded.
This study was conducted after obtaining the institutional ethical committee clearance and informed written consent from the subjects or parents of the selected sample. Alginate impressions of maxillary arches were made using appropriate perforated metal trays and the casts were prepared using dental stone devoid of air bubbles especially in the anterior third of the palate. The individual palatal rugae were then delineated using sharp graphite pencil on dental casts, under adequate light [Figure 1].
Figure 1.

Delineation of palatal rugae pattern on dental casts
Variables studied were:
Palatal rugae
The palatal rugae pattern was recorded according to the classification given by Lysell, 1955;[4] Thomas and Kotze, 1983;[6] and Kapali, 1997.[7] These classifications include length, unification, and shape of rugae, respectively.
Incisive papilla
The shape of the incisive papilla was evaluated as elliptical, triangular, or thin (thin and narrow shape).[8]
Median palatal raphae
The median palatal raphae was recorded as short (S), medium (M), or long (L) according to Filho IEM et al. (2009).[8]
Dental arch shape
The dental arch was assessed and classified according to Testut, 1944,[9] which include:
Hyperbolic
When the dental arch segments are divergent throughout their perimeter.
Parabolic
When the dental arch segments are divergent, yet in a less marked manner.
Epsilon
When the dental arch segments are parallel to each other.
Elliptical
When the dental arch segments are convergent.
Comparison of the number, shape, and length of palatal rugae on either sides of the palate along with the shape of incisive papilla, length of the median palatal raphae, and dental arch form were analyzed between males and females using Chi-square and Mann-Whitney U tests.
Results
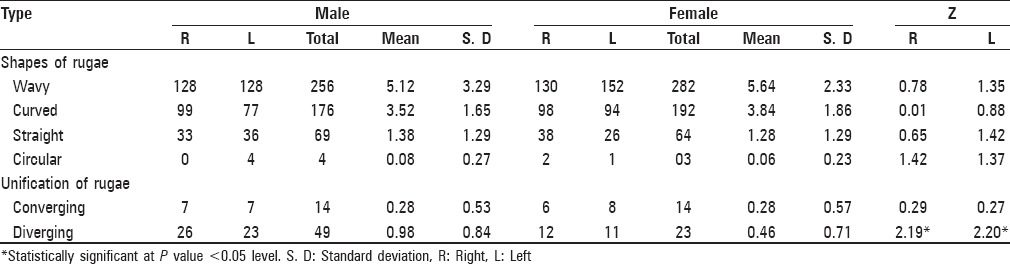
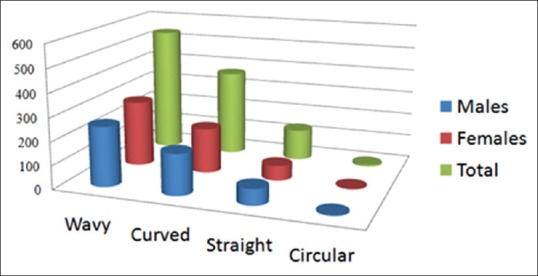
The total number of rugae was more on the right side of the palate in both males and females than on the left side with numbers greater in males than in females, but with no significant difference [Table 1]. The predominant rugae shape in both males and females were wavy patterns followed by curved, then straight, and circular. More number of wavy and curved types of rugae was observed in females than in males [Figure 2]. When unification of the rugae was analyzed, diverging type was higher in number than converging type, in both males and females on both sides of the palate. However, the total number of diverging rugae was more in males than in females with statistical significance (P < 0.05) [Table 2].
Table 1.
Distribution of total number of rugae pattern in both the genders
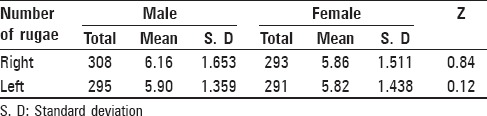
Figure 2.
Distribution of various shapes of palatal rugae
Table 2.
Distribution of different types of rugae in males and females
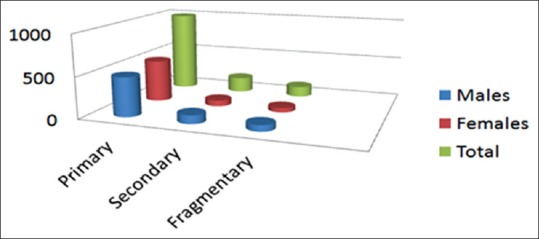
On observing the length of the rugae, primary rugae appeared to be most prevalent than secondary and fragmentary types in either of the genders. The number of primary rugae in females and secondary rugae in males was significantly more than their counterparts. (P < 0.05) [Table 3 and Figure 3].
Table 3.
Distribution of rugae length in males and females

Figure 3.
Distribution of various lengths of rugae
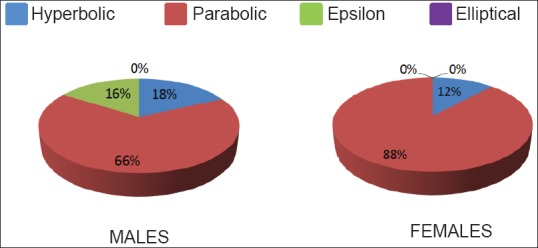
The most common dental arch form was found to be parabolic type followed by hyperbolic and epsilon types. None of the sample had elliptical type of dental arch form [Figure 4].
Figure 4.
Percentage distribution of dental arch forms
Elliptical type of incisive papilla was found to be most pronounced followed by triangular and thin or narrow types [Figure 5]. On evaluating the length of the median palatal raphae, medium type was observed in most of the subjects followed by long and short types [Figure 6]. None of the variables showed statistically significant difference between males and females except for the number of primary, secondary, and diverging types of rugae.
Figure 5.
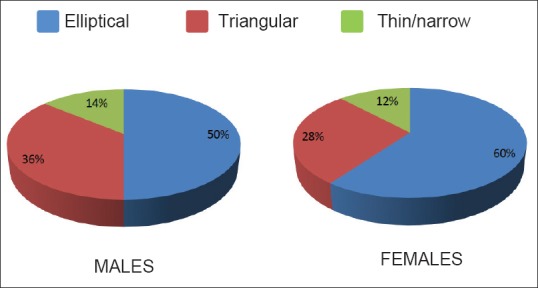
Percentage distribution of types of incisive papillae
Figure 6.
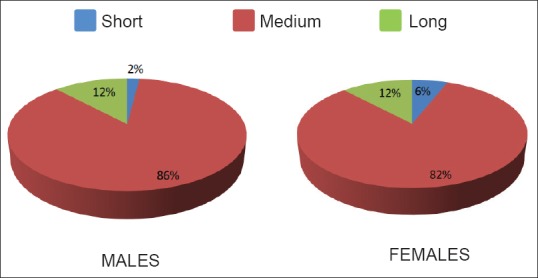
Percentage of extent of the median palatal raphae in males and females
Discussion
The traditional methods for human identification include anthropometry, fingerprints, dental records, gender determination, age estimation, weighing, identifying by specific characteristics, and blood-group differentiation.[8] Among these, the most accurate means of identification are fingerprints followed by dental records, which is the second most reliable method. In Forensic odontology, teeth restorations, bony protuberances, and palatal rugae present a vast majority of individual details.
Palatoscopy was first suggested by Harrison Allen (1889)[10] as an alternate method of identification. Palatal rugae was first described by Winslow (1753),[11] and the earliest illustration of them was given by Santorini (1775).[12] The anatomical position of the rugae inside the mouth, surrounded by cheeks, lips, tongue, buccal pad of fat, teeth, and bone keeps them well protected from trauma and high temperatures. Thus, they can be used as a reference landmark in forensic identification.[13]
The first system of classification was developed by Goria (1911)[14] and was rudimentary. In 1955, Lysell classified rugae comprehensively including incisive papilla, later it was modified by Thomas and Kotze in 1983 and Kapali et al. (1997), which included unification and cross-linking and shape of the rugae.
Sognnaes[15] advocated the use of dental casts from jaws rather than from dentures for a more reliable result. Jacob and Shaila[16] reported 100% accuracy from the tracings of entire cast and 79% accuracy with palatine rugae. Limson and Julian[17] evaluated the photographs of delineated rugae patterns of the cast using a computer software program and reported digitized rugae patterns matched the patterns in the stored records with highest sensitivity and specificity. In our study, we have used dental stone casts for recording the rugae pattern, incisive papilla, and median palatal raphae as it provides three-dimensional view in delineating all the selected variables.
In the present study, the number of rugae was slightly more in males than in females with no significant difference observed on both sides of the palate. These results were in accordance with the findings of Shetty M et al. (2011);[18] Bharat ST et al., (2011);[19] and Indira AP et al. (2012).[20] However, the right side of the palate had higher number of rugae than on the left side without any statistical significance. These observations were in agreement with the reports given by Indira AP et al. (2012). In contrast, Dhoke and Usato (1994);[21] and Surekha R et al. (2012)[22] reported that the right side of the palate had fewer rugae than the left side.
On observing the shape of the rugae, the present study revealed that the wavy pattern appears to be the most predominant pattern in both males and females followed by curved, straight, and circular pattern. Our results were similar with the findings reported by Abdellatif AM et al. (2011),[23] which was conducted in Egyptians and Saudi pediatric population groups. In Indian population, similar results were reported by Nayak P et al. (2007);[24] Kotrashetti et al. (2011);[25] Satish KN et al. (2012);[26] Surekha R et al. (2012), and in Australian Aborigines and Caucasian population by Kapali et al. (1997). In contrast, Shetty SK et al. (2005)[27] revealed that Indian males had more curved pattern and Tibetan females had wavier pattern than their counterparts.
When unification of rugae was analyzed in both males and females, diverging type was more common than converging type with more number seen in males than in females, with no significant difference. In contrast, Fahmi FM et al. (2001),[28] observed that Saudi females had more converging rugae than males. Whereas, Shetty SK et al. (2005); Shetty M (2011); and Surekha R (2012) reported that unification of rugae did not show any specific trend.
On analyzing the length of the palatal rugae, females had significantly higher number of primary rugae than males, whereas secondary rugae were significantly more in males. Similarly, Shetty SK et al. (2005) reported that Mysorean males and Tibetan females had more number of primary rugae than their respective counterparts. In contrast, Shetty M and Premalatha K (2011) reported that the number of primary rugae did not show any significant difference among the genders.
The present study revealed that most dental arches were parabolic followed by hyperbolic and elliptical shapes, which differs with the findings of Filho IME et al. (2009) who reported highest distribution of hyperbolic dental arches followed by parabolic and elliptical shapes.
Variation of rugae pattern, number, and orientation exist not only among people but also to a lesser extent—in the right and left sides of the same person. In general, no bilateral symmetry exists in the rugae pattern,[29] which is similar with the results of our study.
In this study, significant difference was observed in two variables between males and females. Based on this, palatal rugoscopy can be documented as an adjunctive investigatory aid in sex determination. Similarly, Saraf A et al. (2011)[30] reported palatoscopy as a useful tool in sex determination. In contrary, Kumar S et al. (2012) suggested it as an inefficient tool for sex determination.
The results of the present study conducted in Nalgonda children were discussed with references of all age-groups as literatures on pediatric population is limited.
Conclusion
Palatal rugoscopy is one of the pragmatic methods of human identification in the decree of justice. Rugae pattern, incisive papilla, median palatal raphae, as well as dental arch form was found to be unique to each individual as neither two sides of the palate nor two palates were alike. Thus, palatoscopy might be a useful fact-finding aid in forensic odontology. Wavy shape of the rugae, elliptical incisive papilla, medium length of the median palatal raphae, and parabolic dental arch form were found to be most predominant in Nalgonda pediatric population. Based on the significant differences observed in two variables between males and females, palatoscopy may be useful as an adjunctive aid in sex determination. Within the limitations of the present study, the authors consider the above interpretations to be taken as preliminary data as it was carried out in a small sample. We, thus presume that examination of large samples in detail would be beneficial to further substantiate our present findings and to reach an unambiguous conclusion.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.English WR, Robinson SF, Summitt JB, Oesterle LJ, Brannon RB, Morlang WM. Individuality of human palatal rugae. J Forensic Sci. 1988;33:718–26. [PubMed] [Google Scholar]
- 2.Caldas IM, Magalhaes T, Afonso A. Establishing identity using cheiloscopy and palatoscopy. Forensic Sci Int. 2007;165:1–9. doi: 10.1016/j.forsciint.2006.04.010. [DOI] [PubMed] [Google Scholar]
- 3.Sassouni V. Palato print, physioprint and roentgenographic cephalometry as new methods in human identification (Preliminary report) J Forensic Sci. 1957;2:428–42. [Google Scholar]
- 4.Lysell L. Plicae palatinae transversae and papillae incisiva in man; a morphologic and genetic study. Acta Odontol Scand. 1955;13:135–7. [PubMed] [Google Scholar]
- 5.Harrison A. The palatal rugae in man. Proc Acad Nat Soc. 1889;6:245. [Google Scholar]
- 6.Kapali S, Townsend G, Richards L, Parish T. Palatal rugae pattern in Australian Arborigines and Caucasians. Aus Dent J. 1997;42:129–33. doi: 10.1111/j.1834-7819.1997.tb00110.x. [DOI] [PubMed] [Google Scholar]
- 7.Thomas CJ, Kotze TJ. The palatal rugae pattern: A new classification. J Dent Assoc S Afr. 1983;38:153–7. [PubMed] [Google Scholar]
- 8.Filho EM, Helena SP, Arsenio SP, Suzana MC. Palatal rugae patterns as bioindicator of identification in forensic dentistry. RFO. 2009;14:227–33. [Google Scholar]
- 9.Testut L. Barcelone: S alvat Editores; 1944. Tratado de Anatomia Humana. [Google Scholar]
- 10.Allen H. The palatal rugae in man. Dent Cosm. 1889;31:66–80. [Google Scholar]
- 11.Winslow JB. Exposition anatomique de la structure du corps humain. 1732;4:681. [Google Scholar]
- 12.Santorini JD. Septeemdecim Tabulae. Parmae. 1775 [Google Scholar]
- 13.Patil MS, Patil SB, Acharya AB. Palatine rugae and their significance in clinical dentistry: A review of the literature. J Am Dent Assoc. 2008;139:1471–8. doi: 10.14219/jada.archive.2008.0072. [DOI] [PubMed] [Google Scholar]
- 14.Goria C. Lysell L, editor. Le rughe del palato in speciale rapporto coll anthropolgia criminale e la psichiatria. 1911. Plicae palatinae transerversae and papilla incisiva in man Acta Odontol Scand. 1955;13:5–137. [PubMed] [Google Scholar]
- 15.Sognnaes RD. Forensic stomatology (third of three parts) N Engl J Med. 1977;296:197–203. doi: 10.1056/NEJM197701272960405. [DOI] [PubMed] [Google Scholar]
- 16.Jacob RF, Shalla CL. Postmrtem identification of edentulous deceased: Denture tissue surface anatomy. J Forensic Sci. 1987;32:698–702. [PubMed] [Google Scholar]
- 17.Limson KS, Julian R. Computerized recording of the palatal rugae pattern and an evaluation of its application in forensic identification. J Forensic Odontostomatol. 2004;22:1–4. [PubMed] [Google Scholar]
- 18.Shetty M, Premalatha K. Study of palatal rugae pattern among the student population in Mangalore. J Indian Acad Forensic Med. 2011;33:112–4. [Google Scholar]
- 19.Bharat ST, Kumar GR, Dhanapal R, Saraswathi T. Sex determination by discriminant function analysis of palatal rugae from a population of coastal Andhra. J Forensic Dent Sci. 2011;3:58–62. doi: 10.4103/0975-1475.92144. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Indira A, Gupta M, David MP. Usefulness of palatal rugae patterns in establishing identity: Preliminary results from Bengaluru city, India. J Forensic Dent Sci. 2012;4:2–5. doi: 10.4103/0975-1475.99149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Dhoke M, Osato S. Morphological study of the palatal rugae in Japanese. 1. Bialteral differences in the regressive evolution of the palatal rugae. JPN J Oral Biol. 1994;36:126–40. [Google Scholar]
- 22.Surekha R, Anila K, Reddy VS, Hunasgi S, RaviKumar S, Ramesh N. Assessment of palatal rugae patterns in Manipuri and Kerala population. J Forensic Dent Sci. 2012;4:93–6. doi: 10.4103/0975-1475.109896. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Abdellatif AM, Awad SM, Hammad SM. Comparative study of palatal rugae shape in two samples of Egyptian and Saudi children. Pediatric Dent J. 2011;21:123–8. [Google Scholar]
- 24.Nayak P, Acharya AB, Padmini AT, Kaveri H. Difference in the palatal rugae shape in two populations of India. Arch Oral Biol. 2007;52:977–82. doi: 10.1016/j.archoralbio.2007.04.006. [DOI] [PubMed] [Google Scholar]
- 25.Kotrashetti VS, Hollikatti K, Mallapur MD, Hallikeremath SR, Kale AD. Determination of palatal rugae patterns among two ethnic populations of India by logistic regression analysis. J Forensic Leg Med. 2011;18:360–5. doi: 10.1016/j.jflm.2011.07.007. [DOI] [PubMed] [Google Scholar]
- 26.Kumar S, Vezhavendhan N, Shanthi V, Balaji N, Sumathi MK, Vendhan P. Palatal rugoscopy among puducherry population. J Contemp Dent Pract. 2012;13:401–4. doi: 10.5005/jp-journals-10024-1158. [DOI] [PubMed] [Google Scholar]
- 27.Shetty SK, Kalia S, Patil K, Mahima VG. Palatal rugae pattern in Mysorean and Tibetan populations. Indian J Dent Res. 2005;16:51–5. [PubMed] [Google Scholar]
- 28.Fahmi FM, Al-Shamrani SM, Talic YF. Rugae pattern in a Saudi population sample of males and females. Saudi Dent J. 2001;13:92–5. [Google Scholar]
- 29.van der Linden FP. Changes in position of posterior teeth in relation to ruga points. Am J Orthod. 1978;74:142–61. doi: 10.1016/0002-9416(78)90081-7. [DOI] [PubMed] [Google Scholar]
- 30.Saraf A, Bedia S, Indrukar A, Degwekar S, Bhowate R. Rugae patterns as an adjunct to sex differentiation in forensic identification. J Forensic Odontostomatol. 2011;29:14–9. [PMC free article] [PubMed] [Google Scholar]