

Abstract
Background: Socioeconomic status and demographic factors, such as education, occupation, place of residence, gender, age, and marital status have been reported to be associated with obesity. We conducted a systematic review to summarize evidences on associations between socioeconomic factors and obesity/overweight in Iranian population.
Methods: We systematically searched international databases; ISI, PubMed/Medline, Scopus, and national databases Iran-medex, Irandoc, and Scientific Information Database (SID). We refined data for associations between socioeconomic factors and obesity/overweight by sex, age, province, and year. There were no limitations for time and languages.
Results: Based on our search strategy we found 151 records; of them 139 were from international databases and the remaining 12 were obtained from national databases. After removing duplicates, via the refining steps, only 119 articles were found related to our study domains. Extracted results were attributed to 146596 person/data from included studies. Increased ages, low educational levels, being married, residence in urban area, as well as female sex were clearly associated with obesity.
Conclusion: Results could be useful for better health policy and more planned studies in this field. These also could be used for future complementary analyses.
Keywords: Obesity, Socioeconomic factors, Iran
Introduction
The prevalence of obesity and its health adverse outcomes continues to rise worldwide with alarming rates in developed and developing countries (1-3). Obesity and overweight are con-sidered as one of the leading preventable causes of attributable morbidity and death world-wide (1, 4, 5).
Co-morbidities are either directly caused by increased weight or indirectly related to mech-anisms sharing a common cause such as unhealthy behaviors that are mostly affected by so-cio-economic factors (SEFs) and other related determinants (6).
Evidences revealed that substantial proportion of excess weight mortality intricately is asso-ciated with SEFs (6, 7). These findings suggest the importance of social inequalities effects on unhealthy behaviors (8, 9). It is noticeable that some modifiable lifestyle behaviors and factors relating to SEFs may influence these emerging health programs (10).
Recent evidences have shown that, in developing countries, the burden of obesity tend to shift toward some specific socioeconomic groups (2, 11, 12). Socioeconomic status and de-mographic factors, such as education, occupation, place of residence, gender, age, and marital status have been reported to be associated with excess weight (7). These patterns are mostly complex, dynamic, and may be differ between countries and sub-groups populations (11).
It is clear that decisions about the design, feasibility, planning, funding, implementation, and management of preventive or controlling programs require the most accurate and reliable evi-dence provided through related researches (3, 13-15). Health researchers, professionals and policy-makers call for valid evidences to monitor, prevent, and control of obesity problems (12, 13).
Despite priority of the problem, there is an evident gap in the related literature on these top-ics (1, 2, 15-18). This study aimed to assess the association between SEFs and obesi-ty/overweight in Iranian population. We followed a comprehensive approach to conducting an up-to-date systematic review and meta-analytic comparison of all available studies.
Methods
Search strategy
To assess papers on obesity and/or overweight and related socio-economic factors in Iranian population, the relevant empirical literature searched through several electronic databases, in-cluding: main domestic databases, Iran-Medex, Scientific Information Database (SID), Iran-doc, and also international databases including: PubMed and NLMGateway (for MED-LINE), Institute of Scientific Information (ISI), and SCOPUS. To obtain the most compre-hensive results, we searched these data sources using Medical Subject Headings (MeSH) terms, Emtree, and related equal Persian key words for Iranian databases. The references and citations of relevant articles were also assessed. There was no limitation on age, time and lan-guage (Table 1).
Table 1 . The Search strategy .
| Domain | Search strategy |
| Obesity/overweight | Search strategy in PubMed/Medline ("Body Mass Index"[Mesh] OR "Body Mass Index"[All Fields] OR "Overweight"[Mesh]) OR "Overweight"[All Fields] OR "Obesity"[Mesh] OR "Obesity"[All Fields] OR "Quetelet* Index"[ All Fields] AND ("Iran"[Mesh] OR "iran"[All Fields]) OR Iranian[All Fields] OR I.R.Iran[All Fields] OR "I.R Iran"[All Fields] OR ("persia"[MeSH Terms] OR "persia"[All Fields AND "humans"[MeSH Terms]) |
| Search strategy in ISI Web of Science | |
| Topic= ("Body Mass Index" OR "Overweight" OR "Obesity” OR "Quetelet* Index") AND (("Iran" OR Iranian OR I.R.Iran OR "persia") OR Address= (Iran)) | |
| Search strategy in Scopus | |
| (TITLE-ABS-KEY (Body Mass Index" OR "Overweight" OR "Obesity” OR "Quetelet* Index")) AND (TITLE-ABS-KEY (Iran OR Iranian OR I.R.Iran OR Persia) OR (AFFIL (Iran)) | |
| IranMedex, SID and Irandoc | |
| “Body Mass Index”, “BMI”, “Overweight”, “Obesity”, “Quetelet* Index”, “Chaghi”, “Shakhese tudeh e badani”, “ezafe vazn”, “Dore kamar” , in Persian language | |
| Socioeconomic factors | ((((((("Socioeconomic Factors"[Mesh] OR "Poverty"[Mesh]) OR "Social Class"[Mesh]) OR "Educational Status"[Mesh]) OR "Employment"[Mesh]) OR "Family Characteristics"[Mesh]) OR "Income"[Mesh]) OR "Occupations"[Mesh]) OR "Social Conditions"[Mesh] OR "Standard of Living"[All Fields] OR "living standard"[All Fields] OR "land tenure"[All Fields] OR "High-Income Population"[All Fields] OR "High Income Population"[All Fields] OR ("socioeconomic factors"[MeSH Terms] OR ("socioeconomic"[All Fields] AND "factors"[All Fields]) OR "socioeconomic factors"[All Fields] OR "inequality"[All Fields]) OR ("socioeconomic factors"[MeSH Terms] OR ("socioeconomic"[All Fields] AND "factors"[All Fields]) OR "socioeconomic factors"[All Fields] OR "inequalities"[All Fields]) |
| Geographic area | ((("iran"[MeSH Terms] OR "iran"[All Fields]) OR iranian[All Fields] OR I.R.Iran[All Fields] OR "persia"[MeSH Terms]) OR (("iran"[MeSH Terms] OR "iran"[All Fields]) OR iranian[All Fields] OR I.R.Iran[All Fields] OR persia[Title/Abstract])) OR (("iran"[MeSH Terms] OR "iran"[All Fields]) OR iranian[All Fields] OR I.R.Iran[All Fields] OR persia[Text Word]) |
Definitions
Overweight and obesity were defined as 25≤BMI<30 and BMI≤30, respectively (19). SEFs considered as social and economic factors that differentiate the individuals or groups within the social structure. These factors included the social and economic experiences and realities that help mold one's personality, attitudes, and lifestyle(20) (Table 2).
Table 2 . Socioeconomic factors' definitions .
| Socioeconomic factors | Classic Definition |
| Age group | Persons classified by age from birth (INFANT, NEWBORN) to octogenarians and older (AGED, 80 AND OVER). |
| Sex | The totality of characteristics of reproductive structure, functions, PHENOTYPE, and GENOTYPE, differentiating the MALE from the FEMALE organism. |
| Educational level | Educational attainment or level of education of individuals. |
| Marital status | A demographic parameter indicating a person's status with respect to marriage, divorce, widowhood, singleness, etc. |
| Occupation Income |
Crafts, trades, professions, or other means of earning a living. Revenues or receipts accruing from business enterprise, labor, or invested capital. |
| Residence characteristics | Elements of residence that characterize a population. They are applicable in determining need for and utilization of health services. |
| Urbanization | The process whereby a society changes from a rural to an urban way of life. It refers also to the gradual increase in the proportion of people living in urban areas. |
| Social condition | The state of society as it exists or in flux. While it usually refers to society as a whole in a specified geographical or political region, it is applicable also to restricted strata of a society. |
| Social class | A stratum of people with similar position and prestige; includes social stratification. Social class is measured by criteria such as education, occupation, and income. |
Study selection and eligibility criteria
We included all available related original and systematic review papers that met our search protocol criteria and excluded article with duplicate citation. Aim to study selection, at the first phase, a reviewer check out all searched titles. Non-relevant papers deleted and those were crossed research objectives’ were kept for more evaluation in the next level. In abstract review phase papers were evaluated, in more detailed, considering reported values or related indexes. In final step, remained papers exactly reviewed based on their full-text contents. When there were multiple publications on the same population, only the largest study or the main source of data was included.
Quality assessment and data extraction
The quality assessment and data extraction of eligible papers has been followed inde-pendently by two research experts and probable discrepancy between them resolved based on third expert opinion. Using Cohen’s kappa statistic, agreement of them in quality assessment was 0.92.
Quality assessment form has three parts: general information about the study, sampling qual-ity, and measurement quality. Each study had a unique code and its general information such as the name and characteristics of the corresponding author have been inserted at the top of the form. The sampling quality refers to response rate, sample size, and sampling design and the measurement quality includes type of measurement tools, and accuracy of measure-ment.The final decision was based on the total scores obtained by each paper in ranking scale of: excellent (13-19), good (6-12) or poor (≤ 5).Poor quality papers have been deleted and two other categories considered for data extraction processes.
Data were collected according to a standard protocol including the citation of paper, study design and setting, study year, participants and their recruitment, sex, age, reported Socio-economic Factors, OR (95% CI), main conclusions, and authors’ recommendations.
All included papers have been reviewed and the required information have been extracted and inserted in data extraction sheet. In brief, the data extraction sheet contains detailed in-formation on prevalence or mean, standard deviation, standard error of mean, RO (95% CI), sample size, age, sex, province/district of the country, year, coverage of the study (representa-tiveness), scope of study (rural/urban/both), and other related reported values.
Statistical analysis
The reported results are presented as Odds Ratio (OR) and 95% confidence interval (CI). For more precise comparison, the Odds Ratio (OR), Confidence Interval for 95% (CI 95%) were calculated for possible cases. Heterogeneity of reported values between studies was as-sessed by the Chi-square based Q test and I square statistics. The result of Q test was regard-ed to be statistically significant at P < 0.001. Due to severe heterogeneity among studies re-garding reported values, overall OR was estimated using random-effect meta-analysis model (using the Der-Simonian and Laird method) (21). Forest plot also was used to present result of meta-analysis schematically. The analyses were conducted using STATA 11 software.
Ethical considerations
Present study has been approved by the ethical committee of Tehran University of Medical Science. All of included studies in our review would be cited in all reports and all publica-tions of our study. Whenever we needed more information about a certain study, for obtain-ing required information, we contacted the corresponding author.
Results
We refined data for association between SEFs and obesity/overweight in Iranian popula-tion. Based on our search strategy we found 151 records; of them 139 were from international databases and the remaining 12 were obtained from national databases. After removing duplicates, via the refin-ing steps, only 119 articles were found related to our study domain. The flow diagram of the study selection process is shown in the Fig. 1.
Fig. 1 .
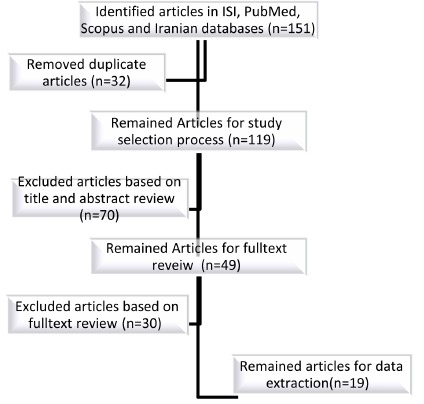
The flow diagram of the study selection process is shown in the
Table 3, shows the association of SEFs and obesity/overweight based on reported factors in eligible population-based studies. For more precise comparison, the OR and 95% confidence interval were calculated for possi-ble cases. We have also included studies’ methodology information. Table 4. The results of heterogene-ity test (I squares) and Estimated OR for related SEFs
Table 3 . The results of including papers on socioeconomic factors and obesity/overweight .
| No | Ref | Study design and Setting | Study year | Participants and their recruitment | Sex (F/M or B:both) | Age (Year) | Socioeconomic Factors | Reported values | Main Conclusion | Recommendations |
| 1 | Amani R. et al.(29) | Cross sectional, Population based/Ahvaz | 2003 | General Population, random sample/ n=637 | F | Mean ± sd: 26.9±5.8 ys (18–40 years) | educational levels |
educational levels illiterate (n =39) BMI:25.2±4.9 primary(n=242) BMI:26.6±4.9 secondary (n=217) BMI:25.8±4.7 higher (university) (n =139) 25±4.1 (p<0.02) |
Women with less educational grades tend to have more body fat. There was Significant difference between BMI and body fat of primary and higher educational levels (P<0.02). | Further studies on related fields with a greater number of subjects of different minority groups are needed. |
| 2 | Asgari F, et al.(30) | Cross sectional, Population based/ ( STEPs Survey) | 2009 | General Population, random sample/ n=20917 (51.8% female) | B | 20≤ years | age/ sex/ place of residence / employment status |
Obesity odds ratio
age
OR:30-40:2.48(2.20-2.80)
female sex:
OR:2.63:(2.32-2.78)
rural place of residence:
OR:1.46(1.33-1.61) Employment status: Other:1.00 Public employment:0.79(0.68-0.92) Private employment:0.76(0.60-0.99) |
OR of obesity went up with increasing age and then it decreased for ages above 50 years. men had lower BMI values than women Rural residents had higher odds of being obese compared with urban residents. Obesity may be more acceptable among unemployed people. | Results may provide better insights of the factors associated with obesity and can be used as a basis to reinforce health programs to prevent obesity in Iran. |
| 4 | Azizi F, et al.(31) | Cross sectional, Population based/ Tehran | 1999- 2001 | General Population, random sample/ n=15005 Tehranian children, adolescents, and adults, 44% males and 56% females. | B/F (56%) | Nearly, 5 % of the study population was between 3–6 years, 6 % between 7–10 years, 9% between 11–14 years, 19% between 15– 24 years, 17% between 25– 34 years, 16% between 35– 44 years, 12% between 45– 54 years, and 10% between 55– 64 years, and 7% over 64 years | sex | obesity was significantly higher in women than in men (29.5% vs 14.4 %, p < 0.001) the prevalence of overweight was greater in men than in women (42.5% vs 38.1%, p < 0.01). In adult population, the prevalence of central obesity (high WHR) was greater in women than in men (67.2% vs 33.0 %, p<0.001) Obes female:OR:2.72(2.42-3.07) Over weight female:OR:1.19(1.09-1.31) | More than 60% of adults in the present study were obese or overweight. Moreover, it is worth mentioning that more than 17% of the children and adolescents in our study suffered from obesity or overweight.. | The results suggest a need for special attention to health status in Tehranian children and adolescents. In case of comparing TLGS data w |
| 5 | Bakhshi E, et al.(32, 33) | Cross sectional, Populatio based/ National Health Survey (NHS) | 1999- 2000 | General Population, cluster-stratified sampling/ 2728 women and men 1364 | B/ F (50 %) | 20–75 (mean: 36.9 y) | age/ Economic Index / educational level/ residence / marital status | Obesity odds ratio Obesity odds ratio age OR: 1.02(1.00-1.05) education high education: 0.60 (0.37-0.7) residence in city 0.70(0.47-1.04) marital status Or:1.13(0.96-130) | Among women, factors that increased obesity included age, low education, Among men, these factors included high economic index, low education. |
better understanding of
the social and cultural
mechanisms of obesity in
couples. The preventive strategies based on the affective factors. |
| 6 | Behzadnia S, et al.(34) | Cross sectional, Population based/Sari | 2009- 2010 | General Population, multi-stage and stratified randomization /, n: 653 . | B/ F (55.5 %) | 7-12 | socio economic status | Economic Index female: 1.002 (0.99-1.01) male: 1.02 (1.01-1.04)Male vs. female: Active workforce:1.21(0.32-4.56) male vs. female: non active workforce: 0.40(0.16-1.00) Higher prevalence of obesity in the children with good socio economic status was found (p=0.001). | In children with moderate SES the prevalence of overweight was 23% (151) and in children with good SES it was 34.9% (227) (p = 0.001). | the need for serious attention to the issue of childhood obesity, performance of more extensive studies, identification of underlying factors precisely and designing the implementation of needed interventions. |
| 7 | Dastgiri S, et al.(35) | Cross sectional, Population based/ Tabriz | 2006 | General Population, Random sampling/ n:200 | B/ F (56%) | 18≤ | sex/ age/ education/ monthly income |
Obesity odds ratio
female sex
OR: 1.81 (0.96-2.66)
education
12+:0.41(0.31-0.63)
age
OR:2.29(1.96-2.99)
Monthly income Female Monthly income($US) ≤65:1 66-130:0.87(0.76-0.96) 131-220:0.72(0.62-0.81) ≥221:0.58(0.41-0.67) Male Monthly income($US) ≤65:1 66-130:0.75(0.62-0.93) 131-220:0.41(0.32-0.68) ≥221:0.32(0.24-0.53) |
Mean
BMI was significantly lower in men than in
women
(25.2 ^ 4.9 vs. 27.1 ^ 5.3 kg m
22
, P , 0.001). Total
prevalence of obesity in the area was 22.4%
(95% CI:
18.0–27.6), with 24% (95% CI: 18.5–31.4)
of women and
18% (95% CI: 12.5–25.6) of men being
obese. both women and men obesity prevalence showed a positive association with age (P for trend ,0.001), while there was a negative correlation of obesity with education and income (P for trend ,0.001). |
crucial necessity of establishing a population-based centre for obesity in the area. More population-based investigations on dietary choices are needed to develop effective preventive strategies to control overweight and obesity disorders in different regions. |
| 8 | Esmaeily H, et al.(16) | Cross sectional, Population based/ Great Khorasan | 2009 | General Population, Cluster-stratified sampling/ n: 4977 | B/ F ( 50.2%) | 15-65 | sex/ residence in city/ marital status | Obesity odds ratio ever married OR:3.50 (2.72-4.49) Residence in city 2.58(2.13-3.13) not high education(≤12y) OR:0.71(0.41-1.0.1) unemployed OR:2.30(1.92-2.76) Overweight odds ratio ever married OR:2.71 (2.29-3.21) Residence in city OR:1.80(1.57-2.05) not high education(≤12y) OR:0.89(0.77-1.03) unemployed OR:1.81(1.61-2.04) | Overweight and obese was significantly more prevalent among women than men and urban- compared to rural-dwellers. A high prevalence of overweight and obesity was seen among individuals who were divorced or widowed and among housewives, or individuals with poor education. Urbanization, age, illiteracy, female gender and divorced, or widowed status were significant predictors of obesity (p<0.001). | A community-based approach using multiple strategies including appropriate education will be required to address this problem |
| 9 | Hajian- Tilaki KO, et al. (36) | Cross sectional, Population based/ /Mazandran | 2004 | General Population, cluster sampling/ n:3600 | B/ F (50%) | 20–70 M: 38.5±14.3, F: 37.5±13.0) | education | Obesity odds ratio Obes high education(≥12y) OR:0.55(0.45–0.71) | The findings of this study indicate that education level is inversely associated with general obesity in both sexes but with abdominal obesity only in women. | Further studies are needed to explore lifestyle factors that are influenced or modified by education in men or women. |
| 10 | Janghorbani M, et al. (37) | National Crosssectional survey/ National | 2004- 2005 | General Population, stratified probability cluster sampling/ n:89440 | B/ F ( 60.8%) | 15-65 (Mean:39.2) | sex/marit al status | Obesity odds ratio ever married 3.64(3.31-3.99) | The marital status appears to influence the likelihood of developing overweight, obesity, and abdominal obesity in both sex ma | There is a need to assess the mechanisms for this association. |
| 11 | Shahraki M, et al. (38) | Cross sectional, Population based/ Sistan and Baluchestan Province | 2004- 2006 | General Population, random sampling/ n:888 | F | ≥20 | education/ marital status | Obesity odds ratio level of education university graduates OR:1.00 intermediary & high school OR:4.20(1.64-10.83) illiterate or low literacy OR:3.70(1.31-10.50) marital status Single OR:0.15(0.02-1.20) | Significant factors associated with obesity by a logistic regression model were education level (OR for university graduates v. illiterate or low literacy levels: 1.00 vs3.7 (P≤0.001), and OR for married v. single subjects: 1.00 vs.0.15; (P≤0.001) | Obesity prevention should be a relevant topic on the public health agenda in developing countries such as Iran. Without developing effective strategies to modify the current situation, it is likely that the obesity epidemic will continue in the future. |
| 12 | Tavassoli AA, et al. (39) | Cross sectional, Population based/ Islamshahr district | 2003 | General Population, random survey/n :1003 | F | 10-65 | place of residence/ education/ marital status | Obesity odds ratio Place of residence no sig diff Literacy ( year) 0-3 n:166 mean BMI 30(6.0) 4-7 n:288 mean BMI 28.4(5.7) 8≤ n:268 mean BMI 25.3(5.4) marital status OR:1.18(0.90-1.46) | The mean BMI was significantly higher in married women and in women with less than 8 years of formal education. The mean WHR was significantly higher in women with less than 8 years of education or with more than 6 parity female adults. | The prevention of overweight and obesity through a healthy diet and increased physical activity should now be an important priority area. |
| 13 | Nematy M, et al. (19) | Cross sectional, Population based/ Razavi-Khorasan Province :2000 | - | General Population, cluster random sampling/ /n | B/(917 m/1045 fe) | ≥60 years /70.2 ± 7.8 | sex/ education | Obesity odds ratio female sex OR:1.71 (1.43-2.07) illiterate vs literate OR:0.47(0.33-0.66) | Regression analysis results indicated that gender (p < 0.001), place of residence (p <0.001), literacy (p = 0.01), and source of income (p <0.001) were significantly associated with the incidence of overweight or obesity. This study showed that 40.6% of elderly subjects were overweight or obese. | Results reinforce the need to plan strategies for primary prevention of this fastgrowing public health problem. |
| 14 | Sotoudeh G, et al.(10) | Cross sectional, Population based/ / Isfahan, Najaf- Abad, and Arak | 2010 | General Population, random sampling/ n:12514 | B/(6,123 M, 6,391 F) | ≥19 38.89±14.93 y | Education/ inco me/ ownership of car/ job/ | Obesity odds ratio Urban vs rural residence OR:2.32 (1.86-2.86) education OR:0.37(0.26-0.41) married vs single OR:2.65(1.90-3.40) Family members >4 vs <4 OR:1.195(0.998-1.432) Income 25-75% vs <0.25% OR:1.134(0.906-1.418) Income >0.75% vs <0.25% OR:1.294(0.997-1.679) Ownership of car OR:2.044(1.711-2.442) Government job vs retired/not working OR:0.700(0.511-0.958) Private job vs retired/not working OR:0.599(0.482-0.744) | The results of the present study showed significant differences in some factors associated with obesity among men and women; such differences should be taken into account for interventional programmes at the individual level and for providing long-term public-health policies. | The association of different socioeconomic and lifestyle factors and their gender differences should be considered for culturallyappropriate intervention strategies to be implemented at the population level for tackling obesity and associated cardiometabolic risk factors. |
| 15 | Maddah M, et al. (40) | Cross sectional, Population based/ / Rasht | 2005 | General Population, multistage sampling method/ n:1054 | F | 14-17 | age | Obesity odds ratio Age group OR: 2.0( 0.18–3.09) | These data indicate that overweight is highly prevalent among adolescent girls, especially in lower social groups in Rasht, and the rate is exceeding those reported in other parts of the country. | Preventive strategies need to be adopted to combat the epidemic of overweight and obesity in this population. |
| 16 | Navadeh S,et al. (41) | Cross sectional, Population based/ /National | 2005 | General Population, random sampling/ n:36252 | F | 20-65 | Age/emp loyment/ residence place/ marital status/ education | Obesity odds ratio HWs vs. employed OR: 1.39 ( 1.18-1.63) ever married OR: 2.15(1.84-2.51) residence in urban OR:1.37(1.21-1.55) Low SEE OR :1.22(1.02-1.45) high education OR: 0.87(0.83-0.91) age OR:1.38(1.33-1.43) | HWs vs. employed women had the adjusted OR 1.39 (CI95%, 1.18-1.63) for obesity. Older women, with higher educational level and socioeconomic status and those living in urban areas were at risk of obesity. In comparison to HWs, working as an Official Clerk (OR=0.66) associated with a decrease in odds of obesity significantly, while others did not. | Being as HW is an independent significant factor for obesity in women. Preventive health care programs to reduce risk of obesity in women should be applied, considering their occupation for achieving more effectiveness. |
| 17 | Maddah M, etal.(42) | Cross sectional, Population based/ / Rasht | 2008 | General Population, ,random sampling/ n:4035 | B/(6028 M, 6223F) | F: 38.6±5.9 M: 43.1±6.4 years | education | Obesity odds ratio High Education OR:0.97(0.74-1.27) Overweight odds ratio High Education OR: 0.77(0.65-0.92) | These results highlight the importance of socioeconomic indicators in obesity research in Iran. Overall prevalence of overweight and obesity was positively related to educational level in men. The lowest rate of overweight/obesity was observed in very low educated men and very high educated women. | - |
Table 4 . The results of heterogeneity test (I squares) and Estimated OR for related SEFs .
| No | Variable | Practical definition | Number of studies | Model of metaanalyses | Estimated OR | 95% CI of OR | Results of heterogeneity test (I squares) |
| 1 | Sex | Female vs. male | 3 | Random-effect meta-analysis model | 2.06 | 1.45- 2.93 | 88.9%, p=0.00 |
| 2 | Age | 30< vs. ≤30 yo | 4 | Random-effect meta-analysis model | 1.66 | 1.24- 2.22 | 99.2%, p=0.00 |
| 3 | Marital status | Ever married vs. never married | 6 | Random-effect meta-analysis model | 2.14 | 1.36- 3.38 | 97.7%, p=0.00 |
| 4 | Education | High education (more than 12yos) vs. low education | 7 | Random-effect meta-analysis model | 0.60 | 0.43- 0.83 | 92.9%, p=0.00 |
| 5 | Living place | Urban vs. rural residence | 5 | Random-effect meta-analysis model | 1.58 | 1.18- 2.11 93.4%, | p=0.00 |
Considering the systematic review results, all included studies were cross-sectional ones. Eight articles were population-based studies and the others were clinical- and hospital-based. Regarding the geographic distribution, we found 4 national, 6 provincial, 5 community, and 1 district level studies. All participants were from general population. All of searched articles were in English or Persian language. Although, we haven't limit the search strategy on certain time; retrieving articles were between 1973 and 2014. Included articles were published be-tween 2002 and 2014 and the studies were conducted between 1999 and 2010. In general, these results were attributed to 146596 person/data from included studies. Excluding 5 stud-ies that focused on female sex, the remained studies covered both sex.
Only one study considered inequality assessment index about obesity. Based on first run of non-communicable disease surveillance study data (STEPs study, 2005) in Shahroud, concen-tration index for obesity was (0.038±0.036) for both sex. It was reported for female (-0.005±0.039) and male (0.194±0.070). It showed that obesity was more prevalent in men with high socioeconomic levels (22).
Other studies focused on different components of SEFs. The findings are scattered, with different ranges of values for Odds. On the other hand, non-standard classifications of SEFs led to greater complexity in estimation and comparability of the results. For instance, regard-ing the education, results have been presented as years of schooling through continue varia-bles or different frame of categorization of educational levels. This factor, only in three stud-ies has been reported by sex; among them the highest OR were reported for university edu-cated persons vs. primary education (for women 0.41(0.31-0.63) and men 1.2+:0.62(0.36-0.71)). Severe heterogeneity of overweight results, did not allow us to include them in meta-analyses.
The results of heterogeneity test (I squares) and estimated OR for related SEFs are present-ed in Table 4. Considering the severe heterogeneity among reported values, to overall estima-tion of OR, for possible variables, of SEFs, we used random-effect model.
Figs. 2-6 present the forest plot of eligible articles for estimating overall OR of obesity ac-cording to related SEFs in Iran.
Fig. 2 .
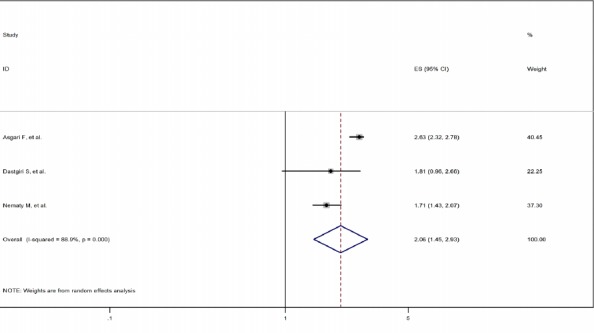
The forest plot of OR of obesity according to sex in Iran using random-effect mode
Fig. 6 .
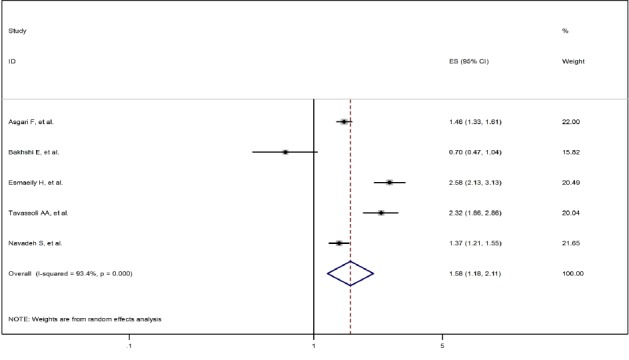
The forest plot of OR of obesity according to living place in Iran using random-effect mode
Fig. 3 .
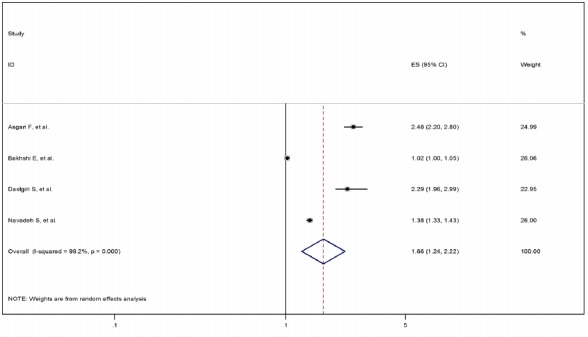
The forest plot of OR of obesity according to age in Iran using random-effect mode
Fig. 4 .
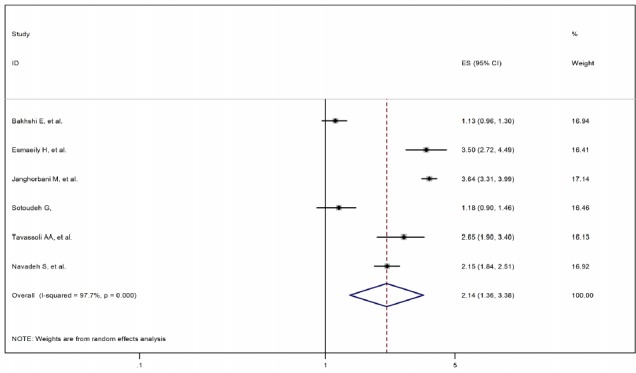
The forest plot of OR of obesity according to marital status in Iran using random-effect mode
Fig. 5 .
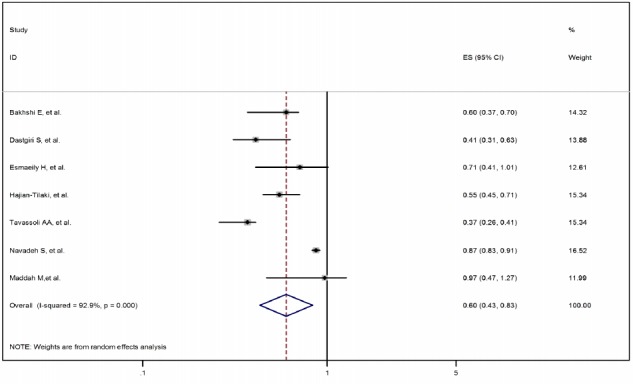
The forest plot of OR of obesity according to education in Iran using random-effect mode
Discussion
This is an updated systematic review on reported association between SEFs and obesi-ty/overweight among the Iranian population according to sex, age, and levels of reported val-ues, from 1973 to 2014. In our study, a total of 17 studies were eligible for inclusion. Our findings provide evidence-based data on the association between SEFs and obesi-ty/overweight.
The analysis revealed that female sex (OR: 2.06, 95%CI: 1.45-2.93), age (OR: 1.66, 95%CI: 1.24-2.22), married status (OR: 2.14, 95%CI: 1.36-3.8), and urban residency (OR: 1.58, 95%CI: 1.18-2.11) increase the risk of obesity. It is considerable that academic education (OR: 0.60, 95%CI: 0.43-0.83) have a reverse association with obesity. Other related studies showed a significant reverse association between low socio-economic situation and obesi-ty/overweight, and direct association between factors such as: female sex, marital status, low education, non-employment and obesity (23-26).
There are few studies on association between SEFs and obesity/overweight in Iran. Moreo-ver the scarcity of data, different studies followed different approaches in their methodology. We also faced a large variety of combinations of unequal determinant factors. Considering above, a case by case, conservative approach was followed to make an accurate conclusion (17, 18, 26).
According to our analysis, age, sex, place of residence, employment, and marital status was studied based on available data. Based on them, age ≥ 30, female sex (vs. male), residence in rural areas (vs. urban), high education (vs. non-academic education), unemployment (vs. em-ployment), and ever married situation (vs. never married) were independent significant factor for obesity (Table 3).
It is mentionable that, only one study considered inequality assessment index about obesity. Based on first run of non-communicable disease surveillance study data (STEPs study, 2005) in Shahroud, concentration index for obesity was (0.038±0.036) for both sex. It was reported -0.005±0.039 and 0.194±0.070 for female and male, respectively; itshowed that obesity is most probable in high socioeconomic levels men (22).
Using principal component analysis, ina comprehensive analyses of national and sub-national mortality effects of metabolic risk factors and smoking in Iran, the sub-national re-gions were defined based on a combination of geography SES. SES was measured using an index constructed from variables from the 2006 census, including years of schooling, em-ployment rates, and family assets (26).
In another national survey of school student with 5,528 student participant, aged 10–18 years, structural equation modeling (path analysis) was applied to evaluate the association be-tween SES and BMI. In this study, higher socioeconomic status was directly associated with BMI in both sexes. In this study, indexes for evaluation of family’s SES were defined based on questions on the parental level of education, parental occupational status, number of inhab-itants in home, and possessing a family private car (27).
In another related experience, to assess the prevalence of Iranian adolescents’ growth disor-ders, sub-national geographical and social classification of the country was considered as the base of SES for definition of living regions (28). It is also important that, there was no com-prehensive study for sub-national evaluation of association between obesity / overweight and its related SEFs in Iran.
Considering the previous studies, the present study has several achievements. This study presents scientific evidences to depict association between SEFs and obesity/overweight among the Iranian population. All available sources of data and domestic data-bases were searched using English/Persian equivalent search terms. As the main limitation, the validity and applicability of our systematic review depends on the quality of the primary studies that are included. As another point, heterogeneity of searched results limits the generalization of our findings.
Conclusion
According to our knowledge, this is the first systematic review of association between SEFs and obesity/overweight in Iran that provide practical information on associations between several socio-demographic factors and obesity. Increased ages, low educational levels, being married, residence in urban area, as well as female sex were clearly associated with obesity. Results could be useful for better health policy and more planned studies in this field. These also can be used for future complementary analyses.
Conflict of interests
The authors declare that they have no competing interests.
Acknowledgements
This study was a part of a Ph.D. dissertation completed by ShirinDjalalinia. Project granted by Ministry of Health and Medical Education of Islamic Republic of Iran and Setad-e-EjraieFarmane Imam. We would like to express our thanks to NCDRC. FF, SD, and NP par-ticipated in study design. SD, NP, and MQ drafted the manuscript. SD, MQ and NP partici-pated in statistical analysis and interpretation of results. SD and NP participated in literature review and data extraction. FF, BL and SD participated in revision of paper. All authors read and approved the final manuscript.
Cite this article as: Djalalinia Sh, Peykari N, Qorbani M, Larijani B, Farzadfar F. Inequality of obesity and socioeconomic factors in Iran: a systematic review and meta- analyses. Med J Islam Repub Iran 2015 (25 July). Vol. 29:241.
References
- 1.Finucane MM, Stevens GA, Cowan MJ, Danaei G, Lin JK, Paciorek CJ. et al. National, regional, and global trends in body-mass index since 1980: systematic analysis of health examination surveys and epidemiological studies with 960 country-years and 91 million participants. The Lancet. 2011;377(9765):557–67. doi: 10.1016/S0140-6736(10)62037-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Stevens GA, Singh GM, Lu Y, Danaei G, Lin JK, Finucane MM. et al. National, regional, and global trends in adult overweight and obesity prevalences. Population Health Metrics. 2012;10:22. doi: 10.1186/1478-7954-10-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Jafari-Adli S, Jouyandeh Z, Qorbani M, Soroush A, Larijani B, Hasani-Ranjbar S. Prevalence of obesity and overweight in adults and children in Iran; a systematic review. Journal of Diabetes & Metabolic Disorders. 2014;13(1):121. doi: 10.1186/s40200-014-0121-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. Jama. 2004;291(10):1238–45. doi: 10.1001/jama.291.10.1238. [DOI] [PubMed] [Google Scholar]
- 5.Djalalinia S, Qorbani M, Peykari N, Kelishadi R. Health impacts of obesity. Pakistan Journal of Medical Sciences. 2015;31(1):4. doi: 10.12669/pjms.311.7033. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bray G. Medical consequences of obesity. The Journal of clinical endocrinology and metabolism. 2004;89(6):2583. doi: 10.1210/jc.2004-0535. [DOI] [PubMed] [Google Scholar]
- 7.Wang Y, Beydoun M. The obesity epidemic in the United States-gender, age, socioeconomic, racial/ethnic, and geographic characteristics: a systematic review and meta-regression analysis. Epidemiologic reviews. 2007;29:6. doi: 10.1093/epirev/mxm007. [DOI] [PubMed] [Google Scholar]
- 8.Nandi A, Glymour M, Subramanian S. Association among socioeconomic status, health behaviors, and all-cause mortality in the United States. Epidemiology (Cambridge, Mass) 2014;25(2):170. doi: 10.1097/EDE.0000000000000038. [DOI] [PubMed] [Google Scholar]
- 9.Vakili M, Abedi P, Sharifi M, Hosseini M. Dietary diversity and its related factors among adolescents: a survey in Ahvaz-Iran. Global journal of health science. 2013;5(2):181–6. doi: 10.5539/gjhs.v5n2p181. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tavassoli AA, Gharipour M, Khosravi A, Kelishadi R, Siadat ZD, Bahonar A. et al. Gender differences in obesogenic behaviour, socioeconomic and metabolic factors in a population-based sample of Iranians: the IHHP study. Journal of health, population, and nutrition. 2010;28(6):602–9. doi: 10.3329/jhpn.v28i6.6609. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Soon H. Pattern of dietary behaviour and obesity in Ahwaz, Islamic Republic of Iran. Eastern Mediterranean Health Journal. 2001;7(1-2):163–70. [PubMed] [Google Scholar]
- 12.Danaei G, Singh GM, Paciorek CJ, Lin JK, Cowan MJ, Finucane MM. et al. The global cardiovascular risk transition: Associations of four metabolic risk factors with national income, urbanization, and western diet in 1980 and 2008. Circulation. 2013;127(14):1493–502. doi: 10.1161/CIRCULATIONAHA.113.001470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Djalalinia S, Kelishadi R, Qorbani M, Peykari N, Kasaeian A, Saeedi Moghaddam S. et al. Suggestions for Better Data Presentation in Papers: An Experience from a Comprehensive Study on National and Sub-national Trends of Overweight and Obesity. Archives of Iranian medicine. 2014;17(12):830–6. [PubMed] [Google Scholar]
- 14.Di Cesare M, Khang Y, Asaria P, Blakely T, Cowan M, Farzadfar F. et al. Inequalities in non-communicable diseases and effective responses. Lancet. 2013;381(9866):585. doi: 10.1016/S0140-6736(12)61851-0. [DOI] [PubMed] [Google Scholar]
- 15.Mirzazadeh A, Haghdoost A, Sadeghirad B, Bahreini F, Ashrafi K, Chack LE. et al. The Prevalence of Obesity in Iran in Recent Decade; a Systematic Review and Meta-Analysis Study. Iranian journal of public health. 2009;38:1–2. [Google Scholar]
- 16.Esmaeily H, Azimi-Nezhad M, Ghayour-Mobarhan M, Parizadeh MR, Safarian M, Parizadeh MJ. et al. Association between socioeconomic factors and obesity in Iran. Pakistan Journal of Nutrition. 2009;8(1):53–6. [Google Scholar]
- 17.Peykari N, Sepanlou S, Djalalinia S, Kasaeian A, Parsaeian M, Ahmadvand A. et al. National and Sub-national Prevalence, Trend, and Burden of Metabolic Risk Factors (MRFs) in Iran: 1990-2013, Study Protocol. Archives of Iranian medicine. 2014;17(1):54. [PubMed] [Google Scholar]
- 18.Kelishadi R, Hovsepian S, Qorbani M, Jamshidi F, Fallah Z, Djalalinia S. et al. National and sub-national prevalence, trend, and burden of cardiometabolic risk factors in Iranian children and adolescents, 1990-2013. Archives of Iranian medicine. 2014;17(1):71. [PubMed] [Google Scholar]
- 19.Nematy M, Sakhdari A, Ahmadi-Moghaddam P, Aliabadi M, Kimiagar M, Ilaty AA. et al. Prevalence of obesity and its association with socioeconomic factors in elderly Iranians from Razavi-Khorasan province. TheScientificWorldJournal. 2009;9:1286–93. doi: 10.1100/tsw.2009.139. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. http://www.ncbi.nlm.nih.gov/mesh/68012959.
- 21.Gardiner J, Luo Z, Roman L. Fixed effects, random effects and GEE: what are the differences? Statistics in medicine. 2009;28(2):221. doi: 10.1002/sim.3478. [DOI] [PubMed] [Google Scholar]
- 22.Emamian MH, Alami A, Fateh M. Socioeconomic inequality in non-communicable disease risk factors in Shahroud, Iran. Iranian J Epidemiology. 2011;7:44–51. [Google Scholar]
- 23.Monteiro CA, Moura EC, Conde WL, Popkin BM. Socioeconomic status and obesity in adult populations of developing countries: a review. Bulletin of the World Health Organization. 2004;82(12):940–6. [PMC free article] [PubMed] [Google Scholar]
- 24.McLaren L. Socioeconomic status and obesity. Epidemiologic reviews. 2007;29(1):29–48. doi: 10.1093/epirev/mxm001. [DOI] [PubMed] [Google Scholar]
- 25.Brennan SL, Henry MJ, Nicholson GC, Kotowicz MA, Pasco JA. Socioeconomic status, obesity and lifestyle in men: the Geelong Osteoporosis Study. Journal of men's health. 2010;7(1):31–41. [Google Scholar]
- 26.Farzadfar F, Danaei G, Namdaritabar H, Rajaratnam JK, Marcus JR, Khosravi A. et al. National and subnational mortality effects of metabolic risk factors and smoking in Iran: a comparative risk assessment. Population Health Metrics. 2011;9 doi: 10.1186/1478-7954-9-55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Kelishadi R, Motlagh ME, Roomizadeh P, Abtahi SH, Qorbani M, Taslimi M. et al. First report on path analysis for cardiometabolic components in a nationally representative sample of pediatric population in the Middle East and North Africa (MENA): the CASPIAN-III Study. Annals of nutrition & metabolism. 2013;62(3):257–65. doi: 10.1159/000346489. [DOI] [PubMed] [Google Scholar]
- 28.Bahreynian M, Motlagh ME, Qorbani M, Heshmat R, Ardalan G, Kelishadi R. Prevalence of growth disorders in a nationally representative sample of Iranian adolescents according to socioeconomic status: the CASPIAN-III Study. Pediatrics & Neonatology. 2014 doi: 10.1016/j.pedneo.2014.12.001. [DOI] [PubMed] [Google Scholar]
- 29.Amani R. Comparison between bioelectrical impedance analysis and body mass index methods in determination of obesity prevalence in Ahvazi women. European journal of clinical nutrition. 2007;61(4):478–82. doi: 10.1038/sj.ejcn.1602545. [DOI] [PubMed] [Google Scholar]
- 30.Asgari F, Biglarian A, Seifi B, Bakhshi A, Miri HH, Bakhshi E. Using quadratic inference functions to determine the factors associated with obesity: findings from the STEPS Survey in Iran. Annals of epidemiology. 2013;23(9):534–8. doi: 10.1016/j.annepidem.2013.07.006. [DOI] [PubMed] [Google Scholar]
- 31.Azizi F, Rahmani M, Emami H, Mirmiran P, Hajipour R, Madjid M. et al. Cardiovascular risk factors in an Iranian urban population: Tehran lipid and glucose study (phase 1) Sozial- und Praventivmedizin. 2002;47(6):408–26. doi: 10.1007/s000380200008. [DOI] [PubMed] [Google Scholar]
- 32.Bakhshi E, Eshraghian MR, Mohammad K, Foroushani AR, Zeraati H, Fotouhi A. et al. The positive association between number of children and obesity in Iranian women and men: results from the National Health Survey. BMC public health. 2008;8:213. doi: 10.1186/1471-2458-8-213. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Bakhshi E, Mohammad K, Eshraghian MR, Seifi B. Factors related to obesity among Iranian men: results from the National Health Survey. Public health nutrition. 2010;13(9):1389–94. doi: 10.1017/S1368980010000108. [DOI] [PubMed] [Google Scholar]
- 34.Behzadnia S, Vahidshahi K, Hamzeh Hosseini S, Anvari S, Ehteshami S. Obesity and related factors in 7-12 year-old elementary school students during 2009-2010 in Sari, Iran. Medicinski glasnik: official publication of the Medical Association of Zenica-Doboj Canton, Bosnia and Herzegovina. 2012;9(1):86–90. [PubMed] [Google Scholar]
- 35.Dastgiri S, Mahdavi R, TuTunchi H, Faramarzi E. Prevalence of obesity, food choices and socio-economic status: a cross-sectional study in the north-west of Iran. Public health nutrition. 2006;9(8):996–1000. doi: 10.1017/s1368980006009827. [DOI] [PubMed] [Google Scholar]
- 36.Hajian-Tilaki KO, Heidari B. Association of educational level with risk of obesity and abdominal obesity in Iranian adults. Journal of public health (Oxford, England) 2010;32(2):202–9. doi: 10.1093/pubmed/fdp083. [DOI] [PubMed] [Google Scholar]
- 37.Janghorbani M, Amini M, Rezvanian H, Gouya MM, Delavari A, Alikhani S. et al. Association of body mass index and abdominal obesity with marital status in adults. Archives of Iranian medicine. 2008;11(3):274–81. [PubMed] [Google Scholar]
- 38.Shahraki M, Shahraki T, Ansari H. The effects of socio-economic status on BMI, waist:hip ratio and waist circumference in a group of Iranian women. Public health nutrition. 2008;11(7):757–61. doi: 10.1017/S1368980007001577. [DOI] [PubMed] [Google Scholar]
- 39.Sotoudeh G, Khosravi S, Khajehnasiri F, Khalkhali HR. High prevalence of overweight and obesity in women of Islamshahr, Iran. Asia Pacific journal of clinical nutrition. 2005;14(2):169–72. [PubMed] [Google Scholar]
- 40.Maddah M. Overweight and obesity among Iranian female adolescents in Rasht: more overweight in the lower social group. Public health nutrition. 2007;10(5):450–3. doi: 10.1017/S1368980007219664. [DOI] [PubMed] [Google Scholar]
- 41.Navadeh S, Sajadi L, Mirzazadeh A, Asgari F, Haghazali M. Housewives' obesity determinant factors in iran; national survey - stepwise approach to surveillance. Iranian journal of public health. 2011;40(2):87–95. [PMC free article] [PubMed] [Google Scholar]
- 42.Maddah M, Solhpour A. Obesity in relation to gender, educational levels and living area in adult population in Rasht, northern Iran. International journal of cardiology. 2010;145(2):310–1. doi: 10.1016/j.ijcard.2009.10.045. [DOI] [PubMed] [Google Scholar]