

Abstract
Nonampullary duodenal adenomas are relatively common in familial adenomatous polyposis (FAP), but nonampullary sporadic duodenal adenomas (SDAs) are rare. Emerging evidence shows that duodenal adenomas, regardless of their anatomic location and whether they are sporadic or FAP-related, share morphologic and molecular features with colorectal adenomas. The available data suggest that duodenal adenomas develop to duodenal adenocarcinomas via similar mechanisms. The optimal approach for management of duodenal adenomas remains to be determined. The techniques for endoscopic resection of duodenal adenoma include snare polypectomy, endoscopic mucosal resection (EMR), endoscopic submucosal dissection (ESD), and argon plasma coagulation ablation. EMR may facilitate removal of large duodenal polyps. Although several studies have reported cases of successful ESD for duodenal adenomas, the procedure is technically difficult to perform safely because of the anatomical properties of the duodenum. Although current clinical practice recommends endoscopic resection of all large duodenal adenomas in patients with FAP, endoscopic treatment is usually insufficient to guarantee a polyp-free duodenum. Surgery is indicated for FAP patients with severe polyposis or nonampullary SDAs or FAP-related polyps not amenable to endoscopic resection. Further studies are needed to develop newer endoscopic techniques to guide diagnostic and therapeutic decisions for future management of nonampullary duodenal adenomas.
Keywords: Duodenal adenoma, Endoscopy, Familial adenomatous polyposis, Endoscopic mucosal resection, Endoscopic submucosal dissection
Core tip: Nonampullary duodenal adenomas are thought to progress to duodenal adenocarcinomas in a stepwise manner, with accumulation of genetic mutations, including those in APC, KRAS, and p53. Recently, using magnifying endoscopy with narrow band imaging, a novel diagnostic algorithm for real-time diagnosis of nonampullary superficial duodenal epithelial tumors was developed. Endoscopic mucosal resection may facilitate removal of large duodenal polyps. Although several studies have reported cases of successful endoscopic submucosal dissection for duodenal adenomas, the procedure is technically difficult to perform safely. Further studies are needed to develop newer endoscopic techniques for the diagnosis and treatment of nonampullary duodenal adenomas.
INTRODUCTION
Sporadic duodenal polyps are uncommon, found in up to only 5% of patients referred for upper gastrointestinal endoscopy[1]. Sporadic duodenal polyps can be classified according to their histopathological subtype and location, as follows: nonampullary sporadic adenoma, ampullary sporadic adenoma, Brunner’s gland adenoma or harmatoma, gastric heterotopia/metaplasia, inflammatory fibroid polyp, lipoma, leiomyoma, carcinoid, gastrointestinal stromal tumors, lymphoma, and solitary Peutz-Jeghers polyps[1]. Nonampullary duodenal adenoma is relatively common in patients with familial adenomatous polyposis (FAP), but sporadic duodenal adenoma (SDA) is rare. Approximately 40% of duodenal adenomas are sporadic, and the remaining 60% present in patients with FAP[2].
The options for endoscopic resection of duodenal adenomas include snare polypectomy, endoscopic mucosal resection (EMR), endoscopic submucosal dissection (ESD), and argon plasma coagulation (APC) ablation[3]. EMR of duodenal neoplasms was first performed in 1992[4]. Endoscopic resection represents an attractive alternative to surgical resection in appropriately selected patients, with lower morbidity and mortality rates[5]. Surgical options include laparoscopic-assisted endoluminal surgery, laparoscopic polyp excision, duodenectomy, and pancreaticoduodenectomy[1]. The morbidity and mortality of these procedures are dependent on patient co-morbidities, together with operator experience and case volume[1]. These techniques are usually reserved for malignant lesions. In this review, we will discuss the clinicopathological characteristics and management of sporadic and FAP-related nonampullary duodenal adenomas.
PREVALENCE AND NATURAL HISTORY OF NONAMPULLARY DUODENAL ADENOMAS
Sporadic duodenal adenomas
In a large retrospective endoscopic series conducted in Germany, 378 duodenal polyps were identified in the course of more than 25000 esophagogastroduodenoscopy (EGD) procedures, corresponding to an incidence of 1.5%[6]. That study showed that 6.9% of 378 patients had duodenal adenomas. A prospective study from Denmark reported that the prevalence of duodenal polyps was 4.6% (27/584) in patients referred for diagnostic EGD, and two of the polyps were adenomas (0.4%)[7]. Our group demonstrated that the prevalence of duodenal polyps was 1.02% (510/50114), and 14 of the polyps were adenomas (0.03%)[8]. With the increasingly widespread use of endoscopy, these tumors are being diagnosed more frequently. These lesions are of particular interest because of the acceptance of the adenoma to carcinoma progression sequence of colorectal tumors, which has also been postulated to be associated with those of the small bowel[9]. Because 30%-85% of duodenal adenomas undergo malignant transformation, their surgical or endoscopic excision is mandatory[10-14].
Okada et al[15] evaluated the risk of adenocarcinoma posed by nonampullary SDAs with an initial diagnosis of low-grade dysplasia (LGD) or high-grade dysplasia (HGD), based on the results of subsequent endoscopic observations and histological assessments. In this study, 46 SDAs (43 LGD lesions, 3 HGD lesions) were followed up for ≥ 6 mo without treatment. Among 43 LGD lesions, 34 (79.1%) showed no histopathological changes during follow-up, whereas the remaining 9 (20.9%) showed progression to HGD, including 2 (4.7%) that eventually progressed to noninvasive carcinoma. All three HGD lesions remained unchanged histologically, based on biopsy, although one of the three lesions resected endoscopically revealed evidence of noninvasive carcinoma. Among 11 lesions initially diagnosed as HGD from biopsy samples, nine were resected immediately or during follow-up. A high percentage of the cancers (54.5%, 6 of 11) were diagnosed from resected specimens. A multivariate analysis identified HGD diagnosed at first biopsy and a lesion diameter of ≥ 20 mm as being significantly predictive of progression to adenocarcinoma. The authors concluded that LGD lesions show a low risk of progression to adenocarcinoma, but some risk of progression to HGD, which warrants careful follow-up biopsy. However, HGD lesions and large nonampullary SDAs ≥ 20 mm in diameter show a high risk of progression to adenocarcinoma and therefore, they should be treated immediately.
Duodenal adenomas in FAP
Duodenal cancer is a leading cause of death in FAP patients with previous colectomy[16,17]. It develops from pre-existing adenomas with a cumulative risk of almost 100% in patients with FAP[16,18-20]. The cumulative risk of duodenal cancer is 3%-10%[19,21]. Duodenal adenomas usually are multiple, sessile, and predominantly located in the mucosal folds of the descending duodenum[16]. In 1989, Spigelman et al[17] developed a staging system for evaluation of the severity of duodenal adenomatosis. Using this system, classification is determined by a five-grade scale (stage 0-IV) based on adenoma number (1-4, 5-20, or > 20), size (< 5, 5-10, or > 10 mm), histologic type (tubular, tubulovillous, or villous) and severity of dysplasia (mild, moderate, or severe). This system allowed evaluation of the duodenal adenoma burden in patients with FAP and estimation of the risk of developing duodenal cancer, which was confirmed in subsequent studies[20,22]. The risk of duodenal cancer increases with age and with progressive adenoma stage[16,22]. It is lowest at 0.7% in stage 0-III disease and greatest in stage IV disease, with rates of 7%-36% over follow-up periods of 7.6-10 years[21,22]. The risk of developing stage IV duodenal polyposis is estimated to be 20%-50% at age 70 years[19-21].
MOLECULAR FEATURES OF NONAMPULLARY DUODENAL ADENOMAS
Duodenal adenomas are thought to progress to duodenal adenocarcinoma in a stepwise manner, with the accumulation of genetic mutations, including those in APC, KRAS, and p53[23]. Despite epidemiologic and histologic evidence suggesting an adenoma-carcinoma sequence analogous to that proposed for most colorectal adenomas, the pathogenesis of small intestinal adenomas and adenocarcinomas is poorly characterized[24]. Nonampullary SDAs show a tubular architecture in all cases[24,25]. Wagner et al[24] evaluated the molecular characteristics of a series of nonampullary SDAs (n = 22) that developed distal to the ampulla, and compared them with the features of sporadic ampullary adenoma (n = 9) and FAP-related polyps (n = 12). Regardless of their anatomic location and whether they were sporadic or FAP-related, approximately 75% of the duodenal adenomas showed Wnt signaling pathway abnormalities, which probably reflect underlying APC, rather than β-catenin, mutations. KRAS mutations were infrequent in nonampullary SDAs (18%), and FAP-related adenomas (9%), moderatley frequent in ampullary adenomas (44%). None of the cases harbored BRAF mutations. In addition, p53 alterations and DNA mismatch repair were rare. These results indicate that duodenal adenomas share morphologic and molecular features with colorectal adenomas, suggesting that they develop via similar mechanisms. Rubio[26] reviewed a cohort of 306 FAP-related or sporadic duodenal adenomas and found gastric duodenal metaplasia (GMD) covering portion of the adenomas in 31.7% (66/208) of the duodenal FAP adenomas and in 59.5% (58/98) of the duodenal sporadic adenomas (P < 0.05). This result suggests that a subset of GMD of unknown cause might be present in the duodenal mucosa before adenomatous transformation, with neoplastic proclivity similar to that of other metaplasias of the gastrointestinal tract (intestinal metaplasia of the esophagus and of the stomach and metaplastic-hyperplastic polyposis of the colon). Adenomatous neoplastic transformation in these patients may be due to the carcinogenic effect of the high concentrations of bile acids and pancreatic juices in the duodenum. Similar to colonic tumors, small intestinal adenocarcinomas are usually preceded by noninvasive precursor lesions such as adenomas, as evidenced by the occurrence of invasive adenocarcinoma within small bowel adenomas, and the presence of residual adenomatous tissue adjacent to, or within, most carcinomas[9,10]. Sun et al[27] evaluated the CpG island methylator phenotype (CIMP) in ampullary and nonampullary SDAs and determined a correlation between CIMP and MLH1 and p16 methylation, as well as KRAS and BRAF mutations. They showed that CIMP+ (more than two markers methylated) was found in 33.3% of duodenal adenomas; 61% of these CIMP+ adenomas were CIMP-high (more than three markers methylated). In addition, CIMP+ status significantly correlated with older patient age, larger size and villous type of tumor, coexistent dysplasia and periampullary location, MLH1 methylation and KRAS mutation in duodenal adenomas. These results suggest that patients with CIMP+ duodenal adenomas have a higher risk of developing malignancy and may require more aggressive management and surveillance.
ENDOSCOPIC DIAGNOSIS
Certain ampullary neoplasms may present early with obstructive jaundice or pancreatitis, as small lesions can cause obstruction of the ampullary orifice, whereas almost all nonampullary neoplasms are incidentally discovered during routine endoscopy. Kiesslich et al[28] demonstrated that conventional chromoendoscopy with indigocarmine detected a significantly greater number of lesions in the duodenum than did standard high-resolution white-light endoscopy (98 vs 28, P = 0.0042). However, the dye spray technique is considered cumbersome, and, no study on adenoma differentiation has been published to date[29]. In 2006, Uchiyama et al[30] reported narrow band imaging (NBI) findings of ampullary polyps classified as type I, oval-shaped villi, type II, pinecone/leaf-shaped villi, or type III, irregular/non-structured. They showed a perfect correlation (100%) of type II and/or type III surface structures with histological findings of adenoma and adenocarcinoma. However, there were a few positive lesions in their study. A recent study involving a large number of patients applied NBI endoscopy in 65 gastric and duodenal polyps using the same criteria, and revealed that NBI had 80% accuracy for the detection of adenoma[31]. In a recent study, probe-based confocal laser endomicroscopy (pCLE) was used together with NBI (GIF H-180; Olympus) for duodenal adenoma diagnosis. It was concluded that pCLE provided greater sensitivity than NBI (92% vs 83%, P = 0.8)[31]. Of note, the criteria for duodenal adenoma diagnosis of pCLE and NBI in this study were adopted from those for Barrett’s esophagus. More recently, a Japanese researcher developed a novel diagnostic algorithm for magnifying endoscopy with NBI (ME-NBI) for nonampullary superficial duodenal epithelial tumors[32]. Lesions displaying a single surface pattern were classified as monotype, and those displaying multiple surface patterns as mixed type. Surface pattern was classified as preserved, micrified, or absent. In addition, vascular pattern was classified as absent, network, intrastructural vascular (ISV), or unclassified. The results showed that all mixed-type lesions (23/23) were category 4 (mucosal high-grade neoplasia) or category 5 (submucosal invasion by carcinoma) tumors according to the revised Vienna classification[33]. Approximately 50% (10/23) of monotype lesions were category 3 (mucosal low grade neoplasia) tumors. Among the monotype lesions, the probability of category 4/5 tumor was 100% (2/2) in lesions with an unclassified vascular pattern, 64.3% (9/14) in lesions with an ISV pattern, 33.3% (1/3) in lesions with an absent pattern, and 25.5% (1/4) in lesions with a network pattern. Taken together, these findings suggest that detailed observation of both the surface and vascular pattern is necessary for monotype lesions, and ME-NBI classification can be used to perform histological diagnosis of nonampullary superficial duodenal epithelial tumors. However, further study is needed to accumulate a greater number of cases and to conduct careful comparisons with pathological findings. A Japanese multicenter study including 364 patients with 396 nonampullary superficial duodenal epithelial tumors showed that a significantly greater number of high-grade dysplasia or superficial adenocarcinomas compared with low-grade dysplasia was found in tumors with a diameter > 5 mm as well as solely or predominantly red coloration[34].
MANAGEMENT OF NONAMPULARRY DUODENAL ADENOMAS
As mentioned previously, endoscopic or surgical resection is recommended for nonampullary SDAs because of malignant potential of this lesion[15,35]. The method of resection depends on the size, location morphology, and pathology of the adenoma. Surgical resection is considered in cases of adenoma ≥ 2 cm, with severe dysplasia, suspicious carcinomatous infiltration, or recurrence after complete endoscopic resection[1].
Endoscopic treatment
Endoscopic resection for the treatment of nonampullary SDAs has the advantages of being less invasiveness. However, the endoscopic techniques are not standardized and most studies regarding endoscopic resection have been of retrospective design or a case series. Several endoscopic resection techniques-including snare polypectomy (Figure 1), EMR (Figure 2), ESD (Figure 3), and APC ablative methods-for management of nonampullary SDAs are available. Endoscopic resection is feasibe as a treatment method for nonampullary SDAs, but it also has limitations regarding complications and recurrence. The extensive second-order arterial blood supply and thin wall of the duodenum contribute to the occurrence of immediate/delayed bleeding and transmural thermal injury causing perforation.
Figure 1.

Snare polypectomy. A: A approximately 10 mm peduculated adenoma in the second portion of the duodenum; B: Snare polypectomy procedure.
Figure 2.
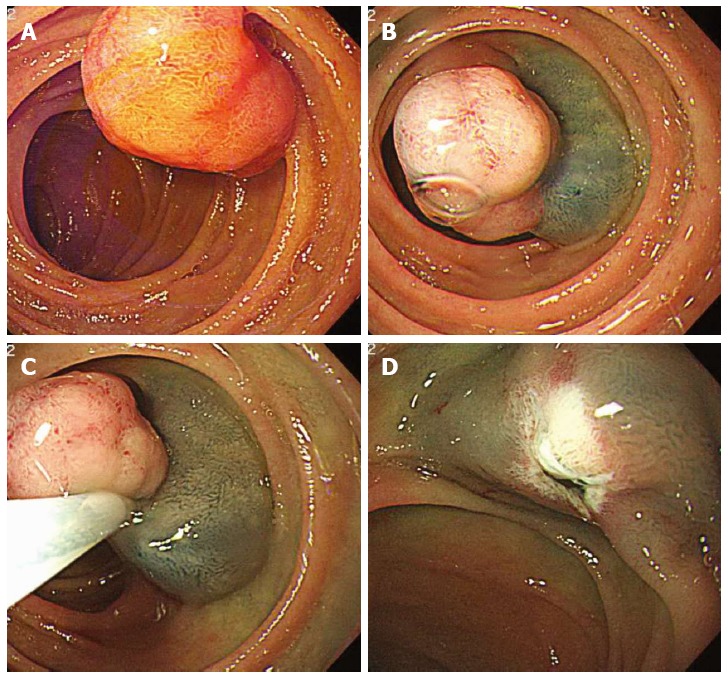
Endoscopic mucosal resection. A: An approximately 20 mm polypoid mass in the second portion of the duodenum; B: Injection of submucosal saline solution with indigocarmine; C: Endoscopic mucosal resection (EMR) procedure; D: A clear, post-EMR ulcer.
Figure 3.
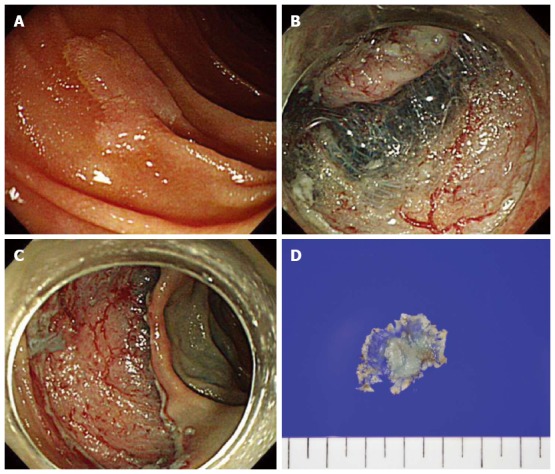
Endoscopic submucosal dissection. A: A 12 mm sized superficial elevated type (IIa) lesion in the second portion of the duodenum; B: Circumferential mucosal incision and submucosal dissedtion; C: The lesion successfully removed en bloc without complications; D: A 27 mm resected specimen with adenoma.
An endoscope that enables optimal enface access to the lesion should be used. A side-viewing endoscope is optimal for lesions on the anterior or medial wall, particularly within 5 cm of the major papilla, and a pediatric colonoscope is preferable for lesions on the posterior or lateral wall[3]. Double balloon endoscopy was reported to enable stable manipulation and successful resection, even in the deep portion of the duodenum[36,37]. Snare polypectomy was reported to be effective, with an 85% eradication rate, in 20 duodenal adenoma cases, but it required repetitive intervention, combined or additional APC ablation, and follow-up due to incomplete resection or tumor recurrence[38]. EMR has been used in the majority of studies on endoscopic adenoma treatment of nonampullary SDAs. A flat or sessile morphology is most common in duodenal adenomas, and submucosal injection of lifting solution raises the lesion on a cushion of submucosal fluid, separating the mucosal and muscle layers. EMR has shown complete resection rates ranging 59% to 100%[5,39-50]. Other modified EMR methods, such as cap-assisted EMR[51], underwater EMR[3], and the band-and-slough technique[52], were reported to be effective endoscopic treatments for adenoma. The extent of the luminal circumference involved by the tumor was reported as the strongest predictor of successful eradication of nonampullary SDAs by endoscopic treatment[42]. The en bloc resection rate of EMR was reported to be 38.1% to 100%, and multiple resections or APC ablation are frequently required due to piecemeal resection[40,42-48,50]. The adenoma recurrence rate after EMR has been reported to be 0%-37%[5,39-41,43-50]. The majority of recurrent adenomas after EMR have been treated by endoscopic resection or ablation techniques[40,41,47,48]. Adenomas of > 2 cm are associated with a higher incidence of recurrence[41]. Adenomas with a villous nature were also reported to have a higher rate of recurrence[48]. The following complications after EMR have been reported: an intraprocedural bleeding rate of 0%-29.2%, delayed bleeding rate of 0%-16.7% and perforation rate of 0%-4.3%[37,39,43,44,46,49,51,53]. There have been fewer reports on ESD for the treatment of nonampullary SDAs, involving a limited number of cases, compared with EMR. ESD has been reported to be an effective method, with a complete resection rate of 80%-100% for nonampullary SDAs; moreover, no recurrence was reported[5,36,37,54-56]. However, duodenal ESD has been reported to have high rates of perforation (6%-50%) and bleeding (0%-7%). Duodenal ESD should be performed with caution in selected patients to avoid serious complications. Endoscopic APC ablation has been applied as both primary and adjunctive treatment for nonampullary SDAs. Entire pathologic evaluation is impossible in APC ablation. Two studies on APC ablation as primary treatment involving limited numbers of patients have been performed, with reported recurrence rates of 10% and 39%[46,57]. APC ablation has been used mainly as an adjunct modality with EMR for removal of remnant or locally recurrent nonampullary SDAs[38-42,46,48,50-52].
Following successful endoscopic resection of nonampullary SDA, follow-up endoscopy at 3-6 mo is recommended to check for recurrence. If recurrence is not detected, endoscopic surveillance at 6-12 mo is required[38,58]. Annual follow-up endoscopy should be performed for at least 2 years after complete resection[41].
Surgical treatment
Surgery remains as the standard treatment for large and complex nonampullary SDAs which are technically impossible to remove using endoscopic techniques. The optimal surgical treatment of nonampullary SDAs has not been established. Four major surgical procedures exist for the removal of duodenal tumors[2,12,14,59-61]; namely, transduodenal excision (transduodenal submucosal excision)[62], local full-thickness resection (wedge resection), pancreas-sparing segmental duodenectomy[63], and pancreaticoduodenectomy. The first three are the so-called “limited resections” and are usually indicated for selected tumors not amenable to endoscopic resection that have no or negligible risk of nodal metastasis[59-61]. The local recurrence rates for these surgical managements of nonampullary SDAs are reportedly low[2,14]. The endoscopy-assissted laparoscopic technique for nonampullary SDAs has been reported to be a safe and minimally invasive treatment option[64,65].
Surveillance and management of duodenal adenomas in patients with FAP
Considering the high incidence of duodenal adenomas with severe dysplasia in FAP and the increased risk of developing duodenal cancer, upper gastrointestinal (GI) endoscopic surveillance is highly recommended. To provide adequate visualization of the entire duodenal mucosa, a forward- and side-viewing endoscope should be used[53]. Although recommendations concerning patient age for initiation of upper GI surveillance are not uniform, performance of the first endoscopy in patients with FAP is recommended at 25-30 years of age[16,66]. Continued endoscopic surveillance after baseline endoscopy is usually performed according to the Spigelman stage. In general, patients with stage 0 receive repeat surveillance endoscopy every 4 years, those with stage I and II every 2-3 years, those with stage III every 6-12 mo with consideration for surgery, and those with stage IV should be referred to a pancreato-biliary surgeon for consideration of surgery[22,66]. Despite routine endoscopic surveillance, a considerable percentage of advanced ampullary neoplasias may not be detected[19]. In addition, several authors report that random biopsy samples from the ampullary region are needed because 12%-54% of normal-appearing papilla may harbor adenoma[16,19-22,67]. The use of chromoendoscopy leads to a marked increase in the number and size of duodenal adenomas detected in patients with FAP and an upgrade of the Spigelman stage[68,69]. A recent study showed that the use of NBI resulted in detection of a greater number of duodenal adenomas, resulting in upgrade of the Spigelman stage in 4.4% of patients[70]. However, NBI did not improve the detection of gastric polyps in comparison with high-resolution endoscopy.
The management of duodenal adenoma in patients with FAP remains a major challenge. It is at present clear whether medical or endoscopic therapies significantly alter long-term cancer risk or improve survival or quality of life in patients with a significant duodenal burden[53,66]. Nonsteroidal anti-inflammatory drugs (NSAIDs) can lead to regression of colorectal adenomas in patients with FAP. One study compared the effect of sulindac with placebo on the number of duodenal polyps[71]. Treatment with sulindac resulted in regressed small (≤ 2 mm) duodenal polyps, whereas larger (≥ 3 mm) duodenal polyps were unaffected. However, most studies regarding the effects of NASIDs and other compounds on prevention or regression of duodenal adenomas in FAP have reported disappointing results[66]. Current endoscopic treatment options for duodenal polyps in patients with FAP include snare polypectomy, EMR, thermal ablation, APC ablation, and photodynamic therapy[53,66]. Most studies indicate the complete resection of non-polypoid flat lesions by snare polypectomy is difficult. EMR may facilitate removal of large flat duodenal polyps in FAP. Endoscopic treatment has been proposed for patients with stage II or III disease[22]. Although current clinical practice recommends endoscopic resection of all large duodenal adenomas unless there is suspicion of advanced histology and submucosal invasion, endoscopic treatment is usually insufficient to guarantee a polyp-free duodenum and should be individualized based on the patient’s overall polyp burden, size and location, and comorbidities[53,66]. Surgical management includes local surgical treatment (duodenotomy with polypectomy), pancreas- or pylorus-preserving duodenectomy and pancreaticoduodenectomy[2,66]. Duodenotomy and polypectomy have proven ineffective in FAP patients with severe duodenal adenomatosis, as evidenced by high recurrence rates[72]. Definitive resection in the form of pancreaticoduodenectomy (standard or pylorus preserving) or pancreas-preserving duodenectomy has been indicated for patients with severe polyposis (stage IV) or polyps that are not amenable to endoscopic resection[2,66]. Recurrence rates are low after these operations, but the risks of morbidity and mortality are relatively high[66].
CONCLUSIONS AND FUTURE PERSPECTIVES
Nonampullary duodenal adenomas are uncommon but are associated with a risk of developing duodenal cancer. The development of endoscopic techniques for early detection and differentiation between adenoma and cancerous lesions, as well as between mucosal and submucosal cancer, is important for the management of nonampullary duodenal adenomas. Although remarkable progress in advanced endoscopic resection throughout the gastrointestinal tract was made during the last decade, endoscopic techniques to remove nonampullary duodenal adenomas have not yet been standardized. Compared with EMR, ESD has a superior complete resection rate with no recurrence. However, duodenal ESD remains challenging due to the high risk of immediate or delayed perforation and bleeding. The use of classical surgery for nonampullary duodenal adenomas that are not amenable to endoscopic resection has decreased with the development of minimally invasive surgery. Current treatment options for duodenal adenomatosis in patients with FAP include frequent endoscopic surveillance and targeted endoscopic treatment or surgical management according to the severity of duodenal lesions. Further studies should be focus on developing new endoscopic techniques to guide diagnostic and therapeutic decisions for future management of nonampullary duodenal adenomas.
Footnotes
Conflict-of-interest statement: Authors declare no conflict of interests for this article.
Open-Access: This article is an open-access article which was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Peer-review started: June 25, 2015
First decision: July 20, 2015
Article in press: October 26, 2015
P- Reviewer: Montalbetti N S- Editor: Yu J L- Editor: A E- Editor: Liu XM
References
- 1.Culver EL, McIntyre AS. Sporadic duodenal polyps: classification, investigation, and management. Endoscopy. 2011;43:144–155. doi: 10.1055/s-0030-1255925. [DOI] [PubMed] [Google Scholar]
- 2.Johnson MD, Mackey R, Brown N, Church J, Burke C, Walsh RM. Outcome based on management for duodenal adenomas: sporadic versus familial disease. J Gastrointest Surg. 2010;14:229–235. doi: 10.1007/s11605-009-1091-4. [DOI] [PubMed] [Google Scholar]
- 3.Bourke MJ. Endoscopic resection in the duodenum: current limitations and future directions. Endoscopy. 2013;45:127–132. doi: 10.1055/s-0032-1326177. [DOI] [PubMed] [Google Scholar]
- 4.Obata S, Suenaga M, Araki K, Fujioka Y, Kimura K, Maeda K, Miura K, Mizutani J. Use of strip biopsy in a case of early duodenal cancer. Endoscopy. 1992;24:232–234. doi: 10.1055/s-2007-1010470. [DOI] [PubMed] [Google Scholar]
- 5.Yamamoto Y, Yoshizawa N, Tomida H, Fujisaki J, Igarashi M. Therapeutic outcomes of endoscopic resection for superficial non-ampullary duodenal tumor. Dig Endosc. 2014;26 Suppl 2:50–56. doi: 10.1111/den.12273. [DOI] [PubMed] [Google Scholar]
- 6.Höchter W, Weingart J, Seib HJ, Ottenjann R. [Duodenal polyps. Incidence, histologic substrate and significance] Dtsch Med Wochenschr. 1984;109:1183–1186. doi: 10.1055/s-2008-1069345. [DOI] [PubMed] [Google Scholar]
- 7.Jepsen JM, Persson M, Jakobsen NO, Christiansen T, Skoubo-Kristensen E, Funch-Jensen P, Kruse A, Thommesen P. Prospective study of prevalence and endoscopic and histopathologic characteristics of duodenal polyps in patients submitted to upper endoscopy. Scand J Gastroenterol. 1994;29:483–487. doi: 10.3109/00365529409092458. [DOI] [PubMed] [Google Scholar]
- 8.Jung SH, Chung WC, Kim EJ, Kim SH, Paik CN, Lee BI, Cho YS, Lee KM. Evaluation of non-ampullary duodenal polyps: comparison of non-neoplastic and neoplastic lesions. World J Gastroenterol. 2010;16:5474–5480. doi: 10.3748/wjg.v16.i43.5474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Sellner F. Investigations on the significance of the adenoma-carcinoma sequence in the small bowel. Cancer. 1990;66:702–715. doi: 10.1002/1097-0142(19900815)66:4<702::aid-cncr2820660419>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- 10.Perzin KH, Bridge MF. Adenomas of the small intestine: a clinicopathologic review of 51 cases and a study of their relationship to carcinoma. Cancer. 1981;48:799–819. doi: 10.1002/1097-0142(19810801)48:3<799::aid-cncr2820480324>3.0.co;2-q. [DOI] [PubMed] [Google Scholar]
- 11.Sakorafas GH, Friess H, Dervenis CG. Villous tumors of the duodenum: biologic characters and clinical implications. Scand J Gastroenterol. 2000;35:337–344. doi: 10.1080/003655200750023877. [DOI] [PubMed] [Google Scholar]
- 12.Galandiuk S, Hermann RE, Jagelman DG, Fazio VW, Sivak MV. Villous tumors of the duodenum. Ann Surg. 1988;207:234–239. doi: 10.1097/00000658-198803000-00002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Krukowski ZH, Ewen SW, Davidson AI, Matheson NA. Operative management of tubulovillous neoplasms of the duodenum and ampulla. Br J Surg. 1988;75:150–153. doi: 10.1002/bjs.1800750221. [DOI] [PubMed] [Google Scholar]
- 14.Farnell MB, Sakorafas GH, Sarr MG, Rowland CM, Tsiotos GG, Farley DR, Nagorney DM. Villous tumors of the duodenum: reappraisal of local vs. extended resection. J Gastrointest Surg. 2000;4:13–21, discussion 22-23. doi: 10.1016/s1091-255x(00)80028-1. [DOI] [PubMed] [Google Scholar]
- 15.Okada K, Fujisaki J, Kasuga A, Omae M, Kubota M, Hirasawa T, Ishiyama A, Inamori M, Chino A, Yamamoto Y, et al. Sporadic nonampullary duodenal adenoma in the natural history of duodenal cancer: a study of follow-up surveillance. Am J Gastroenterol. 2011;106:357–364. doi: 10.1038/ajg.2010.422. [DOI] [PubMed] [Google Scholar]
- 16.Cruz-Correa M, Giardiello FM. Familial adenomatous polyposis. Gastrointest Endosc. 2003;58:885–894. doi: 10.1016/s0016-5107(03)02336-8. [DOI] [PubMed] [Google Scholar]
- 17.Spigelman AD, Williams CB, Talbot IC, Domizio P, Phillips RK. Upper gastrointestinal cancer in patients with familial adenomatous polyposis. Lancet. 1989;2:783–785. doi: 10.1016/s0140-6736(89)90840-4. [DOI] [PubMed] [Google Scholar]
- 18.Burke CA, Beck GJ, Church JM, van Stolk RU. The natural history of untreated duodenal and ampullary adenomas in patients with familial adenomatous polyposis followed in an endoscopic surveillance program. Gastrointest Endosc. 1999;49:358–364. doi: 10.1016/s0016-5107(99)70013-1. [DOI] [PubMed] [Google Scholar]
- 19.Björk J, Akerbrant H, Iselius L, Bergman A, Engwall Y, Wahlström J, Martinsson T, Nordling M, Hultcrantz R. Periampullary adenomas and adenocarcinomas in familial adenomatous polyposis: cumulative risks and APC gene mutations. Gastroenterology. 2001;121:1127–1135. doi: 10.1053/gast.2001.28707. [DOI] [PubMed] [Google Scholar]
- 20.Saurin JC, Gutknecht C, Napoleon B, Chavaillon A, Ecochard R, Scoazec JY, Ponchon T, Chayvialle JA. Surveillance of duodenal adenomas in familial adenomatous polyposis reveals high cumulative risk of advanced disease. J Clin Oncol. 2004;22:493–498. doi: 10.1200/JCO.2004.06.028. [DOI] [PubMed] [Google Scholar]
- 21.Bülow S, Björk J, Christensen IJ, Fausa O, Järvinen H, Moesgaard F, Vasen HF. Duodenal adenomatosis in familial adenomatous polyposis. Gut. 2004;53:381–386. doi: 10.1136/gut.2003.027771. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Groves CJ, Saunders BP, Spigelman AD, Phillips RK. Duodenal cancer in patients with familial adenomatous polyposis (FAP): results of a 10 year prospective study. Gut. 2002;50:636–641. doi: 10.1136/gut.50.5.636. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Rubio CA. Signaling pathways, gene regulation and duodenal neoplasiaa. In: Singh SR, editor. Signaling, Gene Regulation and Cancer. NY: Nova Science Publishers, Inc; 2013. pp. 83–110. [Google Scholar]
- 24.Wagner PL, Chen YT, Yantiss RK. Immunohistochemical and molecular features of sporadic and FAP-associated duodenal adenomas of the ampullary and nonampullary mucosa. Am J Surg Pathol. 2008;32:1388–1395. doi: 10.1097/PAS.0b013e3181723679. [DOI] [PubMed] [Google Scholar]
- 25.Odze RD. Epithelial proliferation and differentiation in flat duodenal mucosa of patients with familial adenomatous polyposis. Mod Pathol. 1995;8:648–653. [PubMed] [Google Scholar]
- 26.Rubio CA. Gastric duodenal metaplasia in duodenal adenomas. J Clin Pathol. 2007;60:661–663. doi: 10.1136/jcp.2006.039388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Sun L, Guzzetta AA, Fu T, Chen J, Jeschke J, Kwak R, Vatapalli R, Baylin SB, Iacobuzio-Donahue CA, Wolfgang CL, et al. CpG island methylator phenotype and its association with malignancy in sporadic duodenal adenomas. Epigenetics. 2014;9:738–746. doi: 10.4161/epi.28082. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Kiesslich R, Mergener K, Naumann C, Hahn M, Jung M, Koehler HH, Nafe B, Kanzler S, Galle PR. Value of chromoendoscopy and magnification endoscopy in the evaluation of duodenal abnormalities: a prospective, randomized comparison. Endoscopy. 2003;35:559–563. doi: 10.1055/s-2003-40240. [DOI] [PubMed] [Google Scholar]
- 29.Pittayanon R, Imraporn B, Rerknimitr R, Kullavanijaya P. Advances in diagnostic endoscopy for duodenal, including ampullary, adenoma. Dig Endosc. 2014;26 Suppl 2:10–15. doi: 10.1111/den.12244. [DOI] [PubMed] [Google Scholar]
- 30.Uchiyama Y, Imazu H, Kakutani H, Hino S, Sumiyama K, Kuramochi A, Tsukinaga S, Matsunaga K, Nakayoshi T, Goda K, et al. New approach to diagnosing ampullary tumors by magnifying endoscopy combined with a narrow-band imaging system. J Gastroenterol. 2006;41:483–490. doi: 10.1007/s00535-006-1800-7. [DOI] [PubMed] [Google Scholar]
- 31.Shahid MW, Buchner A, Gomez V, Krishna M, Woodward TA, Raimondo M, Wallace MB. Diagnostic accuracy of probe-based confocal laser endomicroscopy and narrow band imaging in detection of dysplasia in duodenal polyps. J Clin Gastroenterol. 2012;46:382–389. doi: 10.1097/MCG.0b013e318247f375. [DOI] [PubMed] [Google Scholar]
- 32.Kikuchi D, Hoteya S, Iizuka T, Kimura R, Kaise M. Diagnostic algorithm of magnifying endoscopy with narrow band imaging for superficial non-ampullary duodenal epithelial tumors. Dig Endosc. 2014;26 Suppl 2:16–22. doi: 10.1111/den.12282. [DOI] [PubMed] [Google Scholar]
- 33.Dixon MF. Gastrointestinal epithelial neoplasia: Vienna revisited. Gut. 2002;51:130–131. doi: 10.1136/gut.51.1.130. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Goda K, Kikuchi D, Yamamoto Y, Takimoto K, Kakushima N, Morita Y, Doyama H, Gotoda T, Maehata Y, Abe N. Endoscopic diagnosis of superficial non-ampullary duodenal epithelial tumors in Japan: Multicenter case series. Dig Endosc. 2014;26 Suppl 2:23–29. doi: 10.1111/den.12277. [DOI] [PubMed] [Google Scholar]
- 35.Oka S, Tanaka S, Nagata S, Hiyama T, Ito M, Kitadai Y, Yoshihara M, Haruma K, Chayama K. Clinicopathologic features and endoscopic resection of early primary nonampullary duodenal carcinoma. J Clin Gastroenterol. 2003;37:381–386. doi: 10.1097/00004836-200311000-00006. [DOI] [PubMed] [Google Scholar]
- 36.Endo M, Abiko Y, Oana S, Kudara N, Chiba T, Suzuki K, Koizuka H, Uesugi N, Sugai T. Usefulness of endoscopic treatment for duodenal adenoma. Dig Endosc. 2010;22:360–365. doi: 10.1111/j.1443-1661.2010.01014.x. [DOI] [PubMed] [Google Scholar]
- 37.Honda T, Yamamoto H, Osawa H, Yoshizawa M, Nakano H, Sunada K, Hanatsuka K, Sugano K. Endoscopic submucosal dissection for superficial duodenal neoplasms. Dig Endosc. 2009;21:270–274. doi: 10.1111/j.1443-1661.2009.00908.x. [DOI] [PubMed] [Google Scholar]
- 38.Apel D, Jakobs R, Spiethoff A, Riemann JF. Follow-up after endoscopic snare resection of duodenal adenomas. Endoscopy. 2005;37:444–448. doi: 10.1055/s-2005-861287. [DOI] [PubMed] [Google Scholar]
- 39.Lépilliez V, Chemaly M, Ponchon T, Napoleon B, Saurin JC. Endoscopic resection of sporadic duodenal adenomas: an efficient technique with a substantial risk of delayed bleeding. Endoscopy. 2008;40:806–810. doi: 10.1055/s-2008-1077619. [DOI] [PubMed] [Google Scholar]
- 40.Alexander S, Bourke MJ, Williams SJ, Bailey A, Co J. EMR of large, sessile, sporadic nonampullary duodenal adenomas: technical aspects and long-term outcome (with videos) Gastrointest Endosc. 2009;69:66–73. doi: 10.1016/j.gie.2008.04.061. [DOI] [PubMed] [Google Scholar]
- 41.Abbass R, Rigaux J, Al-Kawas FH. Nonampullary duodenal polyps: characteristics and endoscopic management. Gastrointest Endosc. 2010;71:754–759. doi: 10.1016/j.gie.2009.11.043. [DOI] [PubMed] [Google Scholar]
- 42.Kedia P, Brensinger C, Ginsberg G. Endoscopic predictors of successful endoluminal eradication in sporadic duodenal adenomas and its acute complications. Gastrointest Endosc. 2010;72:1297–1301. doi: 10.1016/j.gie.2010.07.039. [DOI] [PubMed] [Google Scholar]
- 43.Kim HK, Chung WC, Lee BI, Cho YS. Efficacy and long-term outcome of endoscopic treatment of sporadic nonampullary duodenal adenoma. Gut Liver. 2010;4:373–377. doi: 10.5009/gnl.2010.4.3.373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Sohn JW, Jeon SW, Cho CM, Jung MK, Kim SK, Lee DS, Son HS, Chung IK. Endoscopic resection of duodenal neoplasms: a single-center study. Surg Endosc. 2010;24:3195–3200. doi: 10.1007/s00464-010-1114-y. [DOI] [PubMed] [Google Scholar]
- 45.Fanning SB, Bourke MJ, Williams SJ, Chung A, Kariyawasam VC. Giant laterally spreading tumors of the duodenum: endoscopic resection outcomes, limitations, and caveats. Gastrointest Endosc. 2012;75:805–812. doi: 10.1016/j.gie.2011.11.038. [DOI] [PubMed] [Google Scholar]
- 46.Min YW, Min BH, Kim ER, Lee JH, Rhee PL, Rhee JC, Kim JJ. Efficacy and safety of endoscopic treatment for nonampullary sporadic duodenal adenomas. Dig Dis Sci. 2013;58:2926–2932. doi: 10.1007/s10620-013-2708-8. [DOI] [PubMed] [Google Scholar]
- 47.Basford PJ, George R, Nixon E, Chaudhuri T, Mead R, Bhandari P. Endoscopic resection of sporadic duodenal adenomas: comparison of endoscopic mucosal resection (EMR) with hybrid endoscopic submucosal dissection (ESD) techniques and the risks of late delayed bleeding. Surg Endosc. 2014;28:1594–1600. doi: 10.1007/s00464-013-3356-y. [DOI] [PubMed] [Google Scholar]
- 48.Navaneethan U, Lourdusamy D, Mehta D, Lourdusamy V, Venkatesh PG, Sanaka MR. Endoscopic resection of large sporadic non-ampullary duodenal polyps: efficacy and long-term recurrence. Surg Endosc. 2014;28:2616–2622. doi: 10.1007/s00464-014-3512-z. [DOI] [PubMed] [Google Scholar]
- 49.Seo JY, Hong SJ, Han JP, Jang HY, Myung YS, Kim C, Lee YN, Ko BM. Usefulness and safety of endoscopic treatment for nonampullary duodenal adenoma and adenocarcinoma. J Gastroenterol Hepatol. 2014;29:1692–1698. doi: 10.1111/jgh.12601. [DOI] [PubMed] [Google Scholar]
- 50.Nonaka S, Oda I, Tada K, Mori G, Sato Y, Abe S, Suzuki H, Yoshinaga S, Nakajima T, Matsuda T, et al. Clinical outcome of endoscopic resection for nonampullary duodenal tumors. Endoscopy. 2015;47:129–135. doi: 10.1055/s-0034-1390774. [DOI] [PubMed] [Google Scholar]
- 51.Conio M, De Ceglie A, Filiberti R, Fisher DA, Siersema PD. Cap-assisted EMR of large, sporadic, nonampullary duodenal polyps. Gastrointest Endosc. 2012;76:1160–1169. doi: 10.1016/j.gie.2012.08.009. [DOI] [PubMed] [Google Scholar]
- 52.Koritala T, Zolotarevsky E, Bartley AN, Ellis CD, Krolikowski JA, Burton J, Gunaratnam NT. Efficacy and safety of the band and slough technique for endoscopic therapy of nonampullary duodenal adenomas: a case series. Gastrointest Endosc. 2015;81:985–988. doi: 10.1016/j.gie.2014.09.043. [DOI] [PubMed] [Google Scholar]
- 53.Basford PJ, Bhandari P. Endoscopic management of nonampullary duodenal polyps. Therap Adv Gastroenterol. 2012;5:127–138. doi: 10.1177/1756283X11429590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Jung JH, Choi KD, Ahn JY, Lee JH, Jung HY, Choi KS, Lee GH, Song HJ, Kim DH, Kim MY, et al. Endoscopic submucosal dissection for sessile, nonampullary duodenal adenomas. Endoscopy. 2013;45:133–135. doi: 10.1055/s-0032-1326178. [DOI] [PubMed] [Google Scholar]
- 55.Matsumoto S, Miyatani H, Yoshida Y. Endoscopic submucosal dissection for duodenal tumors: a single-center experience. Endoscopy. 2013;45:136–137. doi: 10.1055/s-0032-1310123. [DOI] [PubMed] [Google Scholar]
- 56.Takahashi T, Ando T, Kabeshima Y, Kawakubo H, Shito M, Sugiura H, Omori T. Borderline cases between benignancy and malignancy of the duodenum diagnosed successfully by endoscopic submucosal dissection. Scand J Gastroenterol. 2009;44:1377–1383. doi: 10.3109/00365520903287551. [DOI] [PubMed] [Google Scholar]
- 57.Lienert A, Bagshaw PF. Treatment of duodenal adenomas with endoscopic argon plasma coagulation. ANZ J Surg. 2007;77:371–373. doi: 10.1111/j.1445-2197.2007.04063.x. [DOI] [PubMed] [Google Scholar]
- 58.Kakushima N, Kanemoto H, Tanaka M, Takizawa K, Ono H. Treatment for superficial non-ampullary duodenal epithelial tumors. World J Gastroenterol. 2014;20:12501–12508. doi: 10.3748/wjg.v20.i35.12501. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Perez A, Saltzman JR, Carr-Locke DL, Brooks DC, Osteen RT, Zinner MJ, Ashley SW, Whang EE. Benign nonampullary duodenal neoplasms. J Gastrointest Surg. 2003;7:536–541. doi: 10.1016/S1091-255X(02)00146-4. [DOI] [PubMed] [Google Scholar]
- 60.Yan JQ, Peng CH, Yang WP, Ding JZ, Zhou GW, Ma D, Li HW. Surgical management of benign duodenal tumours. ANZ J Surg. 2010;80:526–530. doi: 10.1111/j.1445-2197.2010.05378.x. [DOI] [PubMed] [Google Scholar]
- 61.Abe N, Suzuki Y, Masaki T, Mori T, Sugiyama M. Surgical management of superficial non-ampullary duodenal tumors. Dig Endosc. 2014;26 Suppl 2:57–63. doi: 10.1111/den.12272. [DOI] [PubMed] [Google Scholar]
- 62.Zhang RC, Xu XW, Wu D, Zhou YC, Ajoodhea H, Chen K, Mou YP. Laparoscopic transduodenal local resection of periampullary neuroendocrine tumor: a case report. World J Gastroenterol. 2013;19:6693–6698. doi: 10.3748/wjg.v19.i39.6693. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Stauffer JA, Raimondo M, Woodward TA, Goldberg RF, Bowers SP, Asbun HJ. Laparoscopic partial sleeve duodenectomy (PSD) for nonampullary duodenal neoplasms: avoiding a whipple by separating the duodenum from the pancreatic head. Pancreas. 2013;42:461–466. doi: 10.1097/MPA.0b013e3182649956. [DOI] [PubMed] [Google Scholar]
- 64.Sakon M, Takata M, Seki H, Hayashi K, Munakata Y, Tateiwa N. A novel combined laparoscopic-endoscopic cooperative approach for duodenal lesions. J Laparoendosc Adv Surg Tech A. 2010;20:555–558. doi: 10.1089/lap.2009.0392. [DOI] [PubMed] [Google Scholar]
- 65.Ohata K, Murakami M, Yamazaki K, Nonaka K, Misumi N, Tashima T, Minato Y, Shozushima M, Mitsui T, Matsuhashi N, et al. Feasibility of endoscopy-assisted laparoscopic full-thickness resection for superficial duodenal neoplasms. ScientificWorldJournal. 2014;2014:239627. doi: 10.1155/2014/239627. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Brosens LA, Keller JJ, Offerhaus GJ, Goggins M, Giardiello FM. Prevention and management of duodenal polyps in familial adenomatous polyposis. Gut. 2005;54:1034–1043. doi: 10.1136/gut.2004.053843. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Lepistö A, Kiviluoto T, Halttunen J, Järvinen HJ. Surveillance and treatment of duodenal adenomatosis in familial adenomatous polyposis. Endoscopy. 2009;41:504–509. doi: 10.1055/s-0029-1214719. [DOI] [PubMed] [Google Scholar]
- 68.Picasso M, Filiberti R, Blanchi S, Conio M. The role of chromoendoscopy in the surveillance of the duodenum of patients with familial adenomatous polyposis. Dig Dis Sci. 2007;52:1906–1909. doi: 10.1007/s10620-006-9653-8. [DOI] [PubMed] [Google Scholar]
- 69.Dekker E, Boparai KS, Poley JW, Mathus-Vliegen EM, Offerhaus GJ, Kuipers EJ, Fockens P, Dees J. High resolution endoscopy and the additional value of chromoendoscopy in the evaluation of duodenal adenomatosis in patients with familial adenomatous polyposis. Endoscopy. 2009;41:666–669. doi: 10.1055/s-0029-1214980. [DOI] [PubMed] [Google Scholar]
- 70.Lopez-Ceron M, van den Broek FJ, Mathus-Vliegen EM, Boparai KS, van Eeden S, Fockens P, Dekker E. The role of high-resolution endoscopy and narrow-band imaging in the evaluation of upper GI neoplasia in familial adenomatous polyposis. Gastrointest Endosc. 2013;77:542–550. doi: 10.1016/j.gie.2012.11.033. [DOI] [PubMed] [Google Scholar]
- 71.Debinski HS, Trojan J, Nugent KP, Spigelman AD, Phillips RK. Effect of sulindac on small polyps in familial adenomatous polyposis. Lancet. 1995;345:855–856. [PubMed] [Google Scholar]
- 72.Penna C, Bataille N, Balladur P, Tiret E, Parc R. Surgical treatment of severe duodenal polyposis in familial adenomatous polyposis. Br J Surg. 1998;85:665–668. doi: 10.1046/j.1365-2168.1998.00684.x. [DOI] [PubMed] [Google Scholar]