

Abstract
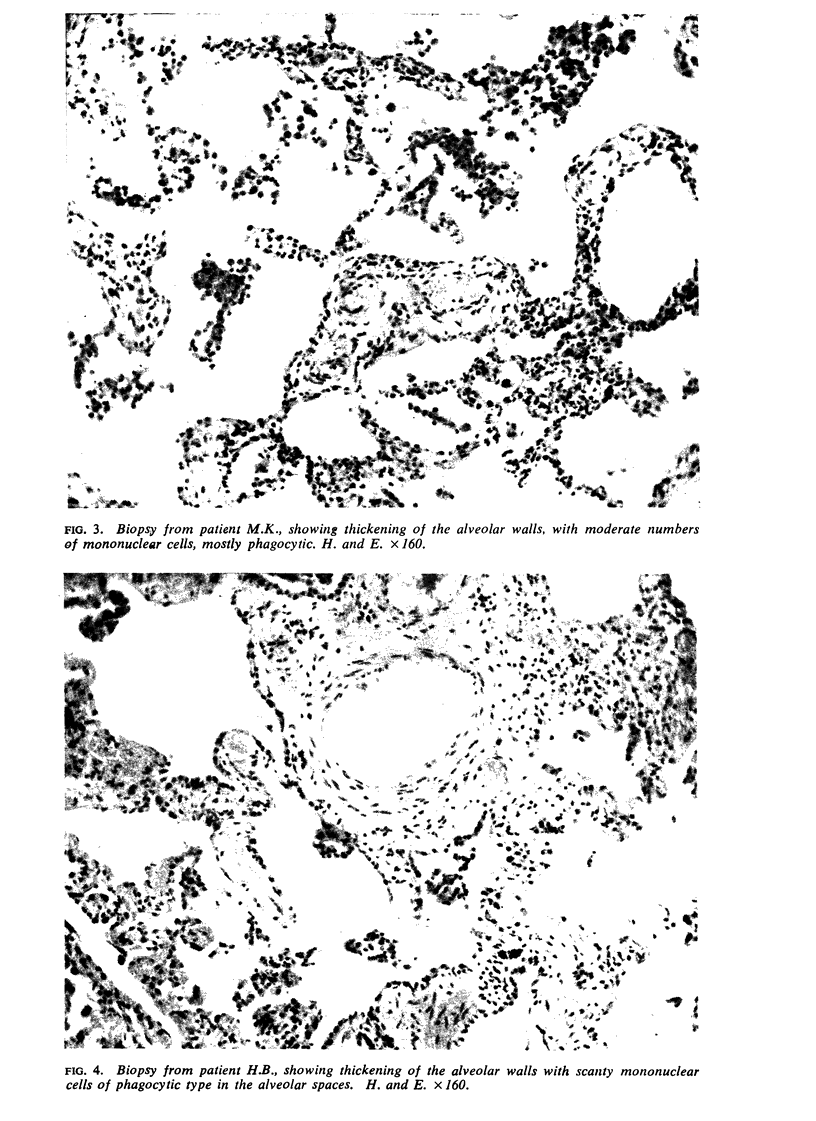
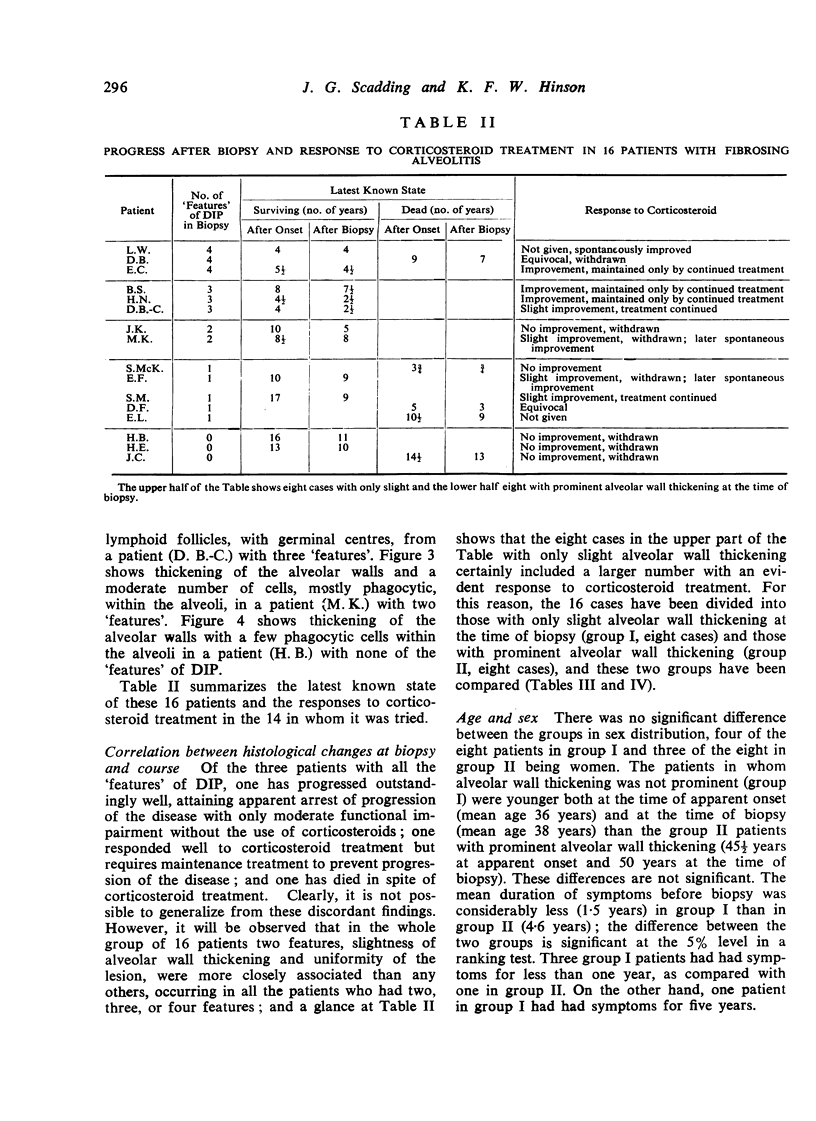
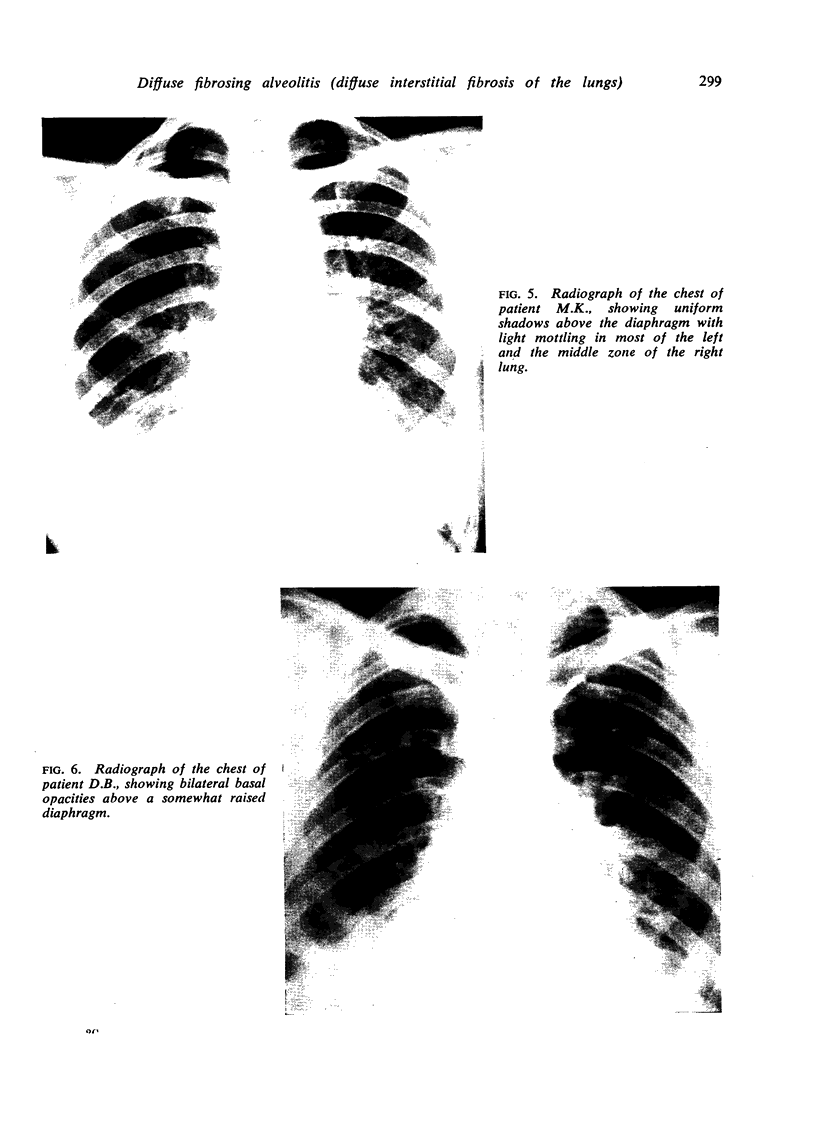
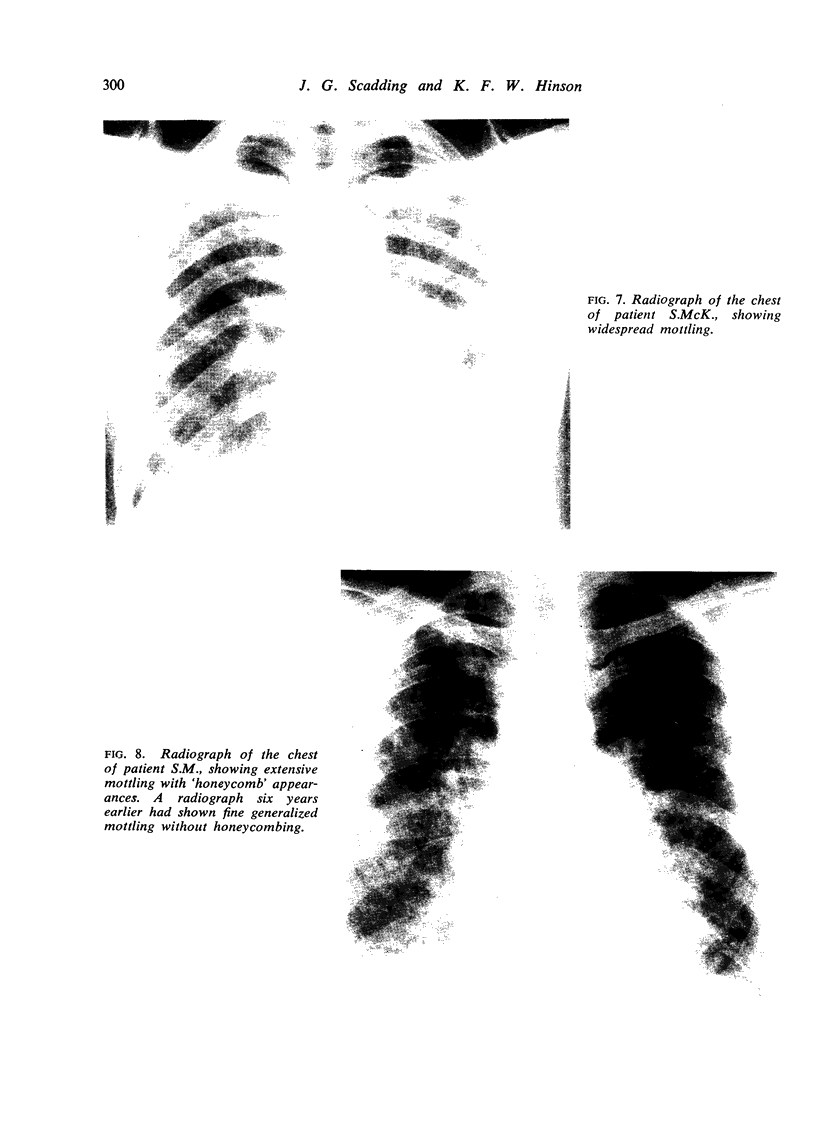
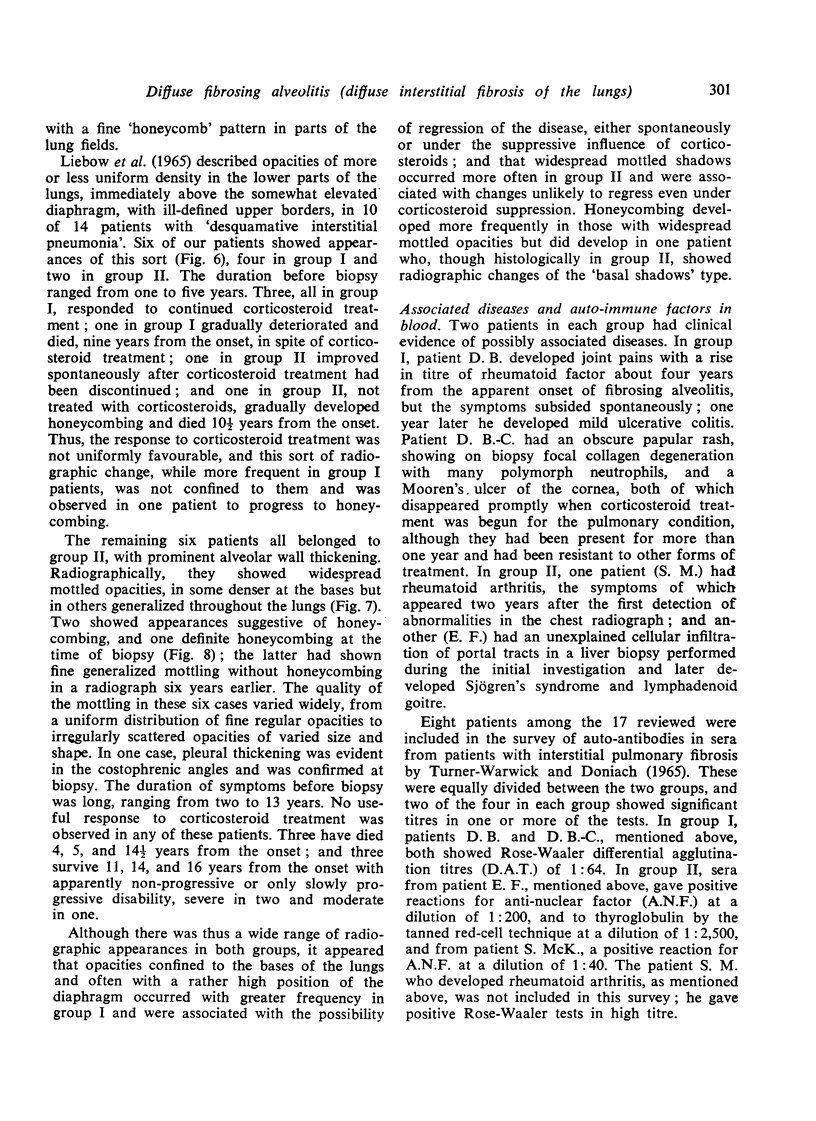
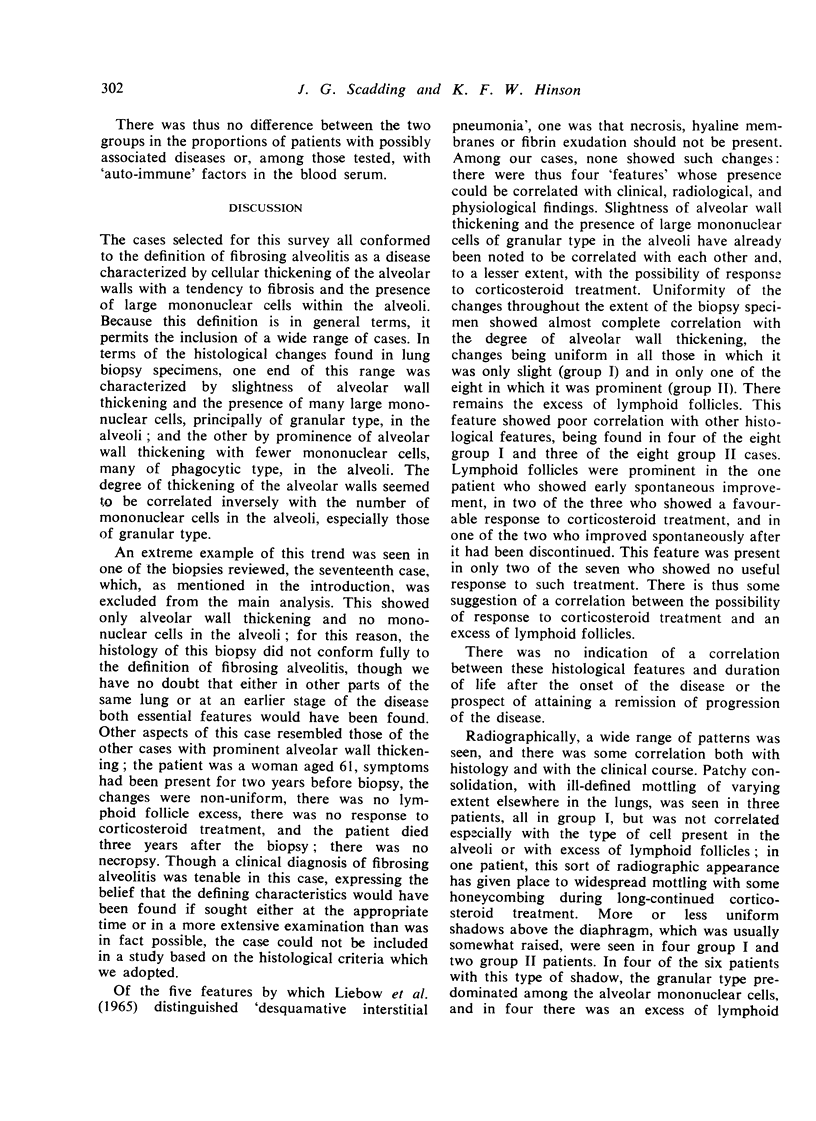
`Fibrosing alveolitis' refers to a broad general category of disease characterized by an inflammatory process in the lung beyond the terminal bronchiole having as its essential features (1) cellular thickening of the alveolar walls with a strong tendency to fibrosis, and (2) the presence of large mononuclear cells, presumably of alveolar origin, within the alveolar spaces. Sixteen cases in which lung biopsies conformed to this general pattern and whose course is known thereafter for at least two years or until death have been reviewed. There was an inverse relationship between the degree of alveolar wall thickening and the number of large mononuclear cells of granular type in the alveolar spaces. Corticosteroid treatment suppressed symptoms and signs in a few of the patients whose biopsy specimens showed only slight alveolar wall thickening and many intra-alveolar mononuclear cells but in none of those with much thickened alveolar walls. More or less prolonged remissions of progression of the disease were observed in a few patients, both with and without prominent alveolar wall thickening. There was no evident relationship between the histology at the time of biopsy and the total duration of the disease from onset to death.
Full text
PDF

Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- DAVIDSON J., GRANT I. W., HILLIS B. R. Diffuse interstitial fibrosis of the lungs (Hamman-Rich syndrome); a review with a report of three additional cases. Am Rev Tuberc. 1956 Oct;74(4):485–510. doi: 10.1164/artpd.1956.74.4.485. [DOI] [PubMed] [Google Scholar]
- LIEBOW A. A., STEER A., BILLINGSLEY J. G. DESQUAMATIVE INTERSTITIAL PNEUMONIA. Am J Med. 1965 Sep;39:369–404. doi: 10.1016/0002-9343(65)90206-8. [DOI] [PubMed] [Google Scholar]
- LIVINGSTONE J. L., LEWIS J. G., REID L., JEFFERSON K. E. DIFFUSE INTERSTITIAL PULMONARY FIBROSIS.A CLINICAL, RADIOLOGICAL, AND PATHOLOGICAL STUDY BASED ON 45 PATIENTS. Q J Med. 1964 Jan;33:71–103. [PubMed] [Google Scholar]
- RUBIN E. H., LUBLINER R. The Hamman-Rich syndrome: review of the literature and analysis of 15 cases. Medicine (Baltimore) 1957 Dec;36(4):397–463. doi: 10.1097/00005792-195712000-00001. [DOI] [PubMed] [Google Scholar]
- SCADDING J. G. Chronic diffuse interstitial fibrosis of the lungs. Br Med J. 1960 Feb 13;1(5171):443–450. doi: 10.1136/bmj.1.5171.443. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Stack B. H., Grant I. W., Irvine W. J., Moffat M. A. Idiopathic diffuse interstitial lung disease. A review of 42 cases. Am Rev Respir Dis. 1965 Dec;92(6):939–948. doi: 10.1164/arrd.1965.92.6P1.939. [DOI] [PubMed] [Google Scholar]
- TURNER-WARWICK M., DONIACH D. AUTO-ANTIBODY STUDIES IN INTERSTITIAL PULMONARY FIBROSIS. Br Med J. 1965 Apr 3;1(5439):886–891. doi: 10.1136/bmj.1.5439.886. [DOI] [PMC free article] [PubMed] [Google Scholar]