

Abstract
Objective
Suicide has been identified as a major public health issue. Exposure to suicide (i.e., knowing someone who died by suicide) is far more pervasive than previously considered and might be associated with significant adverse outcomes. As suicide becomes more commonly discussed in the public arena, a compelling need exists to determine who is exposed to suicide and how this exposure affects those left behind. This study estimated the proportion of the population exposed to suicide and delineated factors that predict significant psychiatric and psychosocial morbidity following that exposure.
Methods
A dual-frame random-digit-dial survey was conducted on a sample of 1,736 U.S. adults in the Commonwealth of Kentucky. Depression and anxiety were compared in suicide-exposed and suicide-unexposed individuals. Relationships were examined between psychiatric outcomes and perceptions of closeness to the decedent.
Results
Forty-eight percent of weighted participants (n=816/1,687) reported lifetime exposure to suicide. Current depression and anxiety symptoms were higher in suicide-exposed than in suicide-unexposed individuals. Suicide-exposed individuals were twice as likely as suicide-unexposed individuals to have diagnosable depression and almost twice as likely to have diagnosable anxiety. Suicide-exposed individuals were more likely than suicide-unexposed individuals to report suicide ideation (9% vs. 5%). Closeness to the decedent increased the odds of depression and anxiety and almost quadrupled the odds of posttraumatic stress disorder.
Conclusion
Exposure to suicide is pervasive and occurs beyond family; as such, it is imperative to identify those with perceived closeness to the decedent. This hidden cohort of suicide-exposed people is at elevated risk for psychopathology and suicidal ideation.
Suicide ranks as one of the leading causes of preventable deaths around the world, making it a public health issue. Approximately one million people globally, including more than 38,000 people in the United States, die by suicide every year.1,2
The father of modern suicidology, Edwin Shneidman, estimated that six people were bereaved by every suicide death,3 although this figure was not based on any empirical evidence. This estimate would identify one in every 64 Americans, or 1.5% of the U.S. population, as a survivor of suicide (i.e., someone whose life has been significantly affected by a suicide).4
Exposure to suicide (i.e., knowing someone who died by suicide) is much more pervasive than previously thought and might be associated with significant adverse outcomes. A recent look at the language around suicide bereavement suggests that the term “exposed to suicide” should be used to describe anyone who knows or identifies with someone who dies by suicide and not merely those who witnessed the death.5
Although previous research has examined suicide exposure within a particular time frame, no research has established what proportion of the population has experienced lifetime exposure to suicide, nor has it delineated factors that predict significant psychiatric and psychosocial morbidity following that exposure. In a 1994 telephone survey of the U.S. general population, 7% of respondents reported that they knew someone who died by suicide in the past year, including 1% who reported losing a relative and 5% who reported such exposure to the suicide death of a friend or acquaintance.6 In a more recent small survey, Cerel and colleagues reported that 40% of participants in a random-digit-dial (RDD) survey of residents of one U.S. state reported lifetime exposure to suicide, with almost 20% reporting that the suicide had a significant impact on their lives.7
A growing body of evidence points to the deleterious impact of suicide on immediate kin.8–11 People bereaved by suicide have been shown to be at risk for their own suicidal behavior, posttraumatic stress disorder (PTSD), prolonged grief, and depression.12,13 Despite these findings, evidence on the effect of suicide death on non-kin relationships, such as classmates14 and coworkers,15 is just beginning to emerge. Clinicians have suggested that suicide bereavement is qualitatively different from that experienced by people bereaved by other abrupt deaths.16 Among people exposed to traumatic death, 35% to 40% will experience prolonged grief and other disabling conditions, another 35% to 40% will regain a balanced life within two years, and the final 20% to 30% will not be significantly affected.17 It is likely, however, that perceived closeness to the decedent, rather than kin relationship, is the key predictor of who will be most impacted by a suicide death.7
Understanding who is exposed to and affected by suicide is important to determine how to best identify and intervene with those at risk for possible deleterious outcomes following suicides in communities. In this study, we evaluated whether or not a participant had been exposed to suicide and then examined the demographic characteristics of suicide-exposed individuals and possible psychiatric risk from that exposure to suicide, and then determined factors that may place them at risk for poor psychiatric outcomes.
METHODS
Data sources
An RDD survey of adults in the Commonwealth of Kentucky was conducted from July 2012 through June 2013. The Commonwealth of Kentucky was selected for the study because it has a sizable military population; as such, it was considered appropriate to find a sufficient sample of veterans.
A dual-frame sample of landline and cell phone numbers, weighted to reflect the true distribution of landline only, cell phone only, and dual-use households in Kentucky, was used to achieve a final sample of 1,736 respondents. Respondents were contacted using a modified, list-assisted Mitofsky-Waksberg RDD method (landline)18 or a cellular RDD (cell phone) sampling technique.19 The Kentucky Survey Research Center was contracted to conduct the telephone interviews. The samples (landline and cell phones) were generated from the Marketing Systems Group's Virtual Genesys product.20 The landline sample was then screened for known business and nonworking numbers prior to dialing.
Because this study was part of a larger study examining suicide exposure in veterans, veterans were deliberately overenrolled compared with their prevalence in the population. The caller initially tried to determine whether or not there was a veteran at the phone number; if not, an adult male was asked to participate. If no veteran or adult male was available, the adult female who answered the phone or another adult female at the residence was asked to participate. This sampling strategy ensured that the sample population of nonveterans was not heavily weighted with women, who might be at home more often and able or willing to answer the telephone. Each number in the sample was contacted up to 15 times. In addition, for those initial calls where contact was successful but the time was not convenient, up to 10 scheduled callbacks were made and one refusal conversion was attempted.
After the target number of 800 nonveterans (n=805) was reached utilizing this methodology, interviews were obtained only of veterans (n=931) to complete the agreed-upon sample size, which resulted in a Council of American Survey Research Organizations (CASRO) response rate of 36%. The CASRO response rate assumes that the nonrespondents in the screening operation had the same eligibility characteristics as those who were successfully screened.21 A large number of refusals were actually hang-ups where we could not determine eligibility.
Overall, calls averaged 12.7 minutes (95% confidence interval [CI] 6.8, 18.6) in length. Following oral consent, the respondent was interviewed by telephone.
Independent variables
Exposure to suicide.
Participants were asked if they knew anyone during their lifetime who died by suicide with the question, “Do you know anyone who has died by suicide?” Those who reported this, exposure to a suicide death, were then asked, “On a 1 to 5 scale with 1 meaning ‘not close’ and 5 meaning ‘very close,’ how close would you describe your relationship with this person?” To assess for recency of the event, participants were asked about the year of death with the question, “Thinking about the year of the suicide that impacted you the most, in what year did the death occur?” Social and/or familial relationship to decedent was measured by an open-ended question, “What was your relationship to the person who died by suicide (they were my__)?.” Finally, individuals were asked how many people the participants had known who had died by suicide.
Demographics.
Demographic data included age, race, sex, marital status, rural/urban residence status based on county of residence, status as a parent (yes/no), and veteran status (yes/no).
Dependent variables
Anxiety and depression.
The Patient Health Questionnaire (PHQ) anxiety and depression modules were used to assess depressive and anxiety symptoms in the last two weeks. The anxiety module (PHQ-GAD-7) includes seven questions, while the depression module (PHQ-DEP9) includes nine questions, one of which is about suicidal ideation. An answer of “yes” to four or more symptoms on each module equates to a probable diagnosis of anxiety or depression. The PHQ takes less than three minutes to administer and has shown good agreement with diagnoses made by independent mental health professionals (for the diagnosis of any one or more PHQ disorders, k=0.65, overall accuracy = 85%, sensitivity = 75%, and specificity = 90%). A conservative cutoff of 10 on each measure was used to indicate moderate symptoms and a probable diagnosis.22 Less conservative cutoff values are lower than 10.
PTSD.
The Short Screening Scale for PTSD is a seven-item measure used to determine PTSD symptoms related to the suicide. Of the seven items, five items query about avoidance and numbing and two items query about hyperarousal. A score of ≥4 on this scale defines probable diagnosis of PTSD, and the scale has been shown to have a sensitivity of 80% and specificity of 97%.23 These items were only administered to participants who indicated they had exposure to suicide and were asked about symptoms since the death.
Analyses
Two-tailed t-tests, chi-squared analysis, and bivariate odds ratios were used to examine group differences and associations between sociodemographic independent variables and responses to the dichotomous variable of suicide exposure. Statistical significance was set at p<0.01.
Hierarchical logistic regression analyses were performed to assess for outcomes of depression, anxiety diagnoses, and suicide ideation in the full population and depression, anxiety, and PTSD in the suicide-exposed subsample. For the full sample analyses, the independent variables for each model were entered in two blocks: (1) veteran status, age, sex, race, rural/urban status; and (2) suicide exposure. For the suicide-exposed subsample analyses, the independent variables for each model were entered in three blocks: (1) veteran status, age, sex, race, rural/urban status; (2) number of people known to have died by suicide and recency of exposure; and (3) perceived closeness to the decedent. A receiver operator characteristics (ROC) analysis was undertaken for each stage of each model to assess sensitivity and accuracy of the models.
Weights
The purpose of this study was to examine a representative population of one southern U.S. state, yet our initial respondents reflected oversampling of veterans. Thus, additional weights were added after taking into account census proportions for veterans and non-veterans to account for oversampling of the veteran population. The weighted sample of 1,703 participants was intended to reflect true population distributions and approximate 2010 U.S. Census estimates for Kentucky for telephone ownership type24 (i.e., landline telephone only, cell phone only, and both landline and cell phone), sex, age, and veteran status.25
RESULTS
Sample demographics
The telephone survey was completed by 1,736 participants, 931 (54%) of whom were veterans. The sample of 1,703 participants had a mean weighted age of 54 years (95% CI 38, 70; range: 19–101) and a median weighted age of 54 years (Table 1). The weighted sample included 784 (46%) males and 919 (54%) females, as well as 181 (11%) veteran participants, similar to the percentage of veterans who reside in the state. Approximately 1,516 (90%) respondents in the weighted sample reported their race/ethnicity as white, 93 (6%) as African American, 20 (1%) as Native American, 17 (1%) as Hispanic, and 43 (3%) as other. The majority of participants (n=992, 58%) were married and 1,132 (80%) reported having children (including adult children). Most of the weighted sample (n=1,527, 90%) reported living in urban areas, while 167 (10%) reported living in rural counties (Table 1).
Table 1.
Comparison of characteristics of suicide-exposed and suicide-unexposeda participants in a random-digit-dial survey, Kentucky, July 2012–June 2013a
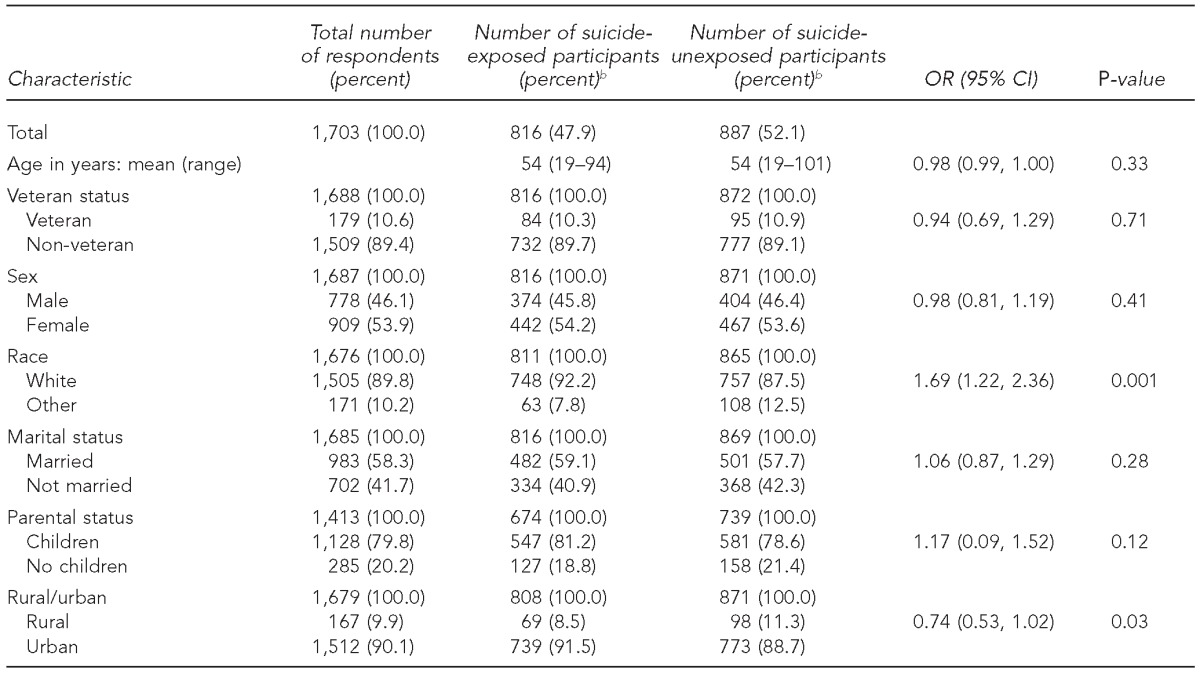
Frequency counts based on total number of recipients who answered each item under analysis.
bProportions are weighted and incorporate sampling weights.
OR = odds ratio
CI = confidence interval
Exposure to suicide
Of the 1,688 participants in the weighted sample who responded to the suicide exposure item, 816 (48%) reported exposure to suicide. Fifteen individuals did not respond to this question and were excluded from further analyses. Demographic characteristics were then examined to determine their association with differences in rates of exposure. The only statistically significant demographic characteristic, or the likelihood that a result or relationship is caused by something other than mere random chance, was race (50% exposure among white people vs. 37% exposure among nonwhite people, c2[1]=10.17, p<0.001). No differences in suicide exposure were noted in relation to veteran status, sex, age, marital status, parental status, or rural-urban status (Table 1).
Association of exposure to suicide with psychiatric risk
Depression and anxiety scores in exposed and unexposed individuals were compared to determine whether or not there were mean differences between these groups. Depression mean scores were higher for suicide-exposed (n=785, mean = 5.31, 95% CI –0.11, 10.73) compared with suicide-unexposed (n=826, mean = 3.92, 95% CI –0.48, 8.32, t[1,512]=–5.64, p<0.001) individuals. Anxiety scores were also higher for suicide-exposed (n=804, mean = 4.86, 95% CI 0.60, 10.32) compared with suicide-unexposed (n=863, mean = 3.45, 95% CI –0.93, 7.83, t[1,537]=–5.79, p<0.001) individuals.
Chi-squared tests for association found cutoff scores for depression were met by 19% of suicide-exposed compared with 10% of suicide-unexposed individuals (p<0.001). Cutoff scores for anxiety (PHQ-GAD) were met by 19% of suicide-exposed compared with 11% of suicide-unexposed individuals (p<0.001) (Table 2).
Table 2.
Prevalence and odds of depression, diagnosis, anxiety diagnosis, and suicidal ideation status, by suicide exposure status, in a random-digit-dial survey, Kentucky, July 2012–June 2013a
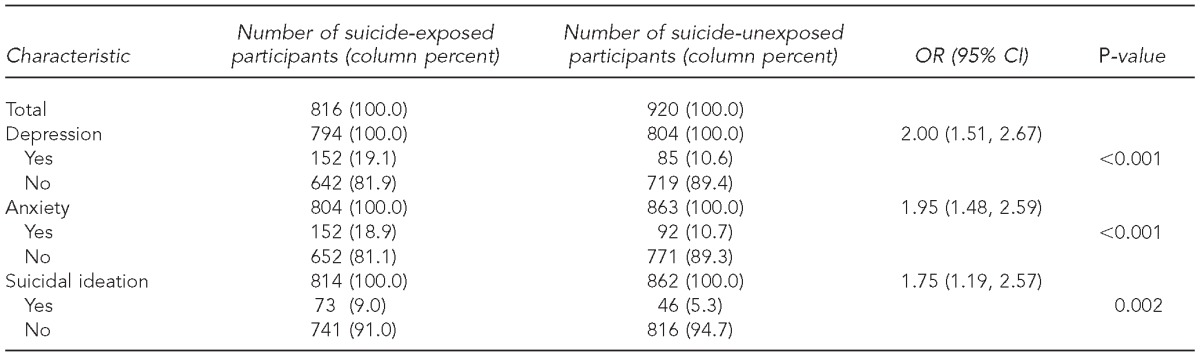
Frequency counts based on total number of recipients who answered each item under analysis. Analyses were conducted on both weighted and unweighted data with similar results. Weighted coefficients are reported. Denominators differ due to missing data.
bAll proportions are weighted and incorporate sampling weights.
OR = odds ratio
CI = confidence interval
A dichotomous item was also used to assess differences in any suicidal ideation vs. no suicidal ideation between groups. A statistically significant difference was found between suicide-exposed (9%) and suicide-unexposed (5%) (p=0.01) individuals in experiencing any level of suicidal ideation in the past two weeks (Table 2).
Finally, logistic regression analyses using covariates of veteran status, age, sex, race, and rural/urban status found that compared with suicide-unexposed individuals, suicide-exposed individuals were twice as likely to have diagnosable depression (adjusted odds ratio [AOR] = 2.13, 95% CI 1.59, 2.86), almost twice as likely to have diagnosable anxiety (AOR=1.93, 95% CI 1.45, 2.57), and almost twice as likely to have suicidal ideation (AOR=1.77, 95% CI 1.21, 2.61). Analyses were conducted on both weighted and unweighted data with similar results.
Risk factors for adverse psychiatric outcomes among suicide-exposed individuals
When participants were asked to state their relationship with the person who died by suicide, their open-ended responses were coded by two authors into non-relative, first-degree relative (e.g., parent, spouse, or sibling), or second-degree relative (e.g., uncle, aunt, nephew, niece, grandparent, grandchild, or half-sibling). Among them, 64% reported the loss of a non-relative, 27% reported the loss of a second-degree relative, and 10% reported the loss of a first-degree relative. Closeness scores averaged 2.95 (95% CI 2.85, 3.06) on a five-point scale (1 = not close and 5 = very close), with 21% scoring 1, 17% scoring 2, 25% scoring 3, 18% scoring 4, and 18% scoring 5. Of the 802 suicide-exposed individuals, 58% reported they knew more than one person who had died by suicide. On average, suicide-exposed participants reported they knew almost three people (2.75, 95% 2.45, 3.05; range: 1–50) who had died by suicide. Seventeen participants (1% of the sample) reported exposure to more than 10 suicides. Participants exposed to multiple suicides were asked to determine the death that caused the most impact on them, and, in terms of timing of the suicide, on average the death for which the respondent reported the most impact occurred (15.29, 95% CI 14.30, 16.27; range: 0–73).
People exposed to suicide were queried about PTSD specifically around the event. Cutoff scores for PTSD from the suicide were met by 87 (11%) respondents.
The number of suicide exposures and perceived closeness to decedent emerged as significant in the final stages of the model for each diagnosis. For each incremental change in the number of suicide exposures, the odds of depression (AOR=1.07, 95% CI 1.02, 1.13), anxiety (OR=1.10, 95% CI 1.03, 1.17), and PTSD (OR=1.09, 95% CI 1.02, 1.17) were slightly increased. For each incremental change in closeness to decedent, the odds of depression and anxiety were almost doubled (AOR=1.64, 95% CI 1.39, 1.93 for depression; AOR=1.68, 95% CI 1.43, 1.98 for anxiety) and the odds of PTSD were almost quadrupled (AOR=3.68, 95% CI 2.69, 5.04) (p<0.001 for all) (Table 3).
Table 3.
Adjusted odds of depression, anxiety, and posttraumatic stress disorder for suicide-exposed individuals, by recency of loss, number known who died by suicide, and perceived closeness, in a random-digit-dial survey, Kentucky, July 2012–June 2013
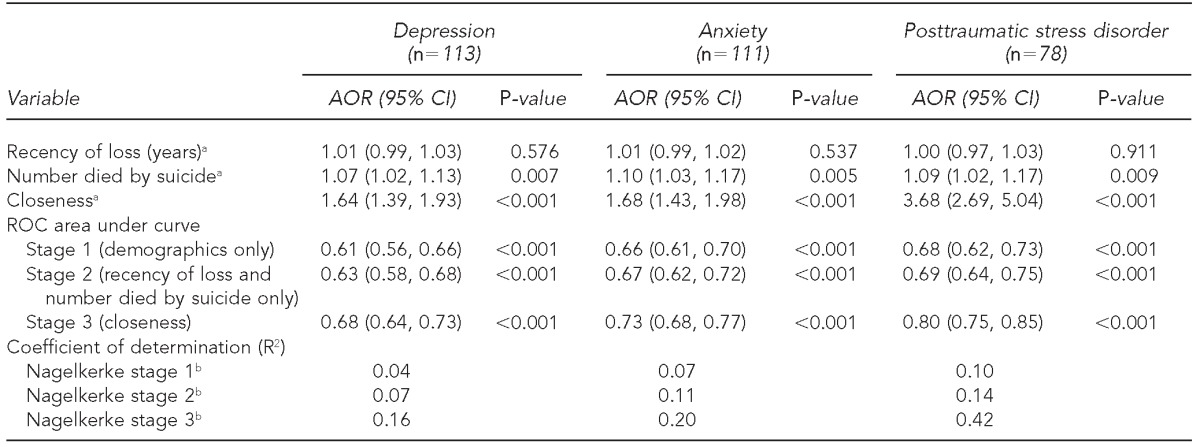
NOTE: All data weighted. Analyses were conducted on both weighted and unweighted data with similar results. Weighted coefficients are reported. All coefficients reported are from final stage (stage 3) of the analysis. Covariates were veteran status, age, sex, race, and rural/urban status.
aRecency of loss is defined as the number of years since the suicide that affected the participant the most. Number died by suicide is the total number of suicide exposures reported by the participant. Closeness is defined as the level of perceived closeness to the suicide decedent on a scale from 1 to 5.
bNagelkerke measurements denote amount of variance explained per stages 1–3 of each model.
AOR = adjusted odds ratio
CI = confidence interval
ROC = receiver operator characteristic
Each stage of the three models predicted mental health outcomes significantly better than chance. Only slight changes of area under the curve (AUC) occurred between the first two stages of each model (2% change in the depression model, 1% change in the anxiety model, and 1% change in the PTSD model). The highest percentage increase in AUC occurred with the addition of perceived closeness to each model (5% change in AUC for depression, 6% change in AUC for anxiety, and 11% change in AUC for PTSD) (Table 3).
DISCUSSION
This study is the first large, population-based study to examine exposure to suicide in the general population. Almost half of participants (48%) reported exposure to one or more suicides. Overall, demographic characteristics were not associated with suicide exposure; like suicide itself, only a few demographic groups were disproportionately affected. The only -demographic variable that was different in terms of exposure was race, with a higher percentage of white people reporting suicide exposure. This finding is unsurprising, because in the Commonwealth of Kentucky, similar to that of the United States, the age-adjusted suicide rate for white people is almost three times the suicide rate for black people (15 vs. 5 per 100,000 population).26
We next examined whether or not exposure to suicide was associated with psychiatric risk. Suicide-exposed individuals were twice as likely as suicide-unexposed individuals to meet screening criteria for depression and almost twice as likely to meet screening criteria for anxiety. Given that approximately half of the population in this representative, population-based sample was exposed to suicide, this vulnerability to psychiatric risk associated with suicide exposure is of concern.
Previously, researchers and clinicians considered suicide's impact on kin to be the primary consequence of this tragic event. We need to reconceptualize suicide bereavement to account for exposure and perceptions of closeness regardless of the categorical relationship to the decedent. Instead, we imagine the impact of suicide to be more diffuse and not restricted to loved ones or family members. Replication of this research, both nationally and internationally, will help shed light on the breadth of the impact of suicide exposure.
Limitations
This study was subject to several limitations. First, the study's cross-sectional design limited any assertions of causality and the study's retrospective nature may have introduced recall bias into study estimates. In addition, a need to acknowledge the long time span between exposure and the study is warranted. Longitudinal studies will be necessary to examine how ratings of personal impact of the death are related to scope, intensity, and length of the impact.5 Second, because the study was drawn from a single southern U.S. state, its generalizability is limited. Third, during the phone interview, we initially queried for a veteran living in the home, which limited the representativeness of the study sample because phone numbers answered by a veteran who agreed to participate were not also eligible for the overall sampling. The inclusion of a cell phone sample and the higher-than-usual obtained sample of men made it more representative than other RDD studies. RDD studies have historically had much higher response rates that can currently be obtained, and these rates have dropped in recent years. The main danger with the modest response rate was that nonrespondents differed from respondents.
Fourth, the sample was weighted to reflect the demographics of the state population in an attempt to reduce the nonresponse bias. People with higher levels of psychiatric symptoms might recall suicides in their lifetime more easily than those without current psychiatric symptoms. To counter this possible confounder, symptoms of depression and anxiety were assessed prior to assessment of suicide exposure in this survey. If anything, it is possible that suicide exposure was underreported because of individuals' reluctance to disclose stigmatizing topics. Because there are a wide range of personal characteristics and life events that could mediate the impact of suicide exposure on an individual (e.g., social support and exposure to the violent details of the death itself), it is also essential that future research delineates variables that might be associated with better or worse responses.5
CONCLUSIONS
It is critical to continue to investigate the psychological well-being of those exposed to suicide to fully appreciate the outcome of suicide death in the community. Most physicians and health professionals are accustomed to working with close relatives only and are unaware of the existence of this hidden cohort of suicide-exposed people who are themselves at risk for psychopathology and suicide.
These findings may inform clinical practice by providing insight into the psychiatric risk associated with suicide exposure and perceptions of closeness to the decedent, which were previously underappreciated. These findings may also assist clinicians in identifying and intervening with those at risk for adverse mental health outcomes.
These results suggest that it will no longer be sufficient for clinicians to ask merely about a family history of suicide. It will also be important for clinicians to probe for any exposure to suicide, regardless of relationship, especially those in which the patient feels particularly close to the person who died by suicide.
These findings should help improve crisis response, “postvention” efforts, and institutional policies in the wake of suicides occurring in a community, workplace, or school. Postvention is an intervention that provides support for the bereaved, works to reduce further suicide risk among impacted communities, and engages individuals who might be influenced by exposure to suicide. By considering the potential breadth of exposure within the population, rather than calculating risk from a narrower group of affected individuals, suicide's true impact will be appreciated.
Footnotes
All authors received funding from the Military Suicide Research Consortium to support this work. The views expressed in this article are those of the authors and do not necessarily represent the official policy or position of the Department of Veterans Affairs, Department of Defense (DoD), or the U.S. government.
This research was supported, in part, by grants awarded to the Denver VA Medical Center (grant #W81XWH-10-2-0178) and to Florida State University (grant #W81XWH-10-2-0181) by the DoD. The DoD had no further role in the study design; the collection, analysis, and interpretation of data; the writing of the report; or in the decision to submit the article for publication.
This study was approved by the University of Kentucky Institutional Review Board and reviewed by DoD's Human Research Protection Office.
REFERENCES
- 1.World Health Organization. Geneva: WHO; 2012. Public health action for the prevention of suicide: a framework. [Google Scholar]
- 2.Caine ED. Forging an agenda for suicide prevention in the United States. Am J Public Health. 2013;103:822–9. doi: 10.2105/AJPH.2012.301078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shneidman ES, Cain A, editors. Survivors of suicide. Springfield (IL): Charles C. Thomas; 1972. [Google Scholar]
- 4.McIntosh JL. Washington: American Association of Suicidology; 2014. U.S.A. suicide 2013: official final data. Also available from: http://mypage.iu.edu/~jmcintos/2013datapgs.pdf [cited 2015 Jul 2] [Google Scholar]
- 5.Cerel J, McIntosh JL, Neimeyer RA, Maple M, Marshall D. The continuum of “survivorship”: definitional issues in the aftermath of suicide. Suicide Life Threat Behav. 2014;44:591–600. doi: 10.1111/sltb.12093. [DOI] [PubMed] [Google Scholar]
- 6.Crosby AE, Sacks JJ. Exposure to suicide: incidence and association with suicidal ideation and behavior: United States, 1994. Suicide Life Threat Behav. 2002;32:321–8. doi: 10.1521/suli.32.3.321.22170. [DOI] [PubMed] [Google Scholar]
- 7.Cerel J, Maple M, Aldrich R, van de Venne J. Exposure to suicide and identification as survivor. Results from a random digit dial survey. Crisis. 2013;34:413–9. doi: 10.1027/0227-5910/a000220. [DOI] [PubMed] [Google Scholar]
- 8.Melhem NM, Porta G, Shamseddeen W, Walker Payne M, Brent DA. Grief in children and adolescents bereaved by sudden parental death. Arch Gen Psychiatry. 2011;68:911–9. doi: 10.1001/archgenpsychiatry.2011.101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Maple M, Edwards H, Plummer D, Minichiello V. Silenced voices: hearing the stories of parents bereaved through the suicide death of a young adult child. Health Soc Care Community. 2010;18:241–8. doi: 10.1111/j.1365-2524.2009.00886.x. [DOI] [PubMed] [Google Scholar]
- 10.Cerel J, Fristad MA, Weller EB, Weller RA. Suicide-bereaved children and adolescents: a controlled longitudinal examination. J Am Acad Child Adolesc Psychiatry. 1999;38:672–9. doi: 10.1097/00004583-199906000-00013. [DOI] [PubMed] [Google Scholar]
- 11.Dyregrov K, Dyregrov A. Siblings after suicide: “the forgotten bereaved”. Suicide Life Threat Behav. 2005;35:714–24. doi: 10.1521/suli.2005.35.6.714. [DOI] [PubMed] [Google Scholar]
- 12.Jordan JR. Is suicide bereavement different? A reassessment of the literature. Suicide Life Threat Behav. 2001;31:91–102. doi: 10.1521/suli.31.1.91.21310. [DOI] [PubMed] [Google Scholar]
- 13.Jordan JR, McIntosh JL. New York: Brunner-Routledge; 2010. Grief after suicide: understanding the consequences and caring for the survivors. [Google Scholar]
- 14.Bartik W, Maple M, Edwards H, Keirnan M. Adolescent survivors of suicide: Australian young people's bereavement narratives. Crisis. 2013;34:211–7. doi: 10.1027/0227-5910/a000185. [DOI] [PubMed] [Google Scholar]
- 15.Lynn CW. When a coworker completes suicide. AAOHN J. 2008;56:459–67. doi: 10.3928/08910162-20081101-02. [DOI] [PubMed] [Google Scholar]
- 16.Cerel J, Jordan JR, Duberstein PR. The impact of suicide on the family. Crisis. 2008;29:38–44. doi: 10.1027/0227-5910.29.1.38. [DOI] [PubMed] [Google Scholar]
- 17.Bonanno GA. New York: Basic Books; 2009. The other side of sadness: what the new science of bereavement tells us about life after loss. [Google Scholar]
- 18.Marketing Systems Group. Mitofsky-Waksberg sampling [cited 2015 Feb 1] Available from: http://www.genesys-sampling.com/pages/template2/site2/60/default.aspx.
- 19.Marketing Systems Group. Cellular random-digit dial (RDD) sample [cited 2015 Feb 1] Available from: http://www.m-s-g.com/web/genesys/cell-phone-sample.aspx.
- 20.Marketing Systems Group. Genesys for Windows. Horsham (PA): Marketing Systems Group; 2013. [Google Scholar]
- 21.Council of American Survey Research Organizations. Port Jefferson (NY): CASRO; 1982. Special report on the definition of response rates. Also available from: https://c.ymcdn.com/sites/www.casro.org/resource/resmgr/docs/casro_on_definitions_of_resp.pdf [cited 2015 Jul 2] [Google Scholar]
- 22.Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 1999;282:1737–44. doi: 10.1001/jama.282.18.1737. [DOI] [PubMed] [Google Scholar]
- 23.Breslau N, Peterson EL, Kessler RC, Schultz LR. Short screening scale for DSM-IV posttraumatic stress disorder. Am J Psychiatry. 1999;156:908–11. doi: 10.1176/ajp.156.6.908. [DOI] [PubMed] [Google Scholar]
- 24.Blumberg SJ, Luke JV, Ganesh N, Davern ME, Boudreaux MH. Wireless substitution: state-level estimates from the National Health Interview Survey, 2010–2011. Natl Health Stat Rep. 2012;61:1–16. [PubMed] [Google Scholar]
- 25.Census Bureau (US) State & county quickfacts: Kentucky 2010 [cited 2014 Jun 17] Available from: http://quickfacts.census.gov.
- 26.Centers for Disease Control and Prevention (US) Injury prevention and control data: data and statistics (WISQARS™): fatal injury data, 2012 [cited 2014 Jun 7] Available from: http://www.cdc.gov/injury/wisqars/fatal.html.