

Abstract
Background
Violence during childhood may affect short and long-term educational factors. There is scant literature on younger children from resource poor settings.
Methods
This study assessed child violence experiences (harsh punishment and exposure to domestic or community violence) and school enrolment, progress and attendance in children attending community-based organisations in South Africa and Malawi (n=989) at baseline and at 15 months' follow-up, examining differential experience of HIV positive, HIV affected and HIV unaffected children.
Results
Violence exposure was high: 45.4% experienced some form of psychological violence, 47.8% physical violence, 46.7% domestic violence and 41.8% community violence. Primary school enrolment was 96%. Violence was not associated with school enrolment at baseline but, controlling for baseline, children exposed to psychological violence for discipline were more than ten times less likely to be enrolled at follow-up (OR 0.09; 95% CI 0.01 to 0.57). Harsh discipline was associated with poor school progress. For children HIV positive a detrimental effect of harsh physical discipline was found on school performance (OR 0.10; 95% CI 0.02 to 0.61).
Conclusion
Violence experiences were associated with a number of educational outcomes, which may have long-term consequences. Community-based organisations may be well placed to address such violence, with a particular emphasis on the challenges faced by children who are HIV positive.
Keywords: Educational outcomes, Children and young people, Maltreatment, Malawi, South Africa, Violence
Introduction
The experience of violence in childhood is all too common.1 A recent WHO report documented that a quarter of adults report abuse of some form in childhood.2 Childhood exposure to violence is associated with a range of negative adult outcomes.2 A number of researchers have proposed definitions and ways to codify violence.3 The nature of the experience allows for distinctions between physical,4 psychological and sexual violence.5 Yet describing the acts may not fully capture the impact of the violence on a child where the same act may have differential impacts.6 Violence has been examined from the home, school and community perspectives.7 However, there may be overlap and interconnection between these.8 Violence in one domain may have ramifications for outcomes in another, and cumulative or multiple violence exposure may occur across domains.9
There is solid evidence for the effects of violence on child mental health. A recent systematic review10 showed the link between child maltreatment and mental disorders, drug use, suicide attempts, sexually transmitted infections and risky sexual behaviour. Children witnessing violence or experiencing abuse themselves are affected in terms of behavioural problems11 and child aggression.12
The evidence for the impact on educational outcomes is not as substantive.13 Educational outcomes are measured in a number of ways, including years of school completed, post-school education, school performance, school attendance, school progress and school dropout.14 Maltreated children perform lower on standardised tests15 and on other academic outcomes such as reading ability.16 Yet not all children exposed to violence struggle academically.17 A recent review13 examined links between childhood maltreatment and school achievement. Most studies are retrospective with children and youth recalling experiences—predominantly multiple maltreatment,18 early onset of violence and out of home care. Many of the studies are skewed as they draw their sample from children within special educational or welfare sectors,19 and psychiatric populations.20 Educational outcomes are often measured with single items. Many studies are confined to adolescence, and younger children are not well represented. Furthermore, many studies are cross-sectional and do not follow up the children over time. The specific forms of violence experienced may need to be examined, as well as contextual factors such as poverty, unemployment, migration and HIV infection.
There is also limited data from low- and middle-income countries (LMICs), even in the context of high levels of violence.21,22 In both South Africa and Malawi, high community violence rates have been recorded.23,24 In Malawi, violence is a key barrier for girls attending and performing well in school25 and impedes academic progress.26 A large South African study27 examined adolescent risk pathways and found that both community violence and child abuse contributed to multiple negative outcomes for children. Exposure to maltreatment for instance predicted adolescent transactional sex.28 Educational outcomes were affected by HIV/AIDS orphanhood and caregiver HIV/AIDS sickness, mediated by living in poverty and child internalising problems. However, these studies focus on adolescent samples (10–17 years) and it would be of interest to track such effects on younger children.28
This study examined the relationship between exposure to violence at home or in the community and educational outcomes for young children aged 4–13 years in South Africa and Malawi at baseline and follow-up (12–15 months later). Given the literature on HIV, orphanhood and educational outcomes,29 specific attention was given to children who were HIV positive and HIV affected children (defined here as those who are HIV negative themselves but live in a household with someone who is HIV positive) in order to explore the effects of HIV as a driver of either violence experience or educational risk in this age group.
Methods
The study reports on data from the Child Community Care study, a longitudinal study of children affected by HIV/AIDS enrolled at community-based organisations (CBOs) in South Africa and Malawi. Baseline data were collected in 2011–2012 with follow-up 12–15 months later.
Sample
CBOs were recruited by drawing up a list of all funded programmes from 11 partner organisations: UNICEF, Save the Children, Bernard van Leer Foundation, Firelight Foundation, World Vision, Comic Relief, REPSSI, Stop AIDS Now, HelpAge, Diana Memorial Fund and the AIDS Alliance. The 588 CBOs that were provided (524 in South Africa and 64 in Malawi) were stratified by funder and geographical region and 28 were randomly selected for inclusion (24 in South Africa and 4 in Malawi—prorated according to population size). Consecutive children aged 4–13 years and their primary caregiver were interviewed from each CBO with a 99% response rate. Interviews were conducted by trained data collectors using mobile phone technology.30
Measures
Child education status
Three education measures were used. School enrolment was measured based on whether the children were enrolled in school. School progress was measured by whether the children were in their age appropriate grade. School attendance was measured by how often children attended school (4=regularly, 3=sometimes, 2=rarely or 1=never). All three items were measured using carer report based on the Child Status Index education domain31 and Pediatric Quality of Life inventory.32
Child violence measures
Exposure to four types of violence was measured. Domestic violence was measured using child-report scale items from a UNICEF survey tool for orphans and vulnerable children33 that enquired about children's exposure to violence in the household as a witness. Exposure was measured with two items: if they ever saw their caregivers hit each other or if they ever saw their caregivers shout at each other. Answers were dichotomous (1=yes, 2=no). Having ever experienced either of the two qualified as having witnessed domestic violence.
Harsh discipline practices that involved punishment or maltreatment in the household were reported by the carer using items from the Parent-Child Conflict Tactics Scale34 and from the International Society for the Prevention of Child Abuse and Neglect (ISPCAN) screening tools35—generating a psychological and a physical violence score. For psychological violence, caregivers were asked four questions about whether and how often they used several psychological strategies to discipline their children (i.e. threatening to send them away, sending them to bed without food, threatening with ghosts or calling them names). Answers ranged from 1=weekly to 4=never. Having ever used any such strategy (answering 1=weekly, 2=monthly or 3=less often) qualified as the caregivers using any harsh psychological discipline. For physical violence, caregivers were asked two questions about whether and how often they used several physically violent measures to discipline their children (i.e. slapping them or hitting them with a stick/hard object). Answers ranged from 1=weekly to 4=never. Having ever used any of these disciplinary strategies qualified as the caregivers using any harsh physical discipline.
Exposure to community violence was assessed using child-report scale items from the UNICEF survey tool that enquired about child's exposure to different forms of violence within the community, both as a victim and witness. Exposure to community violence was measured using three items: whether the children had ever beaten anyone up, whether they had been beaten up outside the home or had ever seen anyone else attacked on the street. Answers were dichotomous (1=yes, 2=no). Having ever experienced any of the three qualified as having experienced community violence.
Data analysis
The data were analysed using SPSS V.22, IBM Corp, Armonk, NY.36 After descriptive analysis to explore frequency data, logistic regressions were used for binary outcomes variables. Linear regressions were used for scale outcomes variables. All analyses were controlled for country, child gender and age, whether the child had lost either or both biological parents, and caregiver education. All types of violence were added in the regression models simultaneously and are thus controlling for each other.
Results
Participants included 989 children (503; 50.9% girls) aged 4–13 years (mean 8.91 years, SD=2.84) attending CBOs in South Africa and Malawi together with their primary caregiver. Of the 989 children, 135 (13.7%) were HIV positive, 222 (22.4%) HIV negative but someone else in their household had HIV, and 632 (63.9%) were neither HIV infected nor affected. Altogether, 19.1% (189) of the caregivers said that they were HIV positive. Out of all the children, 453 (45.8%) had at least one parent die, 574 (58%) reported living in a comfortable home and 856 (86.6%) reported having enough to eat most of the time.
Children who were lost to follow-up (n=156; 15.8%) were more often from South Africa (145; 92.9%) than those who were followed up (129; 82.7%; χ2(1)=10.42; p=0.001). They were also more likely to live in a shack (39; 25.3%) than those who were followed up (18; 13.8%; χ2(1)=12.61; p<0.001), and were less likely to live in a comfortable home (50.7% [79] vs 60.0% [500]; χ2(1)=4.47; p=0.035), but those lost to follow-up were more often food secure (80.1% [125] vs 71.8% [598]; χ2(1)=4.65; p=0.031). Children who were lost to follow-up and children who were followed up did not differ significantly on any of the violence measures at baseline, nor on school progression and attendance. However, those who were lost to follow-up were less often enrolled in school at baseline (145; 92.9%) than those who were followed up (125; 96.9%; χ2(1)=5.64; p=0.018). Those lost to follow-up did not differ on any other demographic variables.
Violence experiences and educational measures
Table 1 describes violence experiences and educational measures. School enrolment was high (952; 96.3%) overall. Yet only 68.3% (675) were in the correct class for their age (only half of children HIV positive were in the correct class [65; 50.0%] compared to 170 [79.1%] of the HIV affected children and 440 [72.5%] of the HIV unaffected children). Attendance was high with 911 (95.7%) attending regularly. Children with HIV had slightly lower attendance (91.5% [119] vs 95.8% [206] of the HIV affected children and 96.5% [586] of the HIV unaffected children).
Table 1.
Baseline descriptive statistics on the occurrence of different kinds of violence and performance in school for the total sample and the sample split by HIV status
| Total sample N=989 | HIV postive N=135 | HIV affected N=222 | HIV unaffected N=632 | χ2 (p-value) | |
|---|---|---|---|---|---|
| Educational measures | |||||
| Enrolled in school | 952 (96.3%) | 130 (96.3%) | 215 (96.8%) | 607 (96.0%) | 0.29 (NS) |
| Correct class | 675 (68.3%) | 65 (50.0%) | 170 (79.1%) | 440 (72.5%) | 35.22 (<0.001) |
| Attendance | |||||
| Regularly | 911 (95.7%) | 119 (91.5%) | 206 (95.8%) | 586 (96.5%) | 15.56 (0.016) |
| Sometimes | 32 (3.4%) | 7 (5.4%) | 8 (3.7%) | 17 (2.8%) | |
| Rarely | 4 (0.4%) | 3 (2.3%) | – | 1 (0.2%) | |
| Never | 5 (0.5%) | 1 (0.8%) | 1 (0.5%) | 5 (0.5%) | |
| Violence measures | |||||
| Discipline: any psychological violence | 449 (45.4%) | 60 (44.4%) | 112 (50.5%) | 277 (43.8%) | 2.96 (NS) |
| Disciple: threaten to send child away | |||||
| Weekly | 3 (0.3%) | – | – | 3 (0.5%) | 8.41 (NS) |
| Monthly | 11 (1.1%) | 1 (0.7%) | 3 (1.4%) | 7 (1.1%) | |
| Less often | 155 (15.7%) | 27 (20.0%) | 43 (19.4%) | 85 (13.4%) | |
| Never | 820 (82.9%) | 107 (79.3%) | 176 (79.3%) | 537 (85.0%) | |
| Discipline: threaten with ghosts | |||||
| Weekly | 4 (0.4%) | – | 1 (0.5%) | 3 (0.5%) | 3.96 (NS) |
| Monthly | 20 (2.0%) | 3 (2.2%) | 7 (3.2%) | 10 (1.6%) | |
| Less often | 132 (13.3%) | 16 (11.9%) | 34 (15.3%) | 82 (13.0%) | |
| Never | 833 (84.2%) | 116 (85.9%) | 180 (81.1%) | 537 (85.0%) | |
| Discipline: withhold meals | |||||
| Weekly | 1 (0.1%) | 1 (0.7%) | – | – | 10.97 (NS) |
| Monthly | 1 (0.1%) | – | 1 (0.5%) | – | |
| Less often | 33 (3.3%) | 3 (2.2%) | 6 (2.7%) | 24 (3.8%) | |
| Never | 954 (96.5%) | 131 (97.0%) | 215 (96.8%) | 608 (96.2%) | |
| Discipline: call dumb, lazy or names | |||||
| Weekly | 23 (2.3%) | 4 (3.0%) | 5 (2.3%) | 14 (2.2%) | 3.47 (NS) |
| Monthly | 24 (2.4%) | 1 (0.7%) | 8 (3.6%) | 15 (2.4%) | |
| Less often | 247 (25.0%) | 32 (23.7%) | 57 (25.7%) | 158 (25.0%) | |
| Never | 695 (70.3%) | 98 (72.6%) | 152 (68.5%) | 445 (70.4%) | |
| Discipline: any physical violence | 473 (47.8%) | 63 (46.7%) | 124 (55.9%) | 286 (45.3%) | 7.49 (0.024) |
| Discipline: use sticks belts or hard object to hit the child | |||||
| Weekly | 4 (0.4%) | – | 3 (1.4%) | 1 (0.2%) | 13.90 (0.031) |
| Monthly | 30 (3.0%) | 5 (3.7%) | 8 (3.6%) | 17 (2.7%) | |
| Less often | 415 (42.0%) | 56 (41.5%) | 108 (48.6%) | 251 (39.7%) | |
| Never | 540 (54.6%) | 74 (54.8%) | 103 (46.4%) | 363 (57.4%) | |
| Discipline: slap or punched the child – head or face (ever) | |||||
| Weekly | 1 (0.1%) | – | 1 (0.5%) | – | 13.93 (0.030) |
| Monthly | 4 (0.4%) | – | – | 4 (0.6%) | |
| Less often | 66 (6.7%) | 9 (6.7%) | 24 (10.8%) | 33 (5.2%) | |
| Never | 918 (92.8%) | 126 (93.3%) | 197 (88.7%) | 595 (94.1%) | |
| Any domestic violence | 441 (45.4%) | 57 (42.2%) | 125 (56.8%) | 259 (42.0%) | 15.04 (0.001) |
| Adults at home hit each other | 201 (20.7%) | 25 (18.5%) | 58 (26.4%) | 118 (19.1%) | 5.63 (NS) |
| Adults shout at each other | 417 (42.9%) | 53 (39.3%) | 118 (53.6%) | 246 (39.9%) | 13.40 (0.001) |
| Any community violence | 413 (42.5%) | 57 (42.2%) | 112 (50.9%) | 244 (39.5%) | 8.57 (0.014) |
| Seen someone being attacked outside home | 354 (36.4%) | 50 (37.0%) | 95 (43.2%) | 209 (33.9%) | 6.09 (0.048) |
| Been attacked outside the home | 132 (13.6%) | 21 (15.6%) | 41 (18.6%) | 70 (11.3%) | 7.87 (0.020) |
| Beaten someone up ever | 309 (31.6%) | 44 (32.6%) | 83 (37.6%) | 182 (29.2%) | 5.33 (NS) |
NS: not significant; –: is indicative of zero participants within the group.
A third of the sample (354; 36.4%) had seen someone attacked near their home. For discipline, 17.1% (169) of children had been threatened to be sent away, 15.8% (156) had been threatened with ghosts and 3.5% (35) had meals withheld. Name calling was common (29.7%; 294), as was hitting with a stick (45.4%; 449). Overall, 449 children (45.4%) reported any form of psychological violence, 473 (47.8%) any form of physical violence, 441 (45.4%) witnessed domestic violence and 413 (42.5%) reported exposure to community violence. Violence burden was calculated to examine how many children experienced none of the four violence measures (15.7%; 155), one type (25.7%; 254), two types (29.3%; 290), three types (19.8%; 196) or all four types of violence (9.5%; 94).
Violence and school performance at baseline
School enrolment
No violence measures were significantly associated with school enrolment for the total sample or for the sample according to HIV status. Overall school enrolment was high (96.3%; 952) and represents a ceiling effect.
Grade progression
Experiencing any physical violence as a form of discipline was associated with a lower odds of being in the correct class (OR 0.57; 95% CI 0.38 to 0.85; see Figure 1). This finding was not different between HIV infected, affected and unaffected children. However, domestic violence was found to be positively associated with grade progression, but only for children in households with no HIV (OR 2.02; 95% CI 1.24 to 3.29). No association was found for children HIV positive (OR 0.56; 95% CI 0.20 to 1.55) or for HIV affected children (OR 0.85; 95% CI 0.34 to 2.13). No other type of violence was associated with school progression at baseline.
Figure 1.

Odds ratio of being in the correct class as a function of type of violence experienced at baseline. Any physical violence was the only significant factor, having a negative effect on whether the child is in the right class or not. *p<0.01. This figure is available in black and white in print and in color at International Health online.
School attendance
A multiple linear regression analysis showed no association of any form of violence with school attendance at baseline.
Longitudinal effect of violence variables on school performance
School enrolment
A multiple logistic regression analysis on the entire sample showed an effect of using psychological violence to discipline the child on school enrolment at follow-up. Controlling for school enrolment at baseline, the children of caregivers using psychological violence for discipline were more than ten times less likely to be enrolled in school at follow-up if they had not been enrolled at baseline (OR 0.09; 95% CI 0.01 to 0.57; see Figure 2). An analysis broken down by HIV status could not be performed because too few children HIV positive and HIV affected children were not enrolled in school. No other type of violence was found to have an effect on school enrolment at follow-up.
Figure 2.
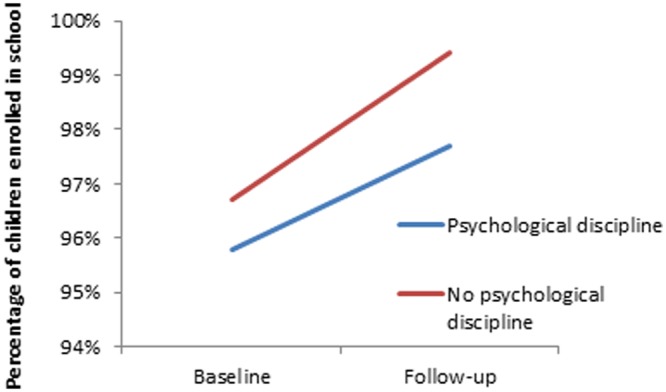
Difference in school enrolment at baseline and follow-up between children who do and do not experience psychological violence as a form of discipline. Children who did not experience psychological violence had significantly lower enrolment at follow-up controlled for baseline enrolment than children who did not experience psychological violence (OR 0.09; 95% CI 0.01–0.57). This figure is available in black and white in print and in color at International Health online.
Grade progression
No form of violence exposure predicted grade progression at follow-up for the whole sample. However, breaking down the analysis by HIV burden, it was found that for HIV positive children (OR 0.10; 95% CI 0.02 to 0.61), but not for the HIV affected (OR 0.59; 95% CI 0.20 to 1.72) and HIV unaffected children (OR 1.31; 95% CI 0.76 to 2.26) using physical violence to discipline the child had a detrimental effect on grade progression (see Figure 3). This indicated that children HIV positive were much less likely to be in the appropriate grade at follow-up when experiencing physical violence at baseline, controlling for grade at baseline. No effect was found for any of the other types of violence on grade progression at follow-up.
Figure 3.
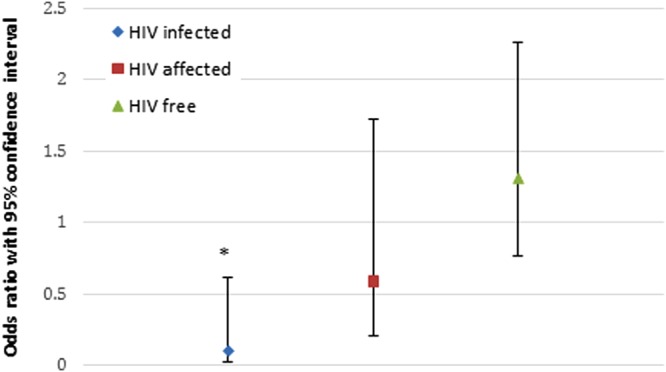
Odds ratio of being in a correct class at follow-up when having experienced physical violence as a form of discipline at baseline as a function of HIV status. For children with HIV, physical violence results in a much lower chance of being in the correct class follow-up, whereas this was not the case for the HIV affected and HIV free children. *p<0.05. This figure is available in black and white in print and in color at International Health online.
School attendance
No effect of any type of violence was found on school attendance at follow-up, controlling for school attendance at baseline (see Table 2).
Table 2.
Overview of found effects in the current study of different types of violence on several educational measures
| School enrolment |
School attendance |
School progress |
||||
|---|---|---|---|---|---|---|
| Discipline | Baseline | Follow-up | Baseline | Follow-up | Baseline | Follow-up |
| Psychological violence | No effect | Significant effect | No effect | No effect | No effect | No effect |
| Physical violence | No effect | No effect | No effect | No effect | Significant effect | Only for HIV infected children |
| Domestic violence | No effect | No effect | No effect | No effect | Only for HIV unaffected children | Significant effect |
Discussion
This study tested the effect of exposure to home and community violence and harsh discipline practices on selected educational outcomes in South Africa and Malawi for primary school children aged 4–13 years. There is very little data available on the relationship between violence and educational outcomes in young children from Sub-Saharan Africa and this is one of the first longitudinal studies to track violence exposure and educational outcomes over time.
In this sample of young children, exposure to violence at home and in the community was very high. Over half had been exposed to two or more types of violence, whereas less than one in six reported no violence exposure at all. At both baseline and at follow-up, we did not find a relationship between community violence and school enrolment, attendance or grade progression. However, we did find a link between violence experienced in the home and schooling outcomes. In terms of enrolment, there was no link between exposure to violence and school enrolment at baseline, but at follow-up children were significantly less likely to be enrolled in school if they were exposed to harsh psychological discipline. Children who experienced harsh physical punishment were less likely to be in the correct grade for their age at baseline. At follow-up, this was still the case, but only for HIV positive children. Witnessing domestic violence was not associated with school enrolment, attendance or grade progression for the full sample at baseline or follow-up. At baseline we noted that exposure to domestic violence predicted higher rates of grade progression at baseline for HIV unaffected children. However, this relationship was not present at follow-up. The relationships between violence exposure and child development is an intricate one, especially in a CBO context. An explanation for this counterintuitive finding may be that children experiencing domestic violence got more help and attention at the CBO, compensating for the otherwise negative experience.
Our data reveal some important findings. First, there are high rates of violence exposure in this population. This has been noted previously in other studies from these countries and the region in general.21,22,36,37 A report on the use of corporal punishment in LMICs found that corporal punishment was very prevalent in several sub-Saharan African countries, with more than 80% of children in the region reporting being beaten at home.38 In both Malawi and South Africa there are also high rates of community and domestic violence. In South Africa, rates of perpetration of physical violence against a partner are as high as 40%,39 while in Malawi 28.5% of women report being exposed to abuse by their partners.40 Children in these countries are also witnesses to violence; in South Africa, 45% of children have witnessed their mother being beaten.41
Second, we found that this exposure to violence has an impact on education outcomes. Specifically, we found an impact of harsh punishment on school enrolment and performance. In terms of enrolment, both countries have policies of universal primary education—with R1 (which should be universally implemented in South Africa) for 4–5 year olds and reception grades commencing at 6 years. We found high school enrolment rates of 96.2% in South Africa and 96.8% in Malawi. However, in spite of this, we found that harsh psychological punishment predicted significantly lower school enrolment at follow-up. This is concerning, as universal primary school education is a core global development priority, with school dropout rates dropping by nearly 50% between 2000 and 2015.42 Research into children being out of school in South Africa has identified costs of transport, child labour in the home or elsewhere, illness, disability and poor school performance as drivers of dropout.43 In Malawi, reasons for non-enrolment include long distances to school and poor quality of available schooling and infrastructure. We located one study from Malawi in which researchers found a high prevalence of violence against girls at home, in the community and at school. The research noted that violence against girls had a negative impact on girls attending and performing well in school.44 However, emotional abuse has not previously specifically been identified as a major barrier to enrolment and may need to be considered more carefully in future research. In addition, this study found that harsh physical violence appeared to affect grade progression—a possible proxy measure for school performance.
Finally, our findings also highlight that children who are HIV positive in particular appear to be most at risk of poor educational outcomes in the context of high exposure to violence. This is likely to be due to a range of inter-related risk factors that affect educational outcomes. We know that many of the risk factors for violence against children are prevalent in families and communities affected by HIV/AIDS.45 Children who are HIV positive have been shown to perform more poorly than their peers on a range of cognitive tests and are also more likely to have mental health problems.46 Further, other factors such as parental death, shifting care arrangements, change in school, illness-induced poverty and increased caregiving responsibilities might affect a child's ability to access schooling and perform well in the context of HIV.47
Given that in this study educational outcomes were specifically linked to exposure to harsh punishment, as opposed to community or domestic violence, CBOs providing services for children affected by HIV/AIDS may be key to intervening on this issue. There is growing interest in the development and implementation of parenting programmes in LMIC settings, with two recently completed reviews of research on this topic indicating a small but growing evidence base.48,49 Current efforts, such as WHO's Parenting for Lifelong Health programme,50 are focused on developing and implementing evidence-based parenting interventions that are appropriate for roll-out in LMIC settings. There is also existing evidence for the role of trained community workers in the rollout of such interventions.51,52 CBOs are well-placed to work with marginalised and isolated families, and support of children in the context of their homes not just at formal services such as clinics or schools,53 and should be engaged in these efforts.
The study has a number of limitations. The sample was drawn from community-based organisation attendees and as such is a group who are already in receipt of some form of intervention; thus, findings cannot automatically generalise to the population at large. Previous studies on violence and educational outcomes focus mainly on school-based violence. The violence measures in this study were confined to the home and the community, and it may well be that children are also being exposed to violence in schools, which was not monitored. Measures were self-report rather than observational, but both caregivers and children reported on outcomes. Response rate at follow-up was 86% and, although high, there may be specific limitations as a result.
These findings suggest that in high HIV endemic countries, younger children are at risk of exposure to a number of harsh discipline practices and witness both domestic and community violence, which in turn may affect educational progress, through enrolment or progression in the first place or attendance and achievements within the classroom setting. Younger children are particularly vulnerable and educational achievement in the early years is an important prerequisite for ongoing educational milestones.
Acknowledgments
Authors' contributions: All authors contributed to the conceptualisation of the study and the analysis plan. IH analysed and interpreted the data. LS drafted and wrote the paper. All authors critically revised the paper for intellectual content and read and approved the final manuscript. LS is guarantor of the paper.
Acknowledgements: We acknowledge the support of Zena Jacobs with all logistics, Natasha Croome, all the Community-Based Organisations, data collectors, children and caregivers, as well as the Coalition for Children Affected by AIDS and the Know Violence in Childhood initiative.
Funding: Funding for the study was provided by Norad/Sweden through a nesting agreement with Help Age.
Competing interests: None declared.
Ethical approval: The study was approved from ethics boards at University College London (reference number 1478/002) and Stellenbosch University (reference number N10/04/112).
References
- 1.Hovdestad W, Campeau A, Potter D, Tonmyr L. A systematic review of childhood maltreatment assessments in population-representative surveys since 1990. PLoS One 2015;10:e0123366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.WHO. Global Status Report on Violence Prevention. Geneva: World Health Organization; 2014. [Google Scholar]
- 3.Barnett D, Manly JT, Cicchetti D. Defining child maltreatment: The interface between policy and research. In: Cicchetii D, Toth. SL (editors). Child abuse, child development, and social policy. New Jersey: Ablex, 1993; 7–74. [Google Scholar]
- 4.Stoltenborgh M, Bakermans-Kranenburg MJ, van Ijzendoorn MH, Alink LR. Cultural-geographical differences in the occurrence of child physical abuse? A meta-analysis of global prevalence. Int J Psychol 2013;48:81–94. [DOI] [PubMed] [Google Scholar]
- 5.Stoltenborgh M, van Ijzendoorn MH, Euser EM, Bakermans-Kranenburg MJ. A global perspective on child sexual abuse: meta-analysis of prevalence around the world. Child Maltreat 2011;16:79–101. [DOI] [PubMed] [Google Scholar]
- 6.Lau AS, Leeb RT, English D et al. . What's in a name? A comparison of methods for classifying predominant type of maltreatment. Child Abuse Negl 2005;29:533–51. [DOI] [PubMed] [Google Scholar]
- 7.Petrenko CL, Friend A, Garrido EF et al. . Does subtype matter? Assessing the effects of maltreatment on functioning in preadolescent youth in out-of-home care. Child Abuse Negl 2012;36:633–44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Pears KC, Kim HK, Fisher PA. Psychosocial and cognitive functioning of children with specific profiles of maltreatment. Child Abuse Negl 2008;32:958–71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Milaniak I, Widom CS. Does child abuse and neglect increase risk for perpetration of violence inside and outside the home? Psychol Violence 2015;5:246–255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Norman RE, Byambaa M, De R, Butchart A et al. . The long-term health consequences of child physical abuse, emotional abuse, and neglect: a systematic review and meta-analysis. PLoS Med 2012;9):e100134. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Blair F, McFarlane J, Nava A et al. . Child witness to domestic abuse: baseline data analysis for a seven-year prospective study. Pediatr Nurs 2015;41:23–9. [PubMed] [Google Scholar]
- 12.Skinner AT, Bacchini D, Lansford JE et al. . Neighborhood danger, parental monitoring, harsh parenting, and child aggression in nine countries. Societies (Basel) 2014;4:45–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Romano E, Babchishin L, Marquis R, Fréchette S. Childhood maltreatment and educational outcomes. Trauma Violence Abuse 2015;16:418–37. [DOI] [PubMed] [Google Scholar]
- 14.Pieterse D. Childhood maltreatment and educational outcomes: evidence from South Africa. Health Econ 2015;24:876–94. [DOI] [PubMed] [Google Scholar]
- 15.Eckenrode J, Rowe E, Laird M, Brathwaite J. Mobility as a mediator of the effects of child maltreatment on academic performance. Child Dev 1995;66:1130–42. [PubMed] [Google Scholar]
- 16.Perez CM, Widom CS. Childhood victimization and long-term intellectual and academic outcomes. Child Abuse Negl 1994;18:617–33. [DOI] [PubMed] [Google Scholar]
- 17.Coohey C, Renner LM, Hua L et al. . Academic achievement despite child maltreatment: a longitudinal study. Child Abuse Negl 2011;35:688–99. [DOI] [PubMed] [Google Scholar]
- 18.Finkelhor D, Ormrod RK, Turner HA. Polyvictimization and trauma in a national longitudinal cohort. Dev Psychopathol 2007;19:149–66. [DOI] [PubMed] [Google Scholar]
- 19.Jonson-Reid M, Drake B, Kim J et al. . A prospective analysis of the relationship between reported child maltreatment and special education eligibility among poor children. Child Maltreatment 2004;9:382–94. [DOI] [PubMed] [Google Scholar]
- 20.Buckle SK, Lancaster S, Powell MB, Higgins DJ. The relationship between child sexual abuse and academic achievement in a sample of adolescent psychiatric inpatients. Child Abuse Negl 2005;29:1031–47. [DOI] [PubMed] [Google Scholar]
- 21.Meinck F, Cluver LD, Boyes ME. Household illness, poverty and physical and emotional child abuse victimisation: Findings from South Africa's first prospective cohort study. BMC Public Health 2015;15:444. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Meinck F, Cluver LD, Boyes ME, Mhlongo EL. Risk and protective factors for physical and sexual abuse of children and adolescents in Africa: A review and implications for practice. Trauma Violence Abuse 2015;16:81–107. [DOI] [PubMed] [Google Scholar]
- 23.Richter L, Dawes A. Child abuse in South Africa: rights and wrongs. Child Abuse Rev 2008;17:79–93. [Google Scholar]
- 24.Norman R, Matzopoulos R, Groenewald P, Bradshaw D. The high burden of injuries in South Africa. Bull World Health Organ 2007;87:695–702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Bisika T, Ntata P, Konyani S. Gender-violence and education in Malawi: a study of violence against girls as an obstruction to universal primary school education. J Gender Studies 2009;18:287–94. [Google Scholar]
- 26.Dunne M, Humphreys S, Leach F. Gender violence in schools in the developing world. Gend Edu 2006;18:75–98. [Google Scholar]
- 27.Cluver L, Orkin M, Boyes ME et al. . Pathways from parental AIDS to child psychological, educational and sexual risk: developing an empirically-based interactive theoretical model. Soc Sci Med 2013;87:185–93. [DOI] [PubMed] [Google Scholar]
- 28.Cluver L, Orkin M, Boyes et al. . Transactional sex amongst AIDS-orphaned and AIDS-affected adolescents predicted by abuse and extreme poverty. J Acquir Immune Defic Syndr 2011;58:336–43. [DOI] [PubMed] [Google Scholar]
- 29.Operario D, Cluver L, Rees H et al. . Orphanhood and completion of compulsory school education among young people in South Africa: Findings from a national representative survey. J Res Adolesc 2008;18:173–86. [Google Scholar]
- 30.Tomlinson M, Solomon W, Singh Y et al. . The use of mobile phones as a data collection tool: A report from a household survey in South Africa. BMC Med Inform Decis Mak 2009;23:51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Nyangara F, O'Donnell K, Murphy R, Nyberg B. Child Status Index: A tool for assessing the well-being of orphans and vulnerable children. USAID 2009.
- 32.Varni JW, Seid M, Kurtin PS. PedsQL™ 4.0: Reliability and validity of the Pediatric Quality of Life Inventory™ Version 4.0 Generic Core Scales in healthy and patient populations. Medical Care 2001;39:800–12. [DOI] [PubMed] [Google Scholar]
- 33.Snider LM, Dawes A. Psychosocial vulnerability and resilience measures for national-level monitoring of orphans and other vulnerable children: recommendations for revision of the UNICEF psychological indicator. South Africa: UNCEF; 2006. [Google Scholar]
- 34.Straus M, Hamby S, Finkelhor D et al. . Identification of child maltreatment with the Parent-Child Conflict Tactics Scales: Development and psychometric data for a national sample of American parents. Child Abuse Negl 1998;22:249–70. [DOI] [PubMed] [Google Scholar]
- 35.Runyan DK, Dunne MP, Zolotor AJ et al. . The development and piloting of the ISPCAN Child Abuse Screening Tool-Parent version (ICAST-P). Child Abuse Negl 2009;33:826–32. [DOI] [PubMed] [Google Scholar]
- 36.The African Child Policy Forum. The African report on violence against children. Ethipia: The African Child Policy Forum; 2015. [Google Scholar]
- 37.UNICEF. Hidden in plain sight: A statistical analysis of violence against children. New York: UNICEF; 2015. [Google Scholar]
- 38.UNICEF. Child disciplinary practices at home: Evidence from a range of low- and middle-income countries. New York: UNICEF; 2010. [Google Scholar]
- 39.Abrahams N, Jewkes R, Laubscher R, Hoffman M. Intimate partner violence: prevalence and risk factors for men in Cape Town, South Africa. Violence Vict 2006;21:247–64. [DOI] [PubMed] [Google Scholar]
- 40.Rico E, Fenn B, Abramsky T, Watts C. Associations between maternal experiences of intimate partner violence and child nutrition and mortality: Findings from Demographic and Health Surveys in Egypt, Honduras, Kenya, Malawi and Rwanda. J Epidemiol Community Health 2011;65:360–7. [DOI] [PubMed] [Google Scholar]
- 41.Seedat M, van Niekerk A, Jewkes R et al. . Violence and injuries in South Africa: Prioritising an agenda for prevention. Lancet 2009;374:1011–22. [DOI] [PubMed] [Google Scholar]
- 42.United Nations. United Nations Sustainable Development Goals; Goal 4: Ensure inclusive and quality education for all and promote lifelong learning. http://www.un.org/sustainabledevelopment/education/ [accessed 16 November 2015].
- 43.Hall K, de Lannoy A. Children's Institute: Education – School attendance. http://www.childrencount.ci.org.za/indicator.php?id=6&indicator=15 [accessed 16 November 2015].
- 44.Bisika T, Ntata P, Konyani S. Gender-violence and education in Malawi: a study of violence against girls as an obstruction to universal primary school education. J Gen Stud 2009;18:287–94. [Google Scholar]
- 45.Skeen S, Macedo A, Tomlinson M et al. . Exposure to violence and psychological well-being in children affected by HIV/AIDS in South Africa and Malawi. In press. [DOI] [PMC free article] [PubMed]
- 46.Laughton B, Cornell M, Boivin M, van Rie A. Neurodevelopment in perinatally HIV-infected children: A concern for adolescence. J Int AIDS Soc 2013;16:18603. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Watkins JA, Sello OM, Cluver L et al. . ‘At school I got myself a certificate’: HIV/AIDS Orphanhood and secondary education: A qualitative study of risk and protective factors. Glob Soc Welf 2014;1:111–21. [Google Scholar]
- 48.Knerr W, Gardner F, Cluver L. Improving positive parenting skills and reducing harsh and abusive parenting in low- and middle-income countries: a systematic review. Prev Sci 2013;14:352–63. [DOI] [PubMed] [Google Scholar]
- 49.Mejia A, Calam R, Sanders MR. A review of parenting programs in developing countries: opportunities and challenges for preventing emotional and behavioral difficulties in children. Clin Child Fam Psychol Rev 2012;15:163–75. [DOI] [PubMed] [Google Scholar]
- 50.WHO. Parenting for Lifelong Health (PLH). Geneva: World Health Organization; http://www.who.int/violence_injury_prevention/violence/child/plh_aim/en/ [accessed 16 November 2015]. [Google Scholar]
- 51.Cooper PJ, Tomlinson M, Swartz L et al. . Improving quality of mother-infant relationship and infant attachment in socioeconomically deprived community in South Africa: Randomised controlled trial. BMJ 2009;338:b974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 52.Vally Z, Murray L, Tomlinson M, Cooper PJ. The impact of dialogic book-sharing training on infant language and attention: A randomized controlled trial in a deprived South African community. J Child Psychol Psychiatry 2015;56:865–73. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 53.Selke HM, Kimaiyo S, Sidle JE et al. . Task-shifting of antiretroviral delivery from health care workers to persons living with HIV/AIDS: clinical outcomes of a community-based program in Kenya. JAIDS 2010;55:483–90. [DOI] [PubMed] [Google Scholar]