

Abstract
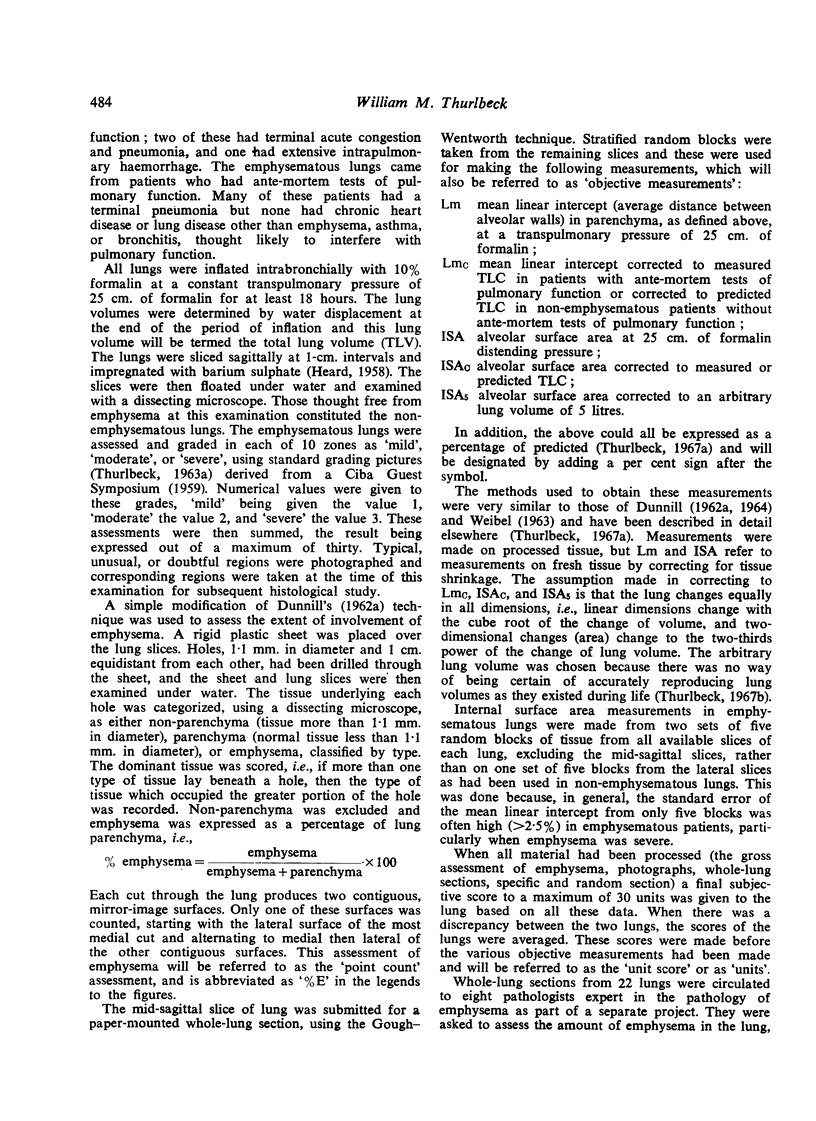
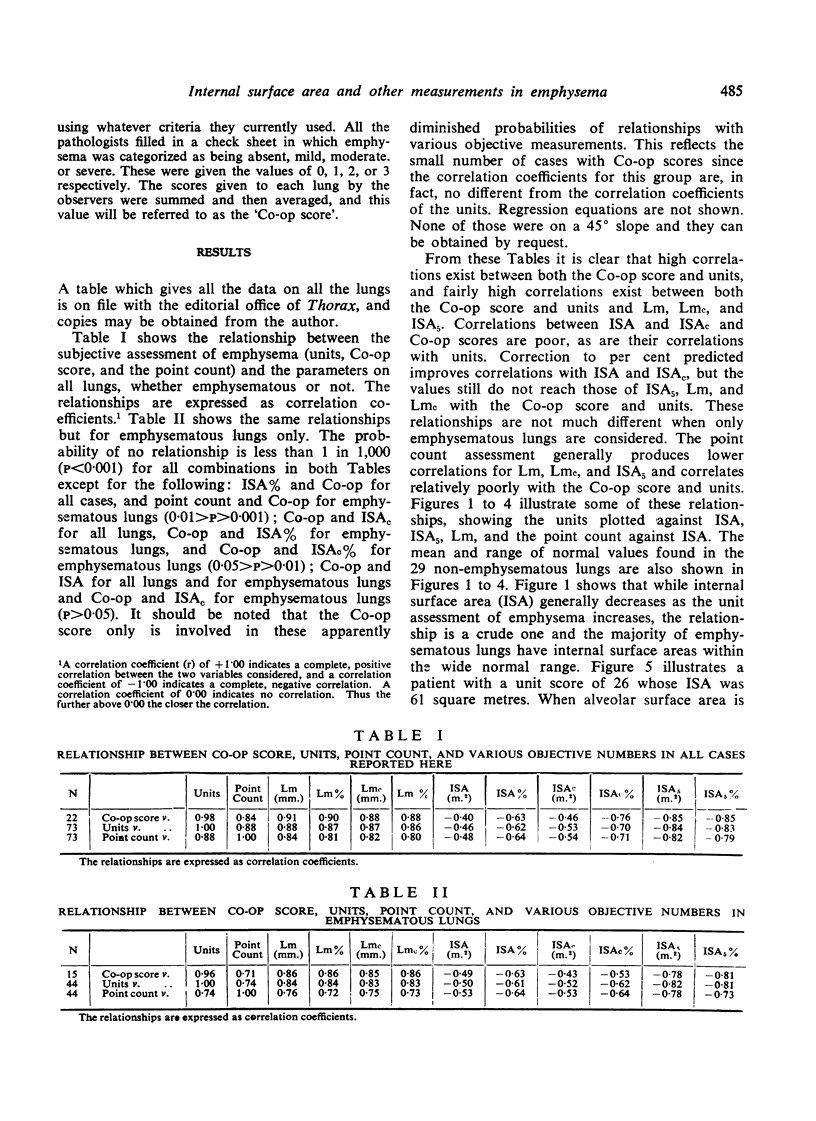
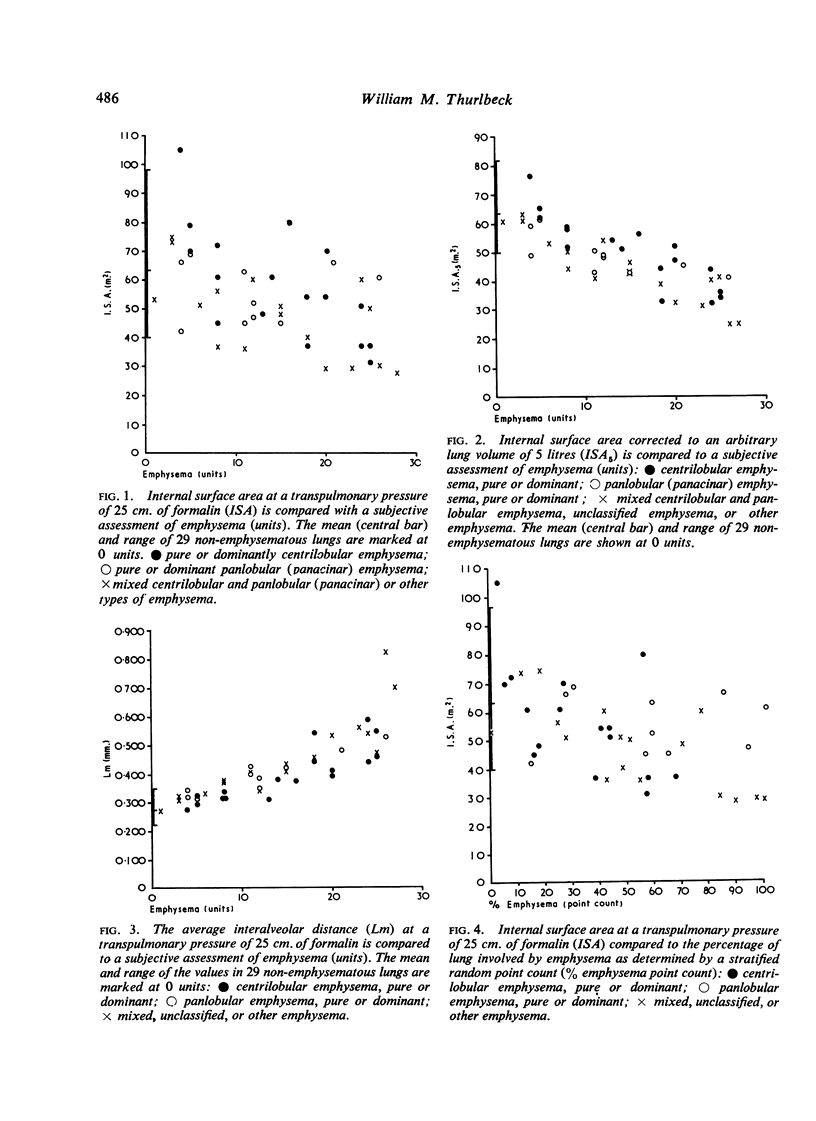
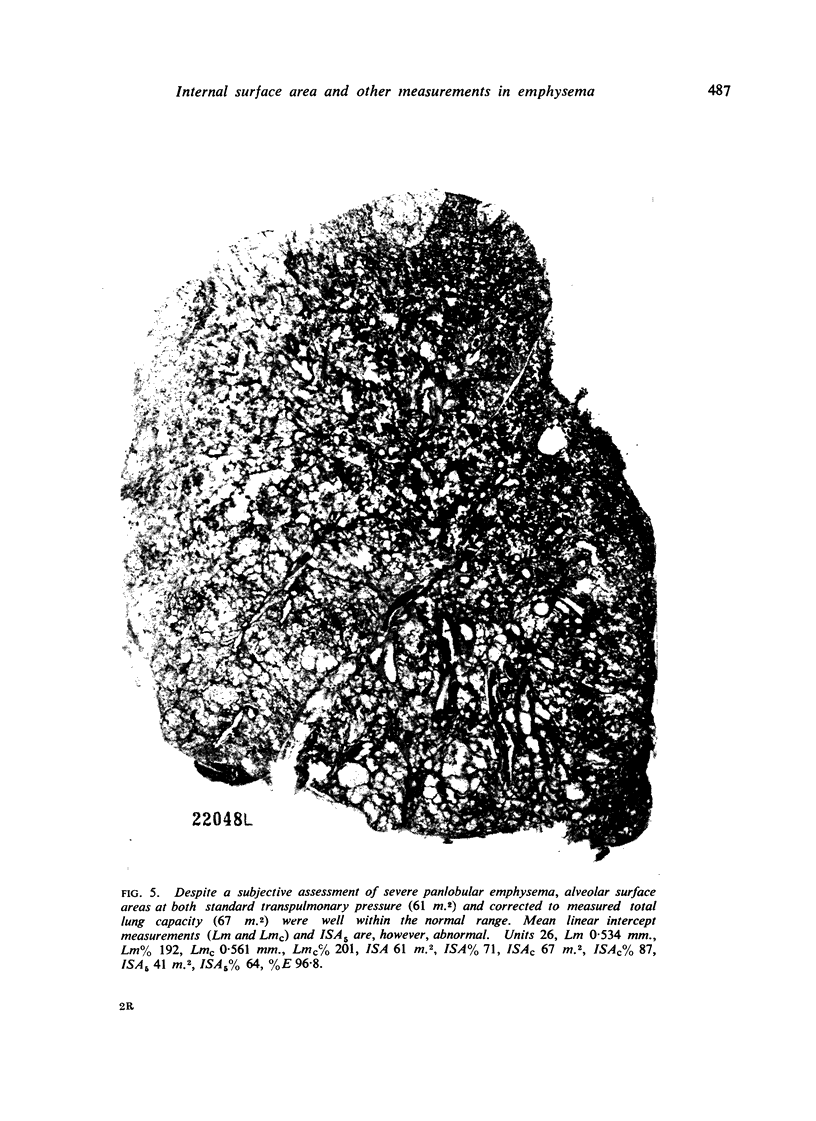
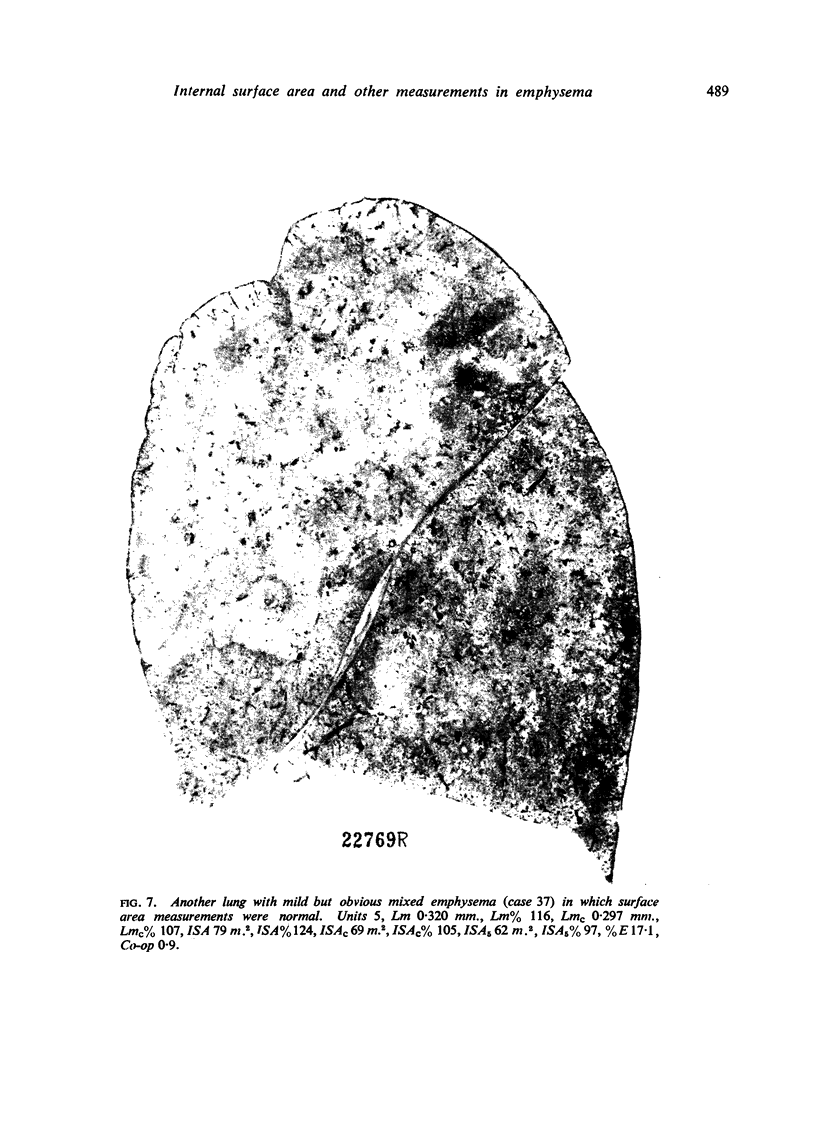
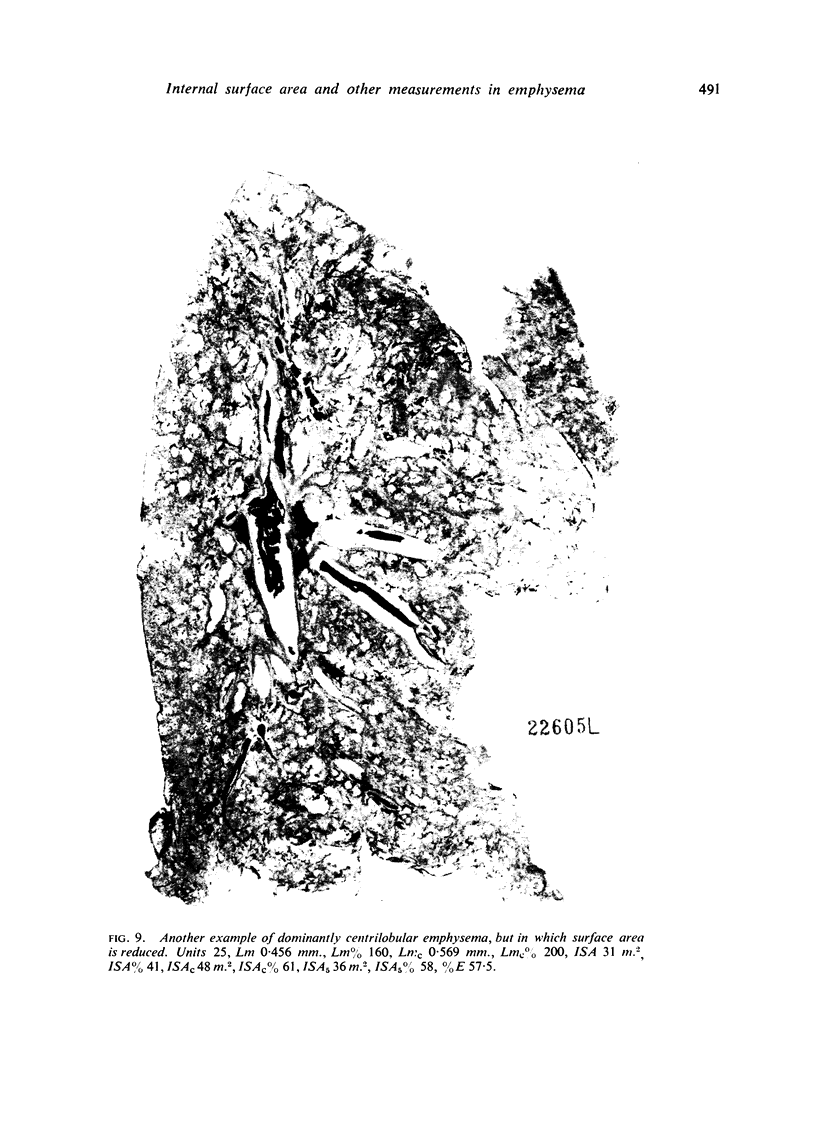
Some measurements of emphysema were made on 29 pairs of non-emphysematous lungs and 44 pairs of emphysematous lungs inflated at a standard transpulmonary pressure of 25 cm. of formalin. These were: a subjective visual assessment (units); an assessment of the volume of the lung parenchyma involved by emphysema (point count); an average subjective visual grading by eight pathologists (Co-op score); mean linear intercept or average distance between alveolar walls at a transpulmonary pressure of 25 cm. of formalin (Lm); mean linear intercept corrected to total lung capacity (LmC); internal (alveolar) surface area at 25 cm. transpulmonary pressure (ISA); internal surface area at total lung capacity (ISAC); internal surface area corrected to an arbitrary lung volume of 5 litres (ISA5). Internal surface area measurements were generally decreased in severe emphysema. Because of the wide range of ISA and ISAC in non-emphysematous lungs, most emphysematous lungs fell within the normal range. The range of ISA5 was smaller in non-emphysematous lungs and most emphysematous lungs fell outside this range. ISA5 in `mild' emphysema was not distinguishable from non-emphysematous lungs. Most emphysematous lungs in which the surface area was decreased less than expected from subjective assessment were examples of centrilobular emphysema. Lm and LmC were increased in emphysema. ISA5, Lm, and LmC paralleled the subjective assessments of emphysema rather better than ISA or ISAC, even when the latter were expressed as a percentage of predicted. Lm and LmC in lungs with mild emphysema fell within the ranges found in non-emphysematous lungs, but the mean value of Lm in lungs with `mild' emphysema was different from the mean Lm of non-emphysematous lungs, at conventional levels of significance. Since objective methods did not recognize adequately examples of `mild' emphysema, a subjective visual grading system (with its limitations) may have a definite place.
Full text
PDF






Images in this article

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- DUGUID J. B., HULSE E. V., RICHARDSON M. W., YOUNG A. E. A method calculating the respiratory surface area of the lung. J Physiol. 1953 Jul;121(1):8P–10P. [PubMed] [Google Scholar]
- DUGUID J. B., YOUNG A., CAUNA D., LAMBERT M. W. THE INTERNAL SURFACE AREA OF THE LUNG IN EMPHYSEMA. J Pathol Bacteriol. 1964 Oct;88:405–421. doi: 10.1002/path.1700880204. [DOI] [PubMed] [Google Scholar]
- HEARD B. E. A pathological study of emphysema of the lungs with chronic bronchitis. Thorax. 1958 Jun;13(2):136–149. doi: 10.1136/thx.13.2.136. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hicken P., Brewer D., Heath D. The relation between the weight of the right ventricle of the heart and the internal surface area and the number of alveoli in the human lung in emphysema. J Pathol Bacteriol. 1966 Oct;92(2):529–546. doi: 10.1002/path.1700920231. [DOI] [PubMed] [Google Scholar]
- Hicken P., Heath D., Brewer D. The relation between the weight of the right ventricle and the percentage of abnormal air space in the lung in emphysema. J Pathol Bacteriol. 1966 Oct;92(2):519–528. doi: 10.1002/path.1700920230. [DOI] [PubMed] [Google Scholar]
- STUART-HARRIS C. H. THE PATHOGENESIS OF CHRONIC BRONCHITIS AND EMPHYSEMA. Scott Med J. 1965 Mar;10:93–107. doi: 10.1177/003693306501000301. [DOI] [PubMed] [Google Scholar]
- THURLBECK W. M. A clinico-pathological study of emphysema in an American hospital. Thorax. 1963 Mar;18:59–67. doi: 10.1136/thx.18.1.59. [DOI] [PMC free article] [PubMed] [Google Scholar]