

Abstract
AIM: Population-based assessment of noncardiac chest pain (NCCP) is lacking. The aim of this study was to evaluate the prevalence, psychosocial factors and health seeking behaviour of NCCP in southern Chinese.
METHODS: A total of 2209 ethnic Hong Kong Chinese households were recruited to participate in a telephone survey to study the epidemiology of NCCP using the Rose angina questionnaire, a validated gastroesophageal reflux disease (GERD) questionnaire and the hospital anxiety-depression scale. NCCP was defined as non-exertional chest pain according to the Rose angina questionnaire and had not been diagnosed as ischaemic heart diseases by a physician.
RESULTS: Chest pain over the past year was present in 454 subjects (20.6%, 95%CI 19-22), while NCCP was present in 307 subjects (13.9%, 95%CI 13-15). GERD was present in 51% of subjects with NCCP and 34% had consulted a physician for chest pain. Subjects with NCCP had a significantly higher anxiety (P < 0.001) and depression score (P = 0.007), and required more days off (P = 0.021) than subjects with no chest pain. By multiple logistic regression analysis, female gender (OR 1.9, 95%CI 1.1-3.2), presence of GERD (OR 2.8, 95%CI 1.6-4.8), and social life being affected by NCCP (OR 6.9, 95%CI 3.3-15.9) were independent factors associated with health seeking behaviour in southern Chinese with NCCP.
CONCLUSION: NCCP is a common problem in southern Chinese and associated with anxiety and depression. Female gender, GERD and social life affected by chest pain were associated with health care utilization in subjects with NCCP.
INTRODUCTION
Noncardiac chest pain (NCCP) is a common problem and affects 23% of the U.S. population[1]. It is a benign condition with an estimated 10 year mortality of less than 1%[2]. However, the associated morbidity, as a result of inability to work and health care utilization, is enormous[3]. Population-based data of NCCP in Asia are lacking[4,5]. Furthermore, the effects of co-existing anxiety and depression on health care utilization in subjects with NCCP are unknown in Chinese. Various studies have shown an increased psychological morbidity in patients attending specialist clinics for functional gastrointestinal diseases[6-10]. This may be due to a causative effect of psychological factors on gastrointestinal symptoms, or the psychological morbidity may be a result of the functional gastrointestinal disease. Alternatively, psychological factors may influence health-seeking behaviour, and patients with co-morbid anxiety or depression may be more likely to seek medical consultation. Thus the aims of this study were to determine the population prevalence of NCCP, the effects of co-existing anxiety and depression and the health seeking behaviour of Chinese subjects with NCCP.
MATERIALS AND METHODS
Data collection
The telephone interview was conducted over a period of two weeks by a professional team of trained telephone interviewers from the Social Sciences Research Centre, the University of Hong Kong in November 2002. The interviewers went through intense training on the delivery of questionnaire to ensure uniformity and the questions to be understood. Random telephone numbers were generated by computer and dialed automatically. Only numbers corresponding to ethnic Chinese households were used in the study. Office numbers, facsimile machines, and non-Chinese households were excluded. Upon identification of target households, the interviewer asked to speak to the household member with the most recent birthday. This aimed to provide randomization among different members of the household. Baseline demographic data, education, occupation and income were assessed, followed by a translated version of the Rose Angina questionnaire[11], a validated GERD questionnaire[12], a validated translated version of the hospital anxiety depression scale[13-15] and assessment of medical care utilization and impact of the disease on social activity as described below. Overall, 3605 ethnic Chinese households were contacted by telephone. The interview was completed in 2209 subjects (response rate = 61.3%, mean age = 40.3 ± 14, 58% female). The demographic characteristics of the study subjects were comparable to the census data of Hong Kong in 2001[16]. This study was approved by the ethics committee of the University of Hong Kong.
Sample size
A previous study demonstrated that the prevalence of NCCP was approximately 23% in Minnesota, USA[1]. To provide a 95% confidence interval ± 2% and a meaningful comparison between health care seekers and non-health care seekers, we estimated a sample size of around 2000 of successful cases.
Questionnaire
The Rose angina questionnaire is a standardized method of measuring angina and myocardial infarction in population surveys and has been validated in different ethnic groups[17-26]. ‘Definite’ angina was defined as chest pain that limits exertion (walking uphill or hurry, or walking at an ordinary pace on the level), is situated over the sternum or in the left chest and left arm, and is relieved within 10 min by rest[11]. ‘Possible’ angina was defined as chest pain that limits exertion and other criteria for definite angina not fulfilled. NCCP was defined as non-exertional chest pain according to the Rose angina questionnaire and had not been diagnosed as ischaemic heart diseases by a physician[27]. Musculoskeletal-like chest pain was defined as chest pain that worsens on breathing, movement or the presence of chest wall tenderness. The duration and characteristics of the chest pain were recorded. In the development of the Chinese version of the questionnaire, the original instrument was translated, back translated and tested for reproducibility in a sample of thirty patients attending the gastrointestinal clinic. The intraclass correlation coefficient of the translated questionnaire was 0.91. Furthermore, we tested the Rose angina questionnaire in a pilot of 50 patients with known coronary heart diseases proven by coronary angiography and 100 healthy controls. The sensitivity and specificity determined by the pilot study was 68% and 95% for the diagnosis of ischemic heart disease respectively.
Gastrointestinal symptoms were assessed by a translated Chinese version of a validated GERD questionnaire[12]. The GERD questionnaire examined the symptoms of heartburn, acid regurgitation, dyspepsia, dysphagia, globus, odynophagia, hoarseness of voice, chronic cough, asthma and pneumonia in details. In addition, past medical history, medication use, past history of esophageal, gastric, cardiac or pulmonary disease; smoking, alcohol intake, and the intake of tea and coffee were assessed. Part of the results on GERD had been presented elsewhere[28]. The severity and frequency of chest pain and other gastrointestinal symptoms were graded on a five-point Likert scale as follows: 1 (none- no symptoms / none in the past year), 2 (mild- symptoms can be easily ignored / less than once per mo), 3 (moderate- awareness of symptoms but easily tolerated / ≥ once per month), 4 (severe- symptoms sufficient to cause an interference with normal activities / ≥ once weekly) and 5 (incapacitating- incapacitating symptoms with an inability to perform daily activities or require day-off / ≥ once daily)[29]. GERD was defined as heartburn and/or acid regurgitation over the past year, which has been shown to be specific for the diagnosis of GERD[30,31]. Patients who had used non-steroidal anti-inflammatory drugs (NSAIDs) / aspirin for at least 3 d at any dosage within 3 mo prior to the survey were considered to be NSAIDs / aspirin users[32]. Anxiety and depression were assessed by the hospital anxiety and depression scale[13]. The Chinese version of this questionnaire has previously been validated[14,15] which consists of 7 questions on anxiety and 7 questions on depression.
Medical care utilization
Medical care utilization of subjects with NCCP was classified into categories including the use of over-the-counter medication, community based medicine, accident and emergency department and admission to hospital. Impact of disease was measured by the proportion of subjects requiring days-off work due to gastrointestinal complaints, and whether subjects reported an adverse effect of the chest pain on their normal social life (social life being affected), i.e. symptoms sufficient to cause an interference with normal daily and social activity.
Statistical analysis
Univariate analysis was performed by Student’s t test for continuous variables and by chi-square test for categorical variables to assess the risk factors associated with NCCP. Multiple logistic regression analysis with sex and age adjustment was then performed to determine the risk factors associated with NCCP. Furthermore, a multiple logistic regression model was designed to determine the factors (severity and frequency of chest pain, presence of heartburn and/or acid regurgitation over the past year, gender, age, educational level (primary school or below, secondary or matriculation and tertiary), occupation (3 levels), anxiety and depression scores and social life being affected by chest pain) associated with health seeking behaviour in NCCP. To find the best model, a backward elimination stepwise procedure was carried out in a way that the factor would be eliminated from the analysis if the corresponding P value was greater than 0.2, in order not to miss out too much information in view of the small sample size. A P value of 0.05 or less was considered statistically significant and all reported P values were 2 sided.
RESULTS
Cardiac chest pain
Chest pain over the past year was present in 454 subjects (20.6%, 95%CI 19-22), of which 147 (6.7%) had ‘possible’ angina by the Rose angina questionnaire and/or ischaemic heart diseases diagnosed by a physician[11,27].
Noncardiac chest pain
NCCP over the past year was present in 307 subjects (13.9%, 95%CI 13-15). The demographic characteristics of subjects with NCCP, cardiac chest pain or no chest pain are given in Table 1. The prevalence of NCCP was higher in men than in women (16.6% vs 11.9%, P = 0.002). Subjects with NCCP were significantly younger than subjects with no chest pain. However, for subjects with cardiac chest pain, the prevalence was similar between men and women (7.5% vs 8%, P = 0.68) and the mean age was similar to subjects with no chest pain. Aspirin usage was significantly higher in subjects with cardiac chest pain than in subjects with no chest pain (20.6% vs 7.7%, P < 0.001). NSAIDs usage was significantly higher in subjects with either NCCP or cardiac chest pain than in subjects with no chest pain. Cigarette and coffee consumption were the highest in subjects with NCCP, while alcohol consumption was similar between subjects with NCCP and subjects with cardiac chest pain. The education level and socioeconomic status were similar in subjects with NCCP, cardiac chest pain or no chest pain (Table 1). The median duration of NCCP was 24 mo (range 0.1 to 360 mo). Most (96%) subjects with NCCP had mild to moderate chest pain over the central chest area (50%) (Table 2). The frequency of chest pain was less than once per mo in three quarters of the subjects. Of the 307 subjects with NCCP, 155 (50.5%) could be classified as having GERD, while 79 (25.7%) had musculoskeletal-like chest pain. But GERD and musculoskeletal-like chest pain were overlapped in 15.6% (48/307) of subjects. The gender difference in NCCP between men and women persisted after exclusion of subjects with musculoskeletal-like chest pain (13.1% vs 8.5%, P = 0.001). Figure 1 shows the age and sex- prevalence rates of NCCP and musculoskeletal-like chest pain over the past year. For men with NCCP over the past year, the prevalence was the highest in 18-24 age group, less common in 25-54 age group and increased again after the age of 55 (Figure 1). In contrast, the prevalence of NCCP in women was almost constant from age 18 to 44, and then dropped gradually with age. The overall prevalence of musculoskeletal-like chest pain was similar between men and women (4.2% vs 4.0%, P = NS), but men aged 18-24 had a higher prevalence when compared to women of similar age (7.9% vs 2.6%, P = 0.034).
Table 1.
Demographic data of study subjects (n = 2209)
| aCardiac | aNo | ||
| aNCCP | chest pain | chest pain | |
| (n = 307) | (n = 147) | (n = 1755) | |
| Mean age | 38 ± 14c | 42 ± 14 | 41 ± 14 |
| Gender (M/F) | 156/151c | 58/89 | 723/1032 |
| Smoking (%) | 20.6 | 16.7 | 16.0 |
| Alcohol (%) | 10.2d | 10.9 | 6.8 |
| Aspirin user (%) | 11.2 | 20.6b | 7.7 |
| NSAID user (%) | 11.6c | 13.9b | 6.0 |
| Coffee (%) | 22.7 | 14.0 | 18.7 |
| Education (%) | |||
| Primary or below | 37 (13) | 28 (21) | 290 (18) |
| Secondary or matriculation | 171 (61) | 88 (65) | 920 (57) |
| Tertiary | 72 (26) | 20 (15) | 392 (25) |
| Total | 280 (100) | 136 (100) | 1602 (100) |
| Monthly income in US$ (%) | |||
| None | 90 (33) | 60 (44) | 539 (35) |
| 1280 or below | 78 (29) | 34 (25) | 364 (24) |
| 1280 – 1920 | 39 (14) | 22 (16) | 254 (16) |
| 1920 – 3200 | 40 (15) | 10 (7) | 228 (15) |
| > 3200 | 25 (9) | 10 (7) | 160 (10) |
| Total | 272 (100) | 136 (100) | 1545 (100) |
| Occupation (%) | |||
| Professional and managerial | 45 (16) | 17 (13) | 262 (16) |
| Technical worker | 37 (13) | 14 (10) | 175 (11) |
| and craftsmen | |||
| Clerical work | 29 (10) | 16 (12) | 243 (15) |
| Service and sales | 32 (12) | 11 (8) | 157 (10) |
| Agriculture and others | 18 (7) | 8 (6) | 87 (6) |
| Non-technical worker | 8 (3) | 4 (3) | 33 (2) |
| Others (students, housewife, | 109 (39) | 66 (49) | 637 (40) |
| retired and unemployed) | |||
| Total | 278 (100) | 136 (100) | 1594 (100) |
aThe total in each individual cell may be smaller because of subject refusal,
P < 0.001 when compared to subjects with no chest pain,
P < 0.01 when compared to subjects with no chest pain,
P < 0.05 when compared to subjects with no chest pain.
Table 2.
Prevalence rates and characteristics of chest pain in studied population
| Male | Female | Total | |
| (n = 938) | (n = 1271) | (n = 2209) | |
| Chest pain over the past year (%) | 213 (22.7) | 241 (19.0) | 454 (20.6) |
| Possible angina by Rose angina | 57 (6.1) | 90 (7.1) | 147 (6.7) |
| Questionnaire or ischaemic heart | |||
| disease diagnosed by physicians(%) | |||
| Noncardiac chest pain-NCCP (%) | 156 (16.6) | 151 (11.9) | 307 (13.9) |
| NCCP severity (%) | |||
| Mild | 69 | 66 | 67 |
| Moderate | 27 | 32 | 29 |
| Severe or incapacitated | 4 | 3 | 4 |
| NCCP frequency (%) | |||
| < once / month | 75 | 76 | 76 |
| ≥ once / month | 22 | 19 | 21 |
| > once / weekly | 3 | 4 | 4 |
| NCCP location | |||
| Central | 46 | 55 | 50 |
| Left | 44 | 37 | 41 |
| Right | 10 | 8 | 9 |
Figure 1.
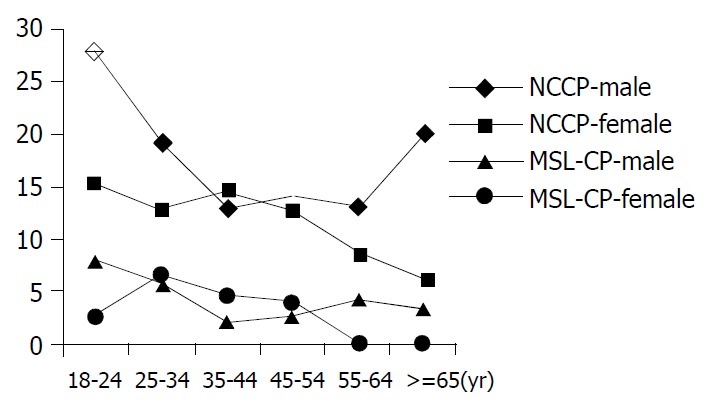
Age and sex-specific prevalence rates (per 100) of noncardiac chest pain (NCCP) and musculoskeletal-like chest pain (MSL-CP) over the past year.
Risk factors for NCCP
By univariate analysis, NCCP was associated with heartburn and/or acid regurgitation, globus, dyspepsia, feeling of acidity in stomach, alcohol and NSAID usage but not with dysphagia, odynophagia, chronic cough, hoarseness of voice, asthma, pneumonia, history of smoking, aspirin usage and coffee intake (Tables 1 and 3). By multiple logistic regression analysis, heartburn and/or acid regurgitation (OR 2.3, 95%CI 1.7-3.1), globus (OR 1.9, 95%CI 1.3-2.8), and NSAIDs use (OR 1.9, 95%CI 1.2-2.9) were independent risk factors associated with NCCP.
Table 3.
Association of non-cardiac chest pain with other GERD symptoms over the past year
| NCCP | No chest pain | OR | |
| (n = 307) | (n = 1755) | (95%CI) | |
| Heartburn and/or acid | 50.5a | 23.2 | 3.4 (2.6-4.3) |
| regurgitation (%) | |||
| Dysphagia (%) | 4.1 | 2.8 | 1.5 (0.8-2.8) |
| Odynophagia (%) | 7.1 | 5.8 | 1.2 (0.8-2.0) |
| Globus (%) | 15.9a | 5.3 | 3.4 (2.3-4.9) |
| Dyspepsia (%) | 21.8b | 14.0 | 1.7 (1.3-2.3) |
| Feeling of acidity | 31.3a | 16.5 | 2.3 (1.8-3.0) |
| in stomach (%) | |||
| Chronic cough (%) | 8.3 | 5.0 | 1.7 (1.1-2.7) |
| Hoarseness of voice (%) | 6.3 | 5.5 | 1.2 (0.7-1.9) |
| Asthma (%) | 4.2 | 2.5 | 1.7 (0.9-3.3) |
| Pneumonia (%) | 0.7 | 0.5 | 1.5 (0.3-6.9) |
P < 0.001 when compared to subjects with no chest pain,
P < 0.01 when compared to subjects with no chest pain.
Health care utilization, days off work and effects of NCCP on social life
Thirty-nine percent of subjects with NCCP over the past year used one or more forms of treatment for their problems. Among the 307 subjects with NCCP over the past year, 14 (5%) purchased over the counter medication, 85 (28%) visited an outpatient clinic; 10 (3%) visited the accident and emergency department, and 11 (4%) were admitted to regional hospitals for further management. NCCP over the past year was significantly correlated with increased health care utilization (P < 0.001, OR 3.2, 95%CI 2.4-4.3). A significantly higher proportion of health seekers with NCCP had moderate to severe chest pain when compared to non-health seekers (39% vs 27%, P = 0.025) (Table 4). However, the proportion of subjects with at least monthly chest pain (28% vs 22% P = 0.265) was similar between health seekers and non-health seekers. GERD (heartburn and/or acid regurgitation) over the past year was more prevalent in NCCP health seekers than in NCCP non-health seekers (67.5% vs 40.1%, P < 0.001). A significantly higher proportion of subjects with NCCP reported their social life was affected by the chest pain (17% vs 9%, P < 0.001, OR 1.9, 95%CI 1.4-2.5) and required days-off (17% vs 12%, P = 0.021, OR 1.4, 95%CI 1.1-1.9) when compared to subjects with no chest pain.
Table 4.
Comparison between subjects with noncardiac chest pain over the past year who did and did not seek health care
| NCCP health care | NCCP non-health | |
| seekers (n = 131) | care seekers (n = 176) | |
| Mean age ± SD | 39 ± 14 | 36 ± 14 |
| Female (%) | 57.5a | 42.8 |
| Chest pain severity | 39.2a | 26.5 |
| moderate or worse (%) | ||
| Chest pain once a | 27.5 | 21.7 |
| month or more (%) | ||
| Chest pain requiring days-off | 35.3b | 3.1 |
| Presence of GERD (heartburn | 67.5b | 40.1 |
| and/or acid regurgitation) (%) | ||
| Social life being affected | 31.4b | 6.2 |
| Mean anxiety score | 5.8 | 5.3 |
| Mean depression score | 4.7 | 4.2 |
P < 0.05 when compared to non-health seekers,
P < 0.001 when compared to non-health seekers.
Anxiety and depression score
Subjects with NCCP symptoms over the past year had higher average anxiety (5.5 vs 4.1, P < 0.001) and depression (4.4 vs 3.8, P = 0.007) scores when compared to subjects with no chest pain. However, for subjects with NCCP symptoms, the mean anxiety score and the mean depression score were similar between NCCP subjects who had sought any medical consultation and those who had not (Table 4).
Determinants of health care utilization in NCCP
By multiple logistic regression analysis, female gender (OR 1.9, 95%CI 1.1-3.2, P = 0.023), the presence of GERD (heartburn and/or acid regurgitation) symptoms over the past year (OR 2.8, 95%CI 1.6-4.8, P < 0.001) and social life being affected by chest pain (OR 6.9, 95%CI 3.3-15.9, P < 0.001) were independent factors associated with health seeking behaviour of subjects with NCCP.
DISCUSSION
The epidemiology of NCCP is scanty in the literature and most studies are not population-based. Locke et al[1] reported a prevalence of 23% in a semi-rural US population. However, chest pain (including both exertional and non-exertional chest pain) with no past history of heart disease was the criteria for the diagnosis of NCCP in the study. Using Rose angina criteria, a population-based study in Mexican American and non-Hispanic white found a prevalence of 30% for chest pain thought not angina[33]. A UK study reported a population prevalence of 24% (Rose angina questionnaire) in 7754 subjects from 24 towns of Britain for “other chest pain”[23]. Recently, a population survey performed in Australia, using a similar definition of NCCP, reported a prevalence of 33% in 672 residents of Penrith[34]. The only independent factor for NCCP was the frequency of heartburn. No particular factor for health seeking behaviour was identified. The criteria of NCCP in our study were similar to the Australian study, but we found a considerably lower prevalence of NCCP (14%) when compared to the Western population. The exact reason is unknown but may be related to the lower prevalence of GERD (both erosive esophagitis and non-erosive reflux disease) in the Chinese population[28,32], as GERD is the most common etiology of NCCP. The gender, age distribution and socio-economic status closely resembled those of the census data of Hong Kong in 2001, suggesting our data are highly representative[16]. Fifty-one percent of subjects with NCCP could be classified as having GERD in our study, suggesting an esophageal cause of the chest pain. Interestingly, both musculoskeletal-like chest pain and GERD were overlapped in 16% of subjects, indicating the difficulty in establishing the etiology of chest pain through a questionnaire. Furthermore, we were not able to exclude panic attacks without proper psychiatric assessment. Nevertheless, we could still obtain useful data about the impact of chest pain of presumably ‘noncardiac’ in origin in the Chinese community. The prevalence of NCCP was unexpectedly high in young men. It could be partially explained by the higher proportion of young men with musculoskeletal-like chest pain when compared to women of similar age. Further endoscopic and physiological studies are warranted to investigate the exact causes of chest pain in these subjects.
By multiple logistic regression analysis, the presence of heartburn and/or acid regurgitation, globus and NSAIDs intake were independent risk factors for NCCP. The symptoms of GERD and globus suggested an esophageal origin of the chest pain, but the positive association of NSAIDs intake with NCCP was interesting. It is unknown whether these subjects took NSAIDs for the symptomatic relief of chest pain or NSAID intake indirectly linked to esophageal chest pain as a result of erosive damage to the esophageal mucosa[35-38]. Furthermore, it has been shown that subjects receiving 1500 mg aspirin per day had higher gastric mechanosensory thresholds[39]. Those who failed to increase sensory thresholds were associated with dyspepsia. Similar mechanism may operate to account for the positive association between NSAIDs and NCCP as a result of abnormal visceral perception.
In the United States, it has been estimated that US$8 billion was spent annually for the initial care of patients who were suspected to have an acute coronary syndrome, but subsequently found not to have coronary artery disease[3]. The socio-economic effects were reflected by the higher proportion of NCCP subjects requiring days-off work and reporting an adverse effect of the illnesses on their social life when compared to subjects with no chest pain. It also concurred with our previous findings that quality of life assessment by SF-36 was significantly lower in patients with NCCP than in healthy controls[40].
Few studies have assessed the factors associated with health care utilization in NCCP. In the Australian study mentioned above, no particular factor was found to be associated with health seeking behaviour. We found that the presence of heartburn and/or acid regurgitation were important in motivating health seeking behaviour of subjects with NCCP. Furthermore, female gender was more commonly associated with health care utilization in subjects with NCCP. Despite the higher prevalence of NCCP in men in our study, women were more likely to seek medical attention and correlated with the findings of female predominance in previous non-population based studies[41,42]. We did not find any effect of anxiety and depression on health care utilization, but subjects feeling their social life affected by chest pain were more likely to seek help.
The major limitation of this study was the diagnosis of NCCP through a questionnaire. In clinical practice, diagnosis of NCCP requires full cardiology evaluation. However, criteria like Rome II are not available for noncardiac chest pain[43], but rather for a sub-group of patient population only (chest pain of presumed esophageal origin). It has been shown in prospective studies that ‘possible’ angina or exertional chest pain was equally reliable for the prediction of future ischemic events, in both men and women[23,26]. Furthermore, self-reported history of doctor-diagnosis of angina has been shown to be a valid measure of angina in population-based studies[27]. Although the sensitivity of Rose angina questionnaire is variable, it is highly specific for the diagnosis of angina[17-26]. In our pilot study, we found that the translated Chinese version of the Rose angina questionnaire had a sensitivity and specificity of 68% and 95%. We used the combination of ‘possible angina’ and history of ischemic heart disease diagnosed by a physician for the diagnosis of cardiac chest pain, hoping that it would reduce the number of unrecognized ischemic heart disease in this study. Furthermore, it is unpractical to perform exercise testing or coronary angiograms in all subjects with chest pain in the setting of a population-based study.
In conclusion, NCCP is a common problem in Chinese and associated with anxiety and depression. Female gender, the presence of GERD symptoms over the past year and social life affected by chest pain are independent factors associated with health care utilization in Chinese.
ACKNOWLEDGEMENTS
The authors would like to thank the Social Science Research Centre of the University of Hong Kong for coordinating and conducting the telephone interview.
Footnotes
Supported by the Competitive Earmarked Research Grant HKU 7487/03M of the Hong Kong Research Grant Council, the Simon K. Y. Lee Gastroenterology Fund of the University of Hong Kong and the Hong Kong Society of Gastroenterology
Edited by Wang XL Proofread by Zhu LH
References
- 1.Locke GR, Talley NJ, Fett SL, Zinsmeister AR, Melton LJ. Prevalence and clinical spectrum of gastroesophageal reflux: a population-based study in Olmsted County, Minnesota. Gastroenterology. 1997;112:1448–1456. doi: 10.1016/s0016-5085(97)70025-8. [DOI] [PubMed] [Google Scholar]
- 2.Chambers J, Bass C. Chest pain with normal coronary anatomy: a review of natural history and possible etiologic factors. Prog Cardiovasc Dis. 1990;33:161–184. doi: 10.1016/0033-0620(90)90007-o. [DOI] [PubMed] [Google Scholar]
- 3.Eslick GD, Coulshed DS, Talley NJ. Review article: the burden of illness of non-cardiac chest pain. Aliment Pharmacol Ther. 2002;16:1217–1223. doi: 10.1046/j.1365-2036.2002.01296.x. [DOI] [PubMed] [Google Scholar]
- 4.Goh KL, Chang CS, Fock KM, Ke M, Park HJ, Lam SK. Gastro-oesophageal reflux disease in Asia. J Gastroenterol Hepatol. 2000;15:230–238. doi: 10.1046/j.1440-1746.2000.02148.x. [DOI] [PubMed] [Google Scholar]
- 5.Wong WM, Cheng C, Hui WM, Lam SK. Noncardiac chest pain. Medical Progress. 2003;30:15–21. [Google Scholar]
- 6.Talley NJ, Fung LH, Gilligan IJ, McNeil D, Piper DW. Association of anxiety, neuroticism, and depression with dyspepsia of unknown cause. A case-control study. Gastroenterology. 1986;90:886–892. doi: 10.1016/0016-5085(86)90864-4. [DOI] [PubMed] [Google Scholar]
- 7.Talley NJ, Jones M, Piper DW. Psychosocial and childhood factors in essential dyspepsia. A case-control study. Scand J Gastroenterol. 1988;23:341–346. doi: 10.3109/00365528809093876. [DOI] [PubMed] [Google Scholar]
- 8.Langeluddecke P, Goulston K, Tennant C. Psychological factors in dyspepsia of unknown cause: a comparison with peptic ulcer disease. J Psychosom Res. 1990;34:215–222. doi: 10.1016/0022-3999(90)90055-9. [DOI] [PubMed] [Google Scholar]
- 9.Harris A, Martin BJ. Increased abdominal pain during final examinations. Dig Dis Sci. 1994;39:104–108. doi: 10.1007/BF02090068. [DOI] [PubMed] [Google Scholar]
- 10.Hui WM, Shiu LP, Lam SK. The perception of life events and daily stress in nonulcer dyspepsia. Am J Gastroenterol. 1991;86:292–296. [PubMed] [Google Scholar]
- 11.Rose GA. The diagnosis of ischaemic heart pain and intermittent claudication in field surveys. Bull World Health Organ. 1962;27:645–658. [PMC free article] [PubMed] [Google Scholar]
- 12.Locke GR, Talley NJ, Weaver AL, Zinsmeister AR. A new questionnaire for gastroesophageal reflux disease. Mayo Clin Proc. 1994;69:539–547. doi: 10.1016/s0025-6196(12)62245-9. [DOI] [PubMed] [Google Scholar]
- 13.Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. 1983;67:361–370. doi: 10.1111/j.1600-0447.1983.tb09716.x. [DOI] [PubMed] [Google Scholar]
- 14.Leung CM, Ho S, Kan CS, Hung CH, Chen CN. Evaluation of the Chinese version of the Hospital Anxiety and Depression Scale. A cross-cultural perspective. Int J Psychosom. 1993;40:29–34. [PubMed] [Google Scholar]
- 15.Lam CL, Pan PC, Chan AW, Chan SY, Munro C. Can the Hospital Anxiety and Depression (HAD) Scale be used on Chinese elderly in general practice. Fam Pract. 1995;12:149–154. doi: 10.1093/fampra/12.2.149. [DOI] [PubMed] [Google Scholar]
- 16.Hong Kong Census 2001. Census and Statistics Department, Hong Kong [Google Scholar]
- 17.Rose GA, Ahmeteli M, Checcacci L, Fidanza F, Glazunov I, De Haas J, Horstmann P, Kornitzer MD, Meloni C, Menotti A, et al. Ischaemic heart disease in middle-aged men. Prevalence comparisons in Europe. Bull World Health Organ. 1968;38:885–895. [PMC free article] [PubMed] [Google Scholar]
- 18.Marmot MG, Syme SL, Kagan A, Kato H, Cohen JB, Belsky J. Epidemiologic studies of coronary heart disease and stroke in Japanese men living in Japan, Hawaii and California: prevalence of coronary and hypertensive heart disease and associated risk factors. Am J Epidemiol. 1975;102:514–525. doi: 10.1093/oxfordjournals.aje.a112189. [DOI] [PubMed] [Google Scholar]
- 19.Erikssen J, Forfang K, Storstein O. Angina pectoris in presumably healthy middle-aged men. Validation of two questionnaire methods in making the diagnosis of angina pectoris. Eur J Cardiol. 1977;6:285–298. [PubMed] [Google Scholar]
- 20.Krogh V, Trevisan M, Panico S, Farinaro E, Mancini M, Menotti A, Ricci G. Prevalence and correlates of angina pectoris in the Italian nine communities study. Research Group ATS-RF2 of the Italian National Research Council. Epidemiology. 1991;2:26–32. doi: 10.1097/00001648-199101000-00005. [DOI] [PubMed] [Google Scholar]
- 21.Kutty VR, Balakrishnan KG, Jayasree AK, Thomas J. Prevalence of coronary heart disease in the rural population of Thiruvananthapuram district, Kerala, India. Int J Cardiol. 1993;39:59–70. doi: 10.1016/0167-5273(93)90297-t. [DOI] [PubMed] [Google Scholar]
- 22.Singh RB, Sharma JP, Rastogi V, Raghuvanshi RS, Moshiri M, Verma SP, Janus ED. Prevalence of coronary artery disease and coronary risk factors in rural and urban populations of north India. Eur Heart J. 1997;18:1728–1735. doi: 10.1093/oxfordjournals.eurheartj.a015167. [DOI] [PubMed] [Google Scholar]
- 23.Lampe FC, Whincup PH, Wannamethee SG, Ebrahim S, Walker M, Shaper AG. Chest pain on questionnaire and prediction of major ischaemic heart disease events in men. Eur Heart J. 1998;19:63–73. doi: 10.1053/euhj.1997.0729. [DOI] [PubMed] [Google Scholar]
- 24.Udol K, Mahanonda N. Comparison of the Thai version of the Rose questionnaire for angina pectoris with the exercise treadmill test. J Med Assoc Thai. 2000;83:514–522. [PubMed] [Google Scholar]
- 25.Fischbacher CM, Bhopal R, Unwin N, White M, Alberti KG. The performance of the Rose angina questionnaire in South Asian and European origin populations: a comparative study in Newcastle, UK. Int J Epidemiol. 2001;30:1009–1016. doi: 10.1093/ije/30.5.1009. [DOI] [PubMed] [Google Scholar]
- 26.Hart CL, Watt GC, Davey Smith G, Gillis CR, Hawthorne VM. Pre-existing ischaemic heart disease and ischaemic heart disease mortality in women compared with men. Int J Epidemiol. 1997;26:508–515. doi: 10.1093/ije/26.3.508. [DOI] [PubMed] [Google Scholar]
- 27.Lampe FC, Walker M, Lennon LT, Whincup PH, Ebrahim S. Validity of a self-reported history of doctor-diagnosed angina. J Clin Epidemiol. 1999;52:73–81. doi: 10.1016/s0895-4356(98)00146-2. [DOI] [PubMed] [Google Scholar]
- 28.Wong WM, Lai KC, Lam KF, Hui WM, Hu WHC, Lam CLK, Xia HHX, Huang JQ, Chan CK, Lam SK, et al. Prevalence, clini-cal spectrum and health care utilisation of gastroesophageal re-flux disease in Chinese population: a population-based study. Gastroenterology. 2003;124(Supp 1):A167. [Google Scholar]
- 29.Wong WM, Lam KF, Lai KC, Hui WM, Hu WH, Lam CL, Wong NY, Xia HH, Huang JQ, Chan AO, et al. A validated symptoms questionnaire (Chinese GERDQ) for the diagnosis of gastro-oesophageal reflux disease in the Chinese population. Aliment Pharmacol Ther. 2003;17:1407–1413. doi: 10.1046/j.1365-2036.2003.01576.x. [DOI] [PubMed] [Google Scholar]
- 30.Klauser AG, Schindlbeck NE, Müller-Lissner SA. Symptoms in gastro-oesophageal reflux disease. Lancet. 1990;335:205–208. doi: 10.1016/0140-6736(90)90287-f. [DOI] [PubMed] [Google Scholar]
- 31.Dent J, Brun J, Fendrick AM, Fennerty MB, Janssens J, Kahrilas PJ, Lauritsen K, Reynolds JC, Shaw M, Talley NJ. An evidence-based appraisal of reflux disease management-the Genval Work-shop Report. Gut. 1999;44(Suppl 2):S1–S16. doi: 10.1136/gut.44.2008.s1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Wong WM, Lam SK, Hui WM, Lai KC, Chan CK, Hu WH, Xia HH, Hui CK, Yuen MF, Chan AO, et al. Long-term prospective follow-up of endoscopic oesophagitis in southern Chinese--prevalence and spectrum of the disease. Aliment Pharmacol Ther. 2002;16:2037–2042. doi: 10.1046/j.1365-2036.2002.01373.x. [DOI] [PubMed] [Google Scholar]
- 33.Mitchell BD, Hazuda HP, Haffner SM, Patterson JK, Stern MP. High prevalence of angina pectoris in Mexican-American men. A population with reduced risk of myocardial infarction. Ann Epidemiol. 1991;1:415–426. doi: 10.1016/1047-2797(91)90011-z. [DOI] [PubMed] [Google Scholar]
- 34.Eslick GD, Jones MP, Talley NJ. Non-cardiac chest pain: prevalence, risk factors, impact and consulting--a population-based study. Aliment Pharmacol Ther. 2003;17:1115–1124. doi: 10.1046/j.1365-2036.2003.01557.x. [DOI] [PubMed] [Google Scholar]
- 35.Wilkins WE, Ridley MG, Pozniak AL. Benign stricture of the oesophagus: role of non-steroidal anti-inflammatory drugs. Gut. 1984;25:478–480. doi: 10.1136/gut.25.5.478. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Semble EL, Wu WC, Castell DO. Nonsteroidal antiinflammatory drugs and esophageal injury. Semin Arthritis Rheum. 1989;19:99–109. doi: 10.1016/0049-0172(89)90054-1. [DOI] [PubMed] [Google Scholar]
- 37.El-Serag HB, Sonnenberg A. Association of esophagitis and esophageal strictures with diseases treated with nonsteroidal anti-inflammatory drugs. Am J Gastroenterol. 1997;92:52–56. [PubMed] [Google Scholar]
- 38.Avidan B, Sonnenberg A, Schnell TG, Sontag SJ. Risk factors for erosive reflux esophagitis: a case-control study. Am J Gastroenterol. 2001;96:41–46. doi: 10.1111/j.1572-0241.2001.03449.x. [DOI] [PubMed] [Google Scholar]
- 39.Holtmann G, Gschossmann J, Buenger L, Gerken G, Talley NJ. Do changes in visceral sensory function determine the development of dyspepsia during treatment with aspirin. Gastroenterology. 2002;123:1451–1458. doi: 10.1053/gast.2002.36556. [DOI] [PubMed] [Google Scholar]
- 40.Wong WM, Lai KC, Lau CP, Hu WH, Chen WH, Wong BC, Hui WM, Wong YH, Xia HH, Lam SK. Upper gastrointestinal evaluation of Chinese patients with non-cardiac chest pain. Aliment Pharmacol Ther. 2002;16:465–471. doi: 10.1046/j.1365-2036.2002.01217.x. [DOI] [PubMed] [Google Scholar]
- 41.Billing E, Hjemdahl P, Rehnqvist N. Psychosocial variables in female vs male patients with stable angina pectoris and matched healthy controls. Eur Heart J. 1997;18:911–918. doi: 10.1093/oxfordjournals.eurheartj.a015378. [DOI] [PubMed] [Google Scholar]
- 42.Kirchgatterer A, Weber T, Auer J, Wimmer L, Mayr H, Maurer E, Eber B. [Analysis of referral diagnoses of patients with normal coronary angiogram] Wien Klin Wochenschr. 1999;111:434–438. [PubMed] [Google Scholar]
- 43.Clouse RE, Richter JE, Heading RC, Janssens J, Wilson JA. Functional esophageal disorders. Gut. 1999;45 Suppl 2:II31–II36. doi: 10.1136/gut.45.2008.ii31. [DOI] [PMC free article] [PubMed] [Google Scholar]