

Abstract
Background
Platelet transfusions are used in modern clinical practice to prevent and treat bleeding in people who are thrombocytopenic due to bone marrow failure. Although considerable advances have been made in platelet transfusion therapy in the last 40 years, some areas continue to provoke debate, especially concerning the use of prophylactic platelet transfusions for the prevention of thrombocytopenic bleeding.
This is an update of a Cochrane review first published in 2004, and previously updated in 2012 that addressed four separate questions: prophylactic versus therapeutic‐only platelet transfusion policy; prophylactic platelet transfusion threshold; prophylactic platelet transfusion dose; and platelet transfusions compared to alternative treatments. This review has now been split into four smaller reviews looking at these questions individually; this review compares prophylactic platelet transfusion thresholds.
Objectives
To determine whether different platelet transfusion thresholds for administration of prophylactic platelet transfusions (platelet transfusions given to prevent bleeding) affect the efficacy and safety of prophylactic platelet transfusions in preventing bleeding in people with haematological disorders undergoing myelosuppressive chemotherapy or haematopoietic stem cell transplantation (HSCT).
Search methods
We searched for randomised controlled trials (RCTs) in the Cochrane Central Register of Controlled Trials (CENTRAL) (Cochrane Library 2015, Issue 6, 23 July 2015), MEDLINE (from 1946), Embase (from 1974), CINAHL (from 1937), the Transfusion Evidence Library (from 1950), and ongoing trial databases to 23 July 2015.
Selection criteria
We included RCTs involving transfusions of platelet concentrates, prepared either from individual units of whole blood or by apheresis, and given to prevent bleeding in people with haematological disorders (receiving myelosuppressive chemotherapy or undergoing HSCT) that compared different thresholds for administration of prophylactic platelet transfusions (low trigger (5 x 109/L); standard trigger (10 x 109/L); higher trigger (20 x 109/L, 30 x 109/L, 50 x 109/L); or alternative platelet trigger (for example platelet mass)).
Data collection and analysis
We used the standard methodological procedures expected by Cochrane.
Main results
Three trials met our predefined inclusion criteria and were included for analysis in the review (499 participants). All three trials compared a standard trigger (10 x 109/L) versus a higher trigger (20 x 109/L or 30 x 109/L). None of the trials compared a low trigger versus a standard trigger or an alternative platelet trigger. The trials were conducted between 1991 and 2001 and enrolled participants from fairly comparable patient populations.
The original review contained four trials (658 participants); in the previous update of this review we excluded one trial (159 participants) because fewer than 80% of participants had a haematological disorder. We identified no new trials in this update of the review.
Overall, the methodological quality of the studies was low across different outcomes according to GRADE methodology. None of the included studies were at low risk of bias in every domain, and all the included studies had some threats to validity.
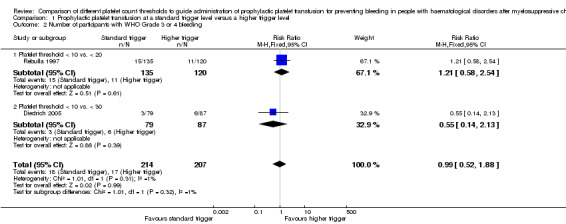
Three studies reported the number of participants with at least one clinically significant bleeding episode within 30 days from the start of the study. There was no evidence of a difference in the number of participants with a clinically significant bleeding episode between the standard and higher trigger groups (three studies; 499 participants; risk ratio (RR) 1.35, 95% confidence interval (CI) 0.95 to 1.90; low‐quality evidence).
One study reported the number of days with a clinically significant bleeding event (adjusted for repeated measures). There was no evidence of a difference in the number of days of bleeding per participant between the standard and higher trigger groups (one study; 255 participants; relative proportion of days with World Health Organization Grade 2 or worse bleeding (RR 1.71, 95% CI 0.84 to 3.48, P = 0.162; authors' own results; low‐quality evidence).
Two studies reported the number of participants with severe or life‐threatening bleeding. There was no evidence of any difference in the number of participants with severe or life‐threatening bleeding between a standard trigger level and a higher trigger level (two studies; 421 participants; RR 0.99, 95% CI 0.52 to 1.88; low‐quality evidence).
Only one study reported the time to first bleeding episode. There was no evidence of any difference in the time to the first bleeding episode between a standard trigger level and a higher trigger level (one study; 255 participants; hazard ratio 1.11, 95% CI 0.64 to 1.91; low‐quality evidence).
Only one study reported on all‐cause mortality within 30 days from the start of the study. There was no evidence of any difference in all‐cause mortality between standard and higher trigger groups (one study; 255 participants; RR 1.78, 95% CI 0.83 to 3.81; low‐quality evidence).
Three studies reported on the number of platelet transfusions per participant. Two studies reported on the mean number of platelet transfusions per participant. There was a significant reduction in the number of platelet transfusions per participant in the standard trigger group (two studies, mean difference ‐2.09, 95% CI ‐3.20 to ‐0.99; low‐quality evidence).
One study reported on the number of transfusion reactions. There was no evidence to demonstrate any difference in transfusion reactions between the standard and higher trigger groups (one study; 79 participants; RR 0.07, 95% CI 0.00 to 1.09).
None of the studies reported on quality of life.
Authors' conclusions
In people with haematological disorders who are thrombocytopenic due to myelosuppressive chemotherapy or HSCT, we found low‐quality evidence that a standard trigger level (10 x 109/L) is associated with no increase in the risk of bleeding when compared to a higher trigger level (20 x 109/L or 30 x 109/L). There was low‐quality evidence that a standard trigger level is associated with a decreased number of transfusion episodes when compared to a higher trigger level (20 x 109/L or 30 x 109/L).
Findings from this review were based on three studies and 499 participants. Without further evidence, it is reasonable to continue with the current practice of administering prophylactic platelet transfusions using the standard trigger level (10 x 109/L) in the absence of other risk factors for bleeding.
Plain language summary
Platelet transfusions are used to prevent bleeding in people with low platelet counts due to treatment‐induced bone marrow failure
Review question
We evaluated the evidence about whether platelet transfusions given to prevent bleeding in people with lower platelet counts (for example 5 x 109/L or below) were as effective and safe as the current standard (10 x 109/L or below), or whether higher platelet count levels (20 x 109/L or below, 30 x 109/L or below, or 50 x 109/L or below) were safer than the current standard (10 x 109/L or below). Our target population was people with blood cancers (for example leukaemia, lymphoma, myeloma) who were receiving intensive (myelosuppressive) chemotherapy treatments or stem cell transplantation.
Background
People with blood cancers may have low platelet counts due to their underlying cancer. Blood cancers may be treated with chemotherapy and stem cell transplantation, and these treatments can cause low platelet counts. Platelet transfusions may be given to prevent bleeding when the platelet count falls below a prespecified threshold platelet count (for example 10 x 109/L), or may be given to treat bleeding (such as a prolonged nosebleed or multiple bruises). Giving platelet transfusions at a lower prespecified threshold platelet count may increase the chance that bleeding will occur, which may be harmful, whereas giving platelet transfusions at a higher prespecified threshold platelet count may mean that people receive unnecessary platelet transfusions. Platelet transfusions can have adverse effects and have cost and resource implications for health services, so unnecessary transfusions should be avoided.
Study characteristics
The evidence is current to July 2015. We found no new studies in this update of the review. This review identified three randomised controlled trials that compared giving platelet transfusions to prevent bleeding when the platelet count is 10 x 109/L (the current standard) or below versus giving platelet transfusions to prevent bleeding at higher platelet count levels (20 x 109/L or below or 30 x 109/L or below). None of the studies compared a lower trigger or alternative trigger to the current standard. These trials were conducted between 1991 and 2001 and included 499 participants. Two trials included adults with leukaemia who were receiving chemotherapy. One trial included children and adults receiving a stem cell transplant.
Two of the three studies reported sources of funding. Neither of the studies that reported funding sources were industry sponsored.
Key results
Giving platelet transfusions to people with low platelet counts due to blood cancers or their treatment to prevent bleeding when the platelet count was 10 x 109/L or below did not increase the risk of bleeding compared to giving a platelet transfusion at higher platelet counts (20 x 109/L or below or 30 x 109/L or below).
Giving platelet transfusions to prevent bleeding only when the platelet count was 10 x 109/L or below resulted in a reduction in the number of platelets given. We found no evidence to demonstrate that giving a platelet transfusion when the platelet count was 10 x 109/L or below decreased the number of transfusion reactions compared to giving platelet transfusions at higher platelet counts (20 x 109/L or below or 30 x 109/L or below).
None of the three studies reported any quality of life outcomes.
Findings from this review were based on three studies and 499 participants. Without further evidence, it is reasonable to continue using platelet transfusions to prevent bleeding based on the current standard transfusion threshold (10 x 109/L).
Quality of the evidence
The evidence for most of the findings was of low quality. This was because participants and their doctors knew which study arm the participant had been allocated to, and also the estimate of the treatment effect was imprecise.
Summary of findings
Summary of findings for the main comparison. Prophylactic platelet transfusion at threshold of 10,000 compared to higher transfusion threshold (20,000 or 30,000) for people with a haematological disorder.
| Prophylactic platelet transfusion at threshold of 10,000 compared to higher transfusion threshold (20,000 or 30,000) for prevention of haemorrhage after chemotherapy and stem cell transplantation | ||||||
| Patient or population: People with a haematological disorder Settings: Receiving intensive chemotherapy or a stem cell transplant Intervention: Prophylactic platelet transfusion at threshold of 10 x 109/L Comparison: Higher transfusion threshold (20 x 109/L or 30 x 109/L) | ||||||
| Outcomes | Illustrative comparative risks* (95% CI) | Relative effect (95% CI) | No of Participants (studies) | Quality of the evidence (GRADE) | Comments | |
| Assumed risk | Corresponding risk | |||||
|
Higher transfusion threshold (20 x 109/L or 30 x 109/L) |
Prophylactic platelet transfusion at threshold of 10 x 109/L | |||||
| Numbers of participants with at least 1 clinically significant bleeding event up to 30 days from study entry | 177 per 1000 | 239 per 1000 (168 to 336) | RR 1.35 (0.95 to 1.9) | 499 (3 studies) | ⊕⊕⊝⊝ low1,2 | The definition of clinically significant bleeding varied between studies, because there were differences in the way bleeding was graded |
| Number of days on which clinically significant bleeding occurred per participant up to 30 days from study entry | Not estimable3 | Not estimable3 | Not estimable3 | 255 (1 study) |
⊕⊕⊝⊝ low1,2 | ‐ |
| Number of participants with WHO Grade 3 or 4 bleeding up to 30 days from study entry | 82 per 1000 |
81 per 1000 (43 to 154) |
RR 0.99 (0.52 to 1.88) |
421 (2 studies) |
⊕⊕⊝⊝ low1,2 | ‐ |
| Time to first bleeding episode (days) | ‐ | ‐ |
HR 1.11 (0.64 to 1.91) |
255 (1 study) |
⊕⊕⊝⊝ low1,2 | ‐ |
| Number of platelet transfusions per participant up to 30 days from study entry | The mean number of platelet transfusions per participant in the 10 x 109/L group was 2.09 lower (3.2 to 0.99 lower) | ‐ | 333 (2 studies) | ⊕⊕⊝⊝ low1,2 | ‐ | |
| Mortality from all causes up to 30 days from study entry | 75 per 1000 |
134 per 1000 (62 to 286) |
RR 1.78 (0.83 to 3.81) |
255 (1 study) |
⊕⊕⊝⊝ low1,2 | ‐ |
| Quality of life ‐ not reported | Not estimable | Not estimable | Not estimable | ‐ | See comment | None of the studies reported quality of life |
| *The basis for the assumed risk (e.g. the median control group risk across studies) is provided in footnotes. The corresponding risk (and its 95% confidence interval) is based on the assumed risk in the comparison group and the relative effect of the intervention (and its 95% CI). CI: Confidence interval; HR: Hazard ratio; RR: Risk ratio | ||||||
| GRADE Working Group grades of evidence High quality: Further research is very unlikely to change our confidence in the estimate of effect. Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate. Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate. Very low quality: We are very uncertain about the estimate. | ||||||
1The number of participants from all three studies may not be large enough to detect a clinically significant difference. The confidence intervals are wide, and therefore there is uncertainty about the result. The level of evidence was downgraded by 1 due to imprecision.
2All of the studies were at high risk of bias due to lack of blinding and more protocol deviations in the standard‐trigger arm (10 x 109/L). The Rebulla study did not perform an intention‐to‐treat analysis and excluded 2 participants who died within 24 hours of entering the study. The level of evidence was downgraded by 1 due to risk of bias.
3The authors of Rebulla 1997 reported a relative proportion of days with WHO Grade 2 or worse bleeding of 1.71 (95% CI 0.84 to 3.48) for the standard versus higher transfusion trigger arms. A permutation test for the comparison of these proportions gives a P value of 0.162, and therefore no significant difference between study arms was found. These results are the authors' own results.
Background
Description of the condition
Haematological malignancies account for between 8% and 9% of all new cancers reported in the United Kingdom and United States (CDC 2012; ONS 2012), and their incidence is increasing (11% to 14% increase in new cases of lymphoma and myeloma between 1991 to 2001 and 2008 to 2010, respectively) (Cancer Research UK 2013). The prevalence of these disorders is also increasing due to increased survival rates (Coleman 2004; Rachet 2009), which are the result of the introduction of intensive chemotherapy treatments and use of stem cell transplantation (Burnett 2011; Fielding 2007; Patel 2009). Over 50,000 haematopoietic stem cell transplants (HSCT) are carried out annually worldwide and are used to treat both malignant and non‐malignant haematological disorders (Gratwohl 2010). Autologous HSCT is the most common type of HSCT (57% to 59%) (Gratwohl 2010; Passweg 2012). However, chemotherapy or stem cell transplantation can lead to prolonged periods of severe thrombocytopenia (De la Serna 2008; Heddle 2009a; Rysler 2010; Stanworth 2013; Wandt 2012).
Platelet transfusions are used in modern clinical practice to prevent and treat bleeding in thrombocytopenic patients with bone marrow failure secondary to chemotherapy or stem cell transplantation. The ready availability of platelet concentrates has undoubtedly made a major contribution in allowing the development of intensive treatment regimens for haematological disorders (malignant and non‐malignant) and other malignancies. The first demonstration of the effectiveness of platelet transfusions was performed in 1910 (Duke 1910). However, it was not until the 1970s and 1980s that the use of platelet transfusions became standard treatment for thrombocytopenic patients with bone marrow failure (Blajchman 2008). Alongside changes in supportive care, the routine use of platelet transfusions in people with haematological disorders since that time has led to a marked decrease in the number of haemorrhagic deaths associated with thrombocytopenia (Slichter 1980). This has resulted in a considerable increase in the demand for platelet concentrates. Currently, platelet concentrates are the second most frequently used blood component. Administration of platelet transfusions to people with haematological disorders now constitutes a significant proportion (up to 67%) of all platelets issued (Cameron 2007; Greeno 2007; Pendry 2011), and the majority of these (69%) are given to prevent bleeding (Estcourt 2012b).
People can become refractory to platelet transfusions. In an analysis of the TRAP 1997 study data, there was a progressive decrease in the post‐transfusion platelet count increments and time interval between transfusions as the number of preceding transfusions increased (Slichter 2005). This effect was seen irrespective of whether or not participants had developed detectable human leukocyte antigen (HLA) antibodies (Slichter 2005).
Platelet transfusions are also associated with adverse events. Mild to moderate reactions to platelet transfusions include rigors, fever, and urticaria (Heddle 2009b). Although these reactions are not life‐threatening, they can be extremely distressing for the patient. Rarer but more serious sequelae include anaphylaxis, transfusion‐transmitted infections, transfusion‐related acute lung injury, and immunomodulatory effects (Benson 2009; Blumberg 2009; Bolton‐Maggs 2012; Heddle 2009b; Knowles 2011; Pearce 2011; Popovsky 1985; Silliman 2003; Taylor 2010).
Any strategy that can safely decrease the need for prophylactic platelet transfusions in people with haematological malignancies will have significant logistical and financial implications as well as decreasing patients’ exposure to the risks of transfusion.
Description of the intervention
Platelet transfusions have an obvious beneficial effect in the management of active bleeding in people with haematological malignancy and severe thrombocytopenia. However, questions still remain about how this limited resource should be used to prevent severe and life‐threatening bleeding (Estcourt 2011). Prophylactic platelet transfusions for people with chemotherapy‐induced thrombocytopenia became standard practice following the publication of several small randomised controlled trials (RCTs) in the late 1970s and early 1980s (Higby 1974; Murphy 1982; Solomon 1978).
Prophylactic platelet transfusion threshold
Prophylactic platelet transfusions are typically given when blood platelet counts fall below a given trigger level. Studies have compared different platelet count thresholds to trigger the administration of prophylactic platelet transfusions. The current consensus is that people should receive a platelet transfusion when the platelet count is less than 10 x 109/L, unless there are other risk factors for bleeding such as sepsis, concurrent use of antibiotics, or other abnormalities of haemostasis (BCSH 2003; BCSH 2004; Board 2009; NBA 2012; Schiffer 2001; Slichter 2007; Tinmouth 2007). The experimental interventions were higher or lower platelet transfusion thresholds.
The previous review raised the issue that a platelet count of 10 x 109/L may not be equivalent to 20 x 109/L as previously thought (Estcourt 2012a).
How the intervention might work
Prophylactic platelet threshold
The morning platelet count has traditionally been used to indicate when a patient requires prophylactic platelet transfusions. It became standard practice to transfuse platelets at platelet counts below 20 x 109/L, in an attempt to prevent bleeding (Beutler 1993). This practice was partly based on the findings of non‐randomised studies that showed that gross haemorrhage (haematuria, haematemesis, and melaena) was present at platelet counts below 5 x 109/L more frequently than when the platelet count was between 5 x 109/L and 100 x 109/L (Gaydos 1962; Slichter 1978). However, these studies did not clearly support the use of a threshold for prophylactic platelet transfusion of 20 x 109/L, nor was any threshold effect seen (Gaydos 1962; Slichter 1978). A similar pattern of increased bleeding at platelet counts ≤ 5 x 109/L was also seen in two recent RCTs (Slichter 2010; Wandt 2012).
The routine use of platelet transfusions in people with haematological malignancies from the 1970s resulted in a decreased mortality rate due to bleeding (less than 1% of patients) (Slichter 1980). Despite the lack of evidence, the widespread use of a threshold platelet count of 20 x 109/L for prophylactic platelet transfusions led to a marked growth in the demand for platelet concentrates (Sullivan 2002). This increased demand stimulated research to address whether the threshold could be safely lowered to 10 x 109/L (Rebulla 1997, reviewed in Stanworth 2004). The consensus formulated from these trials was that people should receive a platelet transfusion when the platelet count is < 10 x 109/L, unless there are other risk factors for bleeding such as sepsis, concurrent use of antibiotics, or other abnormalities of haemostasis (BCSH 2003; BCSH 2004; Board 2009; NBA 2012; Schiffer 2001; Slichter 2007; Tinmouth 2007), when the threshold should be raised.
There have been calls for a further reduction in the threshold to 5 x 109/L because of the previously mentioned evidence for an increased rate of bleeding at a platelet count of ≤ 5 x 109/L (BCSH 2003; Gmür 1991). However, a major concern in doing this is the reported inaccuracy of current automated counters when the platelet count is very low (Harrison 2001). This was well demonstrated in a large multi‐centre study of platelet analyser accuracy when measuring platelet counts < 20 x 109/L (Segal 2005).
Platelet mass has been used as a transfusion trigger for neonatal platelet transfusions (Gerday 2009). Different platelet count thresholds have been the only known trigger used in people with a haematological disorder.
Assessment of bleeding
A bleeding assessment has been seen as a more clinically relevant measure of the effect of platelet transfusions than surrogate markers such as the platelet increment.
Any review that uses bleeding as a primary outcome measure needs to assess the way that the trials have recorded bleeding. Unfortunately, the way bleeding has been recorded and assessed has varied markedly between trials (Cook 2004; Estcourt 2013; Heddle 2003).
Retrospective analysis of bleeding leads to a risk of bias because bleeding events may be missed, and only more severe bleeding is likely to have been documented. Prospective bleeding assessment forms provide more information and are less likely to miss bleeding events. However, different assessors may grade the same bleed differently, and it is very difficult to blind the assessor to the intervention.
The majority of trials have used the WHO system, or a modification of it, for grading bleeding (Estcourt 2013; Koreth 2004; WHO 1979). One limitation of all the scoring systems based on the WHO system is that the categories are relatively broad and subjective, meaning that a small change in a participant's bleeding risk may not be detected. Another limitation is that the modified WHO categories are partially defined by whether a bleeding participant requires a blood transfusion. The threshold for intervention may vary between clinicians and institutions, and so the same level of bleeding may be graded differently in different institutions.
The definition of what constitutes clinically significant bleeding has varied between studies. Although the majority of more recent platelet transfusion studies have classified it as WHO Grade 2 or above (Heddle 2009a; Slichter 2010; Stanworth 2010; Wandt 2012), in the past there has been greater heterogeneity (Cook 2004; Estcourt 2013; Koreth 2004). The difficulties of assessing and grading bleeding may limit the ability to compare results between studies, and this needs to be kept in mind when reviewing the evidence for the effectiveness of prophylactic platelet transfusions at different doses.
Why it is important to do this review
Although considerable advances have been made in platelet transfusion therapy in the last 40 years, 3 major areas continue to provoke debate.
Firstly, what is the optimal prophylactic platelet dose to prevent thrombocytopenic bleeding?
Secondly, which threshold should be used to trigger the transfusion of prophylactic platelets?
Thirdly, are prophylactic platelet transfusions superior to therapeutic platelet transfusions for the prevention or control of life‐threatening thrombocytopenic bleeding?
The initial formulation of this Cochrane review attempted to answer these questions, but the evidence at the time was insufficient for us to draw any definitive conclusions (Stanworth 2004). This review was updated (Estcourt 2012a). For clarity and simplicity, we have now split the review to answer each question separately.
This review focuses solely on the second question: Which threshold should be used to trigger the transfusion of prophylactic platelets?
Avoiding the need for unnecessary prophylactic platelet transfusions in people with haematological disorders will have significant logistical and financial implications for national health services as well as decreasing patients' exposure to the risks of transfusion. These factors are perhaps even more important in the development of platelet transfusion strategies in low‐income countries, where access to blood components is much more limited than in high‐income countries (Verma 2009).
This review did not assess the evidence for the answers to the other two questions, as these are the focus of separate Cochrane reviews, nor did it assess the use of alternative agents instead of prophylactic platelet transfusions because this is the focus of another review.
This review did not assess whether there are any differences in the efficacy of apheresis versus whole‐blood derived platelet products, the efficacy of pathogen‐reduced platelet components, the efficacy of human leukocyte antigen (HLA)‐matched versus random‐donor platelets, or differences between ABO identical and ABO non‐identical platelet transfusions, as recent systematic reviews have covered these topics (Butler 2013; Heddle 2008; Pavenski 2013; Shehata 2009).
Objectives
To determine whether different platelet transfusion thresholds for administration of prophylactic platelet transfusions (platelet transfusions given to prevent bleeding) affect the efficacy and safety of prophylactic platelet transfusions in preventing bleeding in people with haematological disorders undergoing myelosuppressive chemotherapy or haematopoietic stem cell transplantation (HSCT).
Methods
Criteria for considering studies for this review
Types of studies
We included randomised controlled trials (RCTs) in this review irrespective of language or publication status.
Types of participants
People with haematological disorders receiving treatment with myelosuppressive chemotherapy or stem cell transplantation, or both. We included people of all ages, in both inpatient and outpatient clinical settings. If trials consisted of mixed populations of patients (for example people with diagnoses of solid tumours), we used only data from the haematological subgroups. If subgroup data for haematological patients were not provided (after contacting the authors of the trial), we excluded the trial if fewer than 80% of participants had a haematological disorder. We excluded any participants who were not being treated with intensive chemotherapy or a stem cell transplant. We included participants with non‐malignant haematological disorders (for example aplastic anaemia, congenital bone marrow failure syndromes) who were being treated with an allogeneic stem cell transplant. These participants would be expected to be thrombocytopenic during pre‐transplant conditioning therapy and during the transplantation period, requiring platelet transfusion support.
Types of interventions
Participants received transfusions of platelet concentrates, prepared either from individual units of whole blood or by apheresis, and given prophylactically to prevent bleeding. Prophylactic platelet transfusions are typically given when blood platelet counts fall below a given trigger level. There was no restriction on dose or frequency of platelet transfusion or the type of platelet component, but we took this information into account in the analysis, where available.
We included the following comparisons:
Lower platelet count threshold (5 x 109/L) versus standard platelet transfusion threshold (10 x 109/L).
Higher platelet count threshold (20 x 109/L, 30 x 109/L, or 50 x 109/L) versus standard platelet transfusion threshold (10 x 109/L).
Different platelet count thresholds (5 x 109/L, 20 x 109/L, 30 x 109/L, or 50 x 109/L) that do not include a comparison against the standard platelet transfusion threshold (10 x 109/L).
Alternative thresholds to guide prophylactic platelet transfusions (e.g. platelet mass, immature platelet fraction, absolute immature platelet number). As there are currently no standard thresholds used for these alternative platelet measures, we planned to use the study's own thresholds for these alternative measures.
Types of outcome measures
Primary outcomes
Number and severity of bleeding episodes during the first 30 days of the study:
The number of participants with at least one bleeding episode.
The total number of days on which bleeding occurred.
Number of participants with at least one episode of severe or life‐threatening haemorrhage.
Time to first bleeding episode from the start of study.
Secondary outcomes
Mortality (all‐causes, secondary to bleeding, and secondary to infection) within 30 and 90 days from the start of the study.
Number of platelet transfusions per participant and number of platelet components per participant within 30 days from the start of the study.
Number of red cell transfusions per participant and number of red cell components per participant within 30 days from the start of the study.
Platelet transfusion interval within 30 days from the start of the study.
Proportion of participants requiring additional interventions to stop bleeding (surgical, medical e.g. tranexamic acid, other blood products e.g. fresh frozen plasma (FFP), cryoprecipitate).
Overall survival within 30, 90, and 180 days from the start of the study.
Proportion of participants achieving complete remission within 30 and 90 days from the start of the study.
Total time in hospital within 30 days from the start of the study.
Adverse effects of treatments (transfusion reactions, thromboembolism, transfusion‐transmitted infection, development of platelet antibodies, development of platelet refractoriness) within 30 days from the start of the study.
Quality of life, as defined by the individual studies.
We expressed all primary and secondary outcomes in the formats defined in the Measures of treatment effect section of this protocol if data were available, except for two of our outcomes that we planned to be only narrative reports.
These were:
Platelet transfusion interval, as it can be calculated in many different ways and it was unlikely that the exact methodology would be reported sufficiently to allow us to combine the data.
Assessment of quality of life (QoL). We planned to use the study's own measure, as there is no definitive patient‐reported outcome measure for this patient group (Estcourt 2014e).
However, none of the included studies reported either of these outcomes.
Search methods for identification of studies
The Systematic Review Initiative (SRI) Information Specialist (CD) formulated new search strategies in collaboration with the Cochrane Haematological Malignancies Review Group based on those used in previous versions of this review (Estcourt 2012a; Stanworth 2004).
Electronic searches
Bibliographic databases
We searched for RCTs in the following databases:
Cochrane Central Register of Controlled Trials (CENTRAL) (Cochrane Library 2015, Issue 6, 23 July 2015) (Appendix 1)
MEDLINE (OvidSP, 1946 to 23 July 2015) (Appendix 2)
PubMed (epublications only to 23 July 2015) (Appendix 3)
Embase (OvidSp, 1974 to the 23 July 2015) (Appendix 4)
CINAHL (EBSCOhost, 1937 to 23 July 2015) (Appendix 5)
UKBTS/SRI Transfusion Evidence Library (www.transfusionevidencelibrary.com) (1950 to 23 July 2015) (Appendix 6)
Web of Science: Conference Proceedings Citation Index‐Science (CPCI‐S) (Thomson Reuters, 1990 to 23 July 2015) (Appendix 7)
LILACS (BIREME/PAHO/WHO, 1982 to to 23 July 2015) (Appendix 8)
IndMed (ICMR‐NIC, 1985 to 23 July 2015) (Appendix 9)
KoreaMed (KAMJE, 1997 to 23 July 2015) (Appendix 10)
PakMediNet (2001 to 23 July 2015) (Appendix 10)
We updated searches from the original search in January 2002, Stanworth 2004, and the updated search on 10 November 2011 (Estcourt 2012a). We combined searches in MEDLINE, Embase, and CINAHL with adaptations of the Cochrane RCT search filters, as detailed in the Cochrane Handbook for Systematic Reviews of Interventions (Lefebvre 2011). We did not limit searches by language or publication status.
Databases of ongoing trials
We also searched ClinicalTrials.gov (http://clinicaltrials.gov/ct2/search) (Appendix 11), the WHO International Clinical Trials Registry (ICTRP) (http://apps.who.int/trialsearch/) (Appendix 11), the ISRCTN Register (http://www.controlled‐trials.com/isrctn/) (Appendix 12), the EU Clinical Trials Register (https://www.clinicaltrialsregister.eu/ctr‐search) (Appendix 12), and the Hong Kong Clinical Trials Register (http://www.hkclinicaltrials.com/) (Appendix 13) in order to identify ongoing trials to 23 July 2015.
All new search strategies are presented as indicated in Appendices 1 to 13. Search strategies for both the original (2002) and update (2011) searches are presented in Appendix 14.
Searching other resources
We augmented database searching with the following.
Handsearching of reference lists
We checked references of all included trials, relevant review articles, and current treatment guidelines for further literature. We limited these searches to the 'first generation' reference lists.
Personal contacts
We contacted authors of relevant studies, study groups, and experts worldwide known to be active in the field for unpublished material or further information on ongoing studies.
Data collection and analysis
Selection of studies
We updated the selection of studies from the selection of studies performed for the previous version of this review (Estcourt 2012a).
Two out of three independent review authors (LE, PB, and CD) initially screened all electronically derived citations and abstracts of papers identified by the review search strategy for relevance. We excluded studies clearly irrelevant at this stage.
Two independent review authors (LE, PB) then formally assessed the full texts of all potentially relevant trials for eligibility against the criteria outlined above. We resolved all disagreements by discussion without the need to consult a third review author (SS). We sought further information from study authors if an article contained insufficient data to make a decision about eligibility. We designed a study eligibility form for trials of platelet transfusion to help in the assessment of relevance, which included ascertaining whether the participants had haematological disorders and whether the two groups could be defined in the trial on the basis of differences in use of prophylactic platelet transfusion doses. We recorded the reasons why potentially relevant studies failed to meet the eligibility criteria.
Data extraction and management
We updated the data extraction from the data extraction performed for the previous version of this review, Estcourt 2012a, to include new review outcomes that were not part of the previous review (for example platelet transfusion interval, quality of life). We identified no new studies in this updated review.
Two review authors (LE, SS) conducted data extraction according to the guidelines proposed by The Cochrane Collaboration (Higgins 2011a). Any disagreements between the review authors were resolved by consensus. The review authors were not blinded to names of authors, institutions, journals, or the outcomes of the trials. The data extraction forms had been piloted in the previous version of this review (Estcourt 2012a). Due to minor changes in the format, we piloted the forms on a further study; thereafter the two review authors (LE, SS) independently extracted data for all the studies. We extracted the following data.
General information
Review author's name, date of data extraction, study ID, first author of study, author's contact address (if available), citation of paper, objectives of the trial.
Trial details
Trial design, location, setting, sample size, power calculation, treatment allocation, randomisation, blinding, inclusion and exclusion criteria, reasons for exclusion, comparability of groups, length of follow‐up, stratification, stopping rules described, statistical analysis, results, conclusion, and funding.
Characteristics of participants
Age, gender, ethnicity, total number recruited, total number randomised, total number analysed, types of haematological disease, lost to follow‐up numbers, dropouts (percentage in each arm) with reasons, protocol violations, previous treatments, current treatment, prognostic factors.
Interventions
Experimental and control interventions, type of platelet given, timing of intervention, dosage of platelet given, compliance to interventions, additional interventions given especially in relation to red cell transfusions, any differences between interventions.
Assessment of bias
Sequence generation, allocation concealment, blinding (participants, personnel, and outcome assessors), incomplete outcome data, selective outcome reporting, other sources of bias.
Outcomes measured
Number and severity of bleeding episodes. Mortality (all causes), and mortality due to bleeding. Overall survival. Proportion of participants achieving complete remission. Time in hospital. Number of platelet transfusions and platelet components. Number of red cell transfusions and red cell components. Platelet transfusion interval. Proportion of participants requiring additional interventions to stop bleeding (surgical, medical such as tranexamic acid, other blood products such as fresh frozen plasma (FFP), cryoprecipitate). Quality of life. Adverse effects of treatments (for example transfusion reactions, thromboembolism, transfusion‐transmitted infection, development of platelet antibodies or platelet refractoriness).
We used both full‐text versions and abstracts to retrieve the data. We extracted publications reporting on more than one trial using one data extraction form for each trial. We extracted trials reported in more than one publication on one form only. When these sources provided insufficient information, we contacted the authors and study groups for additional details.
One review author performed data entry into software, which a second review author checked for accuracy.
Assessment of risk of bias in included studies
We updated the 'Risk of bias' assessment to include study funding from the 'Risk of bias' assessment performed for the previous version of this review (Estcourt 2012a).
The assessment included information about the design, conduct, and analysis of the trial. We evaluated each criterion on a three‐point scale: low risk of bias, high risk of bias, or unclear (Higgins 2011c). To assess risk of bias, we addressed the following questions in the 'Risk of bias' table for each included study:
Was the allocation sequence adequately generated?
Was allocation adequately concealed?
Was knowledge of the allocated intervention adequately prevented during the study (including an assessment of blinding of participants, personnel, and outcome assessors)?
Were incomplete outcome data adequately addressed (for every outcome separately)?
Are reports of the study free of selective outcome reporting?
Was the study apparently free of other problems that could put it at risk of bias? This included assessing whether protocol deviation was balanced between treatment arms.
Measures of treatment effect
For dichotomous outcomes, we recorded the number of outcomes in the treatment and control groups and estimated the treatment effect measures across individual studies as the relative effect measures (risk ratio with 95% confidence intervals (CIs)).
For continuous outcomes, we recorded the mean and standard deviations. For continuous outcomes measured using the same scale, the effect measure was the mean difference with 95% CIs, or the standardised mean difference for outcomes measured using different scales. For time‐to‐event outcomes, we extracted the hazard ratio from published data according to Parmar 1998 and Tierney 2007.
We did not report the number needed to treat to benefit with CIs and the number needed to treat to harm with CIs because there were no differences between any of the bleeding outcomes.
If we could not report the available data in any of the formats described above, we performed a narrative report.
Unit of analysis issues
We did not prespecify in the protocol how we would deal with any unit of analysis issues. There was a unit of analysis issue for this review for the total number of days of bleeding. We only reported the number of days of bleeding if it had been reported per participant or if an appropriate analysis had been performed by the authors to account for repeated measures. In this review, the Rebulla 1997 authors used a permutation analysis to take into account the repeated events data (Freedman 1989). All other studies had not taken into account unit of analysis issues with this outcome and data were not reported.
Dealing with missing data
We dealt with missing data according to the recommendations in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins 2011b). We contacted four authors to obtain information that was missing or unclear in the published report. Two authors supplied missing data (Heckman 1997; Rebulla 1997).
In trials that included people with haematological disorders as well as people with solid tumours or non‐malignant haematological disorders, we extracted data for the malignant haematology subgroup from the general trial data. We could not do this in one study (Zumberg 2002); we contacted the authors, but they no longer had access to the original data, and the original reports did not provide subgroup data. We therefore excluded this study from the review.
Within an outcome, the preferred analysis was an intention‐to‐treat analysis. When data were missing, we recorded the number of participants lost to follow‐up for each trial.
Assessment of heterogeneity
If we considered studies to be sufficiently homogenous in their study design, we conducted a meta‐analysis and assessed the statistical heterogeneity (Deeks 2011). We assessed statistical heterogeneity of treatment effects between trials using a Chi2 test with a significance level at P < 0.1. We used the I2 statistic to quantify heterogeneity (I2 > 50% moderate heterogeneity, I2 > 80% considerable heterogeneity). We explored potential causes of heterogeneity by sensitivity and subgroup analyses where possible.
Assessment of reporting biases
We did not perform a formal assessment of potential publication bias (small‐trial bias) because we included only three studies in this review (Sterne 2011).
Data synthesis
We performed analyses according to the recommendations of The Cochrane Collaboration (Deeks 2011). We used aggregated data for analysis. For statistical analysis, we entered data into Review Manager 5.3.
Where meta‐analysis was feasible, we used the fixed‐effect model for pooling the data. We used the Mantel‐Haenszel method for dichotomous outcomes, and the inverse‐variance method for continuous outcomes. We used the generic inverse‐variance method for time‐to‐event outcomes.
We used the random‐effects model for sensitivity analyses as part of the exploration of heterogeneity. If we found heterogeneity, as expressed by the I2, to be above 50%, we reported both the fixed‐effect and random‐effects models. If we found heterogeneity to be above 80%, we did not perform a meta‐analysis and commented on results as a narrative.
Summary of findings tables
We used GRADE 2014 to create 'Summary of findings' tables as suggested in the Cochrane Handbook for Systematic Reviews of Interventions (Schünemann 2011). This included the number and severity of bleeding episodes within 30 days from the start of the study (number of participants with at least one bleeding episode; number of days on which bleeding occurred; number of participants with severe or life‐threatening bleeding; time to first bleeding episode), number of platelet transfusions within 30 days from the start of the study, 30‐day mortality, and quality of life.
Subgroup analysis and investigation of heterogeneity
We considered performing subgroup analysis on the following characteristics, if appropriate:
Presence of fever (> 38°C).
Underlying disease.
Type of treatment (autologous haematopoietic stem cell transplantation (HSCT), allogeneic HSCT, or chemotherapy alone).
Age of the participant (paediatric, adults, older adults (> 60 years)).
We did not perform two subgroup analyses due to lack of data; these were presence of fever and type of treatment.
We did not perform meta‐regression because no subgroup contained more than 10 studies (Deeks 2011). We commented on differences between subgroups as a narrative.
Investigation of heterogeneity between studies also included, if appropriate:
Age of the study (as the type of platelet component has changed over the last 40 years).
Different platelet component doses.
We did not assess age of study as a reason for heterogeneity, as all studies recruited participants between 1991 and 2001.
Sensitivity analysis
We had intended to assess the robustness of our findings by the following two sensitivity analyses:
Including only those trials at low risk of bias.
Including only those trials in which 20% of participants or less were lost to follow‐up.
All trials were at risk of bias because none of the three included RCTs blinded investigators to the intervention.
None of the three included trials had more than 20% of participants lost to follow‐up.
We therefore did not perform these two pre‐planned sensitivity analyses.
Results
Description of studies
See Characteristics of included studies and Characteristics of excluded studies; there were no ongoing studies.
Results of the search
See PRISMA flow diagram (Figure 1).
1.
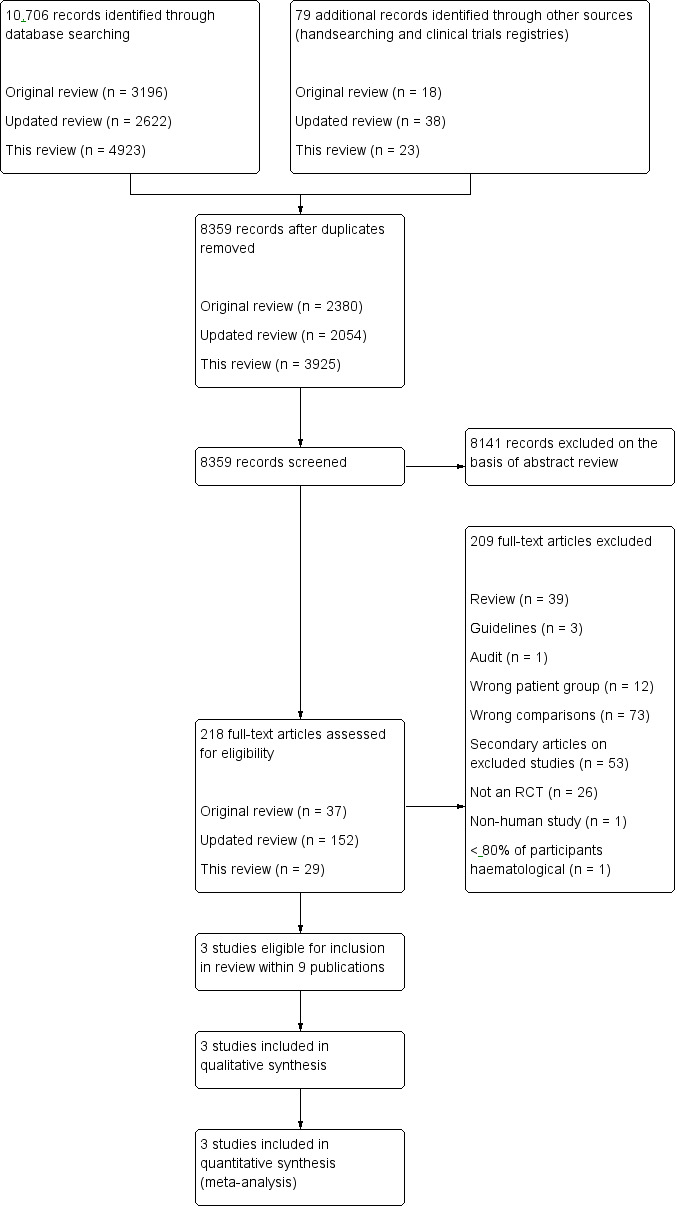
Study flow diagram.
The original search (conducted January 2002) identified a total of 3196 potentially relevant records. There were 2380 records after duplicates were removed, and 2343 records were excluded on the basis of the abstract. The original systematic review identified 37 studies that appeared relevant on the basis of their full text or abstract using the original inclusion/exclusion criteria (Stanworth 2004).This was performed by one review author.
The updated search for the previous review (conducted November 2011) identified a total of 2622 potentially relevant records. There were 2054 records after duplicates were removed, and two review authors excluded 1865 records on the basis of the abstract. We retrieved 152 full‐text articles for relevance. Two review authors (LE, SS) reviewed these full‐text articles and those from the original review (a total of 189 records) (Estcourt 2012a).
The latest update of the search (conducted 23 July 2015) identified a total of 4923 potentially relevant records. There were 3925 records after duplicates were removed. Two review authors (LE, SS) were able to exclude 3896 records on the basis of the abstract. Two review authors (LE, SS) retrieved for relevance and reviewed 29 full‐text articles.
Included studies
See Characteristics of included studies for full details of each study.
Ongoing studies
This update of the review identified no ongoing studies that were eligible for inclusion.
Studies contributing to the main outcome
The three RCTs (9 publications) were published between 1997 and 2005. There were six secondary citations of included studies (cited as secondary references for the relevant included studies).
There were no new studies. The three included studies, Diedrich 2005, Heckman 1997, and Rebulla 1997, were identified in the previous version of this review (Estcourt 2012a). One study that had been included in the original review, Stanworth 2004, was excluded in the previous version of this review, Estcourt 2012a, because fewer than 80% of participants had a haematological disorder, and no subgroup data could be identified (Zumberg 2002).
The three included RCTs were distributed across the review's four subcategories as follows:
No studies compared a lower platelet count threshold (5 x 109/L) versus a standard platelet transfusion threshold (10 x 109/L).
All three studies compared a standard platelet transfusion threshold (10 x 109/L) versus a higher platelet count threshold (20 x 109/L, 30 x 109/L, or 50 x 109/L).
No studies compared different platelet count thresholds (5 x 109/L, 20 x 109/L, 30 x 109/L, or 50 x 109/L) that did not include a comparison against the standard platelet transfusion threshold (10 x 109/L).
No studies compared alternative thresholds to guide prophylactic platelet transfusions (e.g. platelet mass, immature platelet fraction, absolute immature platelet number).
This review therefore only discussed the subcategory that compared a standard platelet transfusion threshold (10 x 109/L) versus a higher platelet count threshold (20 x 109/L, 30 x 109/L, or 50 x 109/L).
See Table 2 for study characteristics including: number and type of participants; type of intervention (actual thresholds used); duration of study; dose of platelet component; type of platelet product; and primary outcome.
1. Characteristics of the included studies.
| Study | Type of participants | Number of participants | Intervention | Platelet component dose | Duration of study | Type of platelet component | Primary outcome |
| Diedrich 2005 | All ages undergoing an allogeneic HSCT | 166 | Prophylactic plt transfusion if plt count < 10 x 109/L versus prophylactic plt transfusion if plt count < 30 x 109/L | Average yield (mean ± SD) 4.10 x 1011 ± 0.2 x 1011 (buffy coat) 3.80 x 1011 ± 0.2 x 1011 (apheresis) |
Maximum duration of observation was 37 days (7 days pre‐HSCT and 30 days post‐HSCT). No information available on the number of participants who died or were lost to follow‐up | Leucodepleted, ABO ‐matched, irradiated pooled random‐donor platelets (buffy coat) 85% Apheresis 15% | Number of platelet transfusions |
| Heckman 1997 | Adults with acute leukaemia | 82 | Prophylactic plt transfusion if plt count ≤ 10 x 109/L versus prophylactic plt transfusion if plt count ≤ 20 x 109/L |
1 apheresis unit. Average yield each study year (number of transfusions) 4.9 x 1011 1991 (n = 502) 4.5 x1011 1992 (n = 418) 4.7 x 1011 1993 (n = 399) 4.0 x 1011 1994 (n = 400) 4.3 x 1011 1995 (n = 398) |
Median 24 days | Leucodepleted Apheresis |
Not reported |
| Rebulla 1997 | Adolescents and adults with AML | 276 | Prophylactic plt transfusion if plt count < 10 x 109/L versus prophylactic plt transfusion if plt count < 20 x 109/L |
Median 2.2 x 1011 (pooled) 2.8 x 1011 (apheresis) |
Mean 27.8 to 29.7 days | Apheresis and pooled products | Frequency and severity of haemorrhage |
AML = acute myeloid leukaemia
HSCT = haematopoietic stem cell transplant
plt = platelet
SD = standard deviation
Study design
All three studies were open‐label studies. Two studies were single‐centre parallel RCTs (Diedrich 2005; Heckman 1997), and one study was a multicentre parallel RCT (Rebulla 1997).
Study size
The number of participants randomised ranged from 78 in Heckman 1997 to 276 in Rebulla 1997.
Setting
Two studies were conducted in the 1990s (Heckman 1997; Rebulla 1997), and one study was conducted in the early 2000s (Diedrich 2005). The studies were conducted in Italy (Rebulla 1997), Sweden (Diedrich 2005), and the United States (Heckman 1997).
Participants
In total, 520 participants were randomised; of these, 499 were included in the analysis. We excluded 21 participants randomised in Rebulla 1997 from the analysis (16 no study records received; two received non‐myeloablative chemotherapy; three died (two within 24 hours of enrolment in the study). Two of the studies examined adults with acute leukaemia; one included adults with acute lymphocytic leukaemia (ALL) or acute myeloid leukaemia (AML) (Heckman 1997), and the other included only adults with AML (Rebulla 1997). Both studies excluded adults with acute promyelocytic leukaemia (APL). The third study included both adults and children undergoing an allogeneic HSCT (Diedrich 2005).
Intervention
Two studies compared a prophylactic transfusion threshold of 10 x 109/L with a threshold of 20 x 109/L (Heckman 1997; Rebulla 1997). One study compared a threshold of 10 x 109/L with a threshold of 30 x 109/L (Diedrich 2005).
Co‐interventions
In two of the three studies a red cell transfusion policy was stated (Diedrich 2005; Rebulla 1997). Both studies transfused red cells when the haemoglobin was less than 80 g/L.
Outcomes
Two of the three studies defined a primary outcome (Diedrich 2005; Rebulla 1997). In Rebulla 1997, the primary outcome was the frequency and severity of bleeding, and the secondary outcome was the number of platelet transfusions, whereas in Diedrich 2005, the number of platelet transfusions was the primary outcome, with bleeding as one of the secondary outcomes. The third study, Heckman 1997, stated that its main aims were to look at platelet use and bleeding complications. All three studies commented on adverse events associated with platelet transfusions.
Funding sources
Two studies reported the funding sources for the trial (Diedrich 2005; Heckman 1997). All funding sources were either charitable foundations or government funds.
Excluded studies
See Characteristics of excluded studies for further details.
Twelve studies were excluded because they compared different participant groups (Andrew 1993; Arnold 2006; Bai 2004; Fanning 1995; Gajic 2006; Gerday 2009; Johansson 2007; Julmy 2009; NCT00699621; Reed 1986; Spiess 2004; Vadhan‐Raj 2002).
Seventy‐three studies compared different types of platelet formulations with outcome measures not relevant to the eligibility criteria (Agliastro 2006; Akkök 2007; Anderson 1997; Arnold 2004; Bentley 2000; Blumberg 2002; Blumberg 2004; Blundell 1996; Carr 1990; Corash 2001; Couban 2002; de Wildt‐Eggen 2000; Diedrich 2009; Di Pietro 1998; Dumont 2011; Gmür 1983; Goodnough 2001; Goodrich 2008; Grossman 1980; Gurkan 2007; Harrup 1999; Heal 1993; Heddle 1994; Heddle 1999; Heddle 2002; Heddle 2005; Heddle 2009; Higby 1974; ISRCTN01292427; ISRCTN49080246; ISRCTN56366401; Kakaiya 1981; Kerkhoffs 2010; Klumpp 1999; Kluter 1996; Lapierre 2003; Leach 1991; Lee 1989; Lozano 2010; Lozano 2011; Lu 2011; McCullough 2004; Messerschmidt 1988; Mirasol 2010; Murphy 1982; Murphy 1986; NCT01615146; Norville 1994; Norville 1997; Oksanen 1991; Oksanen 1994; Pamphilon 1996; Schiffer 1983; Shanwell 1992; Singer 1988; Sintnicolaas 1981; Sintnicolaas 1982; Sintnicolaas 1995; Slichter 1998; Slichter 2006; Slichter 2010; Solomon 1978; Stanworth 2013; Strindberg 1996; Sweeney 2000; Tinmouth 2004; TRAP 1997; Van Marwijk 1991; van Rhenen 2003; Wandt 2012; Wang 2002; Williamson 1994; Zhao 2002).
Three records were guidelines (Follea 2004; Samama 2005; Tosetto 2009).
One record was an audit (Qureshi 2007).
Thirty‐nine records were reviews (Andreu 2009; Avvisati 2003; Benjamin 2002; Blajchman 2008; Buhrkuhl 2010; Casbard 2004; Cid 2007; Dzik 2004; Goodnough 2002; Goodnough 2005; Heal 2004; Heddle 2003; Heddle 2007; Jelic 2006; Levi 2002; Lordkipanidze 2009; Lozano 2003; Martel 2004; McNicol 2003; Paramo 2004; Poon 2003; Rabinowitz 2010; Rayment 2005; Razzaghi 2012; Roberts 2003; Sakakura 2003; Shehata 2009; Shen 2007; Slichter 2004; Slichter 2007; Slichter 2012; Sosa 2003; Strauss 2004; Strauss 2005; Tinmouth 2003; Wandt 2010; Wang 2005; Woodard 2002; Zeller 2014).
Twenty‐six studies were not RCTs (Aderka 1986; Callow 2002; Cameron 2007; Chaoui 2005; Chaurasia 2012; Decaudin 2004; Eder 2007; Elting 2002; Elting 2003; Friedmann 2002; Gil‐Fernandez 1996; Gmür 1991; Greeno 2007; Hardan 1994; Lawrence 2001; Navarro 1998; Nevo 2007; Norol 1998; Paananen 2009; Sagmeister 1999; Verma 2008; Wandt 1998; Wandt 2005; Wandt 2006; Weigand 2009; Zahur 2002).
Fifty‐three records were secondary citations of excluded studies (cited as secondary references for the relevant excluded studies).
One study was a non‐human study (Velik‐Salchner 2007).
One study was a study in which fewer than 80% of the participants were haematological patients, and no data were available on the haematological subgroup (Zumberg 2002). Zumberg 2002 had been included in the previous review Stanworth 2004, but for this reason it has now been excluded.
Risk of bias in included studies
See Figure 2 and Figure 3 for visual representations of the 'Risk of bias' assessments across all studies and for each item in the included studies. See the Characteristics of included studies section 'Risk of bias' table for further information about the bias identified within the individual trials.
2.
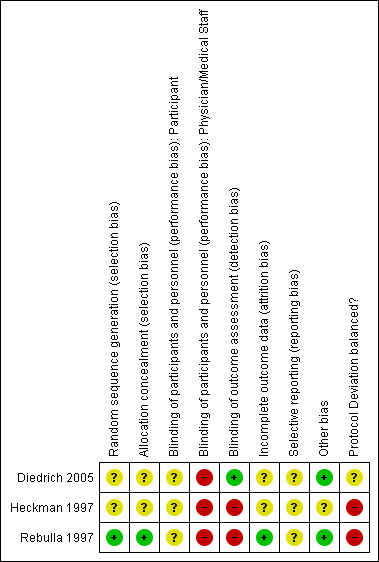
Risk of bias summary: review authors' judgements about each risk of bias item for each included study.
3.
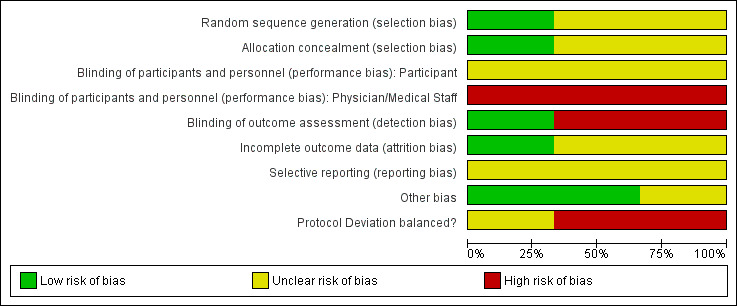
Risk of bias graph: review authors' judgements about each risk of bias item presented as percentages across all included studies.
All three studies had some threats to validity (Diedrich 2005; Heckman 1997; Rebulla 1997). The majority of these potential risks were due to a lack of detail provided on the specific criteria and were thus judged as 'unclear risk' using the Cochrane grading system.
Allocation
We assessed one study as low risk of selection bias due to adequate methods of sequence generation and allocation concealment (Rebulla 1997). We assessed the two remaining studies as unclear risk of selection bias due to the lack of information on sequence generation and allocation concealment (Diedrich 2005; Heckman 1997).
Blinding
We assessed all three studies as high risk of performance bias due to lack of blinding of medical staff (Diedrich 2005; Heckman 1997; Rebulla 1997).
We assessed one study as low risk of detection bias because there was adequate blinding of the bleeding assessor (Diedrich 2005). We assessed the other two studies as high risk of detection bias because the bleeding assessors and medical staff were unblinded (Heckman 1997; unpublished data of Rebulla 1997).
Incomplete outcome data
We assessed one study as low risk of attrition bias because the number of participants with missing outcome data were balanced across the intervention groups (Rebulla 1997). We assessed the two remaining studies as unclear risk of selection bias due to the lack of information on the number of participants lost to follow‐up (Diedrich 2005; Heckman 1997).
Selective reporting
We assessed all three studies as unclear risk of selection bias because as study protocols were not available, it was unclear whether any of the studies were free of selective reporting (Diedrich 2005; Heckman 1997; Rebulla 1997).
Other potential sources of bias
Protocol deviation
We assessed two of the three studies as at high risk of bias due to an imbalance in protocol deviations between the different arms of the studies (Heckman 1997; Rebulla 1997). The third study was insufficiently reported for us to make an adequate assessment (Diedrich 2005). In Heckman 1997, there was a statistically significant difference between the two arms. Fourteen out of 37 participants with a transfusion threshold of 10 x 109/L were affected by protocol deviations, whereas only 6 out of 41 participants with a transfusion threshold of 20 x 109/L were affected. In Rebulla 1997, the pre‐transfusion platelet count was higher than indicated in the protocol in 5.4% of platelet transfusions with a transfusion threshold of 10 x 109/L, but only 2% of platelet transfusions with a higher transfusion trigger were transfused outside the protocol guidelines; whether this was statistically significant was not reported.
Other potential sources
Two of the three studies appeared to be free of other sources of significant bias (Diedrich 2005; Rebulla 1997). The third study was insufficiently reported for us to make an adequate assessment (Heckman 1997).
Effects of interventions
See: Table 1
See Table 1.
In all the included studies, the study's own definition of clinically significant bleeding was used, unless otherwise stated (Table 3). The three studies used different grading systems for assessing bleeding.
2. Assessment and grading of bleeding.
| Study | Bleeding primary outcome of study | Method of bleeding assessment reported | Bleeding severity scale used | RBC usage part of bleeding severity assessment | RBC transfusion policy |
| Rebulla 1997 | Yes | Yes | New scale developed by Rebulla | Yes | Haemoglobin < 80 g/L |
| Heckman 1997 | Not reported | Yes | Ajani 1990 | Yes | Not reported |
| Diedrich 2005 | No | Yes | WHO 1979 | No | Haemoglobin < 80 g/L |
RBC = red blood cell
Number and severity of bleeding episodes
All three studies reported bleeding outcomes. The median study duration was less than 30 days in two studies, Heckman 1997 and Rebulla 1997, and a maximum of 37 days of observation in the third study (Diedrich 2005) (Table 2). We therefore assumed data from all three studies was relevant to the bleeding outcomes.
Number of participants with at least one bleeding episode during the first 30 days of the study
Two of the three studies reported this (Diedrich 2005; Rebulla 1997), and the author supplied data from the third study (Heckman 1997). A meta‐analysis including 499 participants showed no difference between standard versus higher transfusion trigger levels (risk ratio (RR) 1.35, 95% confidence interval (CI) 0.95 to 1.90) (Analysis 1.1), nor was any difference seen if the studies comparing a threshold of 10 x 109/L versus 20 x 109/L were analysed separately (RR 1.41; 95% CI 0.95 to 2.1) (Heckman 1997; Rebulla 1997), to the study comparing a threshold of 10 x 109/L versus 30 x 109/L (RR 1.19, 95% CI 0.59 to 2.37) (Diedrich 2005).
1.1. Analysis.
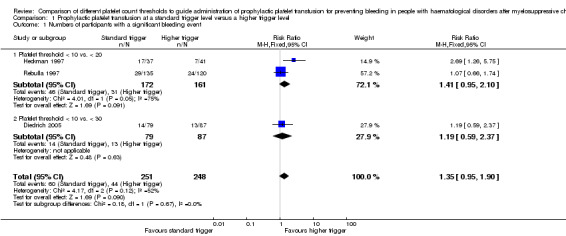
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 1 Numbers of participants with a significant bleeding event.
The total number of days on which bleeding occurred during the first 30 days of the study
This outcome could have a unit of analysis problem due to participants having more than one day of bleeding. The authors of one study performed an analysis that took into account the unit of analysis issues for this outcome (Rebulla 1997). They found that the overall proportion of person‐days of observation during which participants experienced WHO Grade 2 bleeding or worse was 123 out of 4005 (3.1%) and 60 out of 3330 (1.8%) for the standard and higher transfusion trigger arms, respectively, giving a relative proportion of days with WHO Grade 2 or worse bleeding (RR 1.71, 95% CI 0.84 to 3.48). A permutation test for the comparison of these proportions gives a P value of 0.162, and therefore the study authors found no significant difference between study arms. The other two studies did not take into account this unit of analysis issue (Diedrich 2005; Heckman 1997).
Number of participants with at least one episode of severe or life‐threatening haemorrhage during the first 30 days of the study
Two of the studies reported the number of participants with WHO Grade 3 and 4 bleeding (Diedrich 2005; Rebulla 1997). A meta‐analysis of this data showed no difference between a standard versus a higher trigger level (421 participants; RR 0.99, 95% CI 0.52 to 1.88) (Analysis 1.2).
1.2. Analysis.
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 2 Number of participants with WHO Grade 3 or 4 bleeding.
None of the studies reported the number of participants with WHO Grade 4 bleeding alone during the first 30 days of the study.
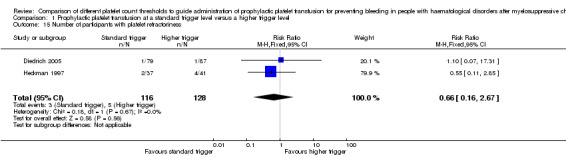
Only Diedrich 2005 reported the number of participants with bleeding that required a red cell transfusion. The study reported no significant difference between a standard versus a higher transfusion trigger level (RR 0.66, 95% CI 0.16 to 2.68) (Analysis 1.3).
1.3. Analysis.
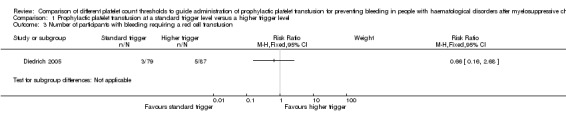
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 3 Number of participants with bleeding requiring a red cell transfusion.
None of the studies reported the number of participants with bleeding that caused cardiovascular compromise.
Time to first bleeding episode from the start of study
One study reported the time to the first bleeding episode (Rebulla 1997), showing no difference between the standard and higher transfusion trigger levels (hazard ratio 1.11, 95% CI 0.64 to 1.91) (Analysis 1.4).
1.4. Analysis.
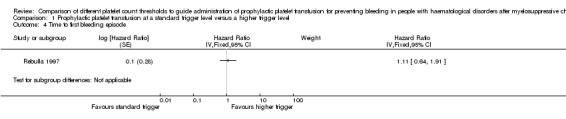
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 4 Time to first bleeding episode.
Mortality
All‐cause mortality within 30 and 90 days
Two of the three studies reported all‐cause mortality (Heckman 1997; Rebulla 1997). However, only one study reported it within a 30‐ or 90‐day study period (Rebulla 1997) (Analysis 1.5), and showed no difference between a standard versus a higher transfusion trigger (RR 1.78, 95% CI 0.83 to 3.81) (Analysis 1.5).
1.5. Analysis.
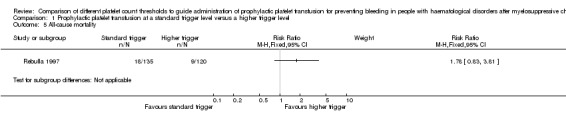
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 5 All‐cause mortality.
Mortality secondary to bleeding within 30 and 90 days
All three studies reported death due to bleeding, but it was only in the largest study that any deaths occurred (Rebulla 1997). One death due to intracerebral haemorrhage in the standard trigger arm was included in the analysis (RR 2.67, 95% CI 0.11 to 64.91) (Analysis 1.6). However, two further deaths due to intracerebral haemorrhage (one in each arm of the study) occurred in participants who were randomised but not included in the analysis. If analysis of the data included all randomised participants, then there was still no evidence of a statistically significant difference in death rate between the two arms of the study (RR 1.85, 95% CI 0.17 to 20.59) (assuming that those participants for which no data forms were returned did not die secondary to bleeding) (Analysis 1.7).
1.6. Analysis.
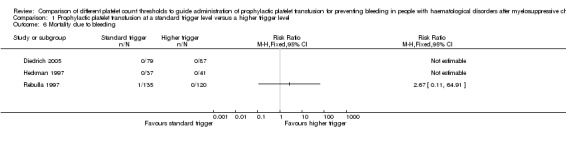
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 6 Mortality due to bleeding.
1.7. Analysis.
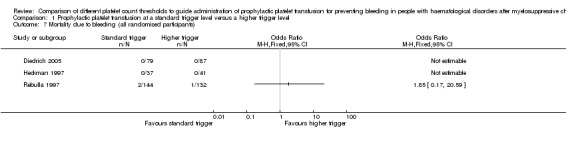
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 7 Mortality due to bleeding (all randomised participants).
Mortality secondary to infection within 30 and 90 days
One of the studies reported death due to infection (Rebulla 1997), showing no significant difference in mortality due to infection between a standard versus a higher transfusion trigger (RR 1.57, 95% CI 0.60 to 4.14) (Analysis 1.8).
1.8. Analysis.
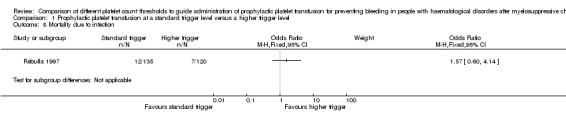
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 8 Mortality due to infection.
Number of platelet transfusions per participant and number of platelet components per participant within 30 days from the start of the study
All three studies reported on the number of platelet transfusions required per participant (Table 4). Diedrich 2005 reported the results as medians and ranges. A meta‐analysis of the other two studies, Heckman 1997 (unpublished data) and Rebulla 1997, showed a reduction in the mean number of platelet transfusions required in the standard threshold arm (mean difference (MD) (fixed effect) ‐2.09, 95% CI ‐3.20 to ‐0.99) (Analysis 1.9).
3. Number of platelet transfusions and number of platelet units.
| Study | Intervention | Number of participants in each arm | Number of platelet transfusions/participant | Comparison statistics | P value | Number of platelet units transfused/participant | Comparison statistics | P value |
| Short‐term follow‐up (up to 30 days) | ||||||||
| Diedrich 2005 | < 10 x 109/L | 79 | Median 4; range 0 to 32 | Not reported | < 0.001 | Not reported | Not reported | Not reported |
| < 30 x 109/L | 87 | Median 10; range 0 to 48 | Not reported | Not reported | ||||
| Heckman 1997 | ≤ 10 x 109/L | 37 | Mean 8.4 ± SD 5.3* | MD ‐3.00, 95% CI ‐5.76 to ‐0.24* |
Not reported | Not reported | Not reported | Not reported |
| ≤ 20 x 109/L | 41 | Mean 11.4 ± SD 7.1* | Not reported | Not reported | ||||
| Rebulla 1997 | < 10 x 109/L | 135 | Mean 7.05 ± SD 4.56 | MD ‐1.92, 95% CI ‐3.12 to ‐0.72 |
0.001 | Not reported | Not reported | Not reported |
| < 20 x 109/L | 120 | Mean 8.97 ± SD 5.17 | Not reported | Not reported | ||||
*unpublished data provided by the author. The paper provided medians and ranges median 7 (5 to 11) for the standard‐trigger arm and median 11 (6 to 15) for the higher‐trigger arm.
CI = confidence interval
MD = mean difference
SD = standard deviation
1.9. Analysis.
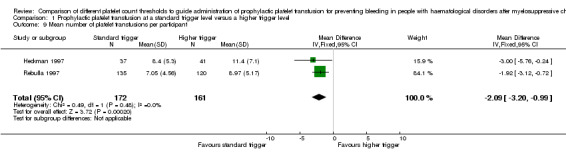
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 9 Mean number of platelet transfusions per participant.
None of the studies reported on the number of platelet components per participant.
Number of red cell transfusions per participant and number of red cell components per participant within 30 days from the start of the study
All three studies reported on the number of red cell transfusions required (Table 5). One of the studies reported the results as medians and ranges and showed no difference in the number of red cell transfusions required. A meta‐analysis of the other two studies, Heckman 1997 (unpublished data) and Rebulla 1997, showed no difference between the two arms in the mean number of red cell transfusions required (MD (fixed effect) 0.66, 95% CI ‐0.43 to 1.76) (Analysis 1.10).
4. Number of red cell transfusions and number of red cell units.
| Study | Intervention | Number of participants in each arm | Number of red cell transfusions/participant | Comparison statistics | P value | Number of red cell units transfused/participant | Comparison statistics | P value |
| Short‐term follow‐up (up to 30 days) | ||||||||
| Diedrich 2005 | < 10 x 109/L | 79 | Median 4; range 0 to 26 | Not reported | Not significant | Not reported | Not reported | Not reported |
| < 30 x 109/L | 87 | Median 4; range 0 to 31 | Not reported | Not reported | ||||
| Heckman 1997 | ≤ 10 x 109/L | 37 | Mean 12.2 ± SD 6.9* | MD 1.50, 95% CI ‐1.22 to 4.22* |
Not reported | Not reported | Not reported | Not reported |
| ≤ 20 x 109/L | 41 | Mean 10.7 ± SD 5.1* | Not reported | Not reported | ||||
| Rebulla 1997 | < 10 x 109/L | 135 | Mean 9.57 ± SD 5.18 | MD 0.50, 95% CI ‐0.70 to 1.70* |
Not reported | Not reported | Not reported | Not reported |
| < 20 x 109/L | 120 | Mean 9.07 ± SD 4.58 | Not reported | Not reported | ||||
*unpublished data provided by the author. The paper provided medians and ranges median 11 (8 to 14) for the standard‐trigger arm and median 10 (6 to 14) for the higher‐trigger arm (P = 0.41).
CI = confidence interval
MD = mean difference
SD = standard deviation
1.10. Analysis.
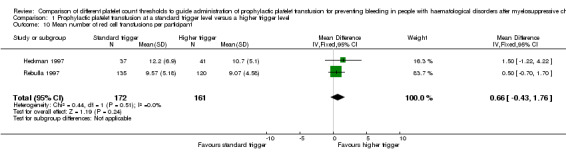
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 10 Mean number of red cell transfusions per participant.
Platelet transfusion interval within 30 days from the start of the study
None of the studies reported on the platelet transfusion interval.
Proportion of participants requiring additional interventions to stop bleeding (surgical, medical e.g. tranexamic acid, other blood products e.g. fresh frozen plasma (FFP), cryoprecipitate)
None of the studies reported on additional interventions to stop bleeding.
Overall survival within 30, 90, and 180 days from the start of the study
All three studies reported all‐cause survival. Only one of these studies reported overall survival within 30, 90 or 180 days, and reported actuarial survival up to 49 days after admission (Rebulla 1997). This was not significantly different between the two groups (P = 0.31).
Proportion of participants achieving complete remission within 30 days and 90 days from the start of the study
Two of the studies reported the number of participants who had achieved a complete remission (Heckman 1997; Rebulla 1997). A meta‐analysis of this data showed no evidence of a difference between the two arms (333 participants; RR 0.92, 95% CI 0.78 to 1.09) (Analysis 1.11).
1.11. Analysis.
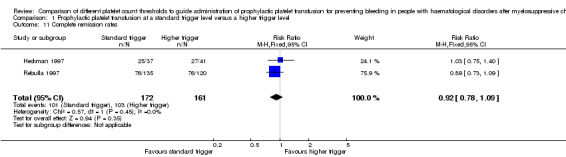
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 11 Complete remission rates.
Total time in hospital within 30 days from the start of the study
All of the studies reported the length of time that participants were in hospital. As these were all reported as medians with ranges or interquartile ranges (Table 6), we could not perform a meta‐analysis. Two of the studies reported no statistically significant difference in hospital stay between the arms of the study (Diedrich 2005; Heckman 1997), whereas the third study did not report any P values (Rebulla 1997).
5. Duration of hospital stay.
| Study | Intervention (transfusion threshold) | Number of participants in each arm | Number of days in hospital (median) | P value |
| Diedrich 2005 | < 10 x 109/L | 79 | 23 Range 9 to 89 |
Not significant |
| < 30 x 109/L | 87 | 23 Range 14 to 140 |
||
| Heckman 1997 | ≤ 10 x 109/L | 37 | 38 IQR 30 to 42 |
0.25* |
| ≤ 20 x 109/L | 41 | 32 IQR 27 to 45 |
||
| Rebulla 1997 | < 10 x 109/L | 135 | 29 Range 3 to 64 |
Not reported |
| < 20 x 109/L | 120 | 28 Range 4 to 54 |
*unpublished data provided by the author.
IQR = interquartile range
Adverse effects of treatments within 30 days from the start of the study
All of the studies reported at least one adverse event of platelet transfusions.
Transfusion reactions
Only Heckman 1997 reported on transfusion reactions secondary to platelet transfusions, and there was insufficient evidence to determine if there was a difference in the number of transfusion reactions between the two arms of the study (RR 0.07, 95% CI 0.00 to 1.09) (Analysis 1.12).
1.12. Analysis.
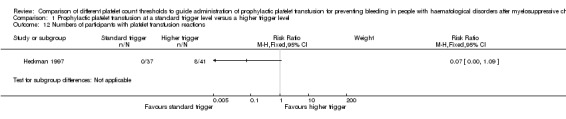
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 12 Numbers of participants with platelet transfusion reactions.
Thromboembolic disease
Only Rebulla 1997 reported deaths due to thromboembolic disease. There was one death in each arm of the study (Analysis 1.13).
1.13. Analysis.
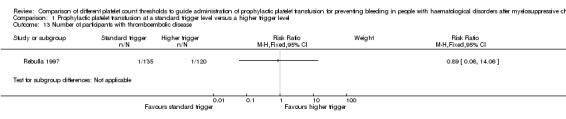
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 13 Number of participants with thromboembolic disease.
Transfusion‐transmitted infection
None of the studies reported on transfusion‐transmitted infection.
Development of platelet antibodies
Only Diedrich 2005 reported on the development of human leukocyte antigen (HLA) antibodies. There was no difference shown between the two arms of the study (RR 1.10, 95% CI 0.07 to 17.31) (Analysis 1.14).
1.14. Analysis.
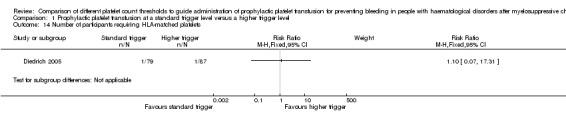
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 14 Number of participants requiring HLA‐matched platelets.
Development of platelet refractoriness
Two of the studies reported on the development of platelet refractoriness (Diedrich 2005; Heckman 1997). A meta‐analysis involving 244 participants showed no difference between the different transfusion trigger levels (RR 0.66, 95% CI 0.16 to 2.67) (Analysis 1.15).
1.15. Analysis.
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 15 Number of participants with platelet refractoriness.
Quality of life (as defined by the individual studies)
None of the studies reported quality of life.
Prespecified subgroup analyses
Presence of fever
Two of the studies commented on an association between fever and bleeding risk (Heckman 1997; Rebulla 1997). However, neither of these studies reported bleeding per treatment arm for participants with or without fever.
Underlying disease
One study commented on status of underlying disease and bleeding risk (Heckman 1997).
The number of participants with at least one clinically significant bleeding episode
In Heckman 1997, the authors performed a multivariate analysis that included age (< 60 years versus ≥ 60 years), disease status (newly diagnosed versus relapsed leukaemia), and arm of the study, and there was no significant difference in the proportion of participants who bled between the standard and higher transfusion trigger levels.
Type of treatment
None of the studies reported this because in each study only one type of treatment was given (chemotherapy or allogenic stem cell transplant).
Age of participant
One study commented on age of participant and bleeding risk (Heckman 1997).
The number of participants with at least one clinically significant bleeding episode
In Heckman 1997, the authors performed a multivariate analysis that included age (< 60 years versus ≥ 60 years), disease status (newly diagnosed versus relapsed leukaemia), and arm of the study, and there was no significant difference in the proportion of participants who bled between the standard and higher transfusion trigger levels.
Platelet component dose
Two of the three included studies used a platelet component dose similar to the intermediate dose used by Slichter 2010 (2.2 x 1011/m2 ± 25%) (Diedrich 2005; Heckman 1997), and one study used a dose between the intermediate and low dose used by Slichter 2010 (1.1 x 1011/m2 ± 25%) (Rebulla 1997). Assuming a body surface area of 1.79 m2 (Sacco 2010), an intermediate platelet component dose equates to 3.9 x 1011 ± 1.0 x 1011, and a low platelet component dose equates to 2.0 x 1011 ± 0.5 x 1011. Only one analysis that included more than one study was affected by removing the data from (Rebulla 1997); this was the number of participants with a significant bleeding event. If only the two higher‐dose studies were included in the analysis, there was a difference between the standard and higher transfusion triggers (RR 1.71, 95% CI 1.04 to 2.82) (Analysis 1.16). However, there was no evidence of a difference between the two platelet component dose subgroups in this analysis (test for subgroup differences: Chi2 = 1.73, df = 1 (P = 0.19), I2 = 42.1%), and therefore only the overall result that showed no evidence of a difference should be considered.
1.16. Analysis.
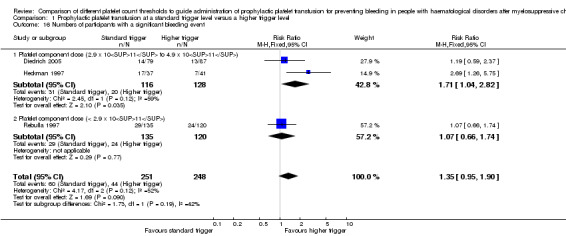
Comparison 1 Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level, Outcome 16 Numbers of participants with a significant bleeding event.
Discussion
Summary of main results
This Cochrane systematic review intended to answer the question, which threshold should be used to trigger the transfusion of prophylactic platelets in participants with haematological disorders undergoing myelosuppressive chemotherapy or stem cell transplantation ? Only one of the four planned comparisons could be performed. No studies compared:
a lower platelet count threshold (5 x 109/L) versus a standard platelet transfusion threshold (10 x 109/L);
different platelet count thresholds (5 x 109/L, 20 x 109/L, 30 x 109/L, or 50 x 109/L) that did not include a comparison against the standard platelet transfusion threshold (10 x 109/L);
alternative thresholds to guide prophylactic platelet transfusions (e.g. platelet mass, immature platelet fraction, absolute immature platelet number).
Three RCTs met our inclusion criteria for this review, all of which had data available and compared a standard platelet transfusion threshold (10 x 109/L) versus a higher platelet count threshold (20 x 109/L, 30 x 109/L, or 50 x 109/L).
These trials were carried out from 1991 to 2001 and enrolled 520 participants from fairly comparable patient populations.
The findings of the review led to the following main conclusions:
Overall, a standard transfusion trigger of 10 x 109/L appears to be as effective as a higher transfusion trigger of 20 x 109/L or 30 x 109/L at preventing clinically significant bleeding. This included no evidence of a difference in the:
number of participants with a clinically significant bleeding event (WHO Grade 2 or above);
number of days with clinically significant bleeding (adjusted for repeated events);
number of participants with severe or life‐threatening bleeding;
time to first clinically significant bleeding episode.
This effect was seen irrespective of the participant's age or underlying disease stage. However, all of this evidence was of low quality, due to risk of bias within the included studies and imprecision of the estimate due to the small total numbers of participants, events, or both.
There was a reduction observed in the number of platelet transfusions required using a threshold of 10 x 109/L.
There was no evidence of a difference in all‐cause mortality.
None of the studies reported quality of life.
There were no differences between the groups with regards to mortality due to bleeding or infection, red cell transfusion requirements, survival, remission rates, hospital stay, or adverse events.
Overall completeness and applicability of evidence
This review provides the most up‐to‐date assessment of the effectiveness and safety of a a standard platelet transfusion threshold (10 x 109/L) versus a higher platelet count threshold (20 x 109/L, 30 x 109/L, or 50 x 109/L) to guide administration of prophylactic platelet transfusions.
The effectiveness and safety of the three other planned comparisons could not be evaluated because no study assessed these comparisons. These planned comparisons were:
a lower platelet count threshold (5 x 109/L) versus standard platelet transfusion threshold (10 x 109/L);
different platelet count thresholds (5 x 109/L, 20 x 109/L, 30 x 109/L, or 50 x 109/L) that did not include a comparison against the standard platelet transfusion threshold (10 x 109/L);
alternative thresholds to guide prophylactic platelet transfusions (e.g. platelet mass, immature platelet fraction, absolute immature platelet number).
(See How the intervention might work for further information on why these planned comparisons were clinically relevant.)
This updated review identified no new studies and no ongoing studies. It is unclear why no future studies are planned; it may be because of the large number of participants required within a study to demonstrate a statistically significant difference (Zisk 2014).
There was no evidence that people with haematological disorders receiving myelosuppressive chemotherapy or HSCT had an increase in clinically significant bleeding events with a standard platelet count threshold compared to a higher platelet count threshold.
The results of this meta‐analysis should not be interpreted without considering the impact of the following factors:
The recording of bleeding is subjective, and all three included studies used different grading systems to measure the severity of bleeding (Table 3).
No difference was demonstrated in the number of participants with clinically significant bleeding, but the 95% confidence interval (0.95 to 1.9) demonstrates that a clinically important difference in the proportion of participants with bleeding could have been missed. When combined, the studies were not adequately powered to detect a difference. In Rebulla 1997, which included 255 participants, the power calculations were based on the assumption that the rate of WHO Grade 2 or above bleeding was 30%, but the actual rate in this study was 20%. If we assume the rate of bleeding was similar in all three studies, to detect a 50% increase in the rate of bleeding (i.e. from 20% to 30%) with 80% power would require 293 participants per arm of the study (586 in total), and to detect a 25% increase in the rate of bleeding (i.e. from 20% to 25%) with 80% power would require 1098 participants per arm of the study (2196 in total). As there were only 499 participants within all three studies, the meta‐analysis would not be sufficiently powered to detect a 50% increase in the rate of bleeding in the restrictive transfusion arm.
There were important differences between the studies that might affect the degree of confidence that can be placed on the assertion of equivalence between higher (20 or 30 x 109/L) and standard (10 x 109/L) platelet count thresholds for prophylactic platelet transfusions. The treatment protocols for administration of platelets varied, particularly the circumstances for which platelet transfusions could be given. In Rebulla 1997, platelets could be given to participants in the 10 x 109/L threshold arm if the platelet count was in the range of 10 to 20 x 109/L and the participant's temperature was above 38°C. This meant that 22.6% of platelet transfusions were given above the threshold of 10 x 109/L. In Diedrich 2005 and Heckman 1997, there were no changes in the transfusion threshold in the presence of fever.
Not all endpoints from all the studies could be incorporated into a meta‐analysis due to differences in the ways the studies had reported the outcomes.
Some of the planned outcomes were not reported by any of the studies.
In all studies, the number of participants that were lost to follow‐up was quite low, and therefore there were minimal implications of missing data outcomes.
Quality of the evidence
All studies were RCTs, however they were all prone to bias and had threats to validity. The ability to assess the risk of bias was limited by most of the studies not reporting study methodology in adequate detail. For example, only one of the three studies reported allocation concealment as adequate (Rebulla 1997), and in all three studies blinding of participants was unknown.
None of the studies blinded medical staff caring for the participants to their patient's study allocation, and two of the three studies did not blind outcome assessors to the participants' study allocations (Heckman 1997; Rebulla 1997). This is likely to reflect the inherent difficulties with blinding platelet transfusion trials because medical staff caring for participants cannot be blinded to their patients' blood results.
We assessed the GRADE quality of evidence as low for:
number of participants with at least one clinically significant bleeding event up to 30 days from study entry;
number of participants with WHO Grade 3 or 4 bleeding up to 30 days from study entry;
time to first clinically significant bleeding event;
mortality from all causes up to 30 days from study entry;
number of platelet transfusions per participant.
The quality of the evidence was low due to risk of bias within the included studies and imprecision of the estimate due to the small total numbers of participants, events, or both.
We did not perform a GRADE assessment of quality of the evidence for quality of life because no study reported this outcome, or for number of days with bleeding, as we relied on the study authors' own analysis.
Potential biases in the review process
There were no obvious biases within the review process. We conducted a wide search, which included ongoing trial databases and contact with researchers in the field; we carefully assessed the relevance of each paper identified; and we made no restrictions for the language in which the paper was originally published or its publication status. We performed all screening and data extractions in duplicate. We prespecified all outcomes and subgroups prior to analysis. The numbers of included studies were insufficient for us to combine to complete a funnel plot in order to examine the risk of publication bias.
Agreements and disagreements with other studies or reviews
One platelet transfusion review was recently published in this area (Kumar 2014). Kumar 2014 performed a systematic review of the use of platelet transfusions in common clinical settings, including the comparison of prophylactic versus therapeutic platelet transfusions. Their review identified the same three studies included in this review (Diedrich 2005; Heckman 1997; Rebulla 1997), as well as including the data from Zumberg 2002. We excluded the data from Zumberg 2002 from this review because fewer than 80% of participants had a haematological malignancy, and no subgroup data were available. The Zumberg 2002 study was at high risk of bias due to the significant number of platelet transfusions (31.9%) given above the level of 10 x 109/L.
The Kumar 2014 review only included the outcome measures of all‐cause mortality, mortality due to bleeding, bleeding ("major" or "significant" bleeding as defined in each study), and number of platelet transfusions. They found no difference in significant bleeding between a standard and higher threshold and a significant decrease in the number of platelet transfusions. This was similar to the finding of our review.
The Kumar 2014 review did not perform a detailed assessment of the risk of bias of the included studies, nor did it consider reasons for heterogeneity between the included studies. Our review is more comprehensive and includes data on different bleeding outcome measures, adverse effects of transfusion, and unpublished study data provided by the authors. We have performed a detailed quality assessment of all identified studies and highlighted their weaknesses and shortcomings.
Authors' conclusions
Implications for practice.
The evidence from this review does not clearly show equivalence of a threshold of 10 x 109/L and 20 x 109/L or 30 x 109/L due to the imprecision of the estimates for the outcomes measured within this review (number of participants with at least one clinically significant bleeding event up to 30 days from study entry; number of participants with WHO Grade 3 or 4 bleeding up to 30 days from study entry; time to first clinically significant bleeding event; mortality from all causes up to 30 days from study entry; number of platelet transfusions per participant). However, without further evidence it is reasonable to continue with the current practice of a platelet transfusion threshold of 10 x 109/L in the absence of other risk factors for bleeding. This practice reduces platelet utilisation and donor exposure.
The effectiveness and safety of the three other planned comparisons cannot be commented on because no study assessed these comparisons. These planned comparisons were: a lower platelet count threshold (5 x 109/L) versus standard platelet transfusion threshold (10 x 109/L); different platelet count thresholds (5 x 109/L, 20 x 109/L, 30 x 109/L, or 50 x 109/L) that did not include a comparison against the standard platelet transfusion threshold (10 x 109/L); alternative thresholds to guide prophylactic platelet transfusions (for example platelet mass, immature platelet fraction, absolute immature platelet number).
Implications for research.
Conclusions on the non‐inferiority of a platelet count threshold of 10 x 109/L compared to 20 x 109/L or 30 x 109/L have been based on underpowered studies leading to imprecise estimates for the outcomes within this review. In the Rebulla 1997 study (255 participants), the power calculations were based on the assumption that the rate of WHO Grade 2 or above bleeding was 30%, but the actual rate in this study was 20%. To detect a 50% increase in the rate of bleeding (that is from 20% to 30%) with 90% power would require 392 participants per arm of the study, and to detect a 25% increase in the rate of bleeding (that is from 20% to 25%) with 80% power would require 1098 participants per arm of the study. The combined results from all three studies would not be sufficiently powered to detect a 50% increase in the rate of bleeding in the standard platelet transfusion threshold (10 x 109/L) arm, if we assumed the rate of bleeding was 20% in all three studies.
No RCTs have compared a lower platelet count threshold (5 x 109/L) versus standard platelet transfusion threshold (10 x 109/L); different platelet count thresholds (5 x 109/L, 20 x 109/L, 30 x 109/L, or 50 x 109/L) that did not include a comparison against the standard platelet transfusion threshold (10 x 109/L); or alternative thresholds to guide prophylactic platelet transfusions (for example platelet mass, immature platelet fraction, absolute immature platelet number) in people with haematological malignancies.
Additional evidence is required from new RCTs to determine the most appropriate platelet transfusion threshold to guide prophylactic platelet transfusions.
Assessment of bleeding in future trials
One of the difficulties within this review was the variability between studies in assessing and grading bleeding. The WHO classification of bleeding, although widely used, has never been validated, and therefore the assumption that all Grade 2 bleeding is clinically significant has been brought into question. For future studies, an international consensus on assessing and grading bleeding would greatly enhance the ability to compare platelet transfusion trials. This would need to be validated and to take into account the impact that bleeding has upon the patient from both a medical perspective and with regard to quality of life.
It is acknowledged that blinding in platelet transfusion trials is difficult. However, whenever possible, the bleeding assessor should be blinded to the intervention.
What's new
| Date | Event | Description |
|---|---|---|
| 23 July 2015 | New search has been performed | Updated search, no new studies identified. |
| 6 March 2014 | New citation required but conclusions have not changed | The previous review, Estcourt 2012a, has now been split into four separate reviews. Protocols have been published for these four separate reviews (Estcourt 2014a; Estcourt 2014b; Estcourt 2014c; Estcourt 2014d). Two new outcomes have been added to the protocol (platelet transfusion interval, quality of life) (Estcourt 2014c). The primary and secondary outcomes have been reported over time‐frames prespecified within the protocol (Estcourt 2014c). The platelet threshold comparisons have been prespecified. |
Notes
The previous review, Estcourt 2012a, has now been split into four separate reviews.
Part of the methods section of this review is based on a standard template established by the Haematological Malignancies Group.
Acknowledgements
We thank the editorial base of the Cochrane Haematological Malignancies Review Group.
We thank the National Institute of Health Research (NIHR). This review is part of a series of reviews that have been funded by the NIHR Cochrane Programme Grant ‐ Safe and Appropriate Use of Blood Components. This research was also supported by the National Institute for Health Research (NIHR) Oxford Biomedical Research Centre Programme. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.
We thank the study authors who provided unpublished data or who kindly searched for data but they were no longer available: B Diedrich, K Heckman, P Rebulla, and M Zumberg.
We thank the authors of the previous reviews: Estcourt 2012a: A Tinmouth; and Stanworth 2004: S Brunskill, N Heddle, C Hyde, and P Rebulla.
Appendices
Appendix 1. CENTRAL (Cochrane Library) 2015 search strategy
#1 MeSH descriptor: [Blood Platelets] explode all trees #2 (platelet* or thrombocyte*):ti #3 #1 or #2 #4 MeSH descriptor: [Blood Transfusion] explode all trees #5 transfus*:ti #6 #4 or #5 #7 #3 and #6 #8 MeSH descriptor: [Platelet Transfusion] explode all trees #9 MeSH descriptor: [Plateletpheresis] explode all trees #10 ((platelet* or thrombocyte*) near/5 (prophyla* or transfus* or infus* or administ* or requir* or need* or product or products or component* or concentrate* or apheres* or pooled or single donor or random donor)) #11 thrombocytopheres* or plateletpheres* #12 ((platelet* or thrombocyte*) near/5 (protocol* or trigger* or threshold* or schedul* or dose* or dosing or usage or utilisation or utilization)) #13 #7 or #8 or #9 or #10 or #11 or #12 #14 MeSH descriptor: [Hematologic Neoplasms] explode all trees #15 MeSH descriptor: [Leukemia] explode all trees #16 MeSH descriptor: [Lymphoma] explode all trees #17 MeSH descriptor: [Multiple Myeloma] explode all trees #18 MeSH descriptor: [Anemia, Aplastic] explode all trees #19 MeSH descriptor: [Bone Marrow Diseases] explode all trees #20 MeSH descriptor: [Thrombocytopenia] explode all trees #21 (thrombocytope* or leukemi* or leukaemi* or lymphoma* or aplastic anemia or aplastic anaemia or myelodysplas* or myeloproliferat* or multiple myeloma or plasma cell myeloma or thrombocythemi* or thrombocythaemi* or polycythemi* or polycythaemi* or myelofibros* or AML or CLL or CML or Hodgkin*) #22 ((haematolog* or hematolog* or blood or red cell* or white cell* or lymph* or marrow or platelet*) near/3 (malignan* or oncolog* or cancer* or neoplasm*)) #23 MeSH descriptor: [Antineoplastic Agents] explode all trees #24 MeSH descriptor: [Stem Cell Transplantation] explode all trees #25 MeSH descriptor: [Bone Marrow Transplantation] this term only #26 MeSH descriptor: [Radiotherapy] explode all trees #27 (chemotherap* or radiotherap* or chemoradiotherap* or chemo‐radiotherap* or stem cell* or bone marrow transplant*) #28 ((haematolog* or hematolog* or hemato‐oncolog* or haemato‐oncolog*) near/2 patients) #29 (malignan* or oncolog* or cancer*):ti #30 #14 or #15 or #16 or #17 or #18 or #19 or #20 or #21 or #22 or #23 or #24 or #25 or #26 or #27 or #28 or #29 #31 #13 and #30
Appendix 2. MEDLINE (Ovid) search strategy (Nov 2011‐2015)
1. BLOOD PLATELETS/ 2. (platelet* or thrombocyte*).ti. 3. 1 or 2 4. exp BLOOD TRANSFUSION/ 5. transfus*.ti. 6. 4 or 5 7. 3 and 6 8. PLATELET TRANSFUSION/ 9. PLATELETPHERESIS/ 10. ((platelet* or thrombocyte*) adj5 (prophyla* or transfus* or infus* or administ* or requir* or need* or product* or component* or concentrate* or apheres* or pooled or single donor or random donor)).tw. 11. (thrombocytopheres* or plateletpheres*).tw. 12. ((platelet* or thrombocyte*) adj5 (protocol* or trigger* or threshold* or schedul* or dose* or dosing or usage or utili?ation)).tw. 13. or/7‐12 14. exp Hematologic Neoplasms/ 15. exp Leukemia/ or exp Lymphoma/ 16. exp Multiple Myeloma/ 17. exp Anemia, Aplastic/ 18. exp Bone Marrow Diseases/ 19. exp Thrombocytopenia/ 20. (thrombocytopeni* or thrombocytopaeni* or leukemia or leukaemia or lymphoma* or aplastic anemia or aplastic anaemia or myelodysplas* or myeloproliferat* or multiple myeloma or plasma cell myeloma or thrombocythemi* or thrombocythaemi* or polycythemi* or polycythaemi* or myelofibros* or AML or CLL or CML or Hodgkin*).tw. 21. ((haematolog* or hematolog* or blood or red cell* or white cell* or lymph* or marrow or platelet*) adj3 (malignan* or oncolog* or cancer* or neoplasm*)).tw. 22. exp Antineoplastic Agents/ 23. exp Stem Cell Transplantation/ or Bone Marrow Transplantation/ or exp Radiotherapy/ 24. (chemotherap* or radiotherap* or chemoradiotherap* or chemo‐radiotherap* or stem cell* or bone marrow transplant*).tw. 25. ((haematolog* or hematolog* or haemato‐oncolog* or hemato‐oncolog*) adj2 patients).tw. 26. (malignan* or oncolog* or cancer*).ti. 27. or/14‐26 28. 13 and 27
Appendix 3. PubMed search strategy (epublications only)
#1 ((platelet* OR thrombocyte*) AND (prophyla* OR transfus* OR infus* OR administ* OR requir* OR need* OR product OR products OR component* OR concentrate* OR apheres* OR pooled OR single donor OR random donor OR protocol* OR trigger* OR threshold* OR schedul* OR dose OR doses OR dosing OR usage OR utilisation OR utilization)) #2 thrombocytopheres* OR plateletpheres* #3 #1 OR #2 #4 (thrombocytop* OR leukemi* OR leukaemi* OR lymphoma* OR aplastic anemia OR aplastic anaemia OR myelodysplas* OR myeloproliferat* OR multiple myeloma OR plasma cell myeloma OR thrombocythemi* OR thrombocythaemi* OR polycythemi* OR polycythaemi* OR myelofibros* OR Hodgkin*) #5 ((haematolog* OR hematolog* OR blood OR red cell* OR white cell* OR lymphom* OR marrow OR platelet*) AND (malignan* OR oncolog* OR cancer OR cancers OR neoplasm*)) #6 #4 OR #5 #7 #3 AND #6 #8 (random* OR blind* OR control group* OR placebo OR controlled trial OR controlled study OR trials OR systematic review OR meta‐analysis OR metaanalysis OR literature OR medline OR cochrane OR embase) AND (publisher[sb] NOT pubstatusnihms) #9 #7 AND #8
Appendix 4. EMBASE (Ovid) search strategy (Nov 2011‐2015)
1. Thrombocyte/ 2. (platelet* or thrombocyte*).ti. 3. 1 or 2 4. Blood Transfusion/ 5. transfus*.ti. 6. 4 or 5 7. 3 and 6 8. Thrombocyte Transfusion/ 9. Thrombocytopheresis/ 10. ((platelet* or thrombocyte*) adj5 (prophyla* or transfus* or infus* or administ* or requir* or need* or product* or component* or concentrate* or apheres* or pooled or single donor or random donor)).tw. 11. (thrombocytopheres* or plateletpheres*).tw. 12. ((platelet* or thrombocyte*) adj5 (protocol* or trigger* or threshold* or schedul* or dose* or dosing or usage or utili?ation)).tw. 13. or/7‐12 14. Hematologic Malignancy/ 15. Lymphoma/ 16. NonHodgkin Lymphoma/ 17. Hodgkin Disease/ 18. exp Myeloproliferative Disorder/ 19. exp Aplastic Anemia/ 20. exp Thrombocytopenia/ 21. (thrombocytopeni* or thrombocytopaeni* or leukemia or leukaemia or lymphoma* or aplastic anemia or aplastic anaemia or myelodysplas* or myeloproliferat* or multiple myeloma or plasma cell myeloma or thrombocythemi* or thrombocythaemi* or polycythemi* or polycythaemi* or myelofibros* or AML or CLL or CML or Hodgkin*).tw. 22. ((haematolog* or hematolog* or blood or red cell* or white cell* or lymph* or marrow or platelet*) adj3 (malignan* or oncolog* or cancer* or neoplasm*)).tw. 23. exp Chemotherapy/ 24. exp Stem Cell Transplantation/ 25. exp Bone Marrow Transplantation/ 26. exp Radiotherapy/ 27. (chemotherap* or radiotherap* or chemoradiotherap* or chemo‐radiotherap* or stem cell* or bone marrow transplant* or rituximab).tw. 28. ((haematolog* or hematolog*) adj2 patients).tw. 29. (malignan* or oncolog* or cancer*).ti. 30. or/14‐29 31. 13 and 30
Appendix 5. CINAHL (EBSCOhost) search strategy (Nov 2011‐2015)
S1 (MH "Blood Platelets") S2 TI (platelet* or thrombocyte*) S3 S1 OR S2 S4 (MH "BLOOD TRANSFUSION+") S5 TI transfus* S6 S4 or S5 S7 S3 and S6 S8 (MH "PLATELET TRANSFUSION") S9 ( MH PLATELETPHERESIS) S10 ((platelet* or thrombocyte*) N5 (prophyla* or transfus* or infus* or administ* or requir* or need* or product* or component* or concentrate* or apheres* or pooled or single donor or random donor)) S11 (thrombocytopheres* or plateletpheres*) S12 ((platelet* or thrombocyte*) N5 (protocol* or trigger* or threshold* or schedul* or dose* or dosing or usage or utili?ation)) S13 S8 OR S9 OR S10 OR S11 OR S12 S14 (MH "Hematologic Neoplasms+") S15 (MH Leukemia+) S16 (MH Lymphoma+) S17 (MH "Multiple Myeloma+") S18 (MH "Anemia, Aplastic+") S19 (MH "Bone Marrow Diseases+") S20 (MH Thrombocytopenia+) S21 (thrombocytopeni* or thrombocytopaeni* or leukemia or leukaemia or lymphoma* or aplastic anemia or aplastic anaemia or myelodysplas* or myeloproliferat* or multiple myeloma or plasma cell myeloma or thrombocythemi* or thrombocythaemi* or polycythemi* or polycythaemi* or myelofibros* or AML or CLL or CML or Hodgkin*) S22 ((haematolog* or hematolog* or blood or red cell* or white cell* or lymph* or marrow or platelet*) N3 (malignan* or oncolog* or cancer* or neoplasm*)) S23 (MH "Antineoplastic Agents+") S24 (MH "Hematopoietic Stem Cell Transplantation") S25 (MH "Bone Marrow Transplantation") S26 (MH Radiotherapy+) S27 (chemotherap* or radiotherap* or chemoradiotherap* or chemo‐radiotherap* or stem cell* or bone marrow transplant*) S28 ((haematolog* or hematolog* or haemato‐oncolog* or hemato‐oncolog*) N2 patients) S29 TI (malignan* or oncolog* or cancer*) S30 S14 OR S15 OR S16 OR S17 OR S18 OR S19 OR S20 OR S21 OR S22 OR S23 OR S24 OR S25 OR S26 OR S27 OR S28 OR S29 S31 S13 and S30
Appendix 6. TRANSFUSION EVIDENCE LIBRARY search strategy (2015)
#1 ((platelet* OR thrombocyte*) AND (prophyla* OR transfus* OR infus* OR administ* OR requir* OR need* OR product OR products OR component* OR concentrate* OR apheres* OR pooled OR single donor OR random donor OR protocol* OR trigger* OR threshold* OR schedul* OR dose OR doses OR dosing OR usage OR utilisation OR utilization)) #2 thrombocytopheres* OR plateletpheres* #3 #1 OR #2 #4 (thrombocytop* OR leukemi* OR leukaemi* OR lymphoma* OR aplastic anemia OR aplastic anaemia OR myelodysplas* OR myeloproliferat* OR multiple myeloma OR plasma cell myeloma OR thrombocythemi* OR thrombocythaemi* OR polycythemi* OR polycythaemi* OR myelofibros* OR Hodgkin*) #5 ((haematolog* OR hematolog* OR blood OR red cell* OR white cell* OR lymphom* OR marrow OR platelet*) AND (malignan* OR oncolog* OR cancer OR cancers OR neoplasm*)) #6 #4 OR #5 #7 #3 AND #6
Appendix 7. Web of Science (CPCI‐S) search strategy (2015)
((platelet* AND (prophyla* OR transfus* OR products OR component* OR concentrate* OR apheres* OR pooled OR single donor OR random donor OR protocol* OR trigger* OR threshold*)) AND (thrombocytop* OR leukemi* OR leukaemi* OR lymphoma* OR aplastic OR myelodysplas* OR myeloproliferat* OR myeloma OR thrombocythemi* OR thrombocythaemi* OR polycythemi* OR polycythaemi* OR myelofibros* OR hodgkin* OR haematological OR hematological)) [in Title] AND (randomized OR randomised OR randomly) [in Title]
Appendix 8. LILACS search strategy (2015)
((platelet* AND (prophyla* OR transfus* OR products OR component* OR concentrate* OR apheres* OR pooled OR single donor OR random donor OR protocol* OR trigger* OR threshold*)) AND (thrombocytop* OR leukemi* OR leukaemi* OR lymphoma* OR aplastic OR myelodysplas* OR myeloproliferat* OR myeloma OR thrombocythemi* OR thrombocythaemi* OR polycythemi* OR polycythaemi* OR myelofibros* OR hodgkin* OR haematological OR hematological)) AND db:("LILACS") AND type_of_study:("clinical_trials" OR "systematic_reviews")
Appendix 9. INDMED search strategy (2015)
(platelet OR platelets OR thrombocyte$ OR thrombocytopheres$ OR plateletpheres$) AND (thrombocytop$ OR leukemi$ OR leukaemi$ OR lymphoma$ OR aplastic OR myelodysplas$ OR myeloproliferat$ OR myeloma OR thrombocythemi$ OR thrombocythaemi$ OR polycyth$ OR myelofibros$ OR Hodgkin$ OR haematological OR hematological OR hematopoietic OR haematopoietic) AND (random$ OR blind$ OR trial$ OR control$)
Appendix 10. KoreaMed & PakMediNet search strategy (2015)
platelet*[ALL] AND "Randomized Controlled Trial" [PT] thrombocyt*[ALL] AND "Randomized Controlled Trial" [PT]
Appendix 11. ClinicalTrials.gov & ICTRP search strategy (2015)
Search Terms/Title: randomized OR randomised Conditions: hematological neoplasm OR hematological malignancies OR leukemia OR lymphoma OR thrombocytopenia OR multiple myeloma OR aplastic anemia OR thrombocythemia OR polycythemia OR myelofibrosis OR hodgkins disease Intervention: platelets OR platelet transfusion
Appendix 12. ISRCTN & EU Clinical Trials Register search strategy (2015)
(hematological OR haematological OR leukemi* OR leukaemi* OR lymphoma OR thrombocytopeni* OR myeloma OR aplastic OR thrombocythemia OR polycythemia OR myelofibrosis OR hodgkin*) AND platelet* transfus* AND random*
Appendix 13. Hong Kong Clinical Trials Register search strategy (2015)
Disease Group: Blood and blood‐forming organs Title: randomized OR randomised
Appendix 14. Previous searches: original (Jan 2002) & update (Nov 2011) search strategies
CENTRAL search strategy (Issue 4, 2011) #1 MeSH descriptor Blood Platelets explode all trees #2 platelet* or thrombocyte* #3 (#1 OR #2) #4 MeSH descriptor Blood Transfusion explode all trees #5 transfus* #6 (#4 OR #5) #7 (#3 AND #6) #8 MeSH descriptor Platelet Transfusion explode all trees #9 (platelet* or thrombocyte*) NEAR/5 (transfus* or infus* or administ* or requir*) #10 (#7 OR #8 OR #9) #11 prophylactic* or prophylax* or prevent* #12 (#10 AND #11)
MEDLINE (Ovid) search strategy (Jan 2002 ‐ Nov 2011)
1. BLOOD PLATELETS/ 2. (platelet* or thrombocyte*).tw. 3. 1 or 2 4. exp BLOOD TRANSFUSION/ 5. transfus*.tw. 6. 4 or 5 7. 3 and 6 8. PLATELET TRANSFUSION/ 9. ((platelet* or thrombocyte*) adj5 (transfus* or infus* or administ* or requir*)).tw. 10. or/7‐9 11. (prophylactic* or prophylax* or prevent*).tw. 12. 10 and 11
EMBASE (Ovid) search strategy (Jan 2002 ‐ Nov 2011) 1. THROMBOCYTE/ 2. (platelet* or thrombocyte*).tw. 3. 1 or 2 4. exp BLOOD TRANSFUSION/ 5. transfus*.tw. 6. 4 or 5 7. 3 and 6 8. THROMBOCYTE TRANSFUSION/ 9. ((platelet* or thrombocyte*) adj5 (transfus* or infus* or administ* or requir*)).tw. 10. or/7‐9 11. (prophylactic* or prophylax* or prevent*).tw. 12. 10 and 11 CINAHL (NHS Evidence) search strategy (Jan 2002 ‐ Nov 2011) 1. BLOOD PLATELETS/ 2. (platelet* or thrombocyte*).ti,ab 3. 1 or 2 4. exp BLOOD TRANSFUSION/ 5. transfus*.ti,ab 6. 4 or 5 7. 3 and 6 8. PLATELET TRANSFUSION/ 9. ((platelet* adj5 transfus*) or (platelet* adj5 infus*) or (platelet* adj5 administ*) or (platelet* adj5 requir*)).ti,ab 10. ((thrombocyte* adj5 transfus*) or (thrombocyte* adj5 infus*) or (thrombocyte* adj5 administ*) or (thrombocyte* adj5 requir*)).ti,ab 11. 7 or 8 or 9 or 10 12. (prophylactic* or prophylax* or prevent*).ti,ab 13. 11 and 12
Free text search strategy for other databases (Nov 2011) (platelet* OR thrombocyte*) AND (transfus* OR infus* OR administ* OR requir*) AND (prophylactic* OR prophylaxis OR prevent OR prevention OR preventing)
MEDLINE & EMBASE search strategy (Jan 2002) 1. Platelet Transfusion.mh. 2. platelet$ adj10 (substitute$ or transfusion$ or prophyla$).tw. 3. 1 or 2 4. haemorrhage.mh. 5. platelet$.tw. 6. 4 and 5 7. exp Blood Transfusion/ 8. 5 and 7 9. 3 or 6 or 8
Data and analyses
Comparison 1. Prophylactic platelet transfusion at a standard trigger level versus a higher trigger level.
| Outcome or subgroup title | No. of studies | No. of participants | Statistical method | Effect size |
|---|---|---|---|---|
| 1 Numbers of participants with a significant bleeding event | 3 | 499 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.35 [0.95, 1.90] |
| 1.1 Platelet threshold < 10 vs. < 20 | 2 | 333 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.41 [0.95, 2.10] |
| 1.2 Platelet threshold < 10 vs. < 30 | 1 | 166 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.19 [0.59, 2.37] |
| 2 Number of participants with WHO Grade 3 or 4 bleeding | 2 | 421 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.99 [0.52, 1.88] |
| 2.1 Platelet threshold < 10 vs. < 20 | 1 | 255 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.21 [0.58, 2.54] |
| 2.2 Platelet threshold < 10 vs. < 30 | 1 | 166 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.55 [0.14, 2.13] |
| 3 Number of participants with bleeding requiring a red cell transfusion | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 4 Time to first bleeding episode | 1 | Hazard Ratio (Fixed, 95% CI) | Subtotals only | |
| 5 All‐cause mortality | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 6 Mortality due to bleeding | 3 | Risk Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 7 Mortality due to bleeding (all randomised participants) | 3 | Odds Ratio (M‐H, Fixed, 95% CI) | Totals not selected | |
| 8 Mortality due to infection | 1 | Odds Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 9 Mean number of platelet transfusions per participant | 2 | 333 | Mean Difference (IV, Fixed, 95% CI) | ‐2.09 [‐3.20, ‐0.99] |
| 10 Mean number of red cell transfusions per participant | 2 | 333 | Mean Difference (IV, Fixed, 95% CI) | 0.66 [‐0.43, 1.76] |
| 11 Complete remission rates | 2 | 333 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.92 [0.78, 1.09] |
| 12 Numbers of participants with platelet transfusion reactions | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 13 Number of participants with thromboembolic disease | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 14 Number of participants requiring HLA‐matched platelets | 1 | Risk Ratio (M‐H, Fixed, 95% CI) | Subtotals only | |
| 15 Number of participants with platelet refractoriness | 2 | 244 | Risk Ratio (M‐H, Fixed, 95% CI) | 0.66 [0.16, 2.67] |
| 16 Numbers of participants with a significant bleeding event | 3 | 499 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.35 [0.95, 1.90] |
| 16.1 Platelet component dose (2.9 x 1011 to 4.9 x 1011) | 2 | 244 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.71 [1.04, 2.82] |
| 16.2 Platelet component dose (< 2.9 x 1011) | 1 | 255 | Risk Ratio (M‐H, Fixed, 95% CI) | 1.07 [0.66, 1.74] |
Characteristics of studies
Characteristics of included studies [ordered by study ID]
Diedrich 2005.
| Methods | Parallel RCT (enrolled September 1996 to September 2001). Single centre. Sweden | |
| Participants |
Inclusion criteria: People undergoing an allogeneic haematopoietic stem cell transplant. All ages. Exclusion criteria: People with a known bleeding disorder or coagulopathy N = 166 (all included in analysis) Arm 1 N = 79 (acute leukaemia N = 47; chronic leukaemia N = 20; non‐malignant haematological disorder N = 4; other malignancy N = 8) Arm 2 N = 87 (acute leukaemia N = 36; chronic leukaemia N = 24; non‐malignant haematological disorder N = 11; other malignancy N = 16) |
|
| Interventions | Comparison between prophylactic platelets with different transfusion triggers Arm 1 (Low transfusion trigger): If platelet count < 10 x 109/L Arm 2 (High transfusion trigger): If platelet count < 30 x 109/L In both arms prior to an operation or a biopsy, a platelet count > 50 x 109/L was aimed for. Platelet dose (mean ± SD):
Platelet type: pooled random‐donor platelets (buffy coat) 85% of platelet transfusions given; apheresis 15% of platelet transfusions given. All were ABO matched, irradiated, and leucodepleted |
|
| Outcomes |
Primary outcome: Number of platelet transfusions Secondary outcomes:
Average number of days participants on study Not reported |
|
| Bleeding scale | WHO Grade 1: petechiae Grade 2: mild blood loss Grade 3 ‐ 4: gross or debilitating blood loss Definition of significant bleeding: WHO Grade 2 ‐ 4 Definition of life‐threatening bleeding: Not stated |
|
| Bleeding assessment | Daily bleeding assessment by nursing staff if inpatient, twice weekly bleeding assessment by nursing staff if outpatient | |
| Red cell transfusion policy | RBCs were transfused when haemoglobin decreased below 80 g/L | |
| Notes |
Participants randomised: documentation for study started 7 days prior to transplant Follow‐up: until 30 days post‐stem cell transplant Stopping rules: not reported Source(s) of funding: Supported by grants from: The Swedish Cancer Society (0070‐B99‐13XAC); The Children’s Cancer Foundation (2000/067, 02/074); The Swedish Medical Research Council (K2000‐06X‐05971‐20A); The Swedish Foundation for Medical Research; The Swedish Society of Medicine (2000‐02‐0553, 2001‐1299); The Cancer Society in Stockholm; The Tobias Foundation Conflicts‐of‐interest statement: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Participants were randomised after stratification, method of randomisation not stated |
| Allocation concealment (selection bias) | Unclear risk | Participants were randomised after stratification, method of allocation concealment not stated |
| Blinding of participants and personnel (performance bias) Participant | Unclear risk | It was unclear whether participants were blinded to the intervention, this was not reported in the published study |
| Blinding of participants and personnel (performance bias) Physician/Medical Staff | High risk | All platelet units were ordered by a nurse in charge of and responsible for the participant. The nurse was not blinded to the treatment arm for practical reasons |
| Blinding of outcome assessment (detection bias) All outcomes | Low risk | Nurses from the ward, blinded to treatment arm, performed daily (inpatients) or twice weekly (outpatients) assessment and reported this. All platelet units were ordered by a different nurse in charge of and responsible for the participant. He or she was not blinded to the treatment arm for practical reasons. A special research nurse collected all data for the study |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient information to make an assessment |
| Selective reporting (reporting bias) | Unclear risk | No protocol available to assess whether all prespecified outcomes have been reported |
| Other bias | Low risk | The study appears to be free of other sources of bias |
| Protocol Deviation balanced? | Unclear risk | In participants with WHO Grade 2 ‐ 4 bleeding, violations of the protocol occurred in 4/14 participants in Arm 1 and 3/13 participants in Arm 2. The number of transfusions in which a protocol deviation occurred was not reported. Whether there were any protocol deviations in those participants that did not bleed was not reported |
Heckman 1997.
| Methods | Parallel RCT (enrolled April 1991 to November 1995). Single centre. United States | |
| Participants |
Inclusion criteria: Unequivocal diagnosis of acute leukaemia (AML, ALL in relapse, acute undifferentiated leukaemia or MDS transformed to AML). Age > 17 years. Person undergoing initial induction chemotherapy or re‐induction following relapse Exclusion criteria: APL. Inherited clotting disorder. Uncontrolled infection at randomisation. History of a bleeding diathesis. DIC at randomisation into the study. Prior entry into the study. Concomitant malignancy or AIDS diagnosis. History of platelet refractory status N = 82 entered into study; 4 ineligible (2 delayed cytogenetic diagnosis of APL. 2 not assessable, transferred to ITU within 24 hrs of registration with severe infections) Arm 1: N = 37 Arm 2: N = 41 |
|
| Interventions | Comparison between prophylactic platelets with different transfusion triggers
Arm 1 (Low transfusion trigger). If platelet count ≤ 10 x 109/L
Arm 2 (High transfusion trigger). If platelet count ≤ 20 x 109/L Platelets given in both arms if serious or life‐threatening bleeding and for procedures at discretion of physician Platelet dose: 1 apheresis unit (approximately 4 to 4.9 x 1011 of platelets) Platelet type: apheresis. Leucodepleted |
|
| Outcomes | Main or primary outcome not stated Outcomes mentioned:
Number of days participants on study (median): Arm 1: 24 days Arm 2: 24 days |
|
| Bleeding scale | Severity was graded using a standardised toxicity scale (Ajani 1990) Grade 1: petechiae, minimum blood loss, blood transfusion not required Grade 2: blood loss requiring transfusion of 1 to 2 units of blood Grade 3: blood loss requiring transfusion of 3 to 4 units of blood Grade 4: blood loss requiring transfusion of > 4 units of blood Definition of significant bleeding: requirement for therapeutic platelet transfusion (unpublished) Definition of life‐threatening bleeding: not stated |
|
| Bleeding assessment | Bleeding episodes defined as blood loss documented in physician or nursing notes or observed by an investigator | |
| Red cell transfusion policy | Not stated | |
| Notes |
Participants randomised: no definition Follow‐up of participants: until unsupported platelet count > 30 x 109/L for 2 days OR transfer to intensive care for > 2 days OR discharge from hospital OR death Stopping guideline: not reported Source(s) of funding: Iowa Leukemia and Cancer Research Fund; The Dr. Richard O. Emmons Memorial Fund; L. McGilliard‐T. Johannes Memorial Fund; The Mamie C. Hopkins Fund Conflicts‐of‐interest statement: not stated |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Unclear risk | Random allocation "by selecting randomised cards from envelopes". No comment on how cards were randomised Randomisation stratified by 4 groups (new diagnosis < 60 years; new diagnosis = 60 years; relapse < 60 years; relapse = 60 years) |
| Allocation concealment (selection bias) | Unclear risk | Attempt to conceal allocation not described. It was not mentioned whether envelopes were opaque or sealed |
| Blinding of participants and personnel (performance bias) Participant | Unclear risk | It was unclear whether participants were blinded to the intervention, this was not reported in the published study |
| Blinding of participants and personnel (performance bias) Physician/Medical Staff | High risk | Bleeding assessors were not blinded to the intervention (additional data supplied by the author and reported in Estcourt 2013). Bleeding assessors included medical staff (nurses and physicians routinely involved with patient care) |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Bleeding assessors were not blinded to the intervention (additional data supplied by the author and reported in Estcourt 2013). Bleeding assessors were a mixture of medical staff (nurses and physicians routinely involved with patient care) and trained research nurses/research investigators |
| Incomplete outcome data (attrition bias) All outcomes | Unclear risk | Insufficient reporting to allow assessment |
| Selective reporting (reporting bias) | Unclear risk | No study protocol available, and outcomes not clearly stated |
| Other bias | Unclear risk | Insufficient information to assess |
| Protocol Deviation balanced? | High risk | In Arm 1 30/311 transfusions deviated from the protocol, whereas in Arm 2 only 7/457 transfusions deviated from the protocol. This affected 14/37 participants in Arm 1 and 6/41 participants in Arm 2 (P = 0.02) |
Rebulla 1997.
| Methods | Parallel RCT (enrolled from March 1994 to March 1996). Multicentre study (21 centres). Italy | |
| Participants |
Inclusion criteria: People with AML; adolescents and adults (aged 16 to 70 yrs); admitted to hospital for 1st course of induction chemotherapy Exclusion criteria: People diagnosed with promyelocytic leukaemia or secondary AML; people who had received a blood transfusion prior to diagnosis of AML N = 329 people screened for trial. 276 randomised. (37 secondary leukaemia; 10 blood transfusion prior to diagnosis; 4 did not meet age criteria; 2 declined to give consent) Arm 1: N = 144; 9 not included in analysis: 8 alive at discharge (no study records received); 1 death on day 5 (cerebral haemorrhage) (no study records received) Arm 2: N = 132; 12 not included in analysis: 8 alive at discharge (no study records received); 2 died within 24 hours of admission (1 cerebral haemorrhage, 1 cardiac arrest); 2 received non‐myeloablative course of chemotherapy |
|
| Interventions | Comparison between prophylactic platelets with different transfusion triggers
Arm 1: (Low transfusion trigger). If platelet count < 10 x 109/L AND temperature < 38°C If platelet count 10 to 20 x 109/L AND temperature > 38°C OR in presence of major or minor bleeding OR if invasive procedures were necessary Arm 2: (High transfusion trigger). If platelet count < 20 x 109/L Platelet dose: 1 unit of platelet rich plasma or buffy coat concentrate per 10 kg body weight or 1 apheresis concentrate given. Number of platelets per transfusion (apheresis) median 280 x 109 (range 110 to 588), pooled concentrate median 217 x 109 (range 140 to 555) Platelet type: Apheresis platelets given to 50% of participants in Arm 1 and 42% of participants in Arm 2 |
|
| Outcomes |
Primary outcome: Frequency and severity of haemorrhage Secondary outcomes:
All outcomes measured to end of study Number of days participants on study (mean) Arm 1 = 29.7 days Arm 2 = 27.8 days |
|
| Bleeding scale | Severity of haemorrhage marked on an 8
‐point scale
0 = no bleeding
1 = petechiae or mucosal or retinal bleeding
2 = melaena, haematemesis, haematuria, or haemoptysis
3 = any bleeding requiring a red cell transfusion
4 = retinal bleeding accompanied by visual impairment
5 = non‐fatal cerebral bleeding
6 = fatal cerebral bleeding
7 = fatal non‐cerebral bleeding Definition of significant haemorrhage: score > 1 Definition of life‐threatening haemorrhage: not stated |
|
| Bleeding assessment | The physician in charge of the participant collected data on the occurrence and type of bleeding | |
| Red cell transfusion policy | Red cells were given when haemoglobin < 80 g/L | |
| Notes |
Participants randomised at: diagnosis Follow‐up of participants: until platelet count > 100 x 109/L OR discharge from hospital OR occurrence of complete remission OR resistance to chemotherapy OR death Stopping guidelines: The trial was scheduled to be stopped if the rate of outcome events reached statistical significance (P < 0.01 by the Chi2 test) Acetaminophen was used as an antipyretic agent Source(s) of funding: not reported Conflicts‐of‐interest statement: not reported |
|
| Risk of bias | ||
| Bias | Authors' judgement | Support for judgement |
| Random sequence generation (selection bias) | Low risk | Participants underwent randomisation as soon as the diagnosis and other inclusion criteria were communicated by telephone to the central randomisation centre at the GIMEMA secretariat in Rome. A random permutated block design was used in the individual centres |
| Allocation concealment (selection bias) | Low risk | The people who handled randomisation, data management, and statistical analysis were not involved in the treatment of the participants |
| Blinding of participants and personnel (performance bias) Participant | Unclear risk | It was unclear whether participants were blinded to the intervention, this was not reported in the published study |
| Blinding of participants and personnel (performance bias) Physician/Medical Staff | High risk | Medical staff routinely involved in the care of the participant were the bleeding assessors and were not blinded to the intervention (additional data supplied by the author and reported in Estcourt 2013) |
| Blinding of outcome assessment (detection bias) All outcomes | High risk | Bleeding assessors were not blinded to the intervention (additional data supplied by the author and reported in Estcourt 2013) |
| Incomplete outcome data (attrition bias) All outcomes | Low risk | Missing outcome data balanced in numbers across intervention groups, with similar reasons for missing data across groups. 21 of the randomised participants were excluded from analysis (16 no study records received. 2 received non‐myeloablative chemotherapy. 3 died (2 within 24 hours of enrolment into the study); 2 of the three deaths were due to an intracerebral haemorrhage. 9 participants were excluded in the standard‐trigger arm: 8 alive at discharge (no study records received); 1 death on day 5 (cerebral haemorrhage) (no study records received). 12 participants were excluded in the higher‐trigger arm: 8 alive at discharge (no study records received); 2 died within 24 hours of admission (1 cerebral haemorrhage, 1 cardiac arrest); 2 received non‐myeloablative course of chemotherapy |
| Selective reporting (reporting bias) | Unclear risk | Study protocol not available to allow judgement |
| Other bias | Low risk | The study appears to be free of other sources of bias |
| Protocol Deviation balanced? | High risk | Pre‐transfusion platelet count higher than indicated in the protocol in 5.4% of platelet transfusions in Arm 1 and 2% of platelet transfusions in Arm 2 |
ALL = acute lymphocytic leukaemia
AML = acute myeloid leukaemia
APL = acute promyelocytic leukaemia
DIC = disseminated intravascular coagulation
GvHD = graft versus host disease
ITU = intensive treatment unit
MDS = myelodysplastic syndrome
RBC = red blood cell
RCT = randomised controlled trial
SD = standard deviation
Characteristics of excluded studies [ordered by study ID]
| Study | Reason for exclusion |
|---|---|
| Aderka 1986 | A non‐randomised retrospective study |
| Agliastro 2006 | Comparison of apheresis versus buffy coat platelet transfusions ( abstract) |
| Akkök 2007 | Comparison of apheresis versus buffy coat platelet transfusions |
| Anderson 1997 | Comparison of apheresis versus buffy coat ‐derived versus platelet rich plasma ‐derived platelet products |
| Andreu 2009 | Review |
| Andrew 1993 | Wrong patient group ‐ premature infants |
| Arnold 2004 | Comparison of apheresis versus whole blood ‐derived platelet transfusions |
| Arnold 2006 | Wrong patient group ‐ intensive treatment unit |
| Avvisati 2003 | Review |
| Bai 2004 | Wrong patient group ‐ solid tumours |
| Benjamin 2002 | Review |
| Bentley 2000 | Comparison of autologous versus allogeneic platelet transfusions |
| Blajchman 2008 | Review |
| Blumberg 2002 | Comparison of washed versus standard platelet transfusions |
| Blumberg 2004 | Comparison of washed versus standard platelet transfusions |
| Blundell 1996 | Comparison of standard versus pathogen inactivated platelets |
| Buhrkuhl 2010 | Review |
| Callow 2002 | A non‐randomised prospective study with historical control |
| Cameron 2007 | A non‐randomised prospective study |
| Carr 1990 | Comparison of ABO‐matched versus mismatched platelet products |
| Casbard 2004 | Systematic review and wrong patient group |
| Chaoui 2005 | Observational prospective study |
| Chaurasia 2012 | A non‐randomised prospective study |
| Cid 2007 | Systematic review of differing platelet transfusion doses |
| Corash 2001 | Comparison of intercept platelet components versus standard platelet components |
| Couban 2002 | Comparison of plasma reduction and leucodepletion |
| de Wildt‐Eggen 2000 | Comparison of platelet concentrates in plasma versus additive solution |
| Decaudin 2004 | Non‐randomised prospective study |
| Di Pietro 1998 | Comparison of HLA ‐matched versus random ‐donor apheresis platelet components |
| Diedrich 2009 | Comparison of platelet products stored 1 ‐ 5 versus 6 ‐ 7 days |
| Dumont 2011 | Comparison of buffy coat versus platelet rich plasma platelet concentrates |
| Dzik 2004 | Review |
| Eder 2007 | Non‐randomised observational study |
| Elting 2002 | Retrospective analysis ‐ lymphoma and solid tumours |
| Elting 2003 | Non‐randomised retrospective cohort ‐ lymphoma and solid tumours |
| Fanning 1995 | Wrong patient group ‐ gynaecological cancer |
| Follea 2004 | Guideline |
| Friedmann 2002 | A non‐randomised retrospective analysis |
| Gajic 2006 | Wrong patient group ‐ intensive treatment unit |
| Gerday 2009 | Wrong patient group ‐ neonates |
| Gil‐Fernandez 1996 | A non‐randomised retrospective historical control study (different platelet transfusion thresholds) |
| Gmür 1983 | Comparison of single ‐donor versus pooled platelet products |
| Gmür 1991 | A non‐randomised prospective cohort observational study (different platelet transfusion thresholds) |
| Goodnough 2001 | Fewer than 80% of participants diagnosed with a haematological disorder ‐ different platelet doses |
| Goodnough 2002 | Review |
| Goodnough 2005 | Review |
| Goodrich 2008 | Comparison of pathogen inactivated versus standard apheresis platelets |
| Greeno 2007 | A non‐randomised prospective observational study (different platelet transfusion thresholds) |
| Grossman 1980 | Comparison of prophylactic versus therapeutic platelet transfusions |
| Gurkan 2007 | Comparison of apheresis versus pooled platelet products |
| Hardan 1994 | A non‐randomised observational study, therapeutic platelets only, historical control reported only as an abstract |
| Harrup 1999 | Comparison of buffy coat plasma versus T‐sol platelet transfusions |
| Heal 1993 | Comparison of ABO ‐compatible versus mismatched platelet transfusions |
| Heal 2004 | Review |
| Heddle 1994 | Comparison of plasma from platelet concentrates versus platelets |
| Heddle 1999 | Comparison of plasma removal versus leucodepletion |
| Heddle 2002 | Comparison of plasma removal versus leucodepletion |
| Heddle 2003 | Systematic review ‐ methods of assessing bleeding outcome |
| Heddle 2005 | Comparison of whole blood ‐derived platelets stored as a pool versus individually |
| Heddle 2007 | Review |
| Heddle 2009 | Comparison of a low dose versus standard platelet component dose |
| Higby 1974 | Comparison of prophylactic platelets versus platelet poor plasma |
| ISRCTN01292427 | Comparison of dynamic light scattering‐screened versus unscreened platelets |
| ISRCTN49080246 | Comparison of 1 ‐ 5 versus 6 ‐ 7 day ‐old platelet transfusions |
| ISRCTN56366401 | Comparison of different types of platelet component |
| Jelic 2006 | Review |
| Johansson 2007 | Wrong patient group ‐ ruptured abdominal aortic aneurysm |
| Julmy 2009 | Wrong patient group ‐ ruptured abdominal aortic aneurysm |
| Kakaiya 1981 | Comparison of apheresis versus pooled platelet concentrates |
| Kerkhoffs 2010 | Comparison of standard platelets versus pathogen inactivated platelets versus platelets stored in PAS II media |
| Klumpp 1999 | A randomised cross‐over study. This study was included within the previous systematic review ; however, due to stricter inclusion/exclusion criteria, this study has now been excluded from the review. Only laboratory outcomes were reported. 37% of participants had a non‐haematological malignancy (breast cancer) |
| Kluter 1996 | Comparison of random ‐donor platelet components from pooled buffy coats versus apheresis platelet components |
| Lapierre 2003 | Comparison of standard apheresis platelet products versus a donor reduction policy |
| Lawrence 2001 | A non‐randomised retrospective historical control study (different platelet transfusion thresholds) |
| Leach 1991 | Comparison of warmed versus standard platelet transfusions |
| Lee 1989 | Comparison of ABO ‐matched versus mismatched platelet transfusions |
| Levi 2002 | Review |
| Lordkipanidze 2009 | Review |
| Lozano 2003 | Review |
| Lozano 2010 | Efficacy of older platelet transfusions |
| Lozano 2011 | Comparison of pathogen inactivated versus conventional platelet products |
| Lu 2011 | Comparison of a low ‐dose versus standard ‐dose platelet component |
| Martel 2004 | Review |
| McCullough 2004 | Comparison of pathogen inactivated versus conventional apheresis platelets |
| McNicol 2003 | Review |
| Messerschmidt 1988 | Comparison of HLA ‐matched versus mismatched platelet transfusions |
| Mirasol 2010 | Comparison of pathogen inactivated versus conventional platelet products |
| Murphy 1982 | Comparison of a prophylactic versus therapeutic platelet transfusion policy |
| Murphy 1986 | Comparison of HLA ‐matched and leucodepleted blood products |
| Navarro 1998 | A non‐randomised retrospective historical control observational study (different platelet transfusion thresholds) |
| NCT00699621 | Wrong patient group ‐ intracerebral haemorrhage |
| NCT01615146 | Comparison of a prophylactic versus therapeutic platelet transfusion policy |
| Nevo 2007 | A non‐randomised retrospective analysis (different platelet thresholds) |
| Norol 1998 | A non‐randomised prospective comparison ( 3 different doses of platelets) |
| Norville 1994 | Comparison of 2 different infusion pumps for platelet transfusions |
| Norville 1997 | Comparison of 2 different infusion rates |
| Oksanen 1991 | Comparison of pre‐ versus poststorage leucodepletion of p latelet rich plasma ‐derived platelet transfusions |
| Oksanen 1994 | Comparison of leucodepleted buffy coat ‐derived platelet transfusions versus historical control |
| Paananen 2009 | Non‐randomised study (unclear whether prospective or retrospective) |
| Pamphilon 1996 | Comparison of buffy coat platelet components, single ‐donor apheresis non‐leucocyte depleted and single ‐donor apheresis leucocyte‐depleted platelet components |
| Paramo 2004 | Review |
| Poon 2003 | Review |
| Qureshi 2007 | Audit of platelet transfusions in the United Kingdom |
| Rabinowitz 2010 | Review |
| Rayment 2005 | Review |
| Razzaghi 2012 | Systematic review of platelet transfusion threshold in people with gastrointestinal bleeding |
| Rebulla 2009 | Comparison of pathogen inactivated versus standard platelet components |
| Reed 1986 | Wrong patient group ‐ massive transfusion |
| Roberts 2003 | Review |
| Roy 1973 | Comparison of different platelet component doses |
| Sagmeister 1999 | A non‐randomised retrospective study (aplastic anaemia) |
| Sakakura 2003 | Review |
| Samama 2005 | Guideline |
| Schiffer 1983 | Comparison of leucodepleted versus standard platelet concentrates |
| Sensebe 2004 | Comparison of different platelet component doses |
| Shanwell 1992 | Comparison of fresh versus stored platelets |
| Shehata 2009 | Systematic review ‐ ABO ‐identical versus non‐identical platelet transfusions |
| Shen 2007 | Review |
| Singer 1988 | Single ‐donor HLA ‐matched versus random ‐donor platelets |
| Sintnicolaas 1981 | Comparison of single ‐donor and multiple ‐donor platelet components |
| Sintnicolaas 1982 | Comparison of a prophylactic versus therapeutic platelet transfusion policy |
| Sintnicolaas 1995 | Comparison of leucocyte depleted versus standard platelets |
| Slichter 1998 | Comparison of apheresis versus pooled platelet components |
| Slichter 2004 | Review |
| Slichter 2006 | Comparison of pathogen inactivated versus conventional apheresis platelets |
| Slichter 2007 | Review |
| Slichter 2010 | Comparison of different platelet component doses |
| Slichter 2012 | Review |
| Solomon 1978 | Comparison of a prophylactic versus therapeutic platelet transfusion policy |
| Sosa 2003 | Review |
| Spiess 2004 | Wrong patient group ‐ cardiac |
| Stanworth 2013 | Comparison of a prophylactic versus therapeutic platelet transfusion policy |
| Steffens 2002 | Comparison of different platelet component doses |
| Strauss 2004 | Review |
| Strauss 2005 | Review |
| Strindberg 1996 | Comparison of apheresis versus buffy coat platelet products |
| Sweeney 2000 | Comparison of pre‐storage leucodepleted versus bedside leucodepleted platelets |
| Tinmouth 2003 | Review |
| Tinmouth 2004 | Comparison of low ‐dose platelet components versus standard ‐dose platelet components |
| Tosetto 2009 | Guideline |
| TRAP 1997 | Comparison of standard pooled platelet product versus irradiated pooled platelet product versus leucodepleted pooled platelet product versus apheresis platelet product |
| Vadhan‐Raj 2002 | Wrong patient group ‐ gynaecological malignancy |
| Van Marwijk 1991 | Comparison of leucodepleted platelet products prepared by filtration or centrifugation |
| van Rhenen 2003 | Comparison of pathogen inactivated versus standard buffy coat ‐derived platelet transfusions |
| Velik‐Salchner 2007 | Non‐human study |
| Verma 2008 | A non‐randomised observational study |
| Wandt 1998 | A non‐randomised prospective cohort study (not randomised at the participant level) |
| Wandt 2005 | A non‐randomised prospective study with an historical case control (therapeutic versus prophylactic platelet transfusions) |
| Wandt 2006 | A non‐randomised prospective study with an historical case control (therapeutic versus prophylactic platelet transfusions) |
| Wandt 2010 | Review |
| Wandt 2012 | Comparison of a prophylactic versus therapeutic platelet transfusion policy |
| Wang 2002 | A comparison of acetaminophen and diphenhydramine versus placebo as premedication for platelet transfusions |
| Wang 2005 | Review |
| Weigand 2009 | Prospective observational study |
| Williamson 1994 | Comparison of standard versus bedside leucodepleted platelet products |
| Woodard 2002 | Review |
| Zahur 2002 | Prospective observational study |
| Zeller 2014 | Review |
| Zhao 2002 | Comparison of leucodepleted versus standard platelet transfusions |
| Zumberg 2002 | This study was included within the previous systematic review ; however, due to stricter inclusion/exclusion criteria, this study has now been excluded from the review. 31% of participants had a non‐haematological malignancy (breast cancer) |
HLA = human leukocyte antigen
Differences between protocol and review
The previous review, Estcourt 2012a, has now been split into four separate reviews. Protocols were published for these four separate reviews (Estcourt 2014a; Estcourt 2014b; Estcourt 2014c; Estcourt 2014d). There have been no changes between the protocol for this review, Estcourt 2014c, and the completed review.
Aspects of the protocol that were not implemented due to lack of data
We did not perform a formal assessment of potential publication bias (small‐trial bias) because the review included fewer than 10 trials (Sterne 2011).
We did not prespecify in the protocol how we would deal with any unit of analysis issues. For this review there was a unit of analysis issue for the total number of days of bleeding. We only reported the number of days of bleeding if it had been reported per participant, or if the authors had performed an appropriate analysis to account for repeated measures. In this review, the Rebulla 1997 authors used a permutation analysis according to Freedman 1989 to take into account the repeated events data; all other studies did not take into account unit of analysis issues with this outcome, and so data were not reported.
We could not perform three of the four planned comparisons, because no included study compared these interventions.
No studies compared a lower platelet count threshold (5 x 109/L) versus a standard platelet transfusion threshold (10 x 109/L).
No studies compared different platelet count thresholds (5 x 109/L, 20 x 109/L, 30 x 109/L, or 50 x 109/L) that did not include a comparison against the standard platelet transfusion threshold (10 x 109/L).
No studies compared alternative thresholds to guide prophylactic platelet transfusions (e.g. platelet mass, immature platelet fraction, absolute immature platelet number).
Secondary outcomes: None of the studies reported on the platelet transfusion interval; additional interventions to stop bleeding; transfusion‐transmitted infection; or quality of life.
Subgroup analyses: We did not perform two subgroup analyses due to lack of data; these were presence of fever and type of treatment. We did not perform meta‐regression because no subgroup contained more than 10 studies (Deeks 2011). We commented on differences between subgroups as a narrative.
Assessment of heterogeneity: We did not assess age of study as a reason for heterogeneity, as all studies recruited participants between 1991 and 2001.
Sensitivity analyses: None of the three included trials had more that 20% of participants lost to follow‐up, and all of the trials had some threats to validity, therefore we performed neither pre‐planned sensitivity analysis.
Contributions of authors
Lise Estcourt: protocol development, searching, selection of studies, eligibility and quality assessment, data extraction and analysis, and content expert.
Simon Stanworth: protocol development, searching, selection of studies, eligibility and quality assessment, data extraction and analysis, and content expert.
Carolyn Doree: protocol development, searching and selection of studies.
Sally Hopewell: protocol development and methodological expert.
Marialena Trivella: protocol development and statistical expert.
Mike Murphy: protocol development and content expert.
Sources of support
Internal sources
-
NHS Blood and Transplant, Research and Development, UK.
To support the work of the Systematic Review Initiative (SRI)
External sources
-
Cochrane Haematological Malignancies Group, Germany.
For their editorial support
-
National Institute for Health Research (NIHR) Cochrane Programme Grant, UK.
For technical systematic review support
Declarations of interest
Lise Estcourt: partly funded by the NIHR Cochrane Programme Grant ‐ Safe and Appropriate Use of Blood Components.
Simon Stanworth: none declared.
Carolyn Doree: none declared.
Sally Hopewell: partly funded by the NIHR Cochrane Programme Grant ‐ Safe and Appropriate Use of Blood Components.
Marialena Trivella: partly funded by the NIHR Cochrane Programme Grant ‐ Safe and Appropriate Use of Blood Components.
Mike Murphy: none declared.
New
References
References to studies included in this review
Diedrich 2005 {published data only (unpublished sought but not used)}
- Diedrich B, Remberger M, Shanwell A, Svahn BM, Ringden O. A prospective randomised trial of a prophylactic platelet transfusion trigger of 10 x 109 per L versus 30 x 109 per L in allogeneic hematopoietic progenitor cell transplant recipients. Transfusion 2005;45:1064‐72. [DOI] [PubMed] [Google Scholar]
Heckman 1997 {published and unpublished data}
- Heckman K, Weiner GJ, Strauss RG, Jones MP, Burns CP. Randomized evaluation of the optimal platelet count for prophylactic platelet transfusions in patients undergoing induction therapy for acute leukaemia (American Society of Hematology 35th Annual Meeting). Blood 1993;82(Abstract):192a. [Google Scholar]
- Heckman KD, Weiner GJ, Davis CS, Strauss RG, Jones MP, Burns CP. Randomized study of prophylactic platelet transfusion threshold during induction therapy for adult acute leukaemia: 10 x 109/L versus 20 x 109/L. Journal of Clinical Oncology 1997;15:1143‐9. [DOI] [PubMed] [Google Scholar]
Rebulla 1997 {published and unpublished data}
- Cook RJ, Heddle NM, Rebulla P, Sigouin CS, Webert KE. Methods for the analysis of bleeding outcomes in randomised trials of platelet transfusion triggers. Transfusion 2004;44:1135‐42. [DOI] [PubMed] [Google Scholar]
- Finazzi G for the GIMEMA Group. The platelet transfusion trigger trial (PTTT): A multivariate analysis of risk factors for major bleeding in acute myeloid leukaemia (AML). Thrombosis and Haemostasis 1997;78(Supplement):768‐9. [Google Scholar]
- GIMEMA Group. Interim report from the platelet transfusion trigger trial (PTTT): a prospective controlled study on bleeding risk in acute myeloid leukaemia (AML) patients randomized to be transfused at ≤10 versus ≤20 x 109/L platelets. Blood 1996;88(10):443a. [Google Scholar]
- Heddle NM, Cook RJ, Sigouin C, Slichter SJ, Murphy M, Rebulla P. A descriptive analysis of international transfusion practice and bleeding outcomes in patients with acute leukaemia. Transfusion 2006;46:903‐11. [DOI] [PubMed] [Google Scholar]
- Rebulla P, Finazzi G, Marangoni F, Avvisati G, Gugliotta L, Tognoni G, et al. The threshold for prophylactic platelet transfusions in adults with acute myeloid leukaemia. The New England Journal of Medicine 1997;337:1870‐5. [DOI] [PubMed] [Google Scholar]
- Webert KE, Cook RJ, Sigouin CS, Rebulla P, Heddle NM. The risk of bleeding in thrombocytopenic patients with acute myeloid leukaemia. Haematologica 2006;91(11):1530‐7. [PubMed] [Google Scholar]
References to studies excluded from this review
Aderka 1986 {published data only}
- Aderka D, Praff G, Santo M, Weinberger A, Pinkhas J. Bleeding due to thrombocytopenia in acute leukaemias and reevaluation of the prophylactic platelet transfusion policy. American Journal of the Medical Sciences 1986;291:147‐51. [DOI] [PubMed] [Google Scholar]
Agliastro 2006 {published data only}
- Agliastro RE, Francisci G, Bonaccorso R, Spicola D, Ziino O, Arico M, et al. Clinical study in pediatric hemato‐oncology patients: efficacy of pathogen inactivated platelets versus apheresis platelets. Transfusion 2006;46(9S):117A. [Google Scholar]
Akkök 2007 {published data only}
- Akkök CA, Brinch L, Lauritzsen GF, Solheim BG, Kjelsden‐Kragh J. Clinical effect of buffy‐coat vs. apheresis platelet concentrates in patients with severe thrombocytopenia after intensive chemotherapy. Vox Sanguinis 2007;93(1):42‐8. [DOI] [PubMed] [Google Scholar]
Anderson 1997 {published data only}
- Anderson NA, Gray S, Copplestone JA, Chan DC, Hamon M, Prentice AG, et al. A prospective randomized study of three types of platelet concentrates in patients with haematological malignancy: corrected platelet count increments and frequency of nonhaemolytic febrile transfusion reactions. Transfusion Medicine 1997;7:33‐9. [DOI] [PubMed] [Google Scholar]
Andreu 2009 {published data only}
- Andreu G, Vasse J, Tardivel R, Semana G. Platelet transfusion: products, indications, dose, threshold and efficacy. Transfusion Clinique Et Biologique 2009;16(2):118‐33. [DOI] [PubMed] [Google Scholar]
Andrew 1993 {published data only}
- Andrew M, Vegh P, Caco C, Kirpalani H, Jefferies A, Ohlsson A, et al. A randomized controlled trial of platelet transfusions in thrombocytopenic premature infants. Journal of Pediatrics 1993;123(2):285‐91. [DOI] [PubMed] [Google Scholar]
Arnold 2004 {published data only}
- Arnold DM, Heddle NM, Carruthers J, Kulczycky M, Sigouin C, Blajchman MA. A randomized crossover trial comparing in‐vivo platelet recovery and survival of leukoreduced apheresis and whole blood derived platelets. Transfusion 2004;44(supplement):1A. [DOI] [PubMed] [Google Scholar]
Arnold 2006 {published data only}
- Arnold DM, Crowther MA, Cook RJ, Sigouin C, Heddle NM, Molnar L, et al. Utilization of platelet transfusions in the intensive care unit: indications, transfusion triggers, and platelet count responses. Transfusion 2006;46(8):1286‐91. [DOI] [PubMed] [Google Scholar]
Avvisati 2003 {published data only}
- Avvisati G, Tirindelli MC, Annibali O. Thrombocytopenia and hemorrhagic risk in cancer patients. Critical Reviews in Oncology/Hematology 2003;48(Suppl 1):S13‐6. [DOI] [PubMed] [Google Scholar]
Bai 2004 {published data only}
- Bai CM, Xu GX, Zhao YQ, Han SM, Shan YD. A multi‐centre clinical trial of recombinant human thrombopoietin in the treatment of chemotherapy‐induced thrombocytopenia in patients with solid tumor. Zhongguo Yi Xue Ke Xue Yuan Xue Bao Acta Academiae Medicinae Sinicae 2004;26(4):437‐41. [PubMed] [Google Scholar]
Benjamin 2002 {published data only}
- Benjamin RJ, Anderson KC. What is the proper threshold for platelet transfusion in patients with chemotherapy‐induced thrombocytopenia?. Critical Reviews in Oncology/Hematology 2002;42(2):163‐71. [DOI] [PubMed] [Google Scholar]
Bentley 2000 {published data only}
- Bentley M, Taylor K, Kelly C, Taylor D, Leach B, Rodwell R, et al. Thrombopoietin derived autologous cryopreserved platelet support for peripheral blood progenitor cell transplantation. Haematology Society of Australia and New Zealand Annual Scientific Meeting. Perth, July 23‐26 2000.
Blajchman 2008 {published data only}
- Blajchman MA, Slichter SJ, Heddle NM, Murphy MF. New strategies for the optimal use of platelet transfusions. Hematology/the Education Program of the American Society of Hematology. American Society of Hematology. Education Program 2008;2008:198‐204. [DOI] [PubMed] [Google Scholar]
Blumberg 2002 {published data only}
- Blumberg N, Heal JM, Rowe JM. Platelet transfusion and clinical outcome in acute leukemia in adults. Transfusion 2002;42(9S):5S. [Google Scholar]
Blumberg 2004 {published data only}
- Blumberg N, Heal JM, Rowe JM. A randomized trial of washed red blood cell and platelet transfusions in adult acute leukemia [ISRCTN76536440]. BMC Blood Disorders 2004; Vol. 4, issue 6. [DOI: 10.1186/1471-2326-4-6] [DOI] [PMC free article] [PubMed]
Blundell 1996 {published data only}
- Blundell EL, Pamphilon DH, Fraser ID, Kagen L, Menitove JE, Aster RH, et al. A prospective randomised study of platelet concentrates irradiated with ultraviolet (UV)‐B light in patients with high grade haematological malignancy. Blood 1992;80(10):215A. [DOI] [PubMed] [Google Scholar]
- Blundell EL, Pamphilon DH, Fraser ID, Menitove JE, Greeenwalt TJ, Snyder EL, et al. A prospective, randomized study of the use of platelet concentrates irradiated with ultraviolet‐B light in patients with hematologic malignancy. Transfusion 1996;36(4):296‐302. [DOI] [PubMed] [Google Scholar]
Buhrkuhl 2010 {published data only}
- Buhrkuhl DC. An update on platelet transfusion in hematooncology supportive care. Transfusion 2010;50(10):2266‐76. [DOI] [PubMed] [Google Scholar]
Callow 2002 {published data only}
- Callow CR, Swindell R, Randall W, Chopra R. The frequency of bleeding complications in patients with haematological malignancy following the introduction of a stringent prophylactic platelet transfusion policy. British Journal of Haematology 2002;118:677‐82. [DOI] [PubMed] [Google Scholar]
Cameron 2007 {published data only}
- Cameron B, Rock G, Olberg B, Neurath D. Evaluation of platelet transfusion triggers in a tertiary‐care hospital. Transfusion 2007;47(2):206‐11. [DOI] [PubMed] [Google Scholar]
Carr 1990 {published data only}
- Carr R, Hutton JL, Jenkins JA, Lucas GF, Amphlett NW. Transfusion of ABO‐mismatched platelets leads to early platelet refractoriness. British Journal of Haematology 1990;75:408‐13. [DOI] [PubMed] [Google Scholar]
Casbard 2004 {published data only}
- Casbard AC, Williamson LM, Murphy MF, Rege K, Johnson T. The role of prophylactic fresh frozen plasma in decreasing blood loss and correcting coagulopathy in cardiac surgery. A systematic review. Anaesthesia 2004;59(6):550‐8. [DOI] [PubMed] [Google Scholar]
Chaoui 2005 {published data only}
- Chaoui D, Chakroun T, Robert F, Rio B, Belhocine R, Legrand O, et al. Reticulated platelets: a reliable measure to reduce prophylactic platelet transfusions after intensive chemotherapy. Transfusion 2005;45(5):766‐72. [DOI] [PubMed] [Google Scholar]
Chaurasia 2012 {published data only}
- Chaurasia R, Elhence P, Nityanand S, Verma A. 'Bleeding' and 'transfusion support' in acute myeloid leukemia patients: the challenges. Indian Journal of Hematology and Blood Transfusion 2012;28(4):249‐50. [Google Scholar]
Cid 2007 {published data only}
- Cid J, Lozano M. Lower or higher doses for prophylactic platelet transfusions: results of a meta‐analysis of randomized controlled trials. Transfusion 2007;47:464‐70. [DOI] [PubMed] [Google Scholar]
Corash 2001 {published data only}
- Corash L, Klueter H, Rhenen D, Gullikson H, Pamphilon D, Cazenave JP, et al. Intercept platelet concentrates (IPC) are effective and safe for support of multiple cycles of thrombocytopenia: the eurosprite phase III trial. Hematology Journal 2001;2(Supplement 1):178‐9. [Google Scholar]
Couban 2002 {published data only}
- Couban S, Carruthers J, Andreou P, Klama LN, Barr R, Kelton JG, et al. Platelet transfusions in children: results of a randomised prospective cross‐over trial of plasma removal and a prospective audit of WBC reduction. Transfusion 2002;42:753‐8. [DOI] [PubMed] [Google Scholar]
Decaudin 2004 {published data only}
- Decaudin D, Vantelon JM, Bourhis JH, Farace F, Bonnet ML, Guillier M, et al. Ex vivo expansion of megakaryocyte precursor cells in autologous stem cell transplantation for relapsed malignant lymphoma. Bone Marrow Transplantation 2004;34(12):1089‐93. [DOI] [PubMed] [Google Scholar]
de Wildt‐Eggen 2000 {published data only}
- Wildt‐Eggen J, Nauta S, Schrijver JG, Marwijk KM, Bins M, Prooijen HC, et al. Reactions and platelet increments after transfusion of platelet concentrates in plasma or an additive solution: a prospective, randomized study. Transfusion 2000;40(4):398‐403. [DOI] [PubMed] [Google Scholar]
Diedrich 2009 {published data only}
- Diedrich B, Ringden O, Watz E, Shanwell A. A randomised study of buffy coat platelets in platelet additive solution 1‐5 versus 6‐7 days prior to prophylactic transfusion of allogeneic haematopoietic cell transplant recipients. Vox Sanguinis 2009;97(3):254‐9. [DOI] [PubMed] [Google Scholar]
- Diedrich B, Watz E, Ringden O, Shanwell A. A randomized study in allogeneic haematopoietic stem cell transplant recipients comparing prophylactic transfusion of buffy coat platelets stored for 1‐5 vs. 6‐7 days. Vox Sanguinis 2008;95(Supp 1):Abstract. [DOI] [PubMed] [Google Scholar]
Di Pietro 1998 {published data only}
- Pietro G, Menicucci A, Venturini S, Graziani G, Sani R, Avanzi G. Platelet transfusion support during bone marrow transplantation. Comparative study between the use of HLA platelet apheresis and random platelet apheresis. Trasfusione del Sangue 1998;43(1):47‐50. [Google Scholar]
Dumont 2011 {published data only}
- Dumont LJ, Dumont DF, Unger ZM, Siegel A, Szczepiorkowski ZM, Corson JS, et al. A randomized controlled trial comparing autologous radiolabeled in vivo platelet(plt) recoveries and survivals of 7‐day‐stored plt‐rich plasma and buffy coat plts from the same subjects. Transfusion 51;6:1241‐8. [DOI] [PubMed] [Google Scholar]
Dzik 2004 {published data only}
- Dzik WH. Predicting hemorrhage using preoperative coagulation screening assays. Current Hematology Reports 2004;3(5):324‐30. [PubMed] [Google Scholar]
Eder 2007 {published data only}
- Eder AF, Kennedy JM, Dy BA, Notari EP, Weiss JW, Fang CT, et al. Bacterial screening of apheresis platelets and the residual risk of septic transfusion reactions: The American Red Cross Experience (2004‐2006). Transfusion 2007;47(7):1134‐42. [DOI] [PubMed] [Google Scholar]
Elting 2002 {published data only}
- Elting LS, Martin CG, Kurtin DJ, Cantor SB, Rubenstein EB, Rodriguez S, et al. The bleeding risk index: a clinical prediction rule to guide the prophylactic use of platelet transfusions in patients with lymphoma or solid tumors. Cancer 2002;94(12):3252‐62. [DOI] [PubMed] [Google Scholar]
Elting 2003 {published data only}
- Elting LS, Cantor SB, Martin CG, Hamblin L, Kurtin D, Rivera E, et al. Cost of chemotherapy‐induced thrombocytopenia among patients with lymphoma or solid tumors. Cancer 2003;97(6):1541‐50. [DOI] [PubMed] [Google Scholar]
Fanning 1995 {published data only}
- Fanning J, Hilgers RD, Murray KP, Bolt K, Aughenbaugh DM. Conservative management of chemotherapy‐induced thrombocytopenia in women with gynecological cancers. Gynecologic Oncology 1995;59:191‐3. [DOI] [PubMed] [Google Scholar]
Follea 2004 {published data only}
- Follea G. Homologous platelet concentrates: products available and utilisation rules in oncology and haematology. Hematologie 2004;10(3):233‐44. [Google Scholar]
Friedmann 2002 {published data only}
- Friedmann AM, Sengul H, Lehmann H, Schwartz C, Goodman S. Do basic laboratory tests or clinical observations predict bleeding in thrombocytopenic oncology patients?. Transfusion Medicine Reviews 2002;16:34‐45. [DOI] [PubMed] [Google Scholar]
Gajic 2006 {published data only}
- Gajic O, Dzik WH, Toy P. Fresh frozen plasma and platelet transfusion for non‐bleeding patients in the intensive care unit: Benefit or harm?. Critical Care Medicine 2006;35(5 Suppl):S170‐3. [DOI] [PubMed] [Google Scholar]
Gerday 2009 {published data only}
- Gerday E, Baer VL, Lambert DK, Pau DA, Sola‐Visner MC, Pysher TJ, et al. Testing platelet mass versus platelet count to guide platelet transfusions in the neonatal intensive care unit. Transfusion 2009;49:2034‐9. [DOI] [PubMed] [Google Scholar]
Gil‐Fernandez 1996 {published data only}
- Gil‐Fernandez JJ, Alegre A, Fernandez‐Villalta MJ, Pinilla I, Gomez Garcia V, Martinez C, et al. Clinical results of a stringent policy on prophylactic platelet transfusion: non‐randomized comparative analysis in 190 bone marrow transplant patients from a single institution. Bone Marrow Transplantation 1996;18:931‐5. [PubMed] [Google Scholar]
Gmür 1983 {published data only}
- Gmür J, Felten A, Osterwalder B, Honegger H, Hermann A, Sauter C, et al. Delayed alloimmunization using random single donor platelet transfusions: a prospective study in thrombocytopenic patients with acute leukemia. Blood 1983;62(2):473‐9. [PubMed] [Google Scholar]
Gmür 1991 {published data only}
- Gmür J, Burger J, Schanz U, Fehr J, Schaffner A. Safety of stringent prophylactic platelet transfusion policy for patients with acute leukaemia. The Lancet 1991;338:1223‐6. [DOI] [PubMed] [Google Scholar]
Goodnough 2001 {published data only}
- Goodnough LT, Kuter DJ, McCullough J, Slichter SJ, DiPersio J, Romo J, et al. Prophylactic platelet transfusions from healthy apheresis platelet donors undergoing treatment with thrombopoietin. Blood 2001;98(5):1346‐51. [DOI] [PubMed] [Google Scholar]
Goodnough 2002 {published data only}
- Goodnough LT, DiPersio JFD. Issues in the management of cancer‐related thrombocytopenia. Oncology 2002;16(11):1558‐67. [PubMed] [Google Scholar]
Goodnough 2005 {published data only}
- Goodnough LT. Risks of blood transfusion. Anesthesiology Clinics of North America 2005;23(2):241‐52. [DOI] [PubMed] [Google Scholar]
Goodrich 2008 {published data only}
- Goodrich R, Follua G, Roberts T. Clinical evaluation of Mirasol PRT treated apheresis platelets in thrombocytopenic patients. Transfusion 2008;48(S2):20A. [Google Scholar]
Greeno 2007 {published data only}
- Greeno E, McCullough J, Weisdorf D. Platelet utilisation and the transfusion trigger: A prospective analysis. Transfusion 2007;72(2):201‐5. [DOI] [PubMed] [Google Scholar]
Grossman 1980 {published data only}
- Grossman L, Mangal A, Hislop TG, Buskard NA. Preliminary report on a randomized study of prophylactic (P) vs. therapeutic (T) platelet transfusions. Blood 1980;80:271. [Google Scholar]
Gurkan 2007 {published data only}
- Gurkan E, Patah PA, Saliba RM, Ramos CA, Anderson BS, Champlin R, et al. Efficacy of prophylactic transfusions using single donor apheresis platelets versus pooled platelet concentrates in AML/MDS patients receiving allogeneic hematopoietic stem cell transplantation. Bone Marrow Transplantation 2007;40(5):461‐4. [DOI] [PubMed] [Google Scholar]
Hardan 1994 {published data only}
- Hardan I, Sofer O, Shpilberg O, Ra'anani P, Ben‐Bassat I. Safety of stringent prophylactic platelet transfusion (PT) policy for lymphoma patients treated by high dose chemotherapy (HDC) and autologous stem cell support. [20th Annual Meeting of the European Group for Bone Marrow Transplantation and 10th Meeting of the Nurses Group]. Bone Marrow Transplant 1994;14(Supplement):Abstract 330. [Google Scholar]
Harrup 1999 {published data only}
- Harrup RA, Kennedy JT, Kiss J, Daniels B. Randomised blinded comparison of buffy coat plasma or T‐sol supported platelet transfusions. Haematology Society of Australia and New Zealand Annual Scientific Meeting. Hobart; Tasmania, October 1999.
Heal 1993 {published data only}
- Heal J, Kemmotsu N, Rowe J, Blumberg N. A survival advantage in leukaemics receiving ABO identical platelets. Blood 1991;78:349a. [DOI] [PubMed] [Google Scholar]
- Heal J, Rowe J, Blumberg N. The importance of ABO identical platelet transfusions. Blood 1991;78:348a. [Google Scholar]
- Heal J, Rowe J, McMican A, Finke K, Blumberg N. A randomised trial of ABO identical versus ABO unmatched platelet transfusions. Blood 1989;74(7 Supp 1):215a. [Google Scholar]
- Heal JM, Rowe JM, McMican A, Masel D, Finke C, Blumberg N. The role of ABO matching in platelet transfusion. European Journal of Haematology 1993;50:110‐7. [DOI] [PubMed] [Google Scholar]
Heal 2004 {published data only}
- Heal JM, Blumberg N. Optimizing platelet transfusion therapy. Blood Reviews 2004;18(3):149‐65. [DOI] [PubMed] [Google Scholar]
Heddle 1994 {published data only}
- Heddle NM, Klama L, Singer J, Richards C, Fedak P, Walker I, et al. The role of the plasma from platelet concentrates in transfusion reactions. The New England Journal of Medicine 1994;331(10):625‐8. [DOI] [PubMed] [Google Scholar]
Heddle 1999 {published data only}
- Heddle NM, Klama L, Meyer R, Walker I, Boshkov L, Roberts R, et al. A randomized controlled trial comparing plasma removal with white cell reduction to prevent reactions to platelets. Transfusion 1999;39(3):231‐8. [DOI] [PubMed] [Google Scholar]
Heddle 2002 {published data only}
- Heddle NM, Blajchman MA, Meyer RM, Lipton JH, Walker IR, Sher GD, et al. A randomized controlled trial comparing the frequency of acute reactions to plasma‐removed platelets and prestorage WBC‐reduced platelets. Transfusion 2002;42(5):556‐66. [DOI] [PubMed] [Google Scholar]
Heddle 2003 {published data only}
- Heddle NM, Cook RJ, Webert KE, Sigouin C, Rebulla P. Methodologic issues in the use of bleeding as an outcome in transfusion medicine studies. Transfusion 2003;43:742‐52. [DOI] [PubMed] [Google Scholar]
Heddle 2005 {published data only}
- Heddle NM, Cook RJ, Blajchman MA, Barty RL, Sigouin CS, Boye DM, et al. Assessing the effectiveness of whole blood‐derived platelets stored as a pool: a randomized block noninferiority trial. Transfusion 2005;45(6):896‐903. [DOI] [PubMed] [Google Scholar]
Heddle 2007 {published data only}
- Heddle NM. Controversy concerning platelet dose. ISBT Science Series, Vol 2, No 1: State of the Art Presentations 2007;2:220‐5. [Google Scholar]
Heddle 2009 {published and unpublished data}
- Heddle NM, Cook RJ, Tinmouth A, Kouroukis CT, Hervig T, Klapper E, et al. A randomized controlled trial comparing standard and low dose strategies for transfusion of platelets (SToP) to patients with thrombocytopenia. Blood 2009;113(7):1564‐73. [DOI] [PubMed] [Google Scholar]
- Heddle NM, Wu C, Vassallo R, Carey P, Arnold D, Lozano M, et al. Adjudicating bleeding events in a platelet dose study: impact on outcome results and challenges. Transfusion 2011;51:2304‐10. [DOI] [PubMed] [Google Scholar]
- NCT00420914. Strategies for Transfusion of Platelets (SToP). http://clinicaltrials.gov/show/NCT00420914 (accessed 15 September 2009).
Higby 1974 {published data only}
- Higby DJ, Cohen E, Holland JF, Sinks L. The prophylactic treatment of thrombocytopenic leukemic patients with platelets: a double blind study. Transfusion 1974;14:440‐5. [DOI] [PubMed] [Google Scholar]
ISRCTN01292427 {published data only}
- ISRCTN01292427. Comparison of in vivo outcome following transfusion of dynamic light scattering‐screened versus unscreened platelets in hematologic malignancy. www.controlled‐trials.com/ISRCTN01292427 (accessed 16 June 2014).
ISRCTN49080246 {published data only}
- ISRCTN49080246. Platelet Process Improvement Project. http://www.controlled‐trials.com/ISRCTN49080246 (accessed 16 June 2011).
ISRCTN56366401 {published data only}
- ISRCTN56366401. Platelet responsiveness and outcome from platelet transfusion ‐ does inherent variation in donor platelet function affect the clinical efficacy of apheresis platelets? A randomised double blind single centre trial. UK Clinical Research Network (UKCRN) http://www.controlled‐trials.com/ISRCTN56366401 (accessed 16 June 2014).
Jelic 2006 {published data only}
- Jelic S, Radulovic S. Chemotherapy‐associated thrombocytopenia current and emerging management strategies. American Journal of Cancer 2006;5(6):371‐82. [Google Scholar]
Johansson 2007 {published data only}
- Johansson PI, Stensballe J, Rosenberg I, Hisløv TL, Jørgensen L, Secher NH. Proactive administration of platelets and plasma for patients with a ruptured abdominal aortic aneurysm: evaluating a change in transfusion practice. Transfusion 2007;47(4):593‐8. [DOI] [PubMed] [Google Scholar]
Julmy 2009 {published data only}
- Julmy F, Ammann RA, Taleghani BM, Fontana S, Hirt A, Leibundgut K. Transfusion efficacy of ABO major‐mismatched platelets (PLTS) in children is inferior to that of ABO‐identical platelets. Transfusion 2009;91(1):21‐33. [DOI] [PubMed] [Google Scholar]
Kakaiya 1981 {published data only}
- Kakaiya RM, Hezzey AJ, Bove JR, Katz AJ, Genco PV, Buchholz DH, et al. Alloimmunization following apheresis platelets vs. pooled platelet concentrates. A prospective randomized study. Transfusion 1981;21(5):600. [Google Scholar]
Kerkhoffs 2010 {published data only}
- Kerkhoffs JH, Novotny VM, Boekhorst PA, Schipperus MR, Zwaginga JJ, Pampus I, et al. Clinical effectiveness and safety of pooled, random donor platelet concentrates, leucoreduced and stored up to seven days in either plasma or additive solution with and without pathogen reduction in hemato‐oncological patients. Transfusion 2009;49(s3):2A. [Google Scholar]
- Kerkhoffs JLH, Putten WL, Novotny VM, Boekhorst PA, Schipperus MR, Zwaginga JJ, et al. Clinical effectiveness of leucoreduced, pooled donor platelet concentrates, stored in plasma or additive solution with and without pathogen reduction. British Journal of Haematology 2010;150(2):209‐17. [DOI] [PubMed] [Google Scholar]
Klumpp 1999 {published data only}
- Ackerman SJ, Klumpp TR, Guzman GI, Herman JH, Gaughan JP, Bleecker GC, et al. Economic consequences of alterations in platelet transfusion dose: analysis of a prospective, randomized, double‐blind trial. Transfusion 2000;40(12):1457‐62. [DOI] [PubMed] [Google Scholar]
- Hermann JH, Klumpp TR, Christman RA, Russo RR, Goldberg SL, Mangan KF. The effect of platelet dose on the outcome of prophylactic platelet transfusion. Transfusion 1995;35(10s):46S. [Google Scholar]
- Klumpp T, Herman JH, Christman RA, Russo RR, Goldberg SL, MacDonald JS, et al. The effect of platelet dose on the interval between platelet transfusions in patients undergoing bone marrow or peripheral blood stem cell transplantation. Proceedings of American Society of Clinical Oncology (ASCO). 1995:536.
- Klumpp TR, Herman JH, Gaughan JP, Russo RR, Christman RA, Goldberg SL, et al. Clinical consequences of alterations in platelet dose: a prospective, randomized, double‐blind trial. Transfusion 1999;39:674‐81. [DOI] [PubMed] [Google Scholar]
Kluter 1996 {published data only}
- Kluter H, Dorges L, Maass E, Wagner T, Bartels H, Kirchner H. In‐vivo evaluation of random donor platelet concentrates from pooled buffy coats. Annals of Hematology 1996;73(2):85‐9. [DOI] [PubMed] [Google Scholar]
Lapierre 2003 {published data only}
- Lapierre V, Benhamou E, Tramalloni D, Brault P, Valteau‐Couanet D, Ducourtieux M, et al. A randomised trial of platelet transfusion policies after blood stem cell transplantation in young children: reduction of number of single platelet concentrate donors per child. Bone Marrow Transplantation 2003;31(Supplement 1):P756. [Google Scholar]
Lawrence 2001 {published data only}
- Lawrence JB, Yomtovian RA, Hammons T, Masarik SR, Chongkolwatana V, Cregar RJ, et al. Lowering the prophylactic platelet transfusion threshold: a prospective analysis. Leukemia & Lymphoma 2001;41:67‐76. [DOI] [PubMed] [Google Scholar]
Leach 1991 {published data only}
- Leach MF, Fairweather RB, Aubuchon JP. Use of warmed single donor platelets in autologous bone marrow transplant patients. Transfusion 1991;31(Suppl):20S. [Google Scholar]
Lee 1989 {published data only}
- Lee EJ, Schiffer CA. ABO compatibility can influence the results of platelet transfusion. Results of a randomized trial. Transfusion 1989;29(5):384‐9. [DOI] [PubMed] [Google Scholar]
Levi 2002 {published data only}
- Levi MM, Vink R, Jonge E. Management of bleeding disorders by prohemostatic therapy. International Journal of Hematology 2002;76(Suppl 2):139‐44. [DOI] [PubMed] [Google Scholar]
Lordkipanidze 2009 {published data only}
- Lordkipanidze M, Diodati JG, Pharand C. Possibility of a rebound phenomenon following antiplatelet therapy withdrawal: a look at the clinical and pharmacological evidence. Pharmacology & Therapeutics 2009;123(2):178‐86. [DOI] [PubMed] [Google Scholar]
Lozano 2003 {published data only}
- Lozano M, Cid J. The clinical implications of platelet transfusions associated with ABO or Rh[D) incompatibility. Transfusion Medicine Reviews 2003;17(1):57‐68. [DOI] [PubMed] [Google Scholar]
Lozano 2010 {published data only}
- Lozano M, Knutson F, Tardivel R, Cid J, Maymó R, Löf H, et al. Frequency of prophylactic transfusion failure: a novel outcome to evaluate platelet components stored more than 5 days. Transfusion 2010;50(Supp 2):25A‐6A. [Google Scholar]
Lozano 2011 {published data only}
- Lozano M, Knutson F, Tardivel R, Cid J, Maymó RM, Löf H, et al. A multi‐centre study of therapeutic efficacy and safety of platelet components treated with amotsalen and ultraviolet A pathogen inactivation stored for 6 or 7 d prior to transfusion. British Journal of Haematology 2011;153(3):393‐401. [DOI] [PubMed] [Google Scholar]
Lu 2011 {published data only}
- Lu FQ, An WX, Kang W, Zhang YL. Effect of reducing prophylactic platelet transfusion dose on bleeding in thrombocytopenia patients [降低预防性血小板输注剂量对慢性血小板减少症患者出血风险的影响]. International Journal of Blood Transfusion and Hematology 2011;34(4):295‐8. [Google Scholar]
- Lu FQ, Wang WM, Yu M. Effect of reducing prophylactic platelet transfusion dose on bleeding in thrombocytopenic patients. Vox Sanguinis 2011;101(S1):310 (P‐577). [Google Scholar]
Martel 2004 {published data only}
- Martel N, Wells PS. A meta‐analysis to determine the risk of heparin induced thrombocytopenia (HIT) and isolated thrombocytopenia in prophylaxis studies comparing unfractionated heparin (UFH) and low molecular weight heparin (LMWH). Blood 2004;104(11):708a‐9a. [DOI] [PubMed] [Google Scholar]
McCullough 2004 {published data only}
- Benjamin RJ, Goodnough LT, Lopez‐Perez I, Strauss R, McCullough J, Slichter S, et al. Fresh (1‐2 day‐old) vs. aged (4‐5 day‐old) INTERCEPT platelets and conventional platelets provide comparable count increments. However fresh platelets result in superior hemostasis: results of the SPRINT trial. Transfusion 2003;43(9S):9A. [Google Scholar]
- Corash L, Lin JS, Sherman CD, Eiden J. Determination of acute lung injury following repeated platelet transfusions. Blood 2010; Vol. 117, issue 3:1014‐20. [PUBMED: 20935256] [DOI] [PubMed]
- Goodnough LT, McCullough J, Slichter S, Strauss R, Lin J, Conlan M. A platelet transfusion threshold of 20 x 109/L compared to 10 x 109/L is associated with increased pre‐transfusion bleeding and increased platelet transfusions: results of the SPRINT study. Transfusion 2002;42(9S):17S. [Google Scholar]
- Kluter H, Chapuis B, Cazenave J, Hastka J, Beris P, Dufour P, et al. Apheresis platelets treated with the INTERCEPT Blood System for pathogen inactivation provide platelet count increments and hemostasis comparable to conventional platelets. Vox Sanguinis 2002;83(Suppl 1):110a. [Google Scholar]
- McCullough J, Vesole DH, Benjamin RJ, Slichter SJ, Pineda A, Synder E, et al. Therapeutic efficacy and safety of platelets treated with a photochemical process for pathogen inactivation: the SPRINT Trial. Blood 2004;104(5):1534‐41. [DOI] [PubMed] [Google Scholar]
- Murphy S, Slichter S, McCullough J, Strauss R, Wood L, Lin J, et al. INTERCEPT platelets are hemostatically as effective as conventional platelet in the prophylaxis and treatment of bleeding: results of the SPRINT trial. Vox Sanguinis 2002;83(109):Abstract. [Google Scholar]
- Murphy S, Synder E, Cable R, Slichter SJ, Strauss RG, McCullough J, et al. Platelet dose consistency and its effect on the number of platelet transfusions for support of thrombocytopenia: an analysis of the SPRINT trial of platelets photochemically treated with amotosalen HCl and ultraviolet A light. Transfusion 2006;46(1):24‐33. [DOI] [PubMed] [Google Scholar]
- Pineda A, McCullough J, Benjamin RJ, Cable R, Strauss RG, Burgstaler E, et al. Pathogen inactivation of platelets with a photochemical treatment with amotosalen HCl and ultraviolet light: process used in the SPRINT trial. Transfusion 2006;46(4):562‐71. [PUBMED: 16584432] [DOI] [PubMed] [Google Scholar]
- Slichter SJ, Murphy S, Buchholz D, Lin J, Corash L, Conlan M. INTERCEPT platelets (plts) and conventional plts provide comparable hemostatic response in thrombocytopenic patients: the SPRINT trial. Blood 2002;11(Pt 2):141b. [Google Scholar]
- Snyder E, McCullough J, Slichter SJ, Strauss RG, Lopez‐Plaza I, Lin JS, et al. Clinical safety of platelets photochemically treated with amotosalen HCl and ultraviolet A light for pathogen inactivation: the SPRINT trial. Transfusion 2005; Vol. 45, issue 12:1864‐75. [PUBMED: 16371039] [DOI] [PubMed]
- Strauss RG, Slichter S, Lopez‐Plaza I, Goodnough LT, McCullough J, Lin J, et al. Intercept platelets exhibit immunological refractoriness comparable to conventional platelets. Haematologica 2004;89(Suppl 1):Abstract. [Google Scholar]
- Vesole D, Stadtmauer E, Goodnough LT, Coutre S, Howard F, Lin JS, et al. Source of donor stem cells impacts incidence of bleeding and platelet and RBC transfusion requirements during stem cell transplantation (SCT): results of the Phase III SPRINT trial of INTERCEPT pathogen inactivated platelets. Biology of Blood and Bone Marrow Transplantation 2004; Vol. 10, issue 2:233.
McNicol 2003 {published data only}
- McNicol A, Israels SJ. Platelets and platelet therapy. Journal of Pharmacological Sciences 2003;93(4):381‐96. [DOI] [PubMed] [Google Scholar]
Messerschmidt 1988 {published data only}
- Messerschmidt GL, Makuch R, Appelbaum F, Ungerleider RS, Abrams R, O'Donnell J, et al. A prospective randomized trial of HLA‐matched versus mismatched single‐donor platelet transfusions in cancer patients. Cancer 1988;62(4):795‐801. [DOI] [PubMed] [Google Scholar]
Mirasol 2010 {published data only}
- Ambruso DR, Thurman G, Marschner S, Goodrich RP. Lack of antibody formation to platelet neoantigens after transfusion of riboflavin and ultraviolet light‐treated platelet concentrates. Transfusion 2009;49(12):2631‐6. [PUBMED: 19694996] [DOI] [PubMed] [Google Scholar]
- Goodrich R, Roberts T, Follea G. Clinical evaluation of Mirasol PRT treated apheresis platelets in thrombocytopenic patients. Transfusion 2008;48(Suppl):20A. Abstract No. S49‐020G. [Google Scholar]
- The Mirasol Clinical Evaluation Study Group. A randomized controlled clinical trial evaluating the performance and safety of platelets treated with MIRASOL pathogen reduction technology. Transfusion 2010;50:2362‐75. [DOI] [PubMed] [Google Scholar]
Murphy 1982 {published data only}
- Murphy S, Litwin S, Herring LM, Koch P, Remischovky J, Donaldson MH, et al. Indications for platelet transfusion in children with acute leukemia. American Journal of Hematology 1982;12:347‐56. [DOI] [PubMed] [Google Scholar]
Murphy 1986 {published data only}
- Murphy MF, Metcalfe P, Thomas H, Eve J, Ord J, Lister TA, et al. Use of leucocyte‐poor blood components and HLA‐matched‐platelet donors to prevent HLA alloimmunization. British Journal of Haematology 1986;62:529‐34. [DOI] [PubMed] [Google Scholar]
Navarro 1998 {published data only}
- Navarro J‐T, Hernandez J‐A, Ribera J‐M, Sancho J‐M, Oriol A, Pujol M, et al. Prophylactic platelet transfusion threshold during therapy for adult acute myeloid leukemia: 10,000/mL. Haematologica 1998;83:998‐1000. [PubMed] [Google Scholar]
NCT00699621 {published data only}
- NCT00699621. Platelet transfusion in acute intracerebral haemorrhage. https://clinicaltrials.gov/ct2/show/NCT00699621 (accessed 14 April 2010).
NCT01615146 {published data only}
- NCT01615146. Outpatient Platelet Transfusions in Myelodysplastic Syndromes and Leukemia: The OPTIMAL Pilot. http://ClinicalTrials.gov/show/NCT01615146 (accessed 16 April 2013).
Nevo 2007 {published data only}
- Nevo S, Fuller AK, Borinsky ME, Vogelsang GB. Acute bleeding complications in patients after haematopoietic stem cell transplantation triggers of 10 x 109 and 20 x 109 per L. Transfusion 2007;47:801‐12. [DOI] [PubMed] [Google Scholar]
Norol 1998 {published data only}
- Norol F, Bierling P, Roudot‐Thoraval F, Ferrer Le Coeur F, Rieux C, Lavaux A, et al. Platelet transfusion: a dose response study. Blood 1998;92:1448‐53. [PubMed] [Google Scholar]
Norville 1994 {published data only}
- Norville R, Hinds P, Wilimas J, Fairclough D, Fischl S, Kunkel K. The effects of infusion methods on platelet count, morphology, and corrected count increment in children with cancer: in vitro and in vivo studies. Oncology Nursing Forum 1994;21(10):1669‐73. [PubMed] [Google Scholar]
Norville 1997 {published data only}
- Norville R, Hinds P, Wilimas J, Fischl S, Kunkel K, Fairclough D. The effects of infusion rate on platelet outcomes and patient responses in children with cancer: an in vitro and in vivo study. Oncology Nursing Forum 1997;24(10):1789‐93. [PubMed] [Google Scholar]
Oksanen 1991 {published data only}
- Oksanen K, Kekomaki R, Ruutu T, Koskimies S, Myllyla G. Prevention of alloimmunization in patients with acute leukemia by use of white cell‐reduced blood components: A randomized trial. Transfusion 1991;31:588‐94. [DOI] [PubMed] [Google Scholar]
Oksanen 1994 {published data only}
- Oksanen K, Ebeling F, Kekomäki R, Elonen E, Sahlstedt L, Volin L, et al. Adverse reactions to platelet transfusions are reduced by use of platelet concentrates derived from buffy coat. Vox Sanguinis 1994;67(4):356‐61. [DOI] [PubMed] [Google Scholar]
Paananen 2009 {published data only}
- Paananen P, Arola MO, Pelliniemi TT, Salmi TT, Lähteenmäki PM. Evaluation of the effects of different transfusion trigger levels during the treatment of childhood acute lymphoblastic leukemia. Journal of Pediatric Haematology/Oncology 2009;31(10):745‐9. [DOI] [PubMed] [Google Scholar]
Pamphilon 1996 {published data only}
- Pamphilon DH. Comparative clinical studies of platelet concentrates: Effects on clinical outcome and the use of healthcare resources. Transfusion Science 1996;17(3):343‐6. [PubMed] [Google Scholar]
Paramo 2004 {published data only}
- Paramo JA, Lecumberri R, Hernandez M, Rocha E. Pharmacological alternatives to blood transfusion: what is new about?. Medicina Clinica 2004;122(6):231‐6. [DOI] [PubMed] [Google Scholar]
Poon 2003 {published data only}
- Poon MC. Management of thrombocytopenic bleeding: is there a role for recombinant coagulation factor VIIa?. Current Hematology Reports 2003;2(2):139‐47. [PubMed] [Google Scholar]
Qureshi 2007 {published data only}
- Qureshi H, Lowe D, Dobson P, Grant‐Casey J, Parris E, Dalton D, et al. National comparative audit of the use of platelet transfusions in the UK. Transfusion Clinique Et Biologique 2007;14(6):509‐13. [DOI] [PubMed] [Google Scholar]
Rabinowitz 2010 {published data only}
- Rabinowitz I. Dose of prophylactic platelet transfusions did not affect bleeding incidence or severity. ACP Journal Club 2010;152(6):11. [DOI] [PubMed] [Google Scholar]
Rayment 2005 {published data only}
- Rayment R, Brunskill SJ, Stanworth S, Soothill PW, Roberts DJ, Murphy MF. Antenatal interventions for fetomaternal alloimmune thrombocytopenia. Cochrane Database of Systematic Reviews 2005, Issue 1. [DOI: 10.1002/14651858.CD004226.pub2] [DOI] [PubMed] [Google Scholar]
Razzaghi 2012 {published data only}
- Razzaghi A, Barkun A. Platelet transfusion threshold in patients with upper gastrointestinal bleeding: a systematic review. Journal of Clinical Gastroenterology 2012;46(6):482‐6. [DOI] [PubMed] [Google Scholar]
Rebulla 2009 {published data only}
- Rebulla P, Grazzini G, Liumbruno GM, Aprili G, Formisano S, Girelli G, et al [The Italian Platelet Technology Assessment Study (IPTAS) Research Group]. Pathogen inactivated platelets and prevention of immunological adverse reactions: the Italian Platelet Technology Assessment Study (IPTAS). Blood Transfusion 2009;7, Suppl 1: 11th European Haemovigilance Seminar:Abstract No. LE08. (Abstract freely available at: http://www.bloodtransfusion.it/articoli/47/en/Doi%200013.pdf. Date accessed: 18 February 2013). [DOI: 10.2450/2009.0013-09] [DOI] [Google Scholar]
Reed 1986 {published data only}
- Reed RL, Ciavarella D, Heimbach DM, Baron L, Pavlin E, Counts RB, et al. Prophylactic platelet administration during massive transfusion. A prospective, randomized, double‐blind clinical study. Annals of Surgery 1986;203(1):40‐8. [DOI] [PMC free article] [PubMed] [Google Scholar]
Roberts 2003 {published data only}
- Roberts IAG, Murray NA. Thrombocytopenia in the newborn. Current Opinion in Pediatrics 2003;15(1):17‐23. [DOI] [PubMed] [Google Scholar]
Roy 1973 {published data only}
- Roy AJ, Jaffe N, Djerassi I. Prophylactic platelet transfusion in children with acute leukemia: A dose response study. Transfusion 1973;13(5):283‐90. [DOI] [PubMed] [Google Scholar]
Sagmeister 1999 {published data only}
- Sagmeister M, Oec L, Gmur J. A restrictive platelet transfusion policy allowing long term support of outpatients with severe aplastic anaemia. Blood 1999;93:3124‐6. [PubMed] [Google Scholar]
Sakakura 2003 {published data only}
- Sakakura M, Wada H. Prevention of hemorrhage occurring in patients with leukemia. Zassh (Nippon‐Naika‐Gakkai‐Zasshi) 2003;92(6):1025‐9. [PubMed] [Google Scholar]
Samama 2005 {published data only}
- Samama CM, Djoudi R, Lecompte T, Nathan DN, Schved JF. Perioperative platelet transfusion: recommendations of the Agence Francaise de Securite Sanitaire des Produits de Sante (AFSSaPS) 2003. Canadian Journal of Anaesthesia 2005;52(1):30‐7. [DOI] [PubMed] [Google Scholar]
- Samama CM, Djoudi R, Lecompte T, Nathan N, Schved JF. Perioperative platelet transfusion. Recommendations of the French Health Products Safety Agency (AFSSAPS) 2003. Minerva Anestesiologica 2006;72(6):447‐52. [PubMed] [Google Scholar]
Schiffer 1983 {published data only}
- Schiffer CA, Dutcher JP, Aisner J, Hogge D, Wiernik PH, Reilly JP, et al. A randomized trial of leukocyte‐depleted platelet transfusion to modify alloimmunization in patients with leukemia. Blood 1983;62:815‐20. [PubMed] [Google Scholar]
Sensebe 2004 {published data only (unpublished sought but not used)}
- Sensebe L, Giraudeau B, Bardiaux L, Deconninck E, Ifrah N, Bidet M‐L, et al. Increasing dose improves the platelet transfusions: results of a prospective multicentre randomised study. Blood 2002;100:(Abstract 2789) 708a. [Google Scholar]
- Sensebe L, Giraudeau B, Baridaux L, Deconinck E, Schmidt A, Bidet ML, et al. The efficiency of transfusing high doses of platelets in hematologic patients with thrombocytopenia: results of a prospective, randomized, open, blinded end point (PROBE) study. Blood 2004;105:862‐4. [DOI] [PubMed] [Google Scholar]
Shanwell 1992 {published data only}
- Shanwell A, Larsson S, Aschan J, Ringden O. A randomized trial comparing the use of fresh and stored platelets in the treatment of bone marrow transplant recipients. European Journal of Haematology 1992;49(2):77‐81. [DOI] [PubMed] [Google Scholar]
Shehata 2009 {published data only}
- Shehata N, Tinmouth A, Naglie G, Freedman J, Wilson K. ABO‐identical versus non‐identical platelet transfusion: a systematic review. Transfusion 2009;49:2442‐53. [DOI] [PubMed] [Google Scholar]
Shen 2007 {published data only}
- Shen Y‐MP, Frenkel EP. Acquired platelet dysfunction. Hematology/Oncology Clinics of North America 2007;21(4):647‐61. [DOI] [PubMed] [Google Scholar]
Singer 1988 {published data only}
- Singer J, Ali AM, Warkentin TE, Blajchman MA, Kelton JG. A prospective randomized study of platelet support in leukemic patients. Transfusion 1988;72(5 Supp):285A. [Google Scholar]
Sintnicolaas 1981 {published data only}
- Sintnicolaas K, Vriesendorp HM, Sizoo W, Stenfert Kroese WF, Haije WG, Hop WC, et al. Delayed alloimmunisation by random single donor platelet transfusions. A randomised study to compare single donor and multiple donor platelet transfusions in cancer patients with severe thrombocytopenia. The Lancet 1981;1(8223):750‐4. [DOI] [PubMed] [Google Scholar]
Sintnicolaas 1982 {published data only (unpublished sought but not used)}
- Sintnicolaas K, Velden K, Sizoo W, Haije WG, Abels J, Lowenberg B. Comparison of prophylactic and therapeutic single‐donor platelet transfusions in patients with acute leukaemia. British Journal of Haematology 1982;50:684. [Google Scholar]
Sintnicolaas 1995 {published data only}
- Sintnicolaas K, Marwijk Kooij M, Prooijen HC, Dijk BA, Putten WL, Claas FH, et al. Leukocyte depletion of random single‐donor platelet transfusions does not prevent secondary human leukocyte antigen‐alloimmunization and refractoriness: A randomized prospective study. Blood 1995;85:824‐8. [PubMed] [Google Scholar]
Slichter 1998 {published data only}
- Slichter SJ, Grabowski M, Townsend‐McCall D, Bolgiano D. Prospective randomized transfusion trial to directly compare fresh and stored apheresis platelets (AP) and pooled random donor platelet concentrates (PC) in thrombocytopenic patients. Blood 1998;92:Abstract. [Google Scholar]
Slichter 2004 {published data only}
- Slichter SJ. Relationship between platelet count and bleeding risk in thrombocytopenic patients. Transfusion Medicine Reviews 2004;18(3):153‐67. [DOI] [PubMed] [Google Scholar]
Slichter 2006 {published data only}
- Slichter SJ, Raife TJ, Davis K, Rheinschmidt M, Buchholz DH, Corash L, et al. Platelets photochemically treated with amotsalen HCl and ultraviolet A light correct prolonged bleeding times in patients with thrombocytopenia. Transfusion 2006;46(5):731‐40. [DOI] [PubMed] [Google Scholar]
Slichter 2007 {published data only}
- Slichter SJ. Evidence‐based platelet transfusion guidelines. Hematology/the Education Program of the American Society of Hematology 2007;2007:172‐8. [DOI] [PubMed] [Google Scholar]
Slichter 2010 {published and unpublished data}
- Assman S, Triulzi DJ, McCullough J, Harrison RW, Slichter SJ. Cost tradeoffs of low‐, medium‐, and high‐dose platelet transfusions. Transfusion 2013;53(Supplement):188A. [Google Scholar]
- Josephson C, Sloan S, Granger S, Castillejo M, Strauss RG, Slichter S, et al. Increased incidence of Grade 2 and higher bleeding in pediatric PLADO trial patients. Transfusion 2009;49(S3):19A‐20A. [Google Scholar]
- Josephson CD, Granger S, Assmann SF, Castillejo M‐I, Strauss RG, Slichter SJ, et al. Bleeding risks are higher in children versus adults given prophylactic platelet transfusions for treatment‐induced hypoproliferative thrombocytopenia. Blood 2012;120(4):748‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kaufman RM, Assmann SF, Triulzi DJ, Strauss RG, Ness P, Granger S, et al. Transfusion‐related adverse events in the platelet dose study. Transfusion 2015;55(1):144‐53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- NCT00128713. Optimal platelet dose strategy for management of thrombocytopenia. http://clinicaltrials.gov/show/NCT00128713 (accessed 16 April 2010).
- Slichter SJ. Background, rationale, and design of a clinical trial to assess the effects of platelet dose on bleeding risk in thrombocytopenic patients. Journal of Clinical Apheresis 2006;21:78‐84. [DOI] [PubMed] [Google Scholar]
- Slichter SJ, Kaufman RM, Assman SF, Brecher ME, Gernsheimer T, Hillyer CD, et al. Effects of prophylactic platelet (Plt) dose on transfusion (Tx) outcomes (PLADO trial). [50th Annual Meeting of the American Society of Hematology]. Blood 2008;112(11):Abstract 285. [Google Scholar]
- Slichter SJ, Kaufman RM, Assmann SF, McCullough J, Triulzi DJ, Strauss RG, et al. Dose of prophylactic platelet transfusions and prevention of haemorrhage. The New England Journal of Medicine 2010;362:600‐13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Triulzi DJ, Assmann SF, Strauss RG, Ness PM, Hess J, Granger S, et al. The effect of platelet characteristics on the platelet increment and HLA alloimmunization in hypoproliferative thrombocytopenia. Transfusion 2010;50(Supplement):3A. [Google Scholar]
- Triulzi DJ, Assmann SF, Strauss RG, Ness PM, Hess JR, Kaufman RM, et al. The impact of platelet transfusion characteristics on post‐transfusion platelet increments and clinical bleeding in patients with hypo‐proliferative thrombocytopenia. Blood 2012;119(23):5553‐62. [DOI] [PMC free article] [PubMed] [Google Scholar]
Slichter 2012 {published data only}
- Slichter SJ. Effects of platelet (Plt) dose on transfusion outcomes. Transfusion Medicine 2012;22:227. [Google Scholar]
Solomon 1978 {published data only}
- Solomon J, Bofenkamp T, Fahey JL, Chillar RK, Beutler E. Platelet prophylaxis in acute non‐lymphoblastic leukemia. The Lancet 1978;1 (8058):267. [DOI] [PubMed] [Google Scholar]
Sosa 2003 {published data only}
- Sosa MEB. Alloimmune thrombocytopenia in the fetus: current management theories. The Journal of Perinatal & Neonatal Nursing 2003;17(3):181‐9. [DOI] [PubMed] [Google Scholar]
Spiess 2004 {published data only}
- Spiess BD, Royston D, Levy JH, Fitch J, Dietrich W, Body S, et al. Platelet transfusions during coronary artery bypass graft surgery are associated with serious adverse outcomes. Transfusion 2004;44(8):1143‐8. [DOI] [PubMed] [Google Scholar]
Stanworth 2013 {published data only}
- Campbell HE, Estcourt LJ, Stokes EA, Llewelyn CA, Murphy MF, Wood EM, et al. TOPPS Study Investigators. Prophylactic platelet transfusions in patients with blood malignancies: cost analysis of a randomized trial. Transfusion 2014;54(10):2394‐403. [DOI] [PubMed] [Google Scholar]
- ISRCTN08758735. A randomised controlled trial of prophylactic versus no‐prophylactic platelet transfusions in patients with haematological malignancies. http://www.controlled‐trials.com/ISRCTN08758735 (accessed 6 February 2010).
- Powter G, Dyer C, Bielby L. Objective assessment of bleeding in patients with haematological malignancies in an international study of platelet transfusions ‐ how was consistency achieved [31st Annual Scientific Meeting of the British Blood Transfusion Society, Birmingham]. Transfusion Medicine 2013;23:46‐7. [Google Scholar]
- Stanworth SJ, Dyer C, Choo L, Bakrania L, Copplestone A, Llewelyn C, et al. Do all patients with hematologic malignancies and severe thrombocytopenia need prophylactic platelet transfusions? Background, rationale, and design of a clinical trial (trial of platelet prophylaxis) to assess the effectiveness of prophylactic platelet transfusions. Transfusion Medicine Reviews 2010;24(3):163‐71. [DOI] [PubMed] [Google Scholar]
- Stanworth SJ, Estcourt L, Powter G, Kahan BC, Dyer C, Bakrania L, et al. The effect of a no‐prophylactic versus prophylactic platelet transfusion strategy on bleeding in patients with hematological malignancies and severe thrombocytopenia (TOPPS trial). A randomized controlled, non‐inferiority trial. Blood 2012;120(Supplement 1):Abstract 1. [Google Scholar]
- Stanworth SJ, Estcourt LJ, Llewelyn CA, Murphy MF, Wood EM, TOPPS Study Investigators. Impact of prophylactic platelet transfusions on bleeding events in patients with hematologic malignancies: a subgroup analysis of a randomized trial. Transfusion 2014;54(10):2385‐93. [DOI] [PubMed] [Google Scholar]
- Stanworth SJ, Estcourt LJ, Powter G, Kahan B, Dyer C, Choo L, et al. A no‐prophylaxis platelet transfusion strategy for hematologic cancers. The New England Journal of Medicine 2013;368(19):1771‐80. [DOI] [PubMed] [Google Scholar]
- Stanworth SJ, Hudson CL, Estcourt LJ, Johnson RJ, Wood EM. Risk of bleeding and use of platelet transfusions in patients with hematologic malignancies: recurrent event analysis. Haematologica 2015;100(6):740‐7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wood EM, Hudson C, Estcourt L, Johnson R, Stanworth SJ. Risk factors for bleeding: A modelling analysis of the TOPPS randomized controlled trial of prophylactic platelet transfusion. Blood 2014;124(21):Abstract. [Google Scholar]
Steffens 2002 {published data only (unpublished sought but not used)}
- Steffens I, Harrison JF, Taylor CPF. A dose response study of platelet transfusion: comparison between triple dose apheresis platelet transfusion and three split standard transfusions. Haematologica 2002;87(Suppl 1):Abstract. [Google Scholar]
Strauss 2004 {published data only}
- Strauss RG. Low‐dose prophylactic platelet transfusions: Time for further study, but too early for routine clinical practice. Transfusion 2004;44(12):1680‐2. [DOI] [PubMed] [Google Scholar]
Strauss 2005 {published data only}
- Strauss RG. Pretransfusion trigger platelet counts and dose for prophylactic platelet transfusions. Current Opinion in Hematology 2005;12(6):499‐502. [DOI] [PubMed] [Google Scholar]
Strindberg 1996 {published data only}
- Strindberg J, Berlin G. Transfusion of platelet concentrates ‐ clinical evaluation of two preparations. European Journal of Haematology 1996;57(4):307‐11. [DOI] [PubMed] [Google Scholar]
Sweeney 2000 {published data only}
- Sweeney JD, Kouttab NM, Penn CL, McHugh KE, Nelson EJ, Oblon DJ. A comparison of prestorage WBC‐reduced whole blood derived platelets in autologous progenitor cell transplant. Transfusion 2000;40(7):794‐800. [DOI] [PubMed] [Google Scholar]
Tinmouth 2003 {published data only}
- Tinmouth AT, Freedman J. Prophylactic platelet transfusions: which dose is the best dose? A review of the literature. Transfusion Medicine Reviews 2003;17(3):181‐93. [DOI] [PubMed] [Google Scholar]
Tinmouth 2004 {published and unpublished data}
- Tinmouth A, Kotchetkova N, Tomlinson G, Crump M, Brandwein J, Tannock I, et al. A randomised phase II trial of low dose and standard dose platelet transfusions during induction therapy for acute leukemia or autologous stem cell transplantation. Vox Sanguinis 2002;83(Suppl 1):8. [Google Scholar]
- Tinmouth A, Tannock IF, Crump M, Tomlinson G, Brandwein J, Minden M, et al. Low‐dose prophylactic platelet transfusions in recipients of an autologous peripheral blood progenitor transplant and patients with acute leukaemia: a randomized controlled trial with a sequential Bayesian design. Transfusion Medicine 2004;44:1711‐9. [DOI] [PubMed] [Google Scholar]
Tosetto 2009 {published data only}
- Tosetto A, Balduini CL, Cattaneo M, Candia E, Mariani G, Molman AC, et al. Management of bleeding and of invasive procedures in patients with platelet disorders and/or thrombocytopenia: Guidelines of the Italian Society for Haemostasis and Thrombosis (SISET). Thrombosis Research 2009;125(5):e13‐8. [DOI] [PubMed] [Google Scholar]
TRAP 1997 {published data only}
- Enright H, Davis K, Gernsheimer T, McCullough JJ, Woodson R, Slichter SJ. Factors influencing moderate to severe reactions to PLT transfusions: experience of the TRAP multicenter clinical trial. Transfusion 2003;43(11):1545‐52. [DOI] [PubMed] [Google Scholar]
- Slichter SJ, Davis K, Enright H, Braine H, Gernsheimer T, Kao KJ, et al. Factors affecting posttransfusion platelet increments, platelet refractoriness, and platelet transfusion intervals in thrombocytopenic patients. Blood 2005;105(10):4106‐14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- The Trial to Reduce Alloimmunization to Platelets Study Group. Leukocyte reduction and ultraviolet B irradiation of platelets to prevent alloimmunization and refractoriness to platelet transfusions. The New England Journal of Medicine 1997;337:1861‐70. [DOI] [PubMed] [Google Scholar]
Vadhan‐Raj 2002 {published data only}
- Vadhan‐Raj S, Kavanagh JJ, Freedman RS, Folloder J, Currie LM, Bueso‐Ramos C, et al. Safety and efficacy of transfusions of autologous cryopreserved platelets derived from recombinant human thrombopoietin to support chemotherapy‐associated severe thrombocytopenia: a randomised cross‐over study. The Lancet 2002;359:2145‐52. [DOI] [PubMed] [Google Scholar]
Van Marwijk 1991 {published data only}
- Marwijk KM, Prooijen HC, Moes M, Bosma‐stants I, Akkerman JW. Use of leukocyte‐depleted platelet concentrates for the prevention of refractoriness and primary HLA alloimmunization: A prospective, randomized trial. Blood 1991;77:201‐5. [PubMed] [Google Scholar]
van Rhenen 2003 {published data only}
- Cazenave JP, Davis K, Corash L. Design of clinical trials to evaluate the efficacy of platelet transfusion: the euroSPRITE trial for components treated with Helinx technology. Seminars in Hematology 2001;38(4 Supp 11):46‐54. [DOI] [PubMed] [Google Scholar]
- Cazenave JP, Rhenen D, Gulliksson H, Pamphilon D, Ljungman P, Davis K, et al. INTERCEPT buffy coat platelets (IPC) are effective during multiple episodes of thrombocytopenia: the EUROSPRITE trial. Transfusion Clinique et Biologique 2001;8(Supp 1):Various. [Google Scholar]
- Ljungman P, Rhenen D, Pamphilon D, Metzel P, Marblie S, Lin J, et al. Results of the EUROSPRITE phase III trial: INTERCEPT buffy coat platelet concentrates (IPC) provide effective hemostasis for thrombocytopenic (TCP) patients (PTS). Transfusion Clinique et Biologique 2001;8(Supp 1):100s. [Google Scholar]
- Pamphilon D, Buchholz DH, Cazenave JP, Conlan M, Corash L, Davis K, et al. The EUROSPRITE phase III trial of INTERCEPT buffy coat platelet concentrates (IPC) demonstrates IPC are safe when transfused to thrombocytopenic (TCP) patients (PTS). Transfusion Clinique et Biologique 2001;8(Supp 1):100‐1s. [Google Scholar]
- Rhenen D, Gulliksson H, Cazenave JP, Pamphilon D, Ljungman P, Kluter H, et al. Transfusion of pooled buffy coat platelet components prepared with photochemical pathogen inactivation treatment: the euroSPRITE trial. Blood 2003;101(6):2426‐33. [DOI] [PubMed] [Google Scholar]
Velik‐Salchner 2007 {published data only}
- Velik‐Salchner C, Haas T, Innerhofer P, Streif W, Nussbaumer W, Klingler A, et al. The effect of fibrinogen concentrate on thrombocytopenia. Journal of Thrombosis and Haemostasis 2007;5(5):1019‐25. [DOI] [PubMed] [Google Scholar]
Verma 2008 {published data only}
- Verma A, Pandey P, Khetan D, Chaudhary R. Platelet transfusions in clinical practice at a multidisciplinary hospital in North India. Transfusion and Apheresis Science 2008;39(1):29‐35. [DOI] [PubMed] [Google Scholar]
Wandt 1998 {published data only}
- Wandt H, Frank M, Ehninger G, Schneider C, Brack N, Daoud A, et al. Safety and cost effectiveness of a 10 x 109/L trigger for prophylactic platelet transfusions compared with the traditional 20 x 109/L trigger: a prospective comparative trial in 105 patients with acute myeloid leukaemia. Blood 1998;91:3601‐6. [PubMed] [Google Scholar]
- Wandt H, Frank M, Link H, Schneider C, Brack N, Daoud A, et al. The 10/NL trigger for prophylactic platelet transfusion in AML: a prospective comparative multicenter study. Annals of Hematology 1995;70(Suppl 1):A140. [Google Scholar]
Wandt 2005 {published data only}
- Wandt H, Frank M, Schaefer‐Eckart K, Wilhelm M. Routine prophylactic platelet transfusions are not necessary in patients with acute myeloid leukaemia. A therapeutic transfusion strategy is safe. Blood 2005;106(11):Abstract. [Google Scholar]
- Wandt H, Reinel H, Schaefer‐Eckart K, Wilhelm M, Birkmann J, Gallmeier WM. New strategy for platelet transfusion for patients with acute myeloid leukaemia: routine prophylactic transfusion replaced by therapeutic transfusion. Blood 2002;100((Abstract 2782)):706a. [Google Scholar]
Wandt 2006 {published data only}
- Wandt H, Schaefer‐Eckart K, Frank M, Birkmann J, Wilhelm M. A therapeutic platelet transfusion strategy is safe and feasible in patients after autologous peripheral blood stem cell transplantation. Bone Marrow Transplant 2006;37(4):387‐92. [DOI] [PubMed] [Google Scholar]
Wandt 2010 {published data only}
- Wandt H. Indication for platelet transfusion in patients with haematological disease: less is more. [German]. Deutsche Medizinische Wochenschrift 2010;135(38):1877‐9. [DOI] [PubMed] [Google Scholar]
Wandt 2012 {published data only}
- NCT00521664. A trial comparing a prophylactic with a therapeutic platelet strategy in two groups. http://clinicaltrials.gov/show/NCT00521664 (accessed 4 January 2010).
- Schaefer‐Eckart K, Wendelin K, Pilz B, Kramer M, Ehninger G, Wilhelm M, et al. Consolidation therapy is associated with significantly lower bleeding risk compared to induction therapy in patients with acute myeloid leukemia. Blood 2014;124(21):Abstract. [Google Scholar]
- Schaefer‐Eckart K, Wendelin K, Wilhelm M, Mahlknecht U, Conradi R, Schaich M, et al. Interim analysis of a prospective randomised study comparing a therapeutic platelet strategy with the prophylactic platelet transfusion standard in patients after autologous peripheral stem cell transplantation (ASCT) [48th Annual Meeting of the American Society of Hematology]. Blood 2006;108(11):Abstract. [Google Scholar]
- Wandt H, Schaefer‐Eckart K, Pilz B, Thalheimer M, Ho A, Schaich M, et al. Experience with a therapeutic platelet transfusion strategy in patients with acute myeloid leukemia. Final results of a randomized multicenter study comparing a prophylactic with a therapeutic transfusion strategy. Onkologie 2010;33(6):Abstract. [Google Scholar]
- Wandt H, Schaefer‐Eckart K, Pilz B, Thalheimer M, Ho AD, Schaich M, et al. Experience with a therapeutic platelet transfusion strategy in acute myeloid leukaemia: Preliminary results of a randomised multicenter study after enrolment of 175 patients [51st ASH Meeting and Exposition]. Blood 2009;11(Supplement):Abstract. [Google Scholar]
- Wandt H, Schaefer‐Eckart K, Wendelin K, Pilz B, Wilhelm M, Thalheimer M, et al. Therapeutic platelet transfusion versus routine prophylactic transfusion in patients with haematological malignancies: an open‐label, multicentre, randomised study. The Lancet 2012;380(9850):1309‐16. [DOI] [PubMed] [Google Scholar]
- Wandt H, Schäfer‐Eckart K, Wendelin K, Rottmann M, Thalmeimer M, Schubert MS, et al. A therapeutic platelet transfusion strategy without routine prophylactic transfusion is feasible and safe and reduces platelet transfusion numbers significantly: final analysis of a randomised study after high‐dose chemotherapy and PBSCT. Bone Marrow Transplantation 2009;43 Supp 1:S23. [Google Scholar]
- Wandt H, Wendelin K, Schaefer‐Eckart K, Thalheimer M, Schubert MS, Conradi R, et al. Therapeutic platelet transfusion strategy without routine prophylactic transfusion is feasible and safe and reduces platelet transfusion numbers significantly: preliminary analysis of a randomized study in patients after high dose chemotherapy and autologous peripheral blood stem cell transplantation. Blood (ASH Annual Meeting Abstracts) 2008;112:Abstract 286. [Google Scholar]
Wang 2002 {published data only}
- Wang SE, Lara PN, Lee OA, Reed J, Wang LR, Palmer P, et al. Acetaminophen and diphenhydramine as premedication for platelet transfusions: a prospective randomized double‐blind placebo‐controlled trial. American Journal of Hematology 2002;70(3):191‐4. [DOI] [PubMed] [Google Scholar]
Wang 2005 {published data only}
- Wang XQ. Using evidence‐based guideline for prophylactic platelet transfusion in patient with myelodysplastic syndrome. Chinese Journal of Evidence‐Based Medicine 2005;5(6):482‐4. [Google Scholar]
Weigand 2009 {published data only}
- Weigand K, Encke J, Meyer FJ, Hinkel UP, Munder M, Stremmel W, et al. Low levels of prothrombin (INR) and platelets do not increase the risk of significant bleeding when placing central venous catheters. Medizinische Klinik 2009;104(5):331‐5. [DOI] [PubMed] [Google Scholar]
Williamson 1994 {published data only}
- Williamson LM, Wimperis JZ, Williamson P, Copplestone JA, Gooi HC, Morgenstern GR, et al. Bedside filtration of blood products in the prevention of HLA alloimmunization: A prospective randomized study. Alloimmunization Study Group. Blood 1994;83:3028‐35. [PubMed] [Google Scholar]
Woodard 2002 {published data only}
- Woodard P, Lubin B, Walters CMC. New approaches to hematopoietic cell transplantation for hematological diseases in children. Pediatric Clinics of North America 2002;49(5):989‐1007. [DOI] [PubMed] [Google Scholar]
Zahur 2002 {published data only}
- Zahur UR, Alam M. Platelet transfusion practice in a tertiary care hospital. Medical Forum Monthly 2002;13(7):27‐9. [Google Scholar]
Zeller 2014 {published data only}
- Zeller MP, Al‐Habsia KS, Heddle NM. Prophylactic platelet transfusions: should they be a treatment of the past?. Current Opinion in Hematology 2014;21(6):521‐7. [DOI] [PubMed] [Google Scholar]
Zhao 2002 {published data only}
- Zhao SM, Cheng XL, Hu J, Xiang GC, Zhang JS, Li RQ. Clinical assessment of preventing febrile nonhemolytic transfusion reaction by leucocyte depleted blood transfusion. Zhongguo Shi Yan Xue Ye Xue Za Zhi 2002;10(6):568‐70. [PubMed] [Google Scholar]
Zumberg 2002 {published and unpublished data}
- Zumberg MS, Rosario ML, Pollock BH, Nejame CF, Allen LS, Boyette R, et al. A prospective randomized trial of prophylactic platelet transfusion d bleeding incidence in hematopoietic stem cell transplant (HSCT) recipients: 10,000µL vs. an 20,000 µL threshold [abstract]. 37th Annual Meeting of the American Society of Clinical Oncology, 2001 May 12‐15; San Fransisco. San Francisco: American Society of Clinical Oncology, 2001.
- Zumberg MS, Roario ML, Nejame CF, Pollock BH, Garzarella L, Kao KJ, et al. A prospective randomized trial of prophylactic platelet transfusion and bleeding incidence in hematopoietic stem cell transplant recipients: 10,000/µL versus 20,000/µL trigger. Biology of Blood and Marrow Transplantation 2002;8:569‐76. [DOI] [PubMed] [Google Scholar]
Additional references
Ajani 1990
- Ajani JA, Welsh SR, Raber MN. Comprehensive criteria for assessing therapy‐induced toxicity. Cancer Investigation 1990;8:141‐53. [DOI] [PubMed] [Google Scholar]
BCSH 2003
- British Committee for Standards in Haematology (BCSH). Guidelines for the use of platelet transfusions. British Journal of Haematology 2003;122:10‐23. [DOI] [PubMed] [Google Scholar]
BCSH 2004
- British Committee for Standards in Haematology (BCSH). Transfusion guidelines for neonates and older children. British Journal of Haematology 2004;124(4):433‐53. [DOI] [PubMed] [Google Scholar]
Benson 2009
- Benson AB, Moss M, Silliman CC. Transfusion‐related acute lung injury (TRALI): a clinical review with emphasis on the critically ill. British Journal of Haematology 2009;147(4):431‐43. [DOI] [PMC free article] [PubMed] [Google Scholar]
Beutler 1993
- Beutler E. Platelet transfusions: the 20,000/μL trigger. Blood 1993;81:1411‐3. [PubMed] [Google Scholar]
Blumberg 2009
- Blumberg N, Spinelli SL, Francis CW, Taubman MB, Phipps RP. The platelet as an immune cell ‐ CD40 ligand and transfusion immune modulation. Immunology Research 2009;45:251‐60. [DOI] [PMC free article] [PubMed] [Google Scholar]
Board 2009
- The Board of the German Medical Association on the Recommendation of the Scientific Advisory Board. Platelet concentrates. Cross‐sectional guidelines for therapy with blood components and plasma derivatives. Transfusion Medicine and Hemotherapy 2009;36:372‐82. [Google Scholar]
Bolton‐Maggs 2012
- Bolton‐Maggs PHB (Ed) and H Cohen on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group. The 2011 Annual SHOT Report. Serious Hazards of Transfusion (SHOT), 2012. [Google Scholar]
Burnett 2011
- Burnett AK, Hills RK, Milligan D, Kjeldsen L, Kell J, Russell NH, et al. Identification of patients with acute myeloblastic leukemia who benefit from the addition of gemtuzumab ozogamicin: results of the MRC AML15 trial. Journal of Clinical Oncology 2011;29(4):369‐77. [DOI] [PubMed] [Google Scholar]
Butler 2013
- Butler C, Doree C, Estcourt LJ, Trivella M, Hopewell S, Brunskill SJ, et al. Pathogen‐reduced platelets for the prevention of bleeding. Cochrane Database of Systematic Reviews 2013, Issue 3. [DOI: 10.1002/14651858.CD009072] [DOI] [PubMed] [Google Scholar]
Cancer Research UK 2013
- Cancer Research UK. Percentage change in European age‐standardised three year average incidence rates, males, UK, 1991‐2001 and 2008‐2010. Cancer Research UK statistics at http://www.cancerresearchuk.org/cancer‐info/cancerstats/ (accessed 14 February 2013).
CDC 2012
- CDC (Centers for Disease Control and Prevention). United States Cancer Statistics. National Program of Cancer Registries (NPCR) http://www.cdc.gov/cancer/npcr/ 2012 (accessed 14 February 2013).
Coleman 2004
- Coleman MP, Rachet B, Woods LM, Mitry E, Riga M, Cooper N, et al. Trends and socioeconomic inequalities in cancer survival in England and Wales up to 2001. British Journal of Cancer 2004;90(7):1367‐73. [DOI] [PMC free article] [PubMed] [Google Scholar]
Cook 2004
- Cook RJ, Heddle NM, Rebulla P, Sigouin CS, Webert KE. Methods for the analysis of bleeding outcomes in randomized trials of platelet transfusion triggers. Transfusion 2004;44:1135‐42. [DOI] [PubMed] [Google Scholar]
De la Serna 2008
- Serna J, Montesinos P, Vellenga E, Rayon C, Parody R, Leon A, et al. Causes and prognostic factors of remission induction failure in patients with acute promyelocytic leukemia treated with all‐trans retinoic acid and idarubicin. Blood 2008;111(7):3395‐402. [DOI] [PubMed] [Google Scholar]
Deeks 2011
- Deeks JJ, Higgins JPT, Altman DG (editors). Chapter 9: Analysing data and undertaking meta‐analyses. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Duke 1910
- Duke WW. The relation of blood platelets to hemorrhagic disease. Description of a method for determining the bleeding time and coagulation time and report of 3 cases of hemorrhagic disease relieved by transfusion. Journal of the American Medical Association 1910;55:1185‐92. [Google Scholar]
Estcourt 2011
- Estcourt LJ, Stanworth SJ, Murphy MF. Platelet transfusions for patients with haematological malignancies: who needs them?. British Journal of Haematology 2011;154(4):425‐40. [DOI] [PubMed] [Google Scholar]
Estcourt 2012b
- Estcourt LJ, Birchall J, Lowe D, Grant‐Casey J, Rowley M, Murphy MF. Platelet transfusions in haematology patients: are we using them appropriately?. Vox Sanguinis 2012;103(4):284‐93. [DOI] [PubMed] [Google Scholar]
Estcourt 2013
- Estcourt LJ, Heddle N, Kaufman RM, McCullough J, Murphy MF, Slichter S, et al. On behalf of the BEST (Biomedical Excellence for Safer Transfusion) Collaborative. The challenges of measuring bleeding outcomes in clinical trials of platelet transfusions. Transfusion 2013;53(7):1531‐43. [DOI] [PubMed] [Google Scholar]
Estcourt 2014a
- Estcourt LJ, Stanworth S, Doree C, Trivella M, Hopewell S, Murphy MF, et al. Different doses of prophylactic platelet transfusion for preventing bleeding in patients with haematological disorders after chemotherapy or stem cell transplantation. Cochrane Database of Systematic Reviews 2014, Issue 3. [DOI: 10.1002/14651858.CD010984] [DOI] [PMC free article] [PubMed] [Google Scholar]
Estcourt 2014b
- Estcourt LJ, Gregg R, Stanworth S, Doree C, Trivella M, Murphy MF, et al. Alternative agents versus prophylactic platelet transfusion for preventing bleeding in patients with haematological disorders after chemotherapy or stem cell transplantation. Cochrane Database of Systematic Reviews 2014, Issue 3. [DOI: 10.1002/14651858.CD010982] [DOI] [PMC free article] [PubMed] [Google Scholar]
Estcourt 2014d
- Estcourt LJ, Crighton GL, Wood EM, Stanworth S, Trivella M, Doree C, et al. A therapeutic‐only versus prophylactic platelet transfusion strategy for preventing bleeding in patients with haematological disorders after chemotherapy or stem cell transplantation. Cochrane Database of Systematic Reviews 2014, Issue 3. [DOI: 10.1002/14651858.CD010981] [DOI] [PMC free article] [PubMed] [Google Scholar]
Estcourt 2014e
- Estcourt LJ, Pinchon D, Symington E, Kelly AM, Doree C, Brunskill S, et al. Does bleeding affect patient reported outcome measures in patients with myelodysplasia or hematologic malignancies: a systematic review. Transfusion 2014;54(4):1166‐79. [DOI: 10.1111/trf.12441] [DOI] [PubMed] [Google Scholar]
Fielding 2007
- Fielding AK, Richards SM, Chopra R, Lazarus HM, Litzow MR, Buck G, et al. Outcome of 609 adults after relapse of acute lymphoblastic leukemia (ALL); an MRC UKALL12/ECOG 2993 study. Blood 2007;109(3):944‐50. [PUBMED: 17032921] [DOI] [PubMed] [Google Scholar]
Freedman 1989
- Freedman L, Sylvester R, Byar DP. Using permutation tests and bootstrap confidence limits to analyze repeated events data from clinical trials. Controlled Clinical Trials 1989;10:129‐41. [DOI] [PubMed] [Google Scholar]
Gaydos 1962
- Gaydos LA, Freireich EJ, Mantel N. The quantitative relation between platelet count and hemorrhage in patients with acute leukaemia. The New England Journal of Medicine 1962;266:905‐9. [DOI] [PubMed] [Google Scholar]
GRADE 2014 [Computer program]
- McMaster University. GRADEpro [www.gradepro.org]. McMaster University, 2015.
Gratwohl 2010
- Gratwohl A, Baldomero H, Aljurf M, Pasquini MC, Bouzas LF, Yoshimi A, et al. Hematopoietic stem cell transplantation: a global perspective. JAMA 2010;303(16):1617‐24. [DOI] [PMC free article] [PubMed] [Google Scholar]
Harrison 2001
- Harrison P, Ault KA, Chapman S, Charie L, Davis B, Fujimoto K, et al. An interlaboratory study of a candidate reference method for platelet counting. American Journal of Clinical Pathology 2001;115:448‐59. [DOI] [PubMed] [Google Scholar]
Heddle 2008
- Heddle NM, Arnold DM, Boye D, Webert KE, Resz I, Dumont LJ. Comparing the efficacy and safety of apheresis and whole blood‐derived platelet transfusions: a systematic review. Transfusion 2008;48(7):1447‐58. [DOI] [PubMed] [Google Scholar]
Heddle 2009a
- Heddle NM, Cook RJ, Tinmouth A, Kouroukis CT, Hervig T, Klapper E, et al. A randomized controlled trial comparing standard and low dose strategies for transfusion of platelets (SToP) to patients with thrombocytopenia. Blood 2009;113(7):1564‐73. [DOI] [PubMed] [Google Scholar]
Heddle 2009b
- Heddle NM, Webbert K. Investigation of acute transfusion reactions. In: Murphy MF, Pamphilion DH editor(s). Practical Transfusion Medicine. 4th Edition. Blackwell, 2009:63‐89. [Google Scholar]
Higgins 2011a
- Higgins JPT, Deeks JJ (editors). Chapter 7: Selecting studies and collecting data. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Higgins 2011b
- Higgins JPT, Deeks JJ, Altman DG (editors). Chapter 16: Special topics in statistics. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Higgins 2011c
- Higgins JPT, Altman DG, Sterne JAC (editors). Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Knowles 2011
- Knowles S (Ed), Cohen H, on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group. The 2010 Annual SHOT Report. Serious Hazards of Transfusion (SHOT), 2011. [Google Scholar]
Koreth 2004
- Koreth R, Weinert C, Weisdorf DJ, Key NS. Measurement of bleeding severity: a critical review. Transfusion 2004;44:605‐17. [DOI] [PubMed] [Google Scholar]
Kumar 2014
- Kumar A, Mhaskar R, Grossman BJ, Kaufman RM, Tobian AAR, Kleinman S, et al. Platelet transfusion: a systematic review of the clinical evidence. Transfusion 2015;55(5):1116‐27. [DOI] [PubMed] [Google Scholar]
Lefebvre 2011
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
NBA 2012
- National Blood Authority. The National Blood Authority’s Patient Blood Management Guideline: Module 3 – Medical. National Blood Authority, 2012. [Google Scholar]
ONS 2012
- Office for National Statistics. Cancer incidence and mortality tables and charts. http://www.ons.gov.uk/ons/index.html 2012 (accessed 14 February 2013), issue tcm77‐259491.
Parmar 1998
- Parmar MK, Torri V, Stewart L. Extracting summary statistics to perform meta‐analyses of the published literature for survival endpoints. Statistics in Medicine 1998;17(24):2815‐34. [DOI] [PubMed] [Google Scholar]
Passweg 2012
- Passweg JR, Baldomero H, Gratwohl A, Bregni M, Cesaro S, Dreger P, et al. The EBMT activity survey: 1990‐2010. Bone Marrow Transplant 2012;47(7):906‐23. [DOI] [PubMed] [Google Scholar]
Patel 2009
- Patel B, Kirkland K, Szydlo R, Pearce R, Clark R, Craddock C, et al. Favorable outcomes with alemtuzumab‐conditioned unrelated donor stem cell transplantation in adults with high‐risk Philadelphia chromosome‐negative acute lymphoblastic leukemia in first complete remission. Haematologica 2009;94:1399‐406. [DOI] [PMC free article] [PubMed] [Google Scholar]
Pavenski 2013
- Pavenski K, Rebulla P, Duquesnoy R, Saw CL, Slichter SJ, Tanael S, et al. International Collaboration for Guideline Development, Implementation. Evaluation for Transfusion Therapies, Collaborators. Efficacy of HLA‐matched platelet transfusions for patients with hypoproliferative thrombocytopenia: a systematic review. Transfusion 2013;53:2230‐42. [DOI: 10.1111/trf.12175] [DOI] [PubMed] [Google Scholar]
Pearce 2011
- Pearce S, Rowe GP, Field SP. Screening of platelet for bacterial contamination at the Welsh Blood Service. Transfusion Medicine 2011;21(1):25‐32. [DOI] [PubMed] [Google Scholar]
Pendry 2011
- Pendry K, Davies T. An audit of use and wastage in the north west of England and North Wales: where have all the platelets gone?. Blood and Transplant Matters 2011;34:17‐9. [Google Scholar]
Popovsky 1985
- Popovsky MA, Moore SB. Diagnostic and pathogenetic considerations in transfusion‐related acute lung injury. Transfusion 1985;25:573‐7. [DOI] [PubMed] [Google Scholar]
Rachet 2009
- Rachet B, Maringe C, Nur U, Quaresma M, Shah A, Woods LM, et al. Population‐based cancer survival trends in England and Wales up to 2007: an assessment of the NHS cancer plan for England. The Lancet Oncology 10;4:351‐69. [DOI] [PubMed] [Google Scholar]
Review Manager 5.3 [Computer program]
- The Nordic Cochrane Centre. Review Manager (RevMan). Version 5.3. Copenhagen: The Cochrane Collaboration, 2014.
Rysler 2010
- Rysler C, Stoffel N, Buser A, Gratwohl A, Tsakiris DA, Stern M. Effect of beta‐blockers, Ca2+antagonists, and benzodiazepines on bleeding incidence in patients with chemotherapy induced thrombocytopenia. Platelets 2010;21(1):77‐83. [DOI] [PubMed] [Google Scholar]
Sacco 2010
- Sacco JJ, Botten J, Macbeth F, Bagust A, Clark P. The average body surface area of adult cancer patients in the UK: a multicentre retrospective study. PLoS One 2010;5(1):e8933. [DOI: 10.1371/journal.pone.0008933] [DOI] [PMC free article] [PubMed] [Google Scholar]
Schiffer 2001
- Schiffer CA, Anderson KC, Bennett CL, Bernstein S, Elting LS, Goldsmith M, et al. Platelet transfusion for patients with cancer: clinical practice guidelines of the American Society of Clinical Oncology. Journal of Clinical Oncology 2001;19:1519‐38. [DOI] [PubMed] [Google Scholar]
Schünemann 2011
- Schünemann HJ, Oxman AD, Higgins JPT, Vist GE, Glasziou P, Guyatt GH. Chapter 11: Presenting results and 'Summary of findings' tables. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Segal 2005
- Segal HC, Briggs C, Kunka S, Casbard A, Harrison P, Machin SJ, et al. Accuracy of platelet counting haematology analysers in severe thrombocytopenia and potential impact on platelet transfusion. British Journal of Haematology 2005;128:520‐5. [DOI] [PubMed] [Google Scholar]
Silliman 2003
- Silliman CC, Boshkov LK, Mehdizadehkashi Z, Elzi DJ, Dickey WO, Podlosky L, et al. Transfusion‐related acute lung injury: epidemiology and a prospective analysis of etiologic factors. Blood 2003;101(2):454‐62. [DOI] [PubMed] [Google Scholar]
Slichter 1978
- Slichter SJ, Harker LA. Thrombocytopenia: mechanisms and management of defects in platelet production. Clinical Haematology 1978;7:523‐39. [PubMed] [Google Scholar]
Slichter 1980
- Slichter SJ. Controversies in platelet transfusion therapy. Annual Reviews of Medicine 1980;31:509‐40. [DOI] [PubMed] [Google Scholar]
Slichter 2005
- Slichter SJ, Davis K, Enright H, Braine H, Gernsheimer T, Kao KJ, et al. Factors affecting posttransfusion platelet increments, platelet refractoriness, and platelet transfusion intervals in thrombocytopenic patients. Blood 2005;105:4106‐14. [DOI] [PMC free article] [PubMed] [Google Scholar]
Stanworth 2010
- Stanworth SJ, Dyer C, Choo L, Bakrania L, Copplestone A, Llewelyn C, et al. Do all patients with hematologic malignancies and severe thrombocytopenia need prophylactic platelet transfusions? Background, rationale, and design of a clinical trial (trial of platelet prophylaxis) to assess the effectiveness of prophylactic platelet transfusions. Transfusion Medicine Reviews 2010;24(3):163‐71. [DOI] [PubMed] [Google Scholar]
Sterne 2011
- Sterne JAC, Egger M, Moher D (editors). Chapter 10: Addressing reporting biases. In: Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Intervention. Version 5.1.0 (updated March 2011). The Cochrane Collaboration, 2011. Available from www.cochrane‐handbook.org.
Sullivan 2002
- Sullivan MT, McCullough J, Schreiber GB, Wallace EL. Blood collection and transfusion in the United States in 1997. Transfusion 2002;42(10):1253‐60. [DOI] [PubMed] [Google Scholar]
Taylor 2010
- Taylor C (Ed), Cohen H, Mold D, Jones H, et al. on behalf of the Serious Hazards of Transfusion (SHOT) Steering Group. The 2009 Annual SHOT Report. SHOT Steering Group, 2010. [Google Scholar]
Tierney 2007
- Tierney JF, Stewart LA, Ghersi D, Burdett S, Sydes MR. Practical methods for incorporating summary time‐to‐event data into meta‐analysis. Trials 2007; Vol. 8, issue 16. [DOI: 10.1186/1745-6215-8-16] [DOI] [PMC free article] [PubMed]
Tinmouth 2007
- Tinmouth AT. Chapter 18: Platelet transfusion, alloimmunization and management of platelet refractoriness. Canadian Blood Services. 4th Edition. Canadian Blood Services, 2007. [Google Scholar]
Verma 2009
- Verma A, Agarwal P. Platelet utilization in the developing world: strategies to optimize platelet transfusion practices. Transfusion and Apheresis Science 2009;41(2):145‐9. [DOI] [PubMed] [Google Scholar]
WHO 1979
- World Health Organization. WHO Handbook for Reporting Results of Cancer Treatment. WHO Offset publication No. 48. Geneva: World Health Organization, 1979. [Google Scholar]
Zisk 2014
- Zisk JL, Mackley A, Clearly G, Chang E, Christensen RD, Paul DA. Transfusing neonates based on platelet count vs. platelet mass: a randomized feasibility‐pilot study. Platelets 2014;25(7):513‐6. [DOI] [PubMed] [Google Scholar]
References to other published versions of this review
Estcourt 2012a
- Estcourt L, Stanworth SJ, Doree C, Hopewell S, Murphy MF, Tinmouth A, et al. Prophylactic platelet transfusion for prevention of bleeding in patients with haematological disorders after chemotherapy and stem cell transplantation. Cochrane Database of Systematic Reviews 2012, Issue 5. [DOI: 10.1002/14651858.CD004269.pub3] [DOI] [PubMed] [Google Scholar]
Estcourt 2014c
- Estcourt LJ, Stanworth S, Doree C, Trivella M, Hopewell S, Murphy MF, et al. Comparison of different platelet count thresholds to guide administration of prophylactic platelet transfusion for preventing bleeding in patients with haematological disorders after chemotherapy or stem cell transplantation. Cochrane Database of Systematic Reviews 2014, Issue 3. [DOI: 10.1002/14651858.CD010983] [DOI] [PMC free article] [PubMed] [Google Scholar]
Stanworth 2004
- Stanworth SJ, Hyde C, Heddle N, Rebulla P, Brunskill S, Murphy MF. Prophylactic platelet transfusion for haemorrhage after chemotherapy and stem cell transplantation. Cochrane Database of Systematic Reviews 2004, Issue 4. [DOI: 10.1002/14651858.CD004269.pub2] [DOI] [PubMed] [Google Scholar]