

INTRODUCTION
Ear surgeons are increasingly concerned about protecting the chorda tympani nerve while avoiding injury to the facial nerve during cochlear implant surgery. The chorda tympani nerve is the sensory branch of the facial nerve and carries taste information and general sensation (e.g., pain and temperature) from the anterior two-thirds of the tongue. It supplies efferent vasodilator fibers to the tongue and secretomotor fibers to the salivary glands in the floor of the mouth and parotid gland.
The chorda tympani nerve is the largest branch of the facial nerve in the intrapetrous compartment; it splits from the facial nerve just before it exits via the stylomastoid foramen. It arises below the nerve to the stapedius and traverses anterosuperiorly via the posterior canaliculus, usually accompanied by the posterior tympanic branch of the stylomastoid artery. This canaliculus opens into the middle ear cavity through an aperture situated at the junction of the posterior and lateral walls of the tympanic cavity. This opening lies just medial to the fibrocartilaginous annulus, and the posterior canaliculus is roughly 0.5 mm in diameter.
The chorda tympani nerve courses through the middle ear and is thus susceptible to damage during ear surgeries, such as stapedectomy[1] and cochlear implantation.[2] Following chorda tympani nerve damage, taste buds disappear from the denervated side of the tongue[3] and taste loss or distortion can occur. Although the peripherally injured chorda tympani nerve usually regenerates to successfully reinnervate taste buds within several weeks,[4] persistent dysgeusia (i.e., taste alteration) can last for months or years[5] and may indicate alterations in central nervous system (CNS) function.
Loundon et al.[6] reported that facial and chorda tympani nerve injury occurred in 1 of 434 (0.23%) cochlear implantation surgeries. Of the 1402 cases from Department of Otorhinolaryngology Head and Neck Surgery of Beijing Friendship Hospital, temporary facial nerve injury was noted in 4 (0.28%) cases, and injury to the posterior wall of the external auditory canal was reported in 14 (0.99%) cases.[7] Here, we described our experience regarding performing cochlear implantation surgery in 180 patients with a profound sensorineural hearing loss by affixing the facial and chorda tympani nerves to the bony wall to maintain their integrity.
METHODS
Subjects
From February 2013 to April 2014, 180 patients (180 ears, 116 males and 64 females) with profound sensorineural hearing loss underwent successful cochlear implantation with no damage to the chorda tympani nerve in Department of Otorhinolaryngology Head and Neck Surgery of Beijing Friendship Hospital. All the patients in this study provided the written informed consent. The study has been approved by the Research Ethics Committee of Beijing Friendship Hospital (BJFH-EC/2013-075). The age range was from 3 to 21 years, and the average age was 13.8 years. All patients presented with hearing loss, including five patients who previously suffered from common cold and high fever, and three patients with a history of umbilical cord around the neck in the 35th week of gestation who were delivered via cesarean due to placenta previa. None of the patients had residual hearing with type A tympanogram, a stapedius muscle reflex in tympanometry, or otoacoustic emissions. All patients had worn hearing aids for at least 6 months but did not obtain any benefit. Twenty-six patients were implanted with Cochlear CI24R CA implants (COCHLEAR, Australia), and the other 154 patients receiving MED-EL Pulsar implants (MED-EL, Austria). All patients underwent temporal bone computed tomography (CT) and magnetic resonance imaging (MRI)scans before surgery.
Surgery
Routine mastoidectomy was performed to expose the eminence of the horizontal semicircular canal and the short crus of the incus. As a marker of the short crus tip of incus, the beginning of the chorda tympani was identified 1 mm behind the tympanomastoid fissure, which was 8 mm away from the short crus sharp of incus. Then, the full length of the chorda tympani was revealed with approximately 1 mm of bony wall below the short crus tip. The vertical part of the facial nerve was revealed in the same step [Figure 1]. If the facial recess width was <1 mm at the plane of the round window, the chorda tympani nerve was separated with a 1-mm diameter diamond burr and then suspended [Figure 2a]. Next, the chorda tympani nerve was anteplaced and adhered to the posterior wall of the external auditory canal with medical glue [Figure 2b]. The width of the facial recess was enlarged at the level of the round window [Figure 2c]. Then the facial recess was opened, and the round window niche was exposed. The niche was removed, and the round window membrane was observed. The cochleostomy was drilled in the promontory, anteroinferiorly to the membrane of round window to enter the scala tympani where the electrode was inserted. Small pieces of temporalis muscle were used to seal the cochleostomy port. Finally, neural response telemetry and electrode impedance were assessed.
Figure 1.
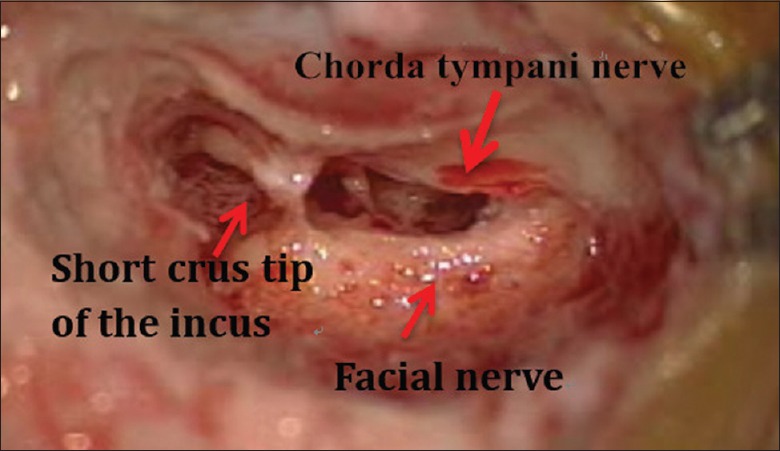
The short crus tip of the incus is a useful marker indicating the chorda tympani nerve and remaining bony wall (approximately 1-mm thick).
Figure 2.
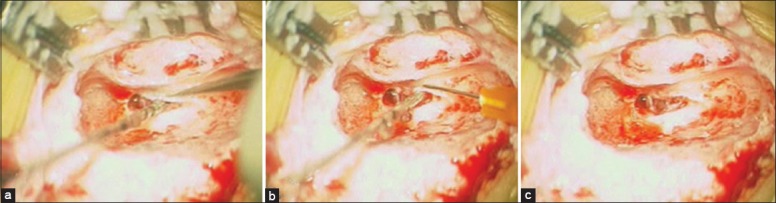
(a) The width of the facial recess is <1 mm at the plane of the round window. The chorda tympani nerve is separated with a 1-mm diameter diamond burr. (b) The chorda tympani nerve is anteplaced and adhered to the posterior wall of the external auditory canal with medical glue. (c) The width of the facial recess is enlarged at the level of the round window.
Taste sensation test
The taste sensation scores were divided into five grades, from 0 to 4, for evaluating the change of four taste sensations (sweet, sour, salty and bitter): 0 means no taste sensation; 1 means only 30% of the taste sensations; 2 means 60% of the taste sensations; 3 means 90% of the taste sensations; and 4 means all four taste sensations are normal. All patients completed taste tests (sweet, sour, salty, and bitter) before surgery, 1 day, and 4 weeks to 1 year after cochlear implantation. The scores of the taste sensation were compared pre- and post-operatively.
Statistical analysis
The scores of the taste sensation were shown as mean ± standard deviation (SD). The paired rank sum test was used to compare the average pre- and post-operative taste sensation scores in 180 cases. A P < 0.05 was considered as statistically significant. Statistical analysis was carried out with SPSS 15.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
In the 32 patients with narrow facial recesses, the average width at the level of the round window was 0.85 mm. The main reason for the narrow facial recess was chorda tympani nerve retropositioning. The chorda tympani nerve was separated, anteplaced, and adhered to the posterior wall of the external auditory canal with medical glue to maintain its integrity. The facial and chorda tympani nerves were revealed with approximately 1 mm of bony wall below the short crus tip, which allowed the chorda tympani nerve to be kept intact in 148 patients with normal-width facial recesses.
None of the 180 patients experienced postoperative complications including injury of the facial or chorda tympani nerve or damage to the posterior wall of the external auditory canal during the 1-year follow-up period.
The average pre- and post-operative taste sensation scores in 180 cases was 3.98 ± 0.15 and 3.96 ± 0.19, respectively, without significant difference (P = 0.083).
DISCUSSION
Hamamoto et al.[8] suggested that the line connecting the CT nerve with the round window passed through the posterior wall of the external auditory canal in 92.3% of individuals, and this characteristic could be useful for preventing CT nerve injury during surgery. But there are a large number of CT nerve variations. In some patients, it may arise from more proximal portion of facial nerve, even close to the geniculate ganglion. The length of the posterior canaliculus is also highly variable, ranging from 3 to 14 mm. In 10% of individuals, there may not be a posterior canaliculus at all in approximately 10% of individuals; rather, it could be replaced by a groove.[9] In our study, the facial recesses narrowed for chorda tympani nerve retropositioning in 32 patients.
Taste is mediated by three cranial nerves: The sensory component of the facial nerve, glossopharyngeal nerve, and vagus nerve. The chorda tympani nerve is one of the three cranial nerves involved in transmitting taste fibers from the anterior two-thirds of the tongue. The mechanism of taste sensation is rather unique in that it involves a complicated feedback loop, with each nerve acting to inhibit signals from other nerves. The chorda tympani nerve exerts a strong inhibitory influence on other taste and pain fibers from the tongue. When the chorda tympani nerve is damaged, its inhibitory function is disrupted, disinhibiting the other taste fibers.[10] chorda tympani nerve injury may induce glial responses at primary nerve terminals in the CNS.[11] Usually, microglial cells respond first, which in turn induce astrocytic responses.[12] As the resident immune cells of the CNS, microglia continually surveys the environment with highly mobile processes and quickly detects and responds to disturbances.[13,14,15] Damage to the chorda tympani nerve results in central glial responses, which may influence long-lasting taste alterations following chorda tympani nerve lesion.[16] This glial activity might also affect nearby trigeminal fibers, which could explain the tingling or burning sensations reported following chorda tympani nerve damage.[17]
Michael and Raut[18] reported that taste disturbance is more likely when the chorda tympani nerve is stretched rather than divided. Division of the chorda tympani nerve seems to have minimal effect on taste perception. Taste sensation from the taste buds is also supplied by the greater petrosal, vagus, and glossopharyngeal nerves, and it has been reported that cutting the chorda tympani nerve may abolish some inhibition of the glossopharyngeal nerve.[19,20] Taste disorders after middle ear surgery are mostly transient, even when the chorda tympani nerves are bilaterally sectioned. In contrast, bilateral chorda tympani nerve lesions may lead to severe, persistent, and distressing xerostomia. Based on this neglected aspect of chorda tympani nerve function, Guinand et al.[21] emphasized the importance of preserving the chorda tympani nerve whenever possible. In our study, the CT nerve was suspended, anteplaced, and adhered to the posterior wall of the auditory canal to enlarge the facial recess in 32 patients with narrow recesses. The full length of the chorda tympani nerve was revealed with approximately 1 mm of bony wall below the short crus tip, which allowed us to keep the chorda tympani nerve intact in 148 patients with normal-width facial recesses. No change in taste sensation was identified compared with preoperative evaluation results.
In conclusion, our identification method successfully preserved chorda tympani nerve structure and function and did not lead to taste loss during cochlear implantation surgery. The chorda tympani nerve may be a useful marker for positioning the facial nerve and keeping the posterior wall of the external auditory canal intact.
Footnotes
Edited by: Xin Chen
Source of Support: This study was supported by grants from the Special Project of the Ministry of Health, China (No. 201202001), the Beijing health technical personnel-training plan (No. 2013-3-063), and Key Laboratory of Otorhinolaryngology-Head and Neck Surgery, Ministry of Education (No. 2013EBYH03).
Conflict of Interest: None declared.
REFERENCES
- 1.Clark MP, O’Malley S. Chorda tympani nerve function after middle ear surgery. Otol Neurotol. 2007;28:335–40. doi: 10.1097/01.mao.0000247820.16325.f0. [DOI] [PubMed] [Google Scholar]
- 2.Lloyd S, Meerton L, Di Cuffa R, Lavy J, Graham J. Taste change following cochlear implantation. Cochlear Implants Int. 2007;8:203–10. doi: 10.1179/cim.2007.8.4.203. [DOI] [PubMed] [Google Scholar]
- 3.Guagliardo NA, Hill DL. Fungiform taste bud degeneration in C57BL/6J mice following chorda-lingual nerve transection. J Comp Neurol. 2007;504:206–16. doi: 10.1002/cne.21436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Yasumatsu K, Kusuhara Y, Shigemura N, Ninomiya Y. Recovery of two independent sweet taste systems during regeneration of the mouse chorda tympani nerve after nerve crush. Eur J Neurosci. 2007;26:1521–9. doi: 10.1111/j.1460-9568.2007.05761.x. [DOI] [PubMed] [Google Scholar]
- 5.Nin T, Umemoto M, Miuchi S, Negoro A, Sakagami M. Treatment outcome in patients with taste disturbance. Nihon Jibiinkoka Gakkai Kaiho. 2006;109:440–6. doi: 10.3950/jibiinkoka.109.440. [DOI] [PubMed] [Google Scholar]
- 6.Loundon N, Blanchard M, Roger G, Denoyelle F, Garabedian EN. Medical and surgical complications in pediatric cochlear implantation. Arch Otolaryngol Head Neck Surg. 2010;136:12–5. doi: 10.1001/archoto.2009.187. [DOI] [PubMed] [Google Scholar]
- 7.Li Y, Zhang D. Perioperative complications of 1396 patients with cochlear implantation (in Chinese) J Clin Otorhinolaryngol Head Neck Surg. 2010;24:433–5. [PubMed] [Google Scholar]
- 8.Hamamoto M, Himi T, Murakami G. Surgical anatomy of the facial nerve and chorda tympani with special reference to cochlear implantation. Nihon Jibiinkoka Gakkai Kaiho. 1999;102:825–34. doi: 10.3950/jibiinkoka.102.825. [DOI] [PubMed] [Google Scholar]
- 9.McManus LJ, Dawes PJ, Stringer MD. Clinical anatomy of the chorda tympani: A systematic review. J Laryngol Otol. 2011;125:1101–8. doi: 10.1017/S0022215111001873. [DOI] [PubMed] [Google Scholar]
- 10.Kiverniti E, Watters G. Taste disturbance after mastoid surgery: Immediate and long-term effects of chorda tympani nerve sacrifice. J Laryngol Otol. 2012;126:34–7. doi: 10.1017/S0022215111002623. [DOI] [PubMed] [Google Scholar]
- 11.Aldskogius H, Kozlova EN. Central neuron-glial and glial-glial interactions following axon injury. Prog Neurobiol. 1998;55:1–26. doi: 10.1016/s0301-0082(97)00093-2. [DOI] [PubMed] [Google Scholar]
- 12.DeLeo JA, Tanga FY, Tawfik VL. Neuroimmune activation and neuroinflammation in chronic pain and opioid tolerance/hyperalgesia. Neuroscientist. 2004;10:40–52. doi: 10.1177/1073858403259950. [DOI] [PubMed] [Google Scholar]
- 13.Davalos DB, Kisley MA, Freedman R. Behavioral and electrophysiological indices of temporal processing dysfunction in schizophrenia. J Neuropsychiatry Clin Neurosci. 2005;17:517–25. doi: 10.1176/jnp.17.4.517. [DOI] [PubMed] [Google Scholar]
- 14.Nimmerjahn A, Kirchhoff F, Helmchen F. Resting microglial cells are highly dynamic surveillants of brain parenchyma in vivo . Science. 2005;27(308):1314–8. doi: 10.1126/science.1110647. [DOI] [PubMed] [Google Scholar]
- 15.Wake AK, Oshinski JN, Tannenbaum AR, Giddens DP. Choice of in vivo versus idealized velocity boundary conditions influences physiologically relevant flow patterns in a subject-specific simulation of flow in the human carotid bifurcation. J Biomech Eng. 2009;131:021013. doi: 10.1115/1.3005157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bartel DL. Glial responses after chorda tympani nerve injury. J Comp Neurol. 2012;520:2712–29. doi: 10.1002/cne.23069. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Eliav E, Kamran B, Schaham R, Czerninski R, Gracely RH, Benoliel R. Evidence of chorda tympani dysfunction in patients with burning mouth syndrome. J Am Dent Assoc. 2007;138:628–33. doi: 10.14219/jada.archive.2007.0234. [DOI] [PubMed] [Google Scholar]
- 18.Michael P, Raut V. Chorda tympani injury: Operative findings and postoperative symptoms. Otolaryngol Head Neck Surg. 2007;136:978–81. doi: 10.1016/j.otohns.2006.12.022. [DOI] [PubMed] [Google Scholar]
- 19.Gopalan P, Kumar M, Gupta D, Phillipps JJ. A study of chorda tympani nerve injury and related symptoms following middle-ear surgery. J Laryngol Otol. 2005;119:189–92. doi: 10.1258/0022215053561657. [DOI] [PubMed] [Google Scholar]
- 20.Leung RM, Ramsden J, Gordon K, Allemang B, Harrison BJ, Papsin BC. Electrogustometric assessment of taste after otologic surgery in children. Laryngoscope. 2009;119:2061–5. doi: 10.1002/lary.20588. [DOI] [PubMed] [Google Scholar]
- 21.Guinand N, Just T, Stow NW, Van HC, Landis BN. Cutting the chorda tympani: Not just a matter of taste. J Laryngol Otol. 2010;124:999–1002. doi: 10.1017/S0022215110000733. [DOI] [PubMed] [Google Scholar]