

Abstract
Infectious disease surveillance systems provide information crucial for protecting populations from influenza epidemics. However, few have reported the nationwide number of patients with influenza-like illness (ILI), detailing virological type. Using data from the infectious disease surveillance system in Japan, we estimated the weekly number of ILI cases by virological type, including pandemic influenza (A(H1)pdm09) and seasonal-type influenza (A(H3) and B) over a four-year period (week 36 of 2010 to week 18 of 2014). We used the reported number of influenza cases from nationwide sentinel surveillance and the proportions of virological types from infectious agents surveillance and estimated the number of cases and their 95% confidence intervals. For the 2010/11 season, influenza type A(H1)pdm09 was dominant: 6.48 million (6.33–6.63), followed by types A(H3): 4.05 million (3.90–4.21) and B: 2.84 million (2.71–2.97). In the 2011/12 season, seasonal influenza type A(H3) was dominant: 10.89 million (10.64–11.14), followed by type B: 5.54 million (5.32–5.75). In conclusion, close monitoring of the estimated number of ILI cases by virological type not only highlights the huge impact of previous influenza epidemics in Japan, it may also aid the prediction of future outbreaks, allowing for implementation of control and prevention measures.
Introduction
Infectious disease surveillance systems provide both quantitative and qualitative information crucial for protecting populations from disastrous epidemics [1–6]. Infectious disease surveillance in Japan, initiated in 1981, has evolved into a comprehensive system of infectious disease control, particularly since the revision of the Infectious Disease Control Law in 1999 [6]. Current surveillance system in Japan, called National Epidemiological Surveillance for Infectious Diseases (NESID), which includes mandatory reporting system for national notifiable diseases and sentinel surveillance system for ubiquitous infectious diseases. National notifiable disease must require having a laboratory confirmation. Sentinel surveillance is based on disease symptom and a confirmed case distribution was reported by infectious agents surveillance, which is 10% samples of the sentinel surveillance. Specimen were randomly selected from these cases and then tested and reported by the Local Public Health Institutes. These relationships were shown in the flow diagram (S1 Appendix). Compared with other surveillance systems around the world, the Japanese system is based on a number of sentinel institutions throughout the country. In the case of influenza-like illness (ILI), almost 5000 sentinel institutions were sampled from across Japan that were representative of geographical regions (public center areas and prefectures), medical institutions (clinics/hospitals and medical departments) and population densities [7]. This carefully designed surveillance system enabled us to estimate the number of ILI patients nationwide and determine the 95% confidence intervals (95% CI) [8,9]. For example, incidence rate (per 1,000) of ILI patients in year 2005 epidemic season was estimated in 142.6 (95% CI: 135.6–149.6) [9]. This quantitative information provided important insight in to future influenza epidemics in Japan.
Identifying the virological types of influenza involved in outbreaks of infection provides essential information for the treatment and prevention of population-wide influenza epidemics. To examine the current influenza epidemic in Japan, infectious agents surveillance, which is laboratory based surveillance, investigated a small number of patients (300–600 patients in the epidemic season) and provided the distribution of virological types among patients every week. This information only reported a fraction of the virological types present among the population, but no further quantitative information was provided by the system. If the estimated number of specific virological types of influenza (i.e. pandemic influenza: A(H1)pdm09) were available, this information would help predict the threat of an influenza epidemic and therefore allow for the appropriate action to be taken.
This study estimated the number of cases of pandemic influenza (A(H1)pdm09) and seasonal-type influenza (A(H3) and B) infection from 2010 to 2014, using data provided from 5000 sentinel sites of the infectious disease surveillance system in Japan.
Methods
The infectious disease surveillance system in Japan
The infectious disease surveillance system in Japan comprises two types of surveillance: sentinel and infectious agents surveillance [7]. Sentinel surveillance, which covers 27 common infectious diseases including ILI, reports weekly numbers of patients throughout Japan. Sentinel medical institutions were selected by local government following the guidelines of the Ministry of Health, Labour and Welfare [10]. These guidelines were intended to ensure equal distribution of sentinel medical institutions throughout the nation. The number of sentinel medical institutions designated within each area and public health center is approximately proportional to its population size. For ILI, the total number of sentinel medical institutions in Japan is approximately 5000. ILI was confirmed by sentinel doctors (mostly using rapid diagnostic testing) of the sentinel medical institution and the number of ILI in each sentinels was reported every week using internet network system. In contrast, infectious agents surveillance is based on specimen samples, which was bought from selected sentinels (500 medical institutions). This laboratory-based surveillance confirmed the virus subtype by Local Public Health Institutes. After pathogens have been isolated from specimens, this information of local centers is sent to the central (Infectious Disease Surveillance Center) and is summarized in an infectious agents surveillance report. Together these surveillance systems provide weekly data on the frequency of infection with different virological types of influenza.
Estimation of the number of patients with specific virological influenza types
Methods for estimating weekly numbers of ILI patients have been described previously [8,9]. In brief, estimations are based on the assumption that all sentinel medical institutions in a public health center are randomly sampled and stratified by the characteristics of the medical institutions (i.e. department type, number of patients). We used a stratified random sampling technique to estimate the total number of ILI cases and their approximate 95% confidence intervals [9].
The weekly numbers of virological type-specific patients were estimated by multiplying the above-mentioned estimated numbers of ILI with the weekly fraction of each virological type identified from the laboratory confirmed cases. The formula of this estimation is shown in the Appendix. We estimated weekly numbers of influenza cases of virological types A(H1)pdm09, A(H3) and B, from week 36 (September 6) of 2010 to week 18 (May 10) of 2014. We also conducted the age-specific estimation by using same method mentioned above. These data were also categorised according to the age of patients: 0–4, 5–19, 20–59 and 60 years and over. All statistical analyses were performed using SAS, version 9.30 (SAS Institute Inc., Cary, NC, USA).
Results
Fig 1 and Table 1 show the weekly estimated number of virological type-specific influenza cases from week 36, year 2010 to week 18, year 2014, in Japan. In the 2010 epidemic season (from September 2010 to May 2011), influenza type A(H1)pdm09 was dominant [total estimated number: 6,480,000 (95% confidence interval (95% CI) 6,330,000–6,630,000]] and the largest weekly number of influenza type A(H1)pdm09 patients was observed in week 4, year 2011 [1,405,000 (1,332,000–1,477,000)], followed by seasonal influenza [A(H3): 364,000 (319,000–409,000) in week 5, B: 357,000 (307,000–407,000) in week 11] (Table 1). The incidence rates of influenza A(H1)pdm09, A(H3) and B were 0.05, 0.03 and 0.02, respectively. While in the 2011 epidemic season (from September 2011 to May 2012), seasonal type influenza A(H3) was dominant [total estimated number: 10,890,000 (10,640,000–11,140,000)], followed by influenza type B [total estimated number: 5,540,000 (5,320,000–5,750,000)]. This trend was similar in the 2012/13 season; however, in the 2013/14 season, influenza type A(H1)pdm09 was again dominant [total estimated number: 6,740,000 (6,530,000–6,950,000)].
Fig 1. Estimated number of cases of influenza infection according to virological type from week 36, 2010 to week 18, 2014, Japan.

Unit of the vertical line: 10,000 patients
Table 1. Estimated number of virological type-specific influenza-like illness patients during the 2010–2014 epidemic seasons.
| Estimated number of influenza patients (95% confidence intervals) | ||||
|---|---|---|---|---|
| 2010/11 | 2011/12 | 2012/13 | 2013/14 | |
| Annual total (10 thousands) | ||||
| A(H1)pdm09 | 648 (633–663) | 3 (1–5) | 26 (20–32) | 674(653–695) |
| A(H3) | 405 (390–421) | 1089 (1064–1114) | 1073(1053–1093) | 254(239–269) |
| B | 284 (271–297) | 554(532–575) | 229 (215–243) | 616 (596–637) |
| Peak week (10 thousands) | ||||
| A(H1)pdm09 | 140.5 (133.2–147.7) | - | - | 110.8 (102.8–118.8) |
| Week 4 | - | - | Week 5 | |
| A(H3) | 36.4 (31.9–40.9) | 174.4(164.4–184.4) | 196.7(188.9–204.5) | 36.4(34.4–45.2) |
| Week 5 | Week 5 | Week 4 | Week 5 | |
| B | 35.7 (30.7–40.7) | 55.9(49.3–62.4) | 26.4(20.8–32.0) | 66.5 (59.6–73.3) |
| Week 11 | Week 10 | Week 6 | Week 12 | |
The estimated number of cases of influenza A(H1)pdm09 infection were excluded because their weekly numbers of patients were all below 5000.
Fig 2 shows the age distribution of patients among the estimated number of virological type-specific influenza cases during the four-year period from 2010 to 2014. During this period, approximately 50% of patients were aged 5–19 or younger, with few patients aged 60 and over, for all of the virus types. Type B influenza incidence showed a particularly strong relationship with younger age groups. For example, in 12 weeks of 2014, the number type B influenza patients of 5–19 years old was 367,000 (95% CI; 318,000–416,000), which was significantly larger than that of 20–59 years old (185,000 (95% CI; 144,000–225,000)).
Fig 2. Age distribution of the estimated number of cases of influenza infection according to virological type from week 36, 2010 to week 18, 2014, Japan.
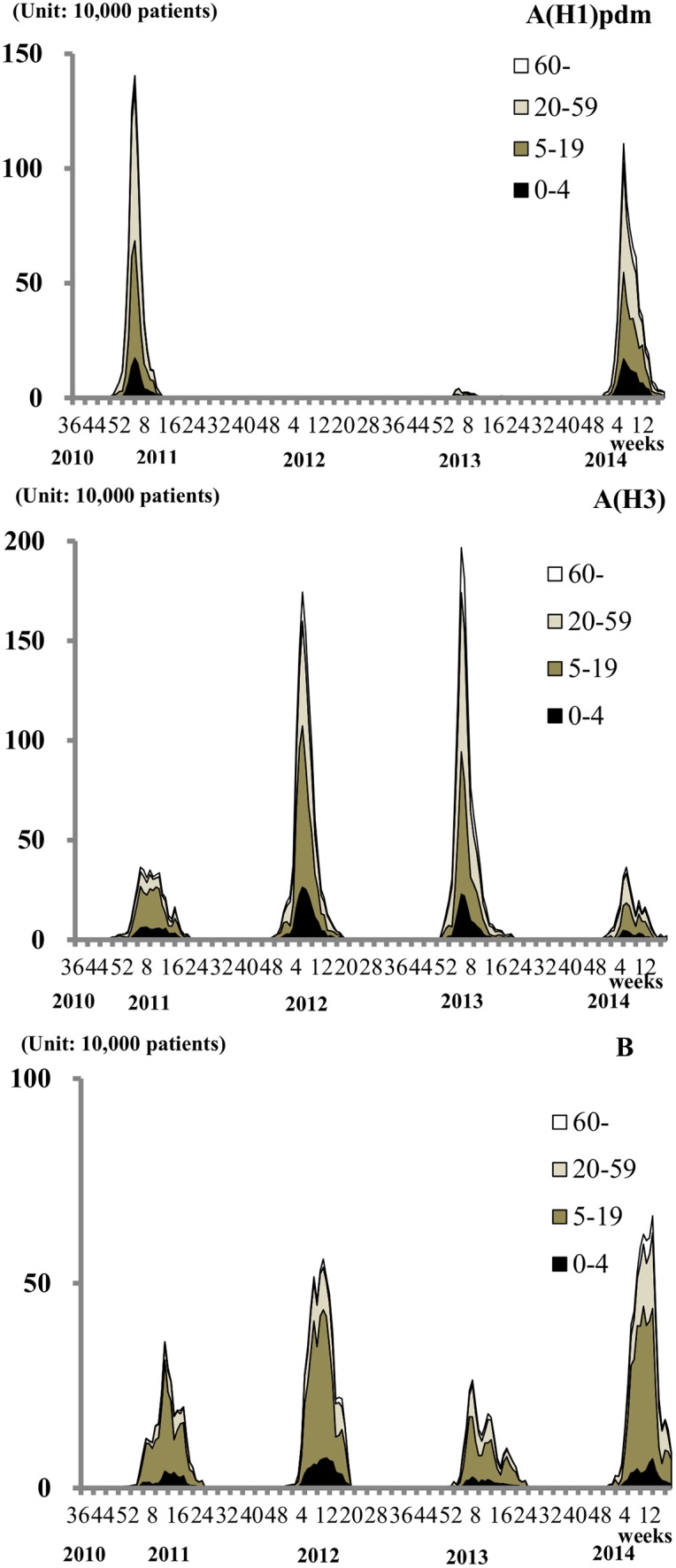
Unit of the vertical line: 10,000 patients
Discussion
In this study, the number of virological type-specific influenza cases over a four-year period (from week 36, 2010 to week 18, 2014) in Japan was estimated using information from the infectious disease surveillance database. An epidemic of influenza A(H1)pdm09 first occurred in Japan in 2009 [11,12]. Our estimated numbers clearly show the huge impact of influenza A(H1)pdm09 on the Japanese population in the 2010/2011 and 2013/2014 seasons.
The proposed method for the estimation of virological type-specific numbers of influenza was based on a stratified-sampling technique. This technique requires a large number of sentinel medical institutions and a well-designed protocol for selecting the location of these institutions. Infectious disease surveillance in Japan, which includes a large number of sentinel medical institutions equally distributed throughout the nation, is best suited to using a sampling technique to estimate the number of influenza patients. In the United States, the Centers for Disease Control and Prevention applied a probabilistic multiplier model for the estimation of the number of influenza A(H1)pdm09 cases nationwide [13]. In this method, a nested structure of six steps was considered for sample collection (including reported cases, test-detected cases, specimen-tested cases, specimen-collected cases, cases seeking medical care for influenza, and total influenza cases) and the multiplier (the inverse of the sampling proportion at each step) was used to estimate the total number of influenza cases [5,13]. This method is straightforward but incorporates many assumptions regarding the “multipliers” in the estimation process. Our estimation method was based on a stratified random sampling technique, the rationale for which was provided by the sampling design. Local public centers selected sentinel medical institutions in Japan based on well-designed criteria to ensure that they were distributed equally across the nation. Although the uncertainty of adherence to these criteria remained in our estimation, a large number of sentinel medical institutions (almost 5000) demonstrated pseudo-stratified random sampling. One study in Japan [14] claimed that our technique might result in an overestimation compared with other methods. This was because the sentinel medical institutions with a high frequency of patient visits were more likely to be included in the infectious disease surveillance system. Improved methods for the unbiased selection of sentinel medical institutions would therefore be desirable [15]. Data on the virological type of influenza cases were derived from laboratory-based infectious agents surveillance. This type of surveillance generated fewer samples compared with sentinel surveillance, leading to instability in the estimation of virological type-specific influenza. Confidence intervals represent the stability of an assessing estimation and the narrow range of confidence intervals shown in Table 1 demonstrate that the annual estimate of the number of virological type-specific influenza cases showed acceptable stability.
Several limitations should mentioned for our study. First, we did not present any regional-specific result that could compare the dominant sub/types of influenza in different regions. In the database of infectious disease agents surveillance, we do not have any regional-based information of influenza sub/types. We suppose that the dominant subtype of influenza in some regions might be different from those of other regions. In case that a regional specific information of influenza virus type is available, we can apply our methods for estimating the regional specific results. The enhancement of infectious disease agents surveillance is desirable to achieve that goal.
Second, we should comment on the inherent bias of our estimation. As we mentioned, the selection of sentinel medical institutions is based on the protocol. In the protocol, the sentinel doctors were encouraged to choose samples randomly, but the decision were totally depend on the doctors. So, we cannot deny the possibility of an inherent bias of specimen selection in the surveillance.
From a public health perspective, the annual estimated number of cases of influenza-like illness throughout the nation provides essential information on which to base future prevention and control strategy decisions to avoid nationwide influenza epidemics. For example, the estimated number of influenza A(H1)pdm09 cases in the 2010/11 season showed a magnitude similar to the first epidemic of this virological type of influenza in 2009 in Japan. This information is vital in preparing for future influenza epidemics [16], with preparations including vaccine storage, increasing medical facilities and provisions, and assigning a budget for ensuing costs. In our opinion, data on the weekly number of patients with virological type-specific influenza could also be made available if this estimation process was built into the infectious surveillance system. This close monitoring of infections would enable early stage intervention to help prevent future influenza epidemics.
Supporting Information
Footnote; This flow diagram cited was Reference 7.
Appendix: The formula for the point estimate and the 95% confidence intervals for the number of virological type-specific influenza-like illness cases.
i is an age category and j is a category of virological type of influence-like illness. A proportion of virological type j in an age-category i sample from the virological surveillance system is pij and its variance is v1ij. Estimated number of cases of influenza-like illness and its variance in the age category i is αi and v2i, which is derived from previous studies [8,9]. The estimated number of cases of influenza-like illness from virological type j in the age category i is αij = pijαi and its variance is expressed as [17]. Finally, the total estimated number of cases of virological type (j) -specific influenza-like illness and its variance was derived by α∙j = Σipijαi and v∙j = Σivij. The approximate 95% confidence interval for α∙∙ is given to be .
(PPTX)
Data Availability
Data are from the infectious disease surveillance system in Japan. Some restrictions of data availability exist for protected and sensitive content, please contact to Yoshitaka Murakami for using data.
Funding Statement
This research was supported by a Grant-in-Aid from the Ministry of Health, Labor and Welfare, Health and Labor Sciences Research Grants, Japan (Research on Emerging and Re-emerging Infectious Disease). The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
References
- 1.Reed C, Kim IK, Singleton JA, Chaves SS, Flannery B, Finelli L, et al. Estimated influenza illnesses and hospitalizations averted by vaccination—United States, 2013–14 influenza season. MMWR Morb Mortal Wkly Rep. 2014;63(49):1151–4. [PMC free article] [PubMed] [Google Scholar]
- 2.Fleming DM, Elliot AJ. Lessons from 40 years' surveillance of influenza in England and Wales. Epidemiol Infect. 2008. July;136(7):866–75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Flahault A, Blanchon T, Dorléans Y, Toubiana L, Vibert JF, Valleron AJ. Virtual surveillance of communicable diseases: a 20-year experience in France. Stat Methods Med Res. 2006;15(5):413–21. [DOI] [PubMed] [Google Scholar]
- 4.Lee JS, Shin KC, Na BK, Lee JY, Kang C, Kim JH, et al. Influenza surveillance in Korea: establishment and first results of an epidemiological and virological surveillance scheme. Epidemiol Infect. 2007;135(7):1117–23. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Wang X, Yang P, Seale H, Zhang Y, Deng Y, Pang X, et al. Estimates of the true number of cases of pandemic (H1N1) 2009, Beijing, China. Emerg Infect Dis. 2010;16(11):1786–8. 10.3201/eid1611.100323 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Ohshiro H, Kawamoto K, Nose T. Surveillance system of infectious diseases in Japan. J Epidemiol. 1996;6(3 Suppl):S81–5. [DOI] [PubMed] [Google Scholar]
- 7.Taniguchi K, Hashimoto S, Kawado M, Murakami Y, Izumida M, Ohta A, et al. Overview of infectious disease surveillance system in Japan, 1999–2005. J Epidemiol. 2007;17 Suppl:S3–13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Hashimoto S, Murakami Y, Taniguchi K, Shindo N, Osaka K, Fuchigami H, et al. Annual incidence rate of infectious diseases estimated from sentinel surveillance data in Japan. J Epidemiol. 2003;13(3):136–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kawado M, Hashimoto S, Murakami Y, Izumida M, Ohta A, Tada Y, et al. Annual and weekly incidence rates of influenza and pediatric diseases estimated from infectious disease surveillance data in Japan, 2002–2005. J Epidemiol. 2007; 17 Suppl:S32–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Tuberculosis and Infectious Diseases Control Division, Health Service Bureau, the Ministry of Health, Labour and Welfare of Japan. The guideline for National Epidemiological Surveillance of Infectious Diseases (kansensho-hasseidokochosajigyo-jissiyoko). Weekly News of Public Health (Shukan-hoken-eisei) 1999; 998: 14–26. (in Japanese). [Google Scholar]
- 11.Ohta A, Hashimoto S, Murakami Y, Kawado M, Taniguchi K, Tada Y, et al. Characteristics of geographical spread and temporal accumulation of the 2009 influenza A (H1N1) epidemic in Japan Based on National Surveillance Data. Jpn J Infect Dis. 2014;67(5):368–73. [DOI] [PubMed] [Google Scholar]
- 12.Shimada T, Gu Y, Kamiya H, Komiya N, Odaira F, Sunagawa T, et al. Epidemiology of influenza A(H1N1)v virus infection in Japan, May-June 2009. Euro Surveill. 2009;14(24). pii: 19244. [DOI] [PubMed] [Google Scholar]
- 13.Reed C, Angulo FJ, Swerdlow DL, Lipsitch M, Meltzer MI, Jernigan D, et al. Estimates of the prevalence of pandemic (H1N1) 2009, United States, April-July 2009. Emerg Infect Dis. 2009;15(12):2004–7. 10.3201/eid1512.091413 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nakamura Y, Sugawara T, Kawanohara H, Ohkusa Y, Kamei M, Oishi K. Evaluation of estimated number of influenza patients from national sentinel surveillance using the national database of electronic medical claims. Jpn J Infect Dis. 2015;68(1):27–9. 10.7883/yoken.JJID.2014.092 Epub 2014 Nov 25. [DOI] [PubMed] [Google Scholar]
- 15.Hashimoto S, Kawado M, Murakami Y, Ohta A, Shigematsu M, Tada Y, et al. Number of sentinel medical institutions needed for estimating prefectural incidence in influenza surveillance in Japan. J Epidemiol. 2014;24(3):183–92. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Fineberg HV. Pandemic preparedness and response—lessons from the H1N1 influenza of 2009. N Engl J Med. 2014;370(14):1335–42. 10.1056/NEJMra1208802 [DOI] [PubMed] [Google Scholar]
- 17.Armitage P, Berry G, Matthews JNS. Statistical methods in medical research fourth edition. Oxon: Blackwell Science, 2002. 161. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Footnote; This flow diagram cited was Reference 7.
Appendix: The formula for the point estimate and the 95% confidence intervals for the number of virological type-specific influenza-like illness cases.
i is an age category and j is a category of virological type of influence-like illness. A proportion of virological type j in an age-category i sample from the virological surveillance system is pij and its variance is v1ij. Estimated number of cases of influenza-like illness and its variance in the age category i is αi and v2i, which is derived from previous studies [8,9]. The estimated number of cases of influenza-like illness from virological type j in the age category i is αij = pijαi and its variance is expressed as [17]. Finally, the total estimated number of cases of virological type (j) -specific influenza-like illness and its variance was derived by α∙j = Σipijαi and v∙j = Σivij. The approximate 95% confidence interval for α∙∙ is given to be .
(PPTX)
Data Availability Statement
Data are from the infectious disease surveillance system in Japan. Some restrictions of data availability exist for protected and sensitive content, please contact to Yoshitaka Murakami for using data.