

Abstract
Introduction:
Simultaneous bipolar dislocation of the clavicle is uncommon and unusual, although it has been documented as panclavicular dislocation, floating clavicle, and complete dislocation of the clavicle. A review of the recent literature indicated that most bipolar clavicular dislocations have been treated non-operatively.
Case Report:
We report the case of a 23 year polytrauma patient with bipolar dislocation of the right clavicle. Patient presented to us 2 weeks post injury and had an unstable corao-clavicular joint. On radiographic assessment a simultaneous dislocation of the coraco-clavicular and sterno-clavicular joints of right side was diagnosed. In view of the unstable condition of the right clavicle, young age of the patient, requirement of high physical activity a decision for operative treatment for clavicle dislocation was taken. Patient was treated surgically with open reduction and tension band wiring with good result.
Conclusion:
Although bipolar dislocation of the clavicle are rare a high index of suspicion will avoid missed diagnosis. Open reduction and internal fixation is a good option in young patients and gives good short term result.
Keywords: Bipolar clavicle dislocation, open reduction, Tension band wiring
Introduction
Simultaneous bipolar dislocation of the clavicle is uncommon and unusual, although it has been documented as panclavicular dislocation, floating clavicle, and complete dislocation of the clavicle [1-13]. Porral reported the first case of a dislocation of both ends of the clavicle in 1831 [11]. A review of the recent literature indicated that most bipolar clavicular dislocations have been treated non-operatively [7]. We report the case of a 23 year old polytrauma patient with bipolar dislocation of the right clavicle treated surgically.
Case Report
A 23 year old man suffered a motor-cycle accident. He sustained contusion of both lungs, multiple fractures of the 1st to 6th ribs left hand, and of the 3rd to 6th ribs right hand, fracture of the transverse processus of the 1st and of the 8th to 10th dorsal vertebrae, a fracture of the sacrum left hand, and a bipolar dislocation of the right clavicle.
First aid was performed at a primary center and patient was transferred to our hospital after 2 weeks. The anteriorly dislocated sternoclavicular joint could be reduced passively, but was unstable, and the protruding anterior deformity quickly recurred. On physical examination there was no evidence of neurologic or vascular deficits. The lateral end of the clavicle was tender and was palpable in a posteriorly displaced position. On the radiograph of the right shoulder and of the thorax a type four dislocation of the right acromioclavicular joint according to Rockwood [14] and an anterior dislocation of the right sternoclavicular joint was detected [15] (Fig. 1). Fractures ofthe spine and the sacrum were treaded conservatively, the patient was mobilized using analgesics and physiotherapy. In view of the unstable condition of the right clavicle, young age of the patient, requirement of high physical activity a decision for operative treatment for clavicle dislocation was taken. At 3 weeks after the accident, open reduction of both the acromioclavicular and the sternoclavicular joint and internal fixation by cerclage wires was performed (Fig.2). Postoperative follow-up was uneventful. After another 2 weeks the patient was discharged. The wires were removed at 8 weeks. The patient subsequently regained a full range of motion of the shoulder. 18 months after injury, the patient was referred to the senior one of us (T.S.) for evaluation. The patient had no complaints of pain or discomfort and both shoulders had a full range of motion. The patient could perform all activities of daily living and had returned to his former work.
Figure 1.
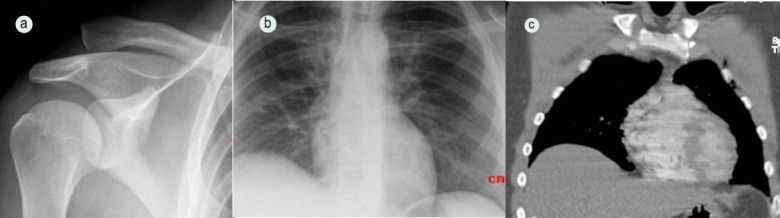
a-Anteroposterior view of the right shoulder shows a dislocation of the acromioclavicular joint. b- Anteroposterior view of both sternoclvicular joints shows a widening of the joint space of the right sternoclavicular joint. c-CT scan of the thorax and both sternoclavicular joints confirms widening of the joint space of the right sternoclavicular joint.
Figure 2.
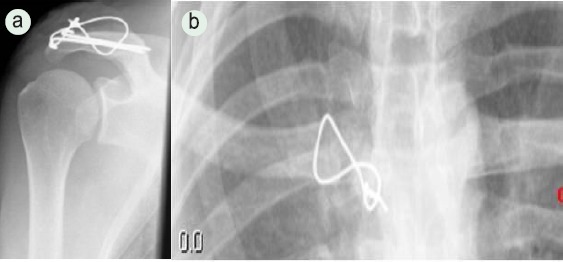
a-Postoperative radiograph of the right coraco-clavicular joint shows stabilization with a K-wire and cerclage wire. b- stabilization of the right sternoclavicular joint with a cerclage wire
Discussion
Simultaneous bipolar dislocation of the clavicle is uncommon and unusual [1-13]. The predominant mechanism of injury causing acromioclavicular separation is a downward blow to the acromion, which tears the coracoclavicular and acromioclavicular ligaments and leads to a superior displacement of the distal pole of the clavicle. The mechanism of injury in sternoclavicular dislocation can be either direct or indirect. The least common mechanism is a direct blow on the anterior aspect of the medial end of the clavicle, causing it to dislocate posterior to the manubrium. A medially directed force on the lateral aspect of the shoulder can result in the more common anterior or superior dislocation of the medial end of the clavicle. Most orthopaedic surgeons recommend reduction of a posterior sternoclavicular dislocation [12]. However, the treatment of an isolated dislocation of the acromioclavicubar or sternoclavicular joint is still controversial. Several therapeutic alternatives have been recommended for these dislocations. Slings, braces, shoulder spicas, and ligament repair or reconstruction, as well as internal fixation. Because of the rarity of simultaneous dislocation of both poles of the clavicle, little is known about the treatment of this injury [8].
A review of the recent literature indicated that most bipolar clavicular dislocations have been treated non-operatively [7]. Gearen et al. [8] treated bipolar clavicular dislocation in a young patient with a shoulder - spica cast in order to maintain the reduction of the clavicle at the acromioclavicular joint that had been obtained by manipulation. Although the unstable reduction could not be maintained, a good functional result ensued.
Cook and Horowitz [5] reported the case of a patient who had a bipolar clavicular dislocation with a grade II acromioclavicular separation whom they treated non- operatively with closed reduction. Several days after treatment, the clavicle redislocated, but this went unreported. At follow-up several months later, both clavicular joints were stable with deformity.
Beckman [2] reviewed 16 cases of patients who had biterminal dislocation of the clavicle that was treated by closed manipulation. Ten patients obtained a good functional result. In one shoulder that could not be manipulated because of the patient’s poor general condition, symptoms involving the brachial plexus developed; a total claviculectomy provided a good functional result. Another patient who had a retrosternal dislocation had severe limitation of motion. The reasons for the remaining poor results were not stated.
The acromioclavicular joint has been well described [12]. It is a diarthrodial joint with a complete or a partial meniscus. The acromioclavicuhar ligaments are thin and are reinforced by the deltoid and trapezius muscles. The conoid ligament medially and the trapezoid laterally connect the clavicle to the coracoid process and are strong stabilizers of the acromioclavicuhar joint. A posterior dislocation of the acromioclavicular joint can be detected clinically by palpation of the end of the clavicle posterior to the acromion and within the substance of the trapezius. The displacement (that is, the widening of the acromioclavicular joint space) may be seen on an anteroposterior radiograph like in our case. An axillary lateral radiograph or a computed CT scan can confirm the diagnosis by showing the posterior displacement of the clavicle from the acromion. The sternoclavicular joint connects the large medial end of the Acknowledgments: Indian Orthopaedic Research Group for help in manuscript preparation clavicle with a small sternal site of articulation. The joint is stabilized by a dense fibrocartilaginous disc, as well as by the rhomboid ligament between the clavicle and the first rib, the capsular ligaments anteriorly and posteriorly between the clavicle and the manubrium, and the interclavicuhar ligament superiorly. The displacement in a dislocation of the sternoclavicular joint may be anterior or posterior [12]. The injuries may be classified as Type I- sprain with ligaments intact and no instability, Type II-persistent subluxation, and Type Ill- dislocation with gross disruption of the ligament [12, 15]. In the current case a 23 year old polytrauma patient suffered biterminal dislocation of the right clavicle. The sternoclavicular joint showed an anterior dislocation, the acromioclavicular joint showed a grade IV dislocation according to Rockwood. In our case there were several additional injuries especially serial fractures of the ribs. In respect to the young age of the patient with high physical demands and the polytrauama condition we performed open reduction of both joints with internal stabilization. At latest follow up after 18 months a good result was achieved. Review of the literature did not show satisfying results with conservative treatment of this rare injury and we believe conservative treatment should be reserved for elderly and multimorbid patients.
Conclusion
Bipolar Clavicular dislocations are rare and a high index of suspicion should be excercised in polytrauma patients with unipolar clavicle dislocations to avoid missed diagnosis. Although a conservative treatment is reported we believe operative treatment should be offered to young patients especially in cases with high physical demands.
Clinical Message.
Operative treatment is suggested in young physically demanding patients presenting with bipolar clavicular dislocations
Footnotes
Conflict of Interest: Nil
Source of Support: None
References
- 1.Arenas AJ, Pampliega T, Iglesias J. Surgical management of bipolar claviculardislocation. Acta Orthop Belg. 1993;59(2):202–5. [PubMed] [Google Scholar]
- 2.Beckman T. A Case of Simultaneous Luxation of Both Ends of the Clavicle. Acta Chir Scandinavica. 1924;56:156–163. [Google Scholar]
- 3.Benabdallah O. Bipolar luxation of the clavicle. Apropos of a case. Rev ChirOrthop Reparatrice Appar Mot. 1991;77(4):263–6. [PubMed] [Google Scholar]
- 4.Caranfil R. Bipolar luxation of the clavicle. A case report. Acta Orthop Belg. 1999 Mar;65(1):102–4. [PubMed] [Google Scholar]
- 5.Cook F, Horowitz M. Bipolar clavicular dislocation. Report of a case. J BoneJoint Surg Am. 1987 Jan;69(1):145–7. [PubMed] [Google Scholar]
- 6.Dieme C, Bousso A, Sane A, Sané JC, Niane M, Ndiaye A, Sy MH, Seye S. Bipolar dislocation of the clavicle or floating clavicle. A report of 3 cases. Chir Main. 2007;26(2):113–6. doi: 10.1016/j.main.2007.02.004. [DOI] [PubMed] [Google Scholar]
- 7.Echo BS, Donati RB, Powell CE. Bipolar clavicular dislocation treated surgically. A case report. J Bone Joint Surg Am. 1988 Sep;70(8):1251–3. [PubMed] [Google Scholar]
- 8.Gearen PF, Petty W. Panclavicular dislocation. Report of a case. J Bone Joint Surg Am. 1982 Mar;64(3):454–5. [PubMed] [Google Scholar]
- 9.Jain AS. Traumatic Floating Clavicle. A Case Report. J. Bone and Joint Surg. 1984;66-B(4):560–561. doi: 10.1302/0301-620X.66B4.6746693. [DOI] [PubMed] [Google Scholar]
- 10.Pang KP, Yung SW, Lee TS, Pang CE. Bipolar clavicular injury. Med JMalaysia. 2003 Oct;58(4):621–4. [PubMed] [Google Scholar]
- 11.Porral MA. Observation d'une double luxation de la clavicule droite. J.Univ. Hebd. med. chir. prat. 1831;2:78–82. [Google Scholar]
- 12.Sanders JO, Lyons FA, Rockwood CA., Jr Management of dislocations of bothends ofthe clavicle. J Bone Joint Surg Am. 1990 Mar;72(3):399–402. [PubMed] [Google Scholar]
- 13.Scapinelli R. Bipolar dislocation of the clavicle:3D CT imaging and delayedsurgical correction of a case. Arch Orthop Trauma Surg. 2004 Jul;124(6):421–4. doi: 10.1007/s00402-004-0669-2. [DOI] [PubMed] [Google Scholar]
- 14.Rockwood CJ, Williams G, Young D. Disorders ofthe acromioclavicularjoint. In: Rockwood CJ, Matsen FA, editors. In The shoulder. 2nd edition. Philadelphia, PA, USA: WB Saunders; 1998. pp. 483–553. [Google Scholar]
- 15.Rockwood CA. In InstructionalCourse Lectures, The American Academy of Orthopaedic Surgeons. Vol. 24. St. Louis: C. V. Mosby; 1975. Dislocations of the Sternoclavicular Joint; pp. 144–159. [Google Scholar]