

Abstract
Introduction:
A case of young male patients aged 25 years old presented with history of injured from falling heavy object on his back. There was burst Fracture of L5 Vertebrae with grade 3 spondylolisthesis. It was completely different from the types of L5 fracture that had been published up to now. Our patient had combination of a complete burst fracture of the fifth lumbar vertebra with dislocation and complete disruption of the posterior ligamantous and bony complex between L5 and sacrum. We would like to report this unique case of comminuted burst fracture of L5 with grade III spondylolisthesis treated with reconstruction of L5 body from transforaminol approach with the good results & significant neurological improvement till his six month follow up after the operation.
Case Report:
A case of young male patients aged 25 years old presented with history injured from falling heavy object on his back. The physical examination revealed contusion on his back Neurological examination confirmed complete paralysis of L5 and S1 root on both sides. Loss Bladder-bowel function, sphincter tone and peri-anal sensation. Plain radiograph of lumbar-sacral spine showed the anterior dislocation of L5-S1 spondylo-listhesis approximately 75%, with the complete comminuted burst fracture of L5 vertebra.
Conclusion:
Anterior support and reconstruction of vertebral body is of immense importance in Lumbar burst fracture, When combined with posterior short segment fixation. This can be achieved with Usage of expandable cages when opted for posterior only approach. They obviate need of anterior approach for reconstruction of vertebral body.
Keywords: L5 burst Fracture, traumatic spondylolisthesis, expandable cage, posterior reconstruction
Introduction
There has been considerable controversy regarding what constitutes the best treatment for lumbar burst fractures. Goals of thoracolumbar fracture are restoring vertebral column stability and obtaining spinal canal decompression to achieve early mobility of patient [1-5]. Burst fractures of the lumbar spine have unique biomechanical and neurological features as compared with burst fractures in other regions of the spine [6]. Management of thoracolumbar burst fracture is diverse and depends upon various components. Fracture morphology, neurological status and the predilection of surgeon all play important role in determining whether the anterior, posterior or combined approach is to be taken [7]. The fracture of the fifth lumbar vertebra with dislocation in our patient was completely different from the types of L5 fracture that had been published up to now. There have been very few reports in the literature regarding burst fracture of the fifth lumbar vertebra and various pattern of affecting it. Our patient had combination of a complete burst fracture of the fifth lumbar vertebra with dislocation and complete disruption of the posterior ligamantous and bony complex between L5 and sacrum.
Case Report
A case of young male patients aged 25 years old presented with history injured from falling heavy object on his back. At initial evaluation, he had severe pain on his back with deformity of the vertebrae. He felt numbness and had weakness on this both legs. The physical examination revealed contusion on his back Neurological examination confirmed complete paralysis of L5 and S1 root on both sides. Loss Bladder-bowel function, sphincter tone and perianal sensation.
Radiographic findings Plain radiograph of lumbosacral spine showed the anterior dislocation of L5-S1 spondylolisthesis approximately 75%, (Fig.1) with the complete comminuted burst fracture of L5 vertebra (Fig.2) Computed tomography revealed a fracture of right lamina and both pedicle of L5. There was retropulsion of communited fragments inside spinal canal causing sever caudal compression.
Figure 1.
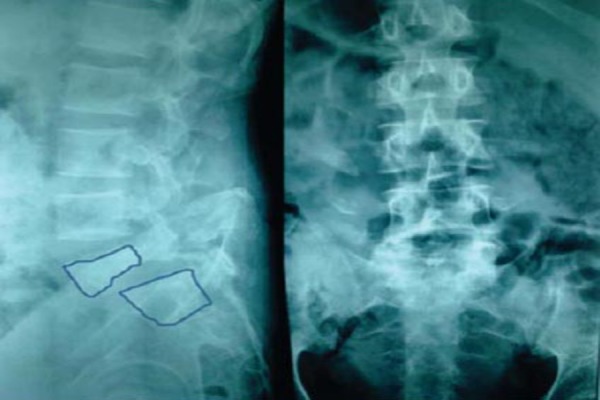
Radiographic Presentation of Lumbosacral Spine; Anteroposterior & Lateral View.
Figure 2.
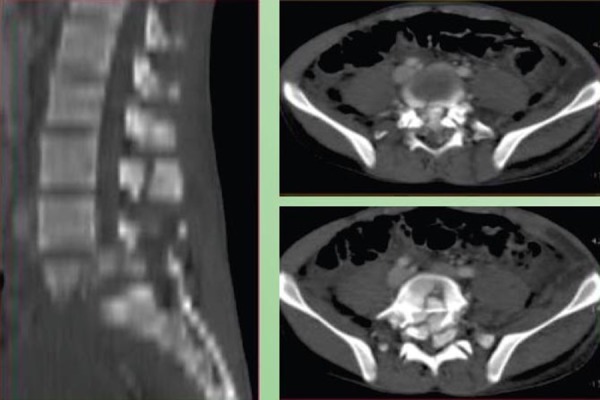
Radiography Presentation of the Lumbosacral Computerized Tomography.
The patient underwent surgery on emergency basis 6hrs after initial injury. In prone position, standard midline posterior subperiosteal dissection was carried out above & below injured vertebral body. Transpedicular screws were placed into L4 and S1 bilaterally. Because of neurological involvement laminectomy & unilateral facectomy was carried out to decompress thecal sac and roots of L5 and S1. Restoration of the affected vertebral body done by distracting L4 and S1 over screws. Complete discetomy of L4/5 and L5/S1 were undertaken. Conservative Corpectomy to decompress thecal sac and accommodate expandable cage was then performed using large curates, kerisons rongerd and pitutary forcepes while the dura and roots were protected. Hollow of expandable cage filled with cancellous bony chips inserted from left side to achieve fusion. Rest of the defect also filled with bony cancellous chips harvested from local laminectomy. Pedicular screws are connected with rod and singal cross connector. The procedure lasted for 4hr, the blood loss was 1200mls. (Fig.3) demonstrate serial images during surgery of pedicle location, screw placement & cage insertion in to achieve vertebral hight. No complication was observed afterward during the admission. Motor power in his lower 2 extremities was still similar to that found initially as well as his sensation. From the (Fig. 4), it shows the new alignment of the spine, however, 25% dislocation of the spines would be observed. On the day fifth after the operation, his pain was relieved. The lumbosacral brace was used and wheelchair ambulation was encouraged. He was discharge on the eighth day after the operation.
Figure 3.
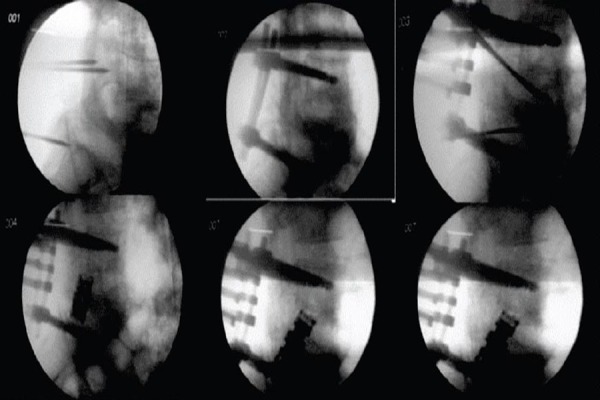
C-Arm Demonstrate Serial Images During Surgery.
Figure 4.

Post-operative Radiograph Showing New Alignment of the Spine.
Result
Patient had recovered of his bladder, bowel function and sphincter tone at end was three months. He had independent ambulatory status with peroni band; although there was persistent paralysis of distal power (L5/S1), there was recovery of proximal muscles in L5/S1 myotomes. Height of vertebral body was restored to normal and maintained at three months without any implant back out or loosening.
Discussion
Burst fractures of the lumbar spine have unique biomechanical and neurological features as compared with burst fractures in other regions of the spine. In the lumbar spine, the body’s center of gravity falls at or posterior to the vertebral axis [8] Slight flexion decreases the lordosis and places the axial load force-of-injury vector through the vertebral body. This dictates the specific pattern of injury as well as the tendency for progressive deformity [9].
From a neurological standpoint, the content and size of the neural canal distinguish the lumbar area from other regions. The cauda equina alone occupies the spinal canal at and caudad to the second lumbar level. Unlike in the spinal cord or the conus medullaris, neurological dysfunction in this area simulates a peripheral-nerve injury with the potential for spontaneous recovery. Additionally, the dimensions of the spinal canal are wider here than in any other region and, indeed, there have been several reports of decreases of as much as 90 per cent in the cross-sectional area of the canal in the absence of a neurological deficit. These features help to explain the infrequency of severe neurological deficits and the potential for neurological recovery when such a deficit is present [10].
There have been very few reports in the literature regarding burst fracture of the fifth lumbar vertebra and various pattern of affecting it. Literature reports only individual patients or very small group of patients. Balanco et al [11] reported five patients with isolated burst fracture vertebra without neurological deficit. All were managed non operatively with short period of rest followed by protected mobilization. It was agreed that conservative treatment is appropriate in those with minimal canal compromise, minor deformity and no neurological deficit. Court –Brown [12] in 1987 reported on their experience with three patients who had burst fracture of fifth lumbar vertebra. They treated two patients conservatively with no major complication. Other patients who had posterior decompression, internal fixation and arthrodesis had persistent back pain. There was loss of lordosis in all three patients, despite the use of instrumentation in one of them. They concluded that current instrumentation cannot adequately maintain the fracture in good alignment.
Controversy continues concerning the best treatment of unstable burst thoracolumbar fractures. Kyphosis correction and canal decompression in case of a neurological deficits are recognized treatment objectives, and various conservative and surgical strategies have been proposed.
In the past, the spectrum of non-operative treatment has ranged from prolonged periods of strict bed rest to early protected mobilization. A variable amount of bed rest ranging from two to twelve weeks has been advocated. Most of series recommended non operative management, although they have stated indication as absence of neurological deficit.[11]
Posterior transpedicular stabilization and staged anterior corpectomy and titanium cage implantation is a safe and reliable method in unstable fractures of thoracolumbar spine [13]. Korovessis et al [14] described direct reduction of thoracolumbar A3 type burst fractures by means of ballone kyphoplasty with calcium phosphate and posterior transpedicular stabilization. Anterior body height ratio improved from 0.6 to 0.9 after surgery. Whereas posterior vertebral body height improved from 0.95 to 1. Shono et al.[15] who have shown in their experimental study that posterior distractive reduction maneuver generates anterior and middle spinal column defects, leading to significant mechanical instabilities, particularly in axial compressive loading. Short-segment posterior pedicle screw fixation technique to resist axial spinal loading anteriorly is not adequate [16], but if the construct is used in neutral mode and adequate strut support is provided anteriorly, the efficacy and utility of pedicle screws is increased.
Anterior only surgical approach for some burst thoracolumbar fractures is advocated in patients with neurological deficits and without injury to the posterior ligamantous complex[17,18]. The anterior aaproch to the fifth lumbar vertebra is associated with danger to the superior hypogastric plexus and large vessel injury [19,20]. The treatment of complex three- column lumbar metastatic disease involves anterior and posterior surgery and often requires a staged reconstruction. Hunt et al describes their surgical technique for inserting an expandable cage via a posterior extra-cavitaory approach while protecting segmental nerves. [19]
The fracture of the fifth lumbar vertebra with dislocation in our patient was completely different from the types of L5 fracture that had been published upto now. Our patient had combination of a complete brust fracture of the fifth lumbar vertebra with dislocation and complete disruption of the posterior ligamantous and bony complex between L5 and sacrum. Hence it was not amenable for reduction posterior distraction ligamentotaxis. Also there was need for anterior reconstruction to avoid loss of reduction and Implant failure.
Conclusion
Traumatic spondylolisthesis is a rare condition with relatively high incidence of neurological involvement. Conservative treatment usually has poor prognosis as the treatment can no stabilized the spine. Interbody fusion allows higher degree of stability and fusion rate. The anterior support reduces the risk of implant failure and recommended strongly. In the present case report, there was more than 50% communited fracture with broken bilateral pedicals of L5 body with Grade III listhesis & retropulsed osteodiscal fragments in neural canal which was not amenable for interbody fusion. Reconstruction of L5 body in addition to decompression of cauda and stabilization of spine was required. We would like to report this unique case of communited brust fracture of L5 with grade III spondylolisthesis treated with reconstruction of L5 body using expandable cage from transforaminol approach with the good results & significant neurological improvement till his three-month follow up after the operation.
Clinical Message.
Lumbar burst fractures- dislocations should be addressed aggressively with surgical management. Anterior support and reconstruction of vertebral body is of immense importance in Lumbar burst fracture, when combined with posterior short segment fixation. This can be achieved with usage of expandable cages when opted for posterior only approach. They obviate need of anterior approach for reconstruction of vertebral body.
Biography




Footnotes
Conflict of Interest: Nil
Source of Support: None
References
- 1.Alvine GF, Swain JM, Asher MA, Burton DC. Treatment of thoracolumbar burst fractures with variable screw placement or Isola instrumentation and arthrodesis: case series and literature review. J Spinal Disord Tech. 2004;17:251–64. doi: 10.1097/01.bsd.0000095827.98982.88. [DOI] [PubMed] [Google Scholar]
- 2.Briem D, Lehmann W, Ruecker AH, Windolf J, Rueger JM, Linhart W. Factors influencing the quality of life after burst fractures of the thoracolumbar transition. Arch Orthop Trauma Surg. 2004;124:461–8. doi: 10.1007/s00402-004-0710-5. [DOI] [PubMed] [Google Scholar]
- 3.Dimar JR, 2nd, Wilde PH, Glassman SD, Puno RM, Johnson JR. Thoracolumbar burst fractures treated with combined anterior and posterior surgery. Am J Orthop. 1996;25:159–65. [PubMed] [Google Scholar]
- 4.Leferink VJ, Zimmerman KW, Veldhuis EF, ten Vergert EM, ten Duis HJ. Thoracolumbar spinal fractures: radiological results of transpedicular fixation combined with transpedicular cancellous bone graft and posterior fusion in 183 patients. Eur Spine J. 2001;10:517–23. doi: 10.1007/s005860100319. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Parker JW, Lane JR, Karaikovic EE, Gaines RW. Successful short- segment instrumentation and fusion for thoracolumbar spine fractures: a consecutive 41/2-year series. Spine (Phila Pa1976) 2000;25:1157–70. doi: 10.1097/00007632-200005010-00018. [DOI] [PubMed] [Google Scholar]
- 6.Andreychik David A, Dirk H, Alander, Karolyn M, Senica E. Shannon Stauffer Burst Fractures of the Second through Fifth Lumbar Vertebrae. Clinical and Radiographic Results. J Bone Joint Surg Am. 1996;78:1156–66. doi: 10.2106/00004623-199608000-00005. [DOI] [PubMed] [Google Scholar]
- 7.Jan Kocis, Peter Wendsche. Petr Visna Complete brust fracture of fifth lumbar vertebra trated by posterior surgery using expandable cage. Acta Neurochir. 2008;150:1301–1305. doi: 10.1007/s00701-008-0149-5. [DOI] [PubMed] [Google Scholar]
- 8.An H. S, Simpson J. M, Ebraheim N. A, Jackson W. T, Moore J, O’Malley N. P. Low lumbar burst fractures: comparison between conservative and surgical treatments. Orthopedics. 1992;15:367–373. doi: 10.3928/0147-7447-19920301-15. [DOI] [PubMed] [Google Scholar]
- 9.Finn C. A, Stauffer E. S. Burst fracture of the fifth lumbar vertebra. Bone and Joint Surg. 1992 Mar;74-A:398–403. [PubMed] [Google Scholar]
- 10.Keene J. S, Fischer S. P, Vanderby R, Jr, Drummond D. S, Turski P. A. Significance of acute posttraumatic bony encroachment of the neural canal. Spine. 1989;14:799–802. doi: 10.1097/00007632-198908000-00004. [DOI] [PubMed] [Google Scholar]
- 11.Blanco JF, De Pedro JA, Hernandez PJ, Paniagua JC, Framian A. Conservative management of brust fracture of the fifth lumbar vertebra. J Spinal Disorders Tech. 2005;18(3):229–231. [PubMed] [Google Scholar]
- 12.Court- Brown CM, Gertzbein SD. The management of burst fracture of fifth lumbar vertebra Spine. 1987;12(3):308–312. doi: 10.1097/00007632-198704000-00022. [DOI] [PubMed] [Google Scholar]
- 13.Payer M. Unstable burst fractures of the thoracolumbar junction treatment by posterior bi-segmental correction/fixation and staged anterior corpectomy and titanium cage implantation. Acta Neurochir. 2006;148(3):299–306. doi: 10.1007/s00701-005-0681-5. [DOI] [PubMed] [Google Scholar]
- 14.Korovessis P, Repantis T, Petsinis G, illiopoulos P, Hadjipalou A. Direct reduction of thoracolumbar burst fractures by means of balloon kyphoplasty with calcium phosphate and stabilization with pedical screw instrumentation and fusion. Spine. 2008;(4):E100–E108. doi: 10.1097/BRS.0b013e3181646b07. [DOI] [PubMed] [Google Scholar]
- 15.Shono Y, McAfee PC, Cunningham BW. Experimental study of thoracolumbar burst fractures—a radiographic and biomechanical analysis of anterior and posterior instrumentation systems. Spine. 1994;19:1711–1722. doi: 10.1097/00007632-199408000-00010. [DOI] [PubMed] [Google Scholar]
- 16.Yoganandan N, Larson SJ, Pintar F. Biomechanics of lumber pedicle screw/plate fixation in trauma. Neurosurgery. 1990;27:873–880. doi: 10.1097/00006123-199012000-00003. [DOI] [PubMed] [Google Scholar]
- 17.Kirkpatrick JS. Thoracolumbar fracture management: anterior approach. J Am Acad Orthop Surg. 2003;11(5):255–365. doi: 10.5435/00124635-200309000-00008. [DOI] [PubMed] [Google Scholar]
- 18.Sasso RC, Best NM, Reilly TM, McGurinre RA. Anterior only stabilistaion of three column thoracolumbar injuries. J Spinal Disord Tech. 2005;18(Suppl 1):7–14. doi: 10.1097/01.bsd.0000137157.82806.68. [DOI] [PubMed] [Google Scholar]
- 19.TRAVIS HUNT, M.D, FRANCIS H, SHEN M.D, VINCENT ARLET., M.D Expandable cage placement via a posterolateral approach in lumbar spine reconstructions. J Neurosurg Spine. 2006;5:271–274. doi: 10.3171/spi.2006.5.3.271. [DOI] [PubMed] [Google Scholar]
- 20.Bingol H, Cingoz F, Yilmaz AT, Yasar M, Tataer H. Vascular complication related to lumbar disc surgery. J Neurosurg. 2004;100(3 Suppl spine):249–253. doi: 10.3171/spi.2004.100.3.0249. [DOI] [PubMed] [Google Scholar]
- 21.Baru SA, Delamarter RB, Schiffrman ML, Willson LA, Watkins RG. Vascular Injury during anterior lumbar surgery. Spine J. 2004;4(4):409–412. doi: 10.1016/j.spinee.2003.12.003. [DOI] [PubMed] [Google Scholar]