

Abstract
Introduction:
Osteochondroma are benign neoplasms which arise from small cartilage nodules within the periosteum. They can be either pedunculated or sessile and are more common in the extremities. They rarely develop in bones like scapula, feet, hands and pelvis. Management of the lesion is by en-bloc excision.
Case Report:
We present a case of 18 year female, who came with a swelling in right groin since 2 years which was diagnosed to be osteochondroma on x-ray and magnetic resonance imaging. Excision biopsy was done as the patient wanted it to be removed for cosmetic purpose and confirmed it to be non-malignant osteochondroma. There has been no recurrence even after 1 year of follow up.
Conclusion:
Thus osteochondroma of the pelvis should be kept in mind as a differential diagnosis when evaluating mass in pelvis. Also these have to be removed when they pose cosmetic problems.
Keywords: Osteochondroma, exostosis, pubic ramus, pelvis, excision, benign osteochondroma, pubic ramus osteochondroma
Introduction
Osteochondroma are benign neoplasms which arise from small cartilage nodules within the periosteum. They can be either pedunculated or sessile and are more common in the extremities, i.e. distal femur, proximal tibia and proximal humerus in decreasing order. They can be multiple and be a part of multiple hereditary exostosis. They rarely develop in bones like scapula, feet, hands and pelvis. Management of the lesion is by en-bloc excision. Indications for excision are cosmetic deformity, pressure symptoms on neuro-vascular bundle or malignant transformation to chondrosarcoma which is rare. [1]
Pelvic osteochondroma has been documented with an incidence of 5% of all osteochondromas. [2] Osteochondroma of the pubic ramus is rare entity and the actual incidence is not known. It can present as a solitary lesion or as a part of multiple hereditary exostosis.
Excision of such a pelvic lesion is required only if there are pressure symptoms. Pelvic osteochondromas can present as compressive neuropathy or compressive symptoms on urethra, bladder or other vital structures and so on. On the contrary a pubic bone mass may need to be removed in young females which might be prominent at labia for cosmetic reasons as in our case.
Case report
An 18 year female came to the out-patient department with complaints of swelling in right groin since 5 years which was insidious in onset, small in size initially but grew over last 5 years and was noticeable to the patient. Patient came for medical help for cosmetic reasons. On examination, there was a bony hard swelling 3 × 5 cms in size in the groin at the pubic tubercle of the right side. It was fixed to the underlying bone. The skin over the swelling was free and mobile. Patient did not have any other swellings elsewhere in the body. Plain x-ray’s of pelvis AP, inlet and outlet view (Fig.1 to 3) and magnetic resonance imaging (Fig 4 & 5) showed bony growth of 54×37×46 mm in size in transverse, craniocaudal and anteroposterior dimension which was arising from right superior pubic ramus and was extrapelvic in situation with a cartilage cap of 4mm. There was no involvement of any neurovascular bundle. Any involvement of urinary tract was also ruled out by micturating cysto-urethrography. Patient was taken up for excision biopsy. Extended ilio-inguinal approach (Fig. 6) was taken and as the soft tissue was retracted cartilage cap of the osteochondroma was seen (Fig. 7). It was excised with osteotome piece meal (Fig. 8). On table manual palpation was done and one more piece was found which was then excised (Fig. 9). Inguinal ligament was closed in layers maintaining the external iliac ring with continuous sutures to prevent future inguinal hernia (Fig. 10). Cosmetic closure of skin was done. Histopathology confirmed it to be benign osteochondroma without any undifferentiated cells. Since then there has been no recurrence even after one year follow up.
Figure 1.

Pelvis AP View.
Figure 3.

Pelvis Outlet View.
Figure 4.
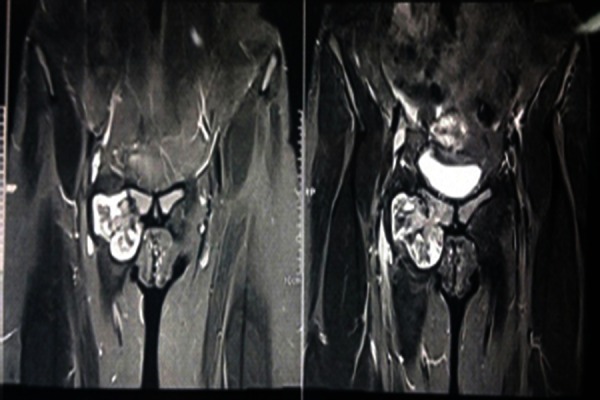
MRI Coronal Cuts showing the growth
Figure 5.
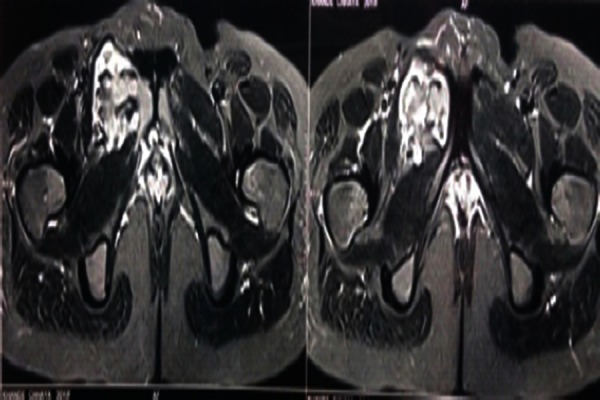
MRI Transverse cuts
Figure 6.

Incision
Figure 7.

Cartilage Cap
Figure 8.
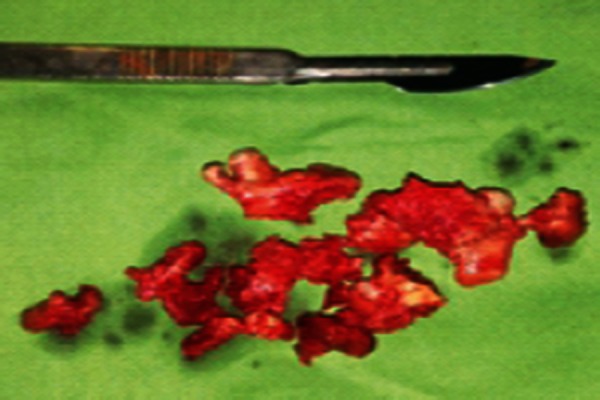
Excised Mass
Figure 9.
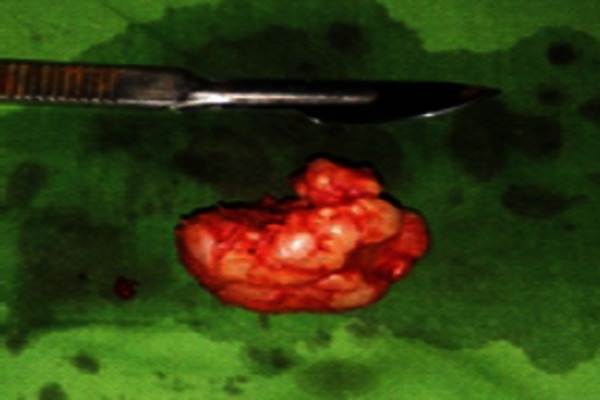
2nd Excised Mass
Figure 10.

Inguinal ligament closure
Figure 2.

Pelvis Inlet View
Discussion
Osteochondromas are benign tumors which have an unknown etiology. It is considered as a developmental physeal abnormality rather than a primary bone neoplasm. A few theories have been suggested which include Virchow theory, Muller theory, Keith theory, and a few more. [3] The most common sites are metaphysis of long bones like distal femur, proximal tibia and proximal humerus. They are also found at other sites but it is uncommon. Osteochondromas can also be found as a part of multiple hereditary exostosis which is thought to be associated with EXT1 and EXT 2 gene. [4] Trauma and inflammation have been suggested as a contributory factors.
Osteochondromas are as such an incidental finding in patients and only a few are symptomatic. It is usually present in growing age and the growth of the mass stops after skeletal maturity. Most common symptom is cosmetic deformity or pain. It can cause compression of the surrounding neurovascular structures which then warrants its removal. There can also be malignant transformation to chondrosarcoma which is rare. Various studies have mentioned about the size of cartilage cap as a predictor for malignancy with a cartilage cap of more than 2 cm after skeletal maturity indicative of malignant transformation [5,6,7,8,9].
Pre operative investigations and planning in patients presenting with a bony neoplasm must be done. It is helpful in distinguishing between benign and malignant tumors. Radiographic and ancillary imaging studies should be sought in advance of surgical intervention. Gitelis et al [10] established a diagnostic strategy for evaluation and differentiation of tumors. Pre-operative X-rays and MRI were done for our patient to see the extent and measure the cartilage cap of the osteochondroma.
Pelvic osteochondroma involving ilium has been reported in literature which caused nerve root compression and had to be removed. [11] Similar cases of iliac bone osteochondroma have been reported by Kumar S et al [12]. Osteochondroma of the pubic symphisis has been reported which was removed due to bladder outlet obstruction. [13] Thus with a thorough search in literature we concluded that it is a rare entity and it was diagnosed due to the compressive symptoms caused by it. Here in our case the swelling near the private part was the cause for the patient to seek medical help. There were no compressive symptoms either on vessels or on urinary tract which was confirmed by arterial Doppler and micturating cysto-urethrography. A similar case was reported by Qaisrani GH [14] and associates which was also present on superior pubic ramus and was removed for cosmetic deformity.
Complete En-Bloc removal of the mass was done in our case for cosmetic reasons and she is being followed up regularly. Even after 1 year there has not been any recurrence of the lesion.
Conclusion
Benign osteochondromas are usually incidental findings and are removed most commonly for cosmetic purposes with a very low incidence of recurrence if removed after skeletal maturity. They can also present with compressive symptoms which warrants its removal. Also pelvic osteochondromas are rare entity but it has to be kept in mind for any bony mass when looking for differentials.
Clinical Messege
Pelvic osteochondromas are rare entity but it has to be kept in mind for any bony mass when looking for differentials.
Biography

Footnotes
Conflict of Interest: Nil
Source of Support: None
Reference
- 1.Robert K, Heck . Benign bone tumors and neoplastic conditions simulating bone tumors. In: Terry Canale S, James H. Beaty, editors. Campbell’s Operative Orthopaedics. 11th ed. Philadelphia: Mobsy Elsevier; 2007. pp. 858–861. [Google Scholar]
- 2.Mark D. Murphey, James J. Choi, Mark J, Kransdorf, et al. Imaging of Osteochondroma: Variants and Complications with Radiologie-Pathologie Correlation. Radiographics. 2000;20:1407–1434. doi: 10.1148/radiographics.20.5.g00se171407. [DOI] [PubMed] [Google Scholar]
- 3.Robert D’Ambrosia. the formation of osteochondroma by epiphyseal cartilage transplantation. Clinical Orthopaedics & Related Research. 1968 Nov;61:103–15. [PubMed] [Google Scholar]
- 4. http://www.ncbi.nlm.nih.gov/books/NBK1235/citedon28/08/2014 .
- 5.Bone and soft tissue pathology(ppg331 -335)- Andrew i.folpe, Carrie y.inwards-a volume in the series foundations in diagnostic pathology, copyright 2010 by saunders an imprint of Elsevier, inc [Google Scholar]
- 6.Cannela P, Gardini F, Boriani S. Exostosis: development, evolution and relationship to malignant degeneration. Ital J Orthop Traumatol. 1981;7:293–8. [PubMed] [Google Scholar]
- 7.Variants of exostoses of the bone in children.-Randy Ray Richardson, MD-Seminars in Roentgenology. 2005 Oct;40(4):380–390. doi: 10.1053/j.ro.2005.01.020. [DOI] [PubMed] [Google Scholar]
- 8.Malghem J.Vande Berg, Noel H, et al. Benign osteochondromas and exostotic chondrosarcomas: evaluation of artilage cap thickness by ultrasound. Skeletal Radiol. 1992;21:33–37. doi: 10.1007/BF00243091. [DOI] [PubMed] [Google Scholar]
- 9.Kreig J. C, Buckwalter J. A, Peterson K. K, El-khoury G.Y, Robinson R.A. extensive growth of an osteochondroma in a skeltellay mature patient. A case report. J. Bone and Joint Surg. 1995 Feb;77-A:269–273. doi: 10.2106/00004623-199502000-00015. 0. [DOI] [PubMed] [Google Scholar]
- 10.Peterson HA. Multiple hereditary osteochondromata. Clin orthop relat res. 1989;239:222–230. [PubMed] [Google Scholar]
- 11.Kim W, Kim K, Lee S, Choy W. Solitary Pelvic Osteochondroma Causing L5 Nerve Root Compression. ORTHOPEDICS. 2009;32(12) doi: 10.3928/01477447-20091020-25. [DOI] [PubMed] [Google Scholar]
- 12.Kumar S, Shah A K, Patel A M, Shah U A. CT and MR images of flat bone osteochondromata from head to foot: A pictorial essay. Indian J Radiol Imaging; 2006;16:589–96. [Google Scholar]
- 13.Wang WY, Du LD, Lv WC, Tian Y, Shao Q, Zhang YH. Osteochondroma of the symphysis pubis: a rare cause of bladder outlet obstruction. Am Surg. 2010 Aug;76(8):916–8. [PubMed] [Google Scholar]
- 14.Qaisrani GH, Muhammad I, Rahman A. Osteochondroma of a pubic bone in a young female. NMJ. 2009;1(2):24–25. [Google Scholar]