

Abstract
Osteoporosis is a disease that affects the bones. It leads to increased risk of fractures as a result of decreased bone mineral density. The goal of this study was to assess the general perception of osteoporosis as well as knowledge of lifestyle, risk factors, and preventive measures among patients in Qatar. The study was conducted between September 2013 and September 2014. The study subjects (n = 93) were patients diagnosed with osteoporosis who attended the Outpatient Rheumatology Clinic at Hamad General Hospital in Doha, Qatar. The results showed that those with a university or graduate degree had a significantly higher level of knowledge about osteoporosis (p = 0.009) than those with less education. Among those in our study, knowledge related to osteoporosis was principally obtained through media sources such as television and radio (39%). In conclusion, osteoporosis patients in Qatar need a better understanding of the disease. Identifying thought patterns related to the perception of osteoporosis and treatment might assist in building a foundation for management modalities and effective preventive strategies for the disease in Qatar.
Keywords: Qatar, osteoporosis, patient perception, public health, knowledge, risk factors
Introduction
Osteoporosis is a disease that affects the bones. It leads to increased risk of fractures as a result of decreased bone mineral density, causing more than 8.9 million fractures worldwide each year. Estimates by the International Osteoporosis Foundation (IOF) indicate that osteoporosis affects 200 million women globally and predict that 1 in 3 women and 1 in 5 men will experience a osteoporotic fracture when over 50 years of age.1
Sadat-Ali et al., in a review of published data from Saudi Arabia, found that the prevalence of osteoporosis was 34% among 5160 healthy women aged 50–79. The prevalence of osteopenia and osteoporosis in three studies of 822 males was 46.3% and 30.7%, respectively.2 For osteoporosis, Shilbayeh reported a prevalence of 29.6% among postmenopausal women in Jordan,3 while Bener et al., reported a prevalence of 12.3% among postmenopausal women in Qatar (n = 821).4
The management of osteoporosis involves several approaches, including medication, lifestyle changes, and fall prevention.5 A number of risk factors play a role in the etiology of this disease. Some, such as vitamin D deficiency, smoking, and alcohol abuse, are modifiable, while others, such as gender, age, and ethnicity, are not.6
The risk of developing osteoporosis can be reduced by following preventive measures that focus on physical activity, dietary supplements, and lifestyle modifications such as reduced smoking and alcohol consumption. These measures collectively play a role in improving bone mass throughout different life stages.7 This is the first study that aims to assess the general perception of osteoporosis among patients in Qatar, as well as their knowledge of associated lifestyle, risk factors, and preventive measures.
Methods
A total of 93 patients diagnosed with osteoporosis participated in the study, out of the 114 approached. The patients attended the Outpatient Rheumatology Clinic at Hamad General Hospital of Hamad Medical Corporation in Doha, Qatar. Patients were recruited over a one-year period between September 2013 and September 2014. Approval from the Institutional Review Board overseeing research at Hamad Medical Corporation was obtained before the commencement of study procedures (13262/13). A waiver of signed informed consent was presented to patients by their physician before their participation in a face-to-face interview, which lasted for 10–15 minutes.
Data collection instrument
The data collection instrument gathered information pertaining to the following seven main categories: socio-demographics, disease and family history, general perception of osteoporosis, lifestyle and risk factors, preventive measures at home, treatment and complications, and sources used by patients to obtain information related to osteoporosis. The patients were asked 33 questions, which were similar to those used in other studies, but modified for Qatar's culture.8,9 The questions had three possible answers: “yes,” “no,” and “do not know.” A pilot test of the data collection instrument was performed, as well as consequent changes, before using the instrument to interview participants.
Statistical analysis
Qualitative and quantitative data were expressed as frequencies, with percentage and mean ± SD. Demographic data and other characteristics of the participants were analyzed using descriptive statistics. Associations between categorical variables were evaluated using a Pearson's chi-squared test and a chi-square test with a continuity correction factor or a Fisher exact test. Continuous variables were analyzed using a t-test. Spearman's correlation coefficient was used to assess the strength of linear relationship between knowledge score and other quantitative and qualitative variables. Linear regression analysis was applied to assess and examine the effect of different factors such as age, gender, education, duration of osteoporosis, history of fracture and family history of osteoporosis on osteoporosis knowledge score. Furthermore, knowledge score were categorized into three groups using an arbitrary cutoff score (very good knowledge (>85% correct answers), good knowledge (75–85% correct answers), and moderate/low knowledge ( < 75% correct answers) and were compared with different factors stated above using one-way analysis of variance (ANOVA) and chi-square test as an exploratory statistical analysis. Significance was based on a two-sided p-value of < 0.05. All statistical analyses were conducted using Statistical Package for Social Sciences (SPSS Inc., Chicago, IL), version 21.0.
Results
In our sample population (n = 93), 92.5% of the participants were female (mean age = 63.31 ± 9.98) and 7.5% were male (mean age = 63.86 ± 12.54). The majority of participants had been diagnosed with osteoporosis more than 5 years earlier (52.7%), while 30.1% had been diagnosed 3–5 years earlier, and 17.2% had been diagnosed less than three years earlier. Additional information on demographics and osteoporosis history is provided in Table 1.
Table 1.
Demographics and osteoporosis history information
| Female | Male | P-value | |
|
| |||
| (n = 86) | (n = 7) | ||
|
| |||
| Age (years) | |||
|
| |||
| (mean ± SD) | 63.31 ± 9.98 | 63.86 ± 12.54 | 0.892 |
|
| |||
| Marital status | |||
|
| |||
| Single | 4 (4.7%) | 2 (28.6%) | 0.265 |
|
| |||
| Married | 76 (88.4%) | 4 (57.1%) | |
|
| |||
| Widowed | 4 (4.7%) | 1 (14.3%) | |
|
| |||
| Divorced | 2 (2.3%) | – | |
|
| |||
| Education | |||
|
| |||
| None | 18 (20.9%) | 1 (14.3%) | 0.399 |
|
| |||
| Elementary/intermediate | 25 (29.1%) | – | |
|
| |||
| High school | 15 (17.4%) | 1 (14.3%) | |
|
| |||
| University/graduate | 28 (32.6%) | 5 (71.4%) | |
|
| |||
| Years since osteoporosis diagnosis | |||
|
| |||
| 0–3 years | 15 (17.4%) | 1 (14.3%) | 0.919 |
|
| |||
| 3–5 years | 26 (30.2%) | 2 (28.6%) | |
|
| |||
| More than 5 years | 45 (52.3%) | 4 (57.1%) | |
|
| |||
| History of fractures | |||
|
| |||
| Yes | 30 (34.9%) | – | 0.139 |
|
| |||
| No | 56 (65.1%) | 7 (100%) | |
|
| |||
| Family history of osteoporosis | |||
|
| |||
| Yes | 27 (31.4%) | 3 (42.9%) | 0.839 |
|
| |||
| No | 59 (68.6%) | 4 (57.1%) | |
|
| |||
When participants were asked about their general perception of osteoporosis, 100% of the males identified osteoporosis as a disease of postmenopause, a disease with low bone density, and a disease associated with an increased risk of fracture, while 82.6%, 75.6%, and 96.5% of the females answered “yes” to the same items, respectively. Table 2 summarizes answers pertaining to the participants’ general perception of osteoporosis.
Table 2.
General perception of osteoporosis
| Female | Male | P-value | |
|
| |||
| (n = 86) | (n = 7) | ||
|
| |||
| Disease of postmenopause | |||
|
| |||
| Yes | 71 (82.6%) | 7 (100.0%) | 0.225 |
|
| |||
| No | 1 (1.2%) | – | |
|
| |||
| Do not know | 14 (16.3%) | – | |
|
| |||
| Disease with low bone density | |||
|
| |||
| Yes | 65 (75.6%) | 7 (100.0%) | 0.555 |
|
| |||
| No | 3 (3.5%) | – | |
|
| |||
| Do not know | 18 (20.9%) | – | |
|
| |||
| Disease with possibility of fracture | |||
|
| |||
| Yes | 83 (96.5%) | 7 (100.0%) | 0.175 |
|
| |||
| No | 2 (2.3%) | – | |
|
| |||
| Do not know | 1 (1.2%) | – | |
|
| |||
Table 3 shows the patients’ perceptions of which risk and lifestyle factors affect their disease. There were no significant differences between the answers provided by males and females (p>0.05).
Table 3.
Knowledge of lifestyle and risk factors
| Female | Male | P-value | |
|
| |||
| (n = 86) | (n = 7) | ||
|
| |||
| Age is a risk factor for osteoporosis | |||
|
| |||
| Yes | 77 (89.5%) | 7 (100.0%) | 0.831 |
|
| |||
| No | 3 (3.5%) | – | |
|
| |||
| Do not know | 6 (7.0%) | – | |
|
| |||
| Osteoporosis cannot be prevented | |||
|
| |||
| Yes | 46 (53.5%) | 2 (28.6%) | 0.351 |
|
| |||
| No | 20 (23.3%) | 4 (57.1%) | |
|
| |||
| Do not know | 20 (23.3%) | 1 (14.3%) | |
|
| |||
| Family history of osteoporosis | |||
|
| |||
| Yes | 74 (86.0%) | 6 (85.7%) | 0.782 |
|
| |||
| No | 3 (3.5%) | – | |
|
| |||
| Do not know | 9 (10.5%) | 1 (14.3%) | |
|
| |||
| Inactivity increases the risk of osteoporosis | |||
|
| |||
| Yes | 70 (81.4%) | 6 (85.7%) | 0.962 |
|
| |||
| No | 8 (9.3%) | – | |
|
| |||
| Do not know | 8 (9.3%) | 1 (14.3%) | |
|
| |||
| Smoking | |||
|
| |||
| Yes | 53 (61.6%) | 6 (85.7%) | 0.499 |
|
| |||
| No | 9 (10.5%) | 1 (14.3%) | |
|
| |||
| Do not know | 24 (27.9%) | – | |
|
| |||
| Chronic disease | |||
|
| |||
| Yes | 59 (68.6%) | 5 (71.4%) | 0.969 |
|
| |||
| No | 6 (7.0%) | – | |
|
| |||
| Do not know | 21 (924.4%) | 2 (28.6%) | |
|
| |||
| Low dairy products consumption | |||
|
| |||
| Yes | 83 (96.5%) | 7 (100%) | 0.542 |
|
| |||
| No | – | – | |
|
| |||
| Do not know | 3 (3.5%) | – | |
|
| |||
| Thin women are at greater risk than heavy women | |||
|
| |||
| Yes | 15 (17.4%) | – | 0.717 |
|
| |||
| No | 49 (57.0%) | 4 (57.1%) | |
|
| |||
| Do not know | 22 (25.6%) | 3 (42.9%) | |
|
| |||
| Low calcium intake may be a risk factor for osteoporosis | |||
|
| |||
| Yes | 83 (96.5%) | 7 (100%) | 0.175 |
|
| |||
| No | 1 (1.2%) | – | |
|
| |||
| Do not know | 2 (2.3%) | – | |
|
| |||
| Dairy products are a major source of calcium | |||
|
| |||
| Yes | 83 (96.5%) | 7 (100%) | 0.542 |
|
| |||
| No | – | – | |
|
| |||
| Do not know | 3 (3.5%) | – | |
|
| |||
| Medications may cause osteoporosis | |||
|
| |||
| Yes | 51 (59.3%) | 4 (57.1%) | 0.903 |
|
| |||
| No | 9 (10.5%) | 1 (14.3%) | |
|
| |||
| Do not know | 26 (30.2%) | 2 (28.6%) | |
|
| |||
| Weight-bearing exercises can help prevent osteoporosis | |||
|
| |||
| Yes | 80 (93.0%) | 6 (85.7%) | 0.273 |
|
| |||
| No | 1 (1.2%) | – | |
|
| |||
| Do not know | 5 (5.8%) | 1 (14.3%) | |
|
| |||
Table 4 shows the patients’ answers to questions about preventive measures at home. There were no significant differences between the answers provided by males and females (p>0.05).
Table 4.
Knowledge of preventive measures at home
| Female | Male | P-value | |
|
| |||
| (n = 86) | (n = 7) | ||
|
| |||
| Measures for fall prevention | |||
|
| |||
| Yes | 63 (73.3%) | 7 (100%) | 0.713 |
|
| |||
| No | 9 (10.5%) | – | |
|
| |||
| Do not know | 14 (16.3%) | – | |
|
| |||
| Hand rails in bathroom | |||
|
| |||
| Yes | 65 (75.6%) | 5 (71.4%) | 0.399 |
|
| |||
| No | 6 (7.0%) | 2 (28.6%) | |
|
| |||
| Do not know | 15 (17.4%) | – | |
|
| |||
| Walk with a walker | |||
|
| |||
| Yes | 68 (79.1%) | 4 (57.1%) | 0.654 |
|
| |||
| No | 9 (10.5%) | 2 (28.6%) | |
|
| |||
| Do not know | 9 (10.5%) | 1 (14.3%) | |
|
| |||
| Room brightly lit | |||
|
| |||
| Yes | 81 (94.2%) | 7 (100%) | 0.538 |
|
| |||
| No | 2 (2.3%) | – | |
|
| |||
| Do not know | 3 (3.5%) | – | |
|
| |||
| Non-slippery shoes | |||
|
| |||
| Yes | 83 (96.5%) | 6 (85.7%) | 0.415 |
|
| |||
| No | 1 (1.2%) | 1 (14.3%) | |
|
| |||
| Do not know | 2 (2.3%) | – | |
|
| |||
| Non-slippery surface in room and bathroom | |||
|
| |||
| Yes | 83 (96.5%) | 7 (100%) | 0.175 |
|
| |||
| No | 1 (1.2%) | – | |
|
| |||
| Do not know | 2 (2.3%) | – | |
|
| |||
The level of knowledge among participants (the total number of correct answers to questions) was categorized into three groups: (1) very good knowledge (>85% correct), (2) good knowledge (75–85% correct), and (3) moderate/low knowledge ( < 75% correct). Overall, 31.2% (n = 29), 47.3% (n = 44), and 21.5% (n = 20) of participants fell into these three categories, respectively. Spearman's correlation analysis showed only education was significantly and positively correlated with knowledge score (r = 0.416; p < 0.001). Age was negatively correlated with knowledge score however, this association was not statistically significant (r = − 0.166; p = 0.112). Both univariate (regression coefficient = 4.58; t = 3.07; p = 0.003), and multivariate linear regression analysis revealed (regression coefficient = 4.31; t = 3.32; p = 0.001) that only higher education was significantly correlated with increased knowledge score. Other variables and factors such as age, gender, duration of osteoporosis, history of fracture and family history of osteoporosis did not show any significant association with osteoporosis knowledge score (p>0.05). Exploratory statistical analysis showed similar findings, patients with a university or graduate degree had a significantly higher level of knowledge when compared to those with less education (p = 0.009). Table 5 shows additional comparisons according to demographics and disease history.
Table 5.
Level of knowledge according to demographics and disease history
| Knowledge level | P-value | |||
|
| ||||
| Very good | Good | Moderate/low | ||
|
| ||||
| (n = 29) | (n = 44) | (n = 20) | ||
|
| ||||
| Age (years) | ||||
|
| ||||
| (mean ± SD) | 62.10 ± 10.77 | 64.07 ± 8.91 | 63.60 ± 11.86 | 0.718 |
|
| ||||
| Age group | ||||
|
| ||||
| ≤ 60 years | 11 (36.7%) | 12 (40.0%) | 7 (23.3%) | 0.608 |
|
| ||||
| >60 years | 18 (28.6%) | 32 (50.8%) | 13 (20.6%) | |
|
| ||||
| Gender | ||||
|
| ||||
| Male | 4 (57.1%) | 1 (14.3%) | 2 (28.6%) | 0.380 |
|
| ||||
| Female | 25 (29.1%) | 43 (50.0%) | 18 (20.9%) | |
|
| ||||
| Marital status | ||||
|
| ||||
| Single | 4 (66.7%) | – | 2 (33.3%) | 0.663 |
|
| ||||
| Married | 23 (28.7%) | 41 (51.2%) | 16 (20.0%) | |
|
| ||||
| Widowed | 2 (40.0%) | 2 (40.0%) | 1 (20.0%) | |
|
| ||||
| Divorced | – | 1 (50.0%) | 1 (50.0%) | |
|
| ||||
| Education | ||||
|
| ||||
| None | 2 (10.5%) | 11 (57.9%) | 6 (31.6%) | 0.009 |
|
| ||||
| Elementary/intermediate | 7 (12.5%) | 11 (56.3%) | 7 (28.0%) | |
|
| ||||
| High school | 2 (28.0%) | 9 (44.0%) | 5 (31.3%) | |
|
| ||||
| University/graduate | 18 (54.5%) | 13 (39.4%) | 2 (6.1%) | |
|
| ||||
| Years since osteoporosis diagnosis | ||||
|
| ||||
| 0–3 years | 3 (18.8%) | 7 (43.8%) | 6 (37.5%) | 0.575 |
|
| ||||
| 3–5 years | 8 (28.6%) | 16 (57.1%) | 4 (14.3%) | |
|
| ||||
| More than 5 years | 18 (36.7%) | 21 (42.9%) | 10 (20.4%) | |
|
| ||||
| History of fractures | ||||
|
| ||||
| Yes | 11 (36.7%) | 13 (43.3%) | 6 (20.0%) | 0.733 |
|
| ||||
| No | 18 (28.6%) | 31 (49.2%) | 14 (22.2%) | |
|
| ||||
| Family history of osteoporosis | ||||
|
| ||||
| Yes | 10 (34.5%) | 13 (43.3%) | 7 (23.3%) | 0.868 |
|
| ||||
| No | 19 (65.5%) | 31 (49.2%) | 13 (20.6%) | |
|
| ||||
In regard to sources of information about osteoporosis, 39% of participants indicated that their information was obtained from the media (television or radio). Figure 1 summarizes the sources of information among participants.
Figure 1.
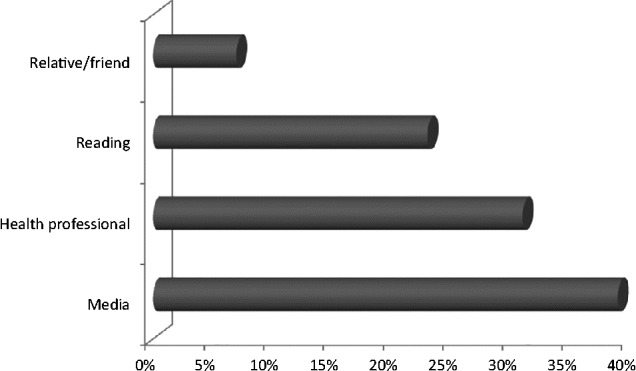
Sources of information about osteoporosis among participants
Discussion
Our study evaluated the general perception of osteoporosis among patients in Qatar, as well as their knowledge of lifestyle, risk factors, and preventive measures. The results of our study, which are consistent with those of other reports, indicate that several aspects of patients’ knowledge and lifetsyle could be improved.7,9,10,11 Overall, there were no significant differences according to gender.
Irrespective of gender, 31.2% of participants had very good knowledge of osteoporosis, providing correct answers to more than 85% of the questions. Most participants were able to identify several osteoporosis risk factors (smoking 63.4%, low dairy products consumption 96.7%, low calcium intake 96.7%). On the other hand, fewer participants were able to identify other factors, such as the fact that thin women are at greater risk than overweight women (17.4%).
Our results confirmed previous findings by Al Attia et al., in a study conducted in the United Arab Emirates that assessed Arab females’ knowledge about osteoporosis. The study found that highly educated women had more knowledge about osteoporosis and its modifiable and non-modifiable risk factors when compared to women with secondary education.10
A large number of participants were able to identify several preventive measures used in the home (handrails 75.3%, use of a walker 77.4%, adequate brightness in the room 94.6%). This is in contrast to the findings of other studies, which found that the majority of participants lacked information on preventive measures and the main risk factors of the disease.7,9,11
With regard to fractures, an Australian study of 1082 postmenopausal women concluded that women's concerns and risk perception related to osteoporosis and associated fractures are “resonably well founded.” Significant associations were found between history of fracture after 45 years of age, younger age, lower self-reported general health, and being “somewhat” and “very concerned” about osteoporosis. However, the study showed that factors such as height loss, aging, smoking, and drinking were not among the factors that caused concern among participants.12
In a study by Sujic et al., that included 1735 fragility fracture patients, 93% of the participants did not think that their fracture was caused by osteoporosis. Only 8.2% changed their perception after 6 months.13 The results highlight an important issue; most fragility fracture patients have low bone density and need to implement preventive measures to avoid future fractures, but this is not likely to occur if patients do not perceive a need to manage their osteoporosis.
The results of the current study showed that media sources, such as television and radio were used more often than healthcare professionals to obtain disease-related information. This is in agreement with the study by Al Attia et al., which identified magazines, newspapers, and television as the major source of information among patients.10 Thus, we recommend that media outlets should be used to deliver disease specific information, as Logsdon et al., have shown such to be effective.14,15
One limitation of the study is that it did not investigate whether patients applied their knowledge to implement changes in lifestyle or dietary habits. Another limitation is the fact that more than half (52.7%) of the study participants had the disease for more than 5 years, giving them more time to acquire knowledge when compared to someone recently diagnosed with the disease. A third limitation is related to gender: 92.5% of the participants were female (probably because of the normal gender-related disease distribution, osteoporosis being more common among women). In a large study (n = 1514) of the Norwegian population, Magnus et al., found that women knew significantly more about osteoporosis than did men (p < 0.001).16 Finally, a larger sample size with adequate statistical power that is representative of the overall population is needed to generalize the findings described above.
Conclusions
The results of this study showed no differences according to gender. Education was associated with a higher level of knowledge about osteoporosis. Television and radio should be targeted in efforts to raise awareness and provide health education. Future research should examine perceptions in a larger sample of patients, as well as in the general population. This should aid in building and directing future modalities for the prevention and treatment of osteoporosis in Qatar. Finally, physicians and healthcare providers should make more effort to teach and inform patients about preventing, treating, and living with osteoporosis.
Conflict of interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
- 1.International Osteoporosis Foundation [Internet]. Nyon: The Foundation; c2015 [cited 2014 Oct 1] Osteoporosis facts and statistics; [about 1 screen] Available from: http://www.iofbonehealth.org/facts-statistics#category-14.
- 2.Sadat-Ali M, Al-Habdan IM, Al-Turki HA, Azam MQ. An epidemiological analysis of the incidence of osteoporosis and osteoporosis-related fractures among the Saudi Arabian population. Ann Saudi Med. 2012;32:637–641. doi: 10.5144/0256-4947.2012.637. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Shilbayeh S. Prevalence of osteoporosis and its reproductive risk factors among Jordanian women: A cross-sectional study. Osteoporos Int. 2003;14:929–940. doi: 10.1007/s00198-003-1458-4. [DOI] [PubMed] [Google Scholar]
- 4.Bener A, Hammoudeh M, Zirie M. Prevalence and predictors of osteoporosis and the impact of life style factors on bone mineral density. APLAR Journal of Rheumatology. 2007;10:227–233. [Google Scholar]
- 5.Kanis JA, Melton LJ, Christiansen C, Johnston CC, Khaltaev N. The diagnosis of osteoporosis. J Bone Miner Res. 1994;9:1137–1141. doi: 10.1002/jbmr.5650090802. [DOI] [PubMed] [Google Scholar]
- 6.Ross PD. Osteoporosis. Frequency, consequences, and risk factors. Arch Intern Med. 1996;156:1399–1411. doi: 10.1001/archinte.156.13.1399. [DOI] [PubMed] [Google Scholar]
- 7.Hernandez-Rauda R, Martinez-Garcia S. Osteoporosis-related life habits and knowledge about osteoporosis among women in El Salvador: A cross-sectional study. BMC Musculoskelet Disord. 2004;5:29. doi: 10.1186/1471-2474-5-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yeap S, Goh E, Das Gupta E. Knowledge about osteoporosis in a Malaysian population. Asia Pac J Pubic Health. 2010;22:233–241. doi: 10.1177/1010539509343948. [DOI] [PubMed] [Google Scholar]
- 9.Ailinger RL, Emerson J. Women's knowledge of osteoporosis. Appl Nurs Res. 1998;11:111–114. doi: 10.1016/s0897-1897(98)80102-x. [DOI] [PubMed] [Google Scholar]
- 10.Al Attia HM, Abu Merhi AA, Al Farhan MM. How much do the Arab females know about osteoporosis? The scope and sources of knowledge. Clin Rheumatol. 2008;27:1167–1170. doi: 10.1007/s10067-008-0926-9. [DOI] [PubMed] [Google Scholar]
- 11.Ungan M, Tümer M. Turkish women's knowledge of osteoporosis. Fam Pract. 2001;18:199–203. doi: 10.1093/fampra/18.2.199. [DOI] [PubMed] [Google Scholar]
- 12.Barcenilla-Wong AL, Chen JS, March LM. Concern and risk perception of osteoporosis and fracture among post-menopausal Australian women: Results from the Global Longitudinal Study of Osteoporosis in Women (GLOW) cohort. Arch Osteoporos. 2013;8:155. doi: 10.1007/s11657-013-0155-y. [DOI] [PubMed] [Google Scholar]
- 13.Sujic R, Gignac MA, Cockerill R, Beaton DE. Factors predictive of the perceived osteoporosis-fracture link in fragility fracture patients. Maturitas. 2013;76:179–184. doi: 10.1016/j.maturitas.2013.07.014. [DOI] [PubMed] [Google Scholar]
- 14.Logsdon MC, Mittelberg M, Myers J. Use of social media and internet to obtain health information by rural adolescent mothers. Appl Nurs Res. 2015;28(1):55–56. doi: 10.1016/j.apnr.2014.04.006. [DOI] [PubMed] [Google Scholar]
- 15.Logsdon MC, Bennett G, Crutzen R. Preferred health resources and use of social media to obtain health and depression information by adolescent mothers. Journal of Child and Adolescent Psychiatric Nursing. 2014;27(4):163–168. doi: 10.1111/jcap.12083. [DOI] [PubMed] [Google Scholar]
- 16.Magnus JH, Joakimsen RM, Berntsen GK, Tollan A, Søogaard AJ. What do Norwegian women and men know about osteoporosis? Osteoporos Int. 1996;6:32–36. doi: 10.1007/BF01626535. [DOI] [PubMed] [Google Scholar]