

Abstract
A 48-year-old married woman diagnosed with rheumatoid arthritis (RA) in 2007, came to our hospital in July 2014 with the complaint of severe pain and swelling over multiple joints, especially over small joints, which was associated with stiffness (more in morning), deformities of fingers and toes, with disturbed sleep and poor quality of life (QOL) for the past 7 years. She received a combination of electro acupuncture (14 sessions), massage (18 sessions), mud (18 sessions), and sauna (3 sessions) (EMMS) therapies for 30-min, 45-min, 30-min, and 15-min per session, respectively for 3 weeks. During and postintervention assessment showed reduction in visual analog scale score for pain, Depression Anxiety and Stress Scales and the Pittsburgh Sleep Quality Index scores. It also showed an increase in the scores of 10-Meter Walk Test, isometric hand-grip test, and short form-36 version-2 health survey. This result suggest that, the EMMS therapy might be considered as an effective treatments in reducing pain, depression, anxiety, and stress with improvement in physical functions, quality of sleep and QOL in patient with RA. EMMS therapies were tolerated and no side effects were reported by the patient. Though the results are encouraging, further studies are required with larger sample size and advanced inflammatory markers.
Keywords: Electro-acupuncture, massage, mud therapy, rheumatoid arthritis, sauna therapy
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic, systemic, polyarticular autoimmune inflammatory disease causing destruction of capsule and synovial lining of joints, especially in the hands, feet and knees. It affects 3 times more women than men and can lead to pain, altered biomechanics and decreased quality of life (QOL).[1]
According to naturopathy accumulation of morbid matter is the cause of diseases,[2] hence eliminating those morbid matters is the cure for disease. To reduce pain and other symptoms, use of complementary and alternative medicine, which includes thermotherapy, acupuncture, massage etc., has increased for RA patients.[3] Acupuncture[4] and massage[5] therapies are commonly employed for most of the pain management, mud[6] was shown to have an anti-inflammatory effect and sauna was assumed to reduce pain and swelling by producing analgesic effect and perspiration. Since these therapies were shown to have effect on either one or the other RA symptoms, and Acupuncture,[4] mud,[6] and sauna[7] therapies alone could not significantly improve pain,[4] erythrocyte sedimentation rate (ESR)[4,6] compared to control[4] and clinico-biochemical and immunological indices[7] respectively in RA, we selected the combination of electro-acupuncture, massage, mud, and sauna (EMMS) therapies to produce better improvement. Hence, this study aimed at evaluating the effect of EMMS therapies in pain, motor function, depression, anxiety, stress, quality of sleep (QOS), and QOL in patient with RA.
CASE DESCRIPTION
A 48-year-old, married woman diagnosed with RA in 2007 underwent irregular conventional management. Her symptoms, as described by her, began with moderate to severe pain associated with swelling, stiffness (more in morning) in multiple joints, especially over small joints, elbow, shoulder, knee, and hip joints with symmetrical distribution and deformities of fingers and toes. RA-factor was positive and her physician advised methotrexate and hydrochloroguine. Patient underwent those medications for 1-year and stopped them after her symptoms improved.
Three years later, she was affected again with similar problems and admitted in a private hospital for 6 days, underwent treatment with methotrexate, hydroxychloroquine, prednisolone, calcium, folic acid, multivitamin supplements, and physiotherapy. At home, she was advised to continue same medications with naproxen, rabeprazole sodium, and diclofenac. Patient underwent those medications for 30 months, but she developed puffiness of face, greying of hair and generalized weakness, because of which she developed fear of taking medication and stopped taking medications. Following this, all those symptoms reduced, except joint pain. Hence, she underwent locally available herbal therapy (patient did not know the name of herbs), but her symptoms worsened day by day and she became stressed and depressed, especially due to deformities. In 2013, she experienced palpitation and underwent electro cardiogram, but findings were normal. Later, she underwent Ayurvedic medicine such as Sinhanad-guggul and Punarnava-mandoor with diclofenac sodium but she could not get improvement and became very much depressed, which was associated with poor QOS and QOL.
When she visited us with the same complaints in July, 2014, we suggested her to take combination EMMS therapies. She stopped taking diclofenac and other Ayurvedic medications on 1st and 3rd day of her stay in the hospital, respectively.
Timeline
A detail of the study from admission of the patient in hospital to follow up has been given in Figure 1.
Figure 1.
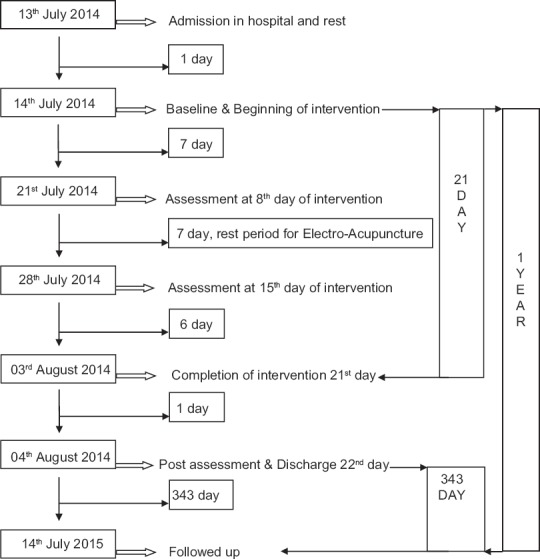
A detail of the study from admission of the patient in hospital to follow up
Intervention
Patient received clinical acupuncture for symptomatic relief of RA. We used 27-needles/session. Points given were GV-20, LI-4, LI-11, BL-11, GB-34, SP-6, KI-3, ST-44, EX-28, and EX-36, as described in Table 1.[5,8] All points were pricked bilaterally except GV-20. Patient was informed about the procedure and sensations of needle insertion, and response was sought. All needles left for 30-min, including 20-min of electrical stimulation/session to all points except GV-20, EX-28, and EX-36 by using CMNS6-1 needle stimulator, China. We used 1-cun filiform locally manufactured stainless steel needles with 0.38-mm diameter and 25-mm length. Patient received 14 sessions of EA with 7 days rest period after first 7 sessions. This rest is traditionally indicated for improvement and adaptation.[5,8] Along with acupuncture, patient received 45-min of Swedish massage, which included touch, stroking, mild friction, mild kneading and joint movements and 30-min of hot-mud application to bilateral hands and legs for 1-session/day for 6 days/week; and sauna-bath once/week for a period of 3 weeks. Assessments were done before, during, and after intervention [Table 2].
Table 1.
Description of acupuncture points
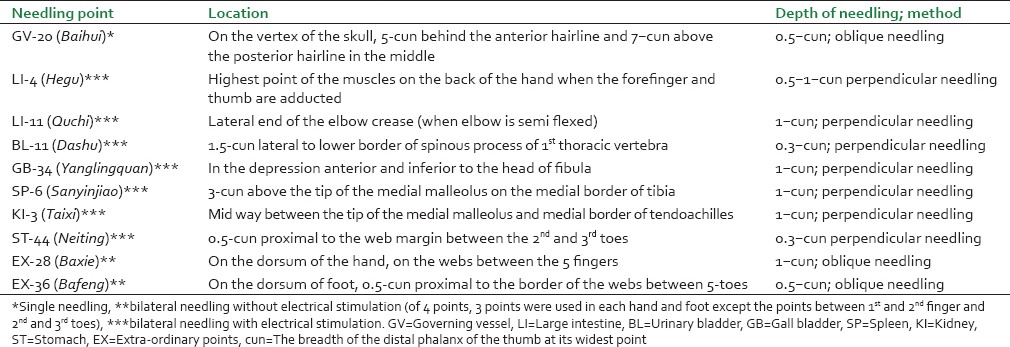
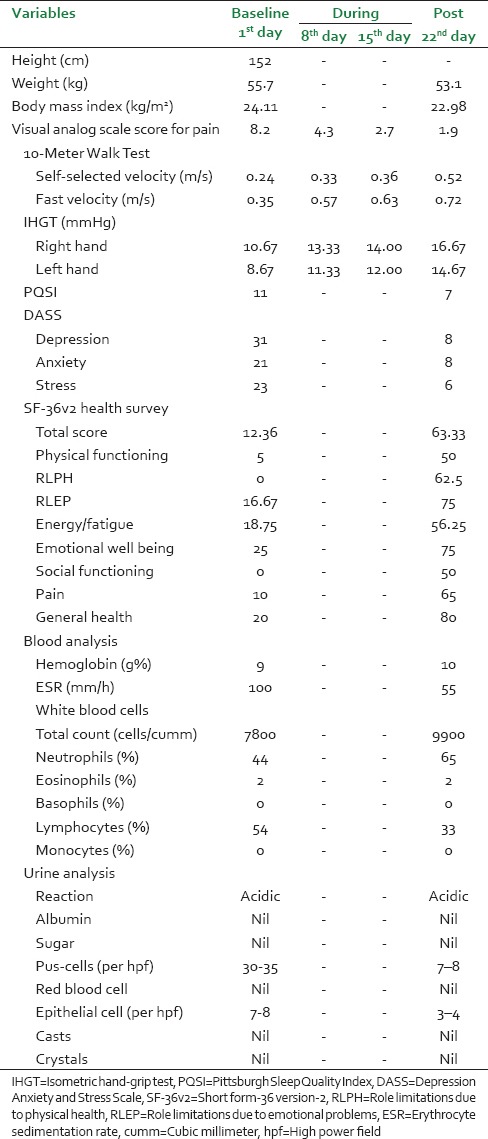
Table 2.
Baseline, during and postassessments of the subject
Outcome measures
Visual analog scale for pain
It was used to evaluate the patient's overall pain intensity of all the joints on a scale of 0–10, where 0 indicate no pain and 10 indicate worst pain. Patient was asked to mark a point on the scale to indicate her pain intensity.[5]
10-meter walk test
It was used to assess walking speed in self-selected velocity and fast velocity. Patient was advised to walk about 10-m without assistance and the time was measured for the intermediate 6-m. Four meters was left out to allow for acceleration and deceleration. We assessed 3-consecutive trials, average of which was considered as final value.[9]
Isometric hand-grip test
Sphygmomanometer cuff was inflated till the mercury column rose to 30-mmHg. Patient was advised to squeeze the cuff as much as possible on 3-successive occasions with 10-s interval. Maximum height of the mercury column reached on each occasion was measured, average of which was considered as final value.[10]
The Pittsburgh Sleep Quality Index
It consists of 7-components in 9-item sleep questionnaire. It was used to evaluate patient's QOS over the preceding month. A total score of 0–4 indicates good sleep quality, 5–10 indicates poor sleep quality, and >10 indicates sleep disorder.[5,11]
Depression Anxiety and Stress Scales
It is a 42-item questionnaire that includes 3-self-report scales designed to measure state of depression, anxiety, and stress. Each scale contains 14-item where patient was asked to use 4-point severity/frequency scales to rate the extent to which she has experienced each state over the past week.[12]
Short form-36 version-2 health survey
It is a 36-item questionnaire that measures health in 8 dimensions. For each dimension item scores were noted, averaged and transformed into a scale of 0–100 where 0 indicates worst possible health and 100 indicates best possible health. Reliability of its domains was shown to have improvement over the previous version of short form-36.[13]
Blood and urine analysis
Blood and urine analysis were done to assess hemoglobin, ESR, white blood cell (WBC) (total and differential counts); reaction, protein, sugar, pus-cells, red blood cells, epithelial-cells, casts, and crystals, respectively.
Follow-up
Patient's follow-up was through mobile communication, after 12th and 49th week of her discharge. From recent follow-up, as per patient and her son (who was with the patient during hospital stay), there is no aggravation of symptoms and improvement was seen in her health status, moreover she started taking part in domestic activities such as cooking etc., which was not the case before EMMS therapy. Since, the patient did not visit our hospital after discharge with any complaint; we did not do any kind of clinical assessments.
RESULTS AND DISCUSSION
Result of our study showed, reduction in visual analog scale (VAS), Depression Anxiety and Stress Scales (DASS), Pittsburgh Sleep Quality Index (PSQI) scores, weight, body mass index, ESR, lymphocytes, pus-cells, and epithelial-cells with increase in 10-Meter Walk Test, isometric hand-grip test, short form-36 version-2 (SF-36v2) health survey scores, hemoglobin, total WBC and neutrophils [Table 2].
There were better reduction in VAS and DASS scores with improvement in 10-Meter Walk Test, self-selected and fast velocities, hand-grip (both hands), and SF-36v2 health survey (all the 8-components), which indicates the better improvement in pain, depression, anxiety, stress, motor-functions, and QOL, respectively in this patient.
Improvement in QOS was observed through reduction in PSQI score but it did not reach the optimum level to indicate good QOS. Mild increase in hemoglobin with better reduction in ESR and Lymphocytes in blood analysis and reduction in pus-cells and epithelial-cells in urine analysis indicates the improvement in health while reduction in chronic inflammation.
This result might be attributed to effect of EMMS therapies on RA in various aspects such as pathological, psychological, mechanical etc. Acupuncture might reduce pain and inflammation through release of endogenous opioids (encephalin, dynorphin, β-endorphin, and endomorphin), serotonin[4] and by lowering tumor necrosis factor-alpha (TNF-α) and vascular endothelial growth factor in peripheral blood and joint synovia to improve internal environment for genesis and development of RA, respectively.[14] Reduction of inflammatory cells infiltration might have allowed diseased joints to heal because TNF is known to destroy articular cartilage, bone resorption, and inhibit bone formation by stimulating protein-degrading enzymes.[1]
Mud therapy might reduce pain, swelling and stiffness, while improve motor functions and daily activities. In a previous study, mud pack was shown to be safe and effective in reducing objective and subjective indices of RA activity for 3 months.[6] Massage might reduce pain, swelling, stress and anxiety; promote muscle relaxation and mobility along with improvement in QOS.[5] Sauna might produce positive effect on locomotor system, psycho-emotional status, and pain.[7] Elevated levels of both depression and anxiety occur in RA and have direct effect on pain via different mechanisms.[14] The reduction in depression, anxiety and stress scores by EMMS therapies might attribute to overall well-being of this patient because those are associated with higher levels of disease activity, pain, fatigue, work disability, health service use, lower treatment compliance, increased suicide risk, and mortality in RA.[15]
Strengths of this study
This is a first RA case, reporting the effects of EMMS therapies. It was well tolerated and no side effects were reported by the patient throughout the study period. It showed more effectiveness in RA, especially in reducing pain, and ESR which was not shown in previous studies where, they used particular treatments such as acupuncture,[4] mud,[6] and sauna.[7]
Limitations of this study
Changes in major inflammatory markers were not assessed; validity and reliability of this result may vary because of single case. Hence, further well planned clinical observational studies with advanced markers are suggested with this positive singular report. Studies are required with large sample size and advanced techniques to validate our results.
CONCLUSION
Results of this study suggest that combination of electro-acupuncture, massage, mud, and sauna therapies were well tolerated and effective in patient with RA.
INFORMED CONSENT
An informed written consent was obtained from the patient for reporting this case.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Cubick EE, Quezada VY, Schumer AD, Davis CM. Sustained release myofascial release as treatment for a patient with complications of rheumatoid arthritis and collagenous colitis: A case report. Int J Ther Massage Bodywork. 2011;4:1–9. doi: 10.3822/ijtmb.v4i3.112. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Rastogi R. Current approaches of research in naturopathy: How far is its evidence base? J Homeopath Ayurvedic Med. 2012;1:1000107. [Google Scholar]
- 3.Jadhav MP, Jadhav PM, Shelke P, Sharma Y, Nadkar M. Assessment of use of complementary alternative medicine and its impact on quality of life in the patients attending rheumatology clinic, in a tertiary care centre in India. Indian J Med Sci. 2011;65:50–7. [PubMed] [Google Scholar]
- 4.Amezaga Urruela M, Suarez-Almazor ME. Acupuncture in the treatment of rheumatic diseases. Curr Rheumatol Rep. 2012;14:589–97. doi: 10.1007/s11926-012-0295-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Mooventhan A, Nivethitha L. Effects of acupuncture and massage on pain, quality of sleep and health related quality of life in patient with systemic lupus erythematosus. J Ayurveda Integr Med. 2014;5:186–9. doi: 10.4103/0975-9476.140484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sukenik S, Buskila D, Neumann L, Kleiner-Baumgarten A, Zimlichman S, Horowitz J. Sulphur bath and mud pack treatment for rheumatoid arthritis at the Dead Sea area. Ann Rheum Dis. 1990;49:99–102. doi: 10.1136/ard.49.2.99. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Matveikov GP, Marushchak VV. An evaluation of the effect of the sauna on the clinical, laboratory and psychological indices in rheumatoid arthritis. Ter Arkh. 1993;65:48–51. [PubMed] [Google Scholar]
- 8.Jayasuriya A. New Delhi: B Jain Publishers (P) Ltd; 2013. Clinical Acupuncture. Revised Edition 2001. [Google Scholar]
- 9.Wolf SL, Catlin PA, Gage K, Gurucharri K, Robertson R, Stephen K. Establishing the reliability and validity of measurements of walking time using the Emory Functional Ambulation Profile. Phys Ther. 1999;79:1122–33. [PubMed] [Google Scholar]
- 10.Downie WW, Leatham PA, Rhind VM, Pickup ME, Wright V. The visual analogue scale in the assessment of grip strength. Ann Rheum Dis. 1978;37:382–4. doi: 10.1136/ard.37.4.382. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Buysse DJ, Reynolds CF, 3rd, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: A new instrument for psychiatric practice and research. Psychiatry Res. 1989;28:193–213. doi: 10.1016/0165-1781(89)90047-4. [DOI] [PubMed] [Google Scholar]
- 12.Lovibond SH, Lovibond PF. 2nd ed. Sydney: Psychology Foundation; 1995. Manual for the Depression Anxiety Stress Scales. [Google Scholar]
- 13.Jenkinson C, Stewart-Brown S, Petersen S, Paice C. Assessment of the SF-36 version 2 in the United Kingdom. J Epidemiol Community Health. 1999;53:46–50. doi: 10.1136/jech.53.1.46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Ouyang BS, Gao J, Che JL, Zhang Y, Li J, Yang HZ, et al. Effect of electro-acupuncture on tumor necrosis factor-a and vascular endothelial growth factor in peripheral blood and joint synovia of patients with rheumatoid arthritis. Chin J Integr Med. 2011;17:505–9. doi: 10.1007/s11655-011-0783-2. [DOI] [PubMed] [Google Scholar]
- 15.Covic T, Cumming SR, Pallant JF, Manolios N, Emery P, Conaghan PG, et al. Depression and anxiety in patients with rheumatoid arthritis: Prevalence rates based on a comparison of the Depression, Anxiety and Stress Scale (DASS) and the Hospital, Anxiety and Depression Scale (HADS) BMC Psychiatry. 2012;12:6. doi: 10.1186/1471-244X-12-6. [DOI] [PMC free article] [PubMed] [Google Scholar]