

Abstract
Introduction:
Nephrolithiasis is a common problem worldwide especially in areas of the hot climate like Saudi Arabia. The aim of this analysis was to study the characteristics of urinary stones in Eastern Saudi Arabia and to report the following: Composition of urinary stones, age and gender distribution, seasonal variation of stone development, comorbid conditions associated with stone development and the incidence of urinary stones.
Methods:
All urinary stones that were submitted to the Johns Hopkins Aramco Healthcare, previously Saudi Aramco Medical Services Organization for analysis from January 2011 through January 2013 were analyzed.
Results:
A total of 384 urinary stones were collected and submitted for analysis from 347 patients. There was a male predominance with a male: female ratio of 3.9:1. The average age was 48.5 ± 12.8 years. Weight abnormality was predominant in both genders, and especially females. Calcium-based stones constituted the great majority (84.6%) followed by uric acid stones (12.8%). The other forms of stones were rare. More stones were recovered during the hot season, May to September. The calculated annual incidence of urolithiasis was 111/100,000 individuals.
Conclusion:
Calcium based stones are the most common urinary stones observed in Eastern Saudi Arabia. There is a clear association between the diagnosis of urinary stones and the hot season
Keywords: Nephrolithiasis, Saudi Arabia, urinary calculi, urolithiasis
INTRODUCTION
Urolithiasis is a common problem with an increasing incidence and prevalence worldwide.[1] There is a geographical variability of urolithiasis with higher prevalence of stone formation in areas of hot climate as compared to moderate climate.[2,3,4,5] Decreased fluid intake, increased perspiration, and increased urinary concentration could predispose to increased crystallization and stone formation. Besides climatic conditions, there are other factors that predispose to stone formation such as genetic factors, dietary habits, water hardness, race, gender, age, occupation, and body weight.[1,4,6,7] Here, we report on the chemical composition of urinary stones and the association with metabolic abnormalities and climatic changes in Eastern Saudi Arabia.
METHODS
We retrospectively analyzed the data of all urinary stones that were submitted for analysis over a period of 25 months – from January 2011 through January 2013. Information was extracted from the computer database at Johns Hopkins Aramco Healthcare (JHAH), previously Saudi Aramco Medical Services Organization. The stones were either passed spontaneously or after fragmentation by shock wave lithotripsy; or extracted surgically by ureteroscopy or percutaneous nephrolithotomy. All stones were submitted to the laboratory of JHAH. No distinction was made between renal stones and urinary bladder stones.
Each stone was kept clean, dry, and transported in a screw-capped plastic container to the Urolithiasis Laboratory in Houston, Texas. All stones were analyzed using infrared spectrum analysis. In brief, representative specimens were taken from all identifiable layers of the calculus. Each specimen was weighed and crushed into a fine powder. An infrared spectrum of each specimen was recorded, and the resulting spectrum compared against reference spectra of all known calculus components including calcium, magnesium, oxalate, uric acid, carbonate, phosphate, ammonia, and cystine.[8]
In addition to the chemical composition of the stones, baseline variables including age, gender, weight, co-existence of co-morbid conditions including diabetes mellitus (DM), hypertension (HTN), dyslipidemia, and hyperuricemia were collected. Time of the year was divided into two seasons, a hot season beginning in May until the end of September, and a moderate season extending from October until the end of April. Meteorological data about the monthly temperature for the city of Dhahran was obtained from the website of the National Meteorology and Environment Center, a branch of the Jiddah Regional Climate Center of South-West Asia located in Jiddah, Saudi Arabia, for the years 1999–2010.[9]
Statistical analysis
Continuous variables were reported as means ± standard deviation, and categorical variables were reported as proportions. Student's t-test was used to compare the means. Pearson correlation test was used to calculate the correlation coefficient between the data sets. P values < 0.05 were considered to be significant. The statistical analyses were performed using Microsoft Office Excel 2010.
The study was approved by the Institutional Review Boards at JHAH.
RESULTS
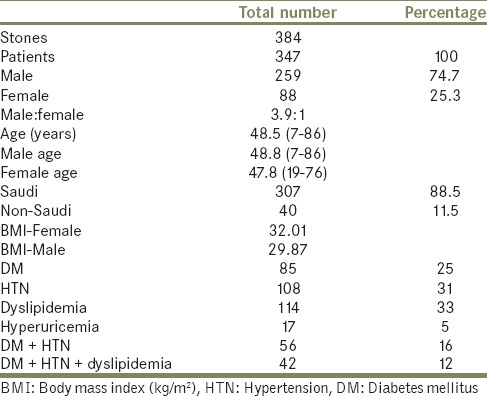
The total number of individuals registered for medical care at JHAH in 2011 and 2012 were 155, 169 and 153, 194, respectively. A total of 384 stones from 347 patients were submitted for analysis between January 1, 2011 and January 31, 2013. Saudi citizens accounted for 307 of the patients and 40 were expatriates. There were 259 males and 88 females, with a male to female ratio of 3.9:1. The mean age was 48.82 ± 12.96 and 47.77 ± 11.2 years for male and female patients, respectively, P = 0.25. The majority of patients were either overweight or obese. The mean body mass index was higher in females compared with males (32.01 ± 11.65 and 29.87 ± 5.95 kg/m2, respectively, P = 0.013) [Table 1]. Metabolic abnormalities including HTN, DM, dyslipidemia, and hyperuricemia were found in a large proportion of patients as shown in Table 1.
Table 1.
Demographics of the study population
Pure calcium oxalate stones were the predominant form accounting for 74.2% of all stones followed by uric acid stones (12.8%) and mixed calcium oxalate/phosphate/uric acid stones (10.4%). There were only five calcium apatite stones, two struvite stones, and three ammonium acid urate stones [Figure 1]. More stones were obtained during the hot season from May to September than during the moderate season from October through April, P = 0.0034 [Figure 2]. There was a positive correlation between the time of the year when the stones were obtained and the monthly temperature, correlation coefficient 0.599. The calculated annual incidence of urolithiasis was 111/100,000 individuals.
Figure 1.
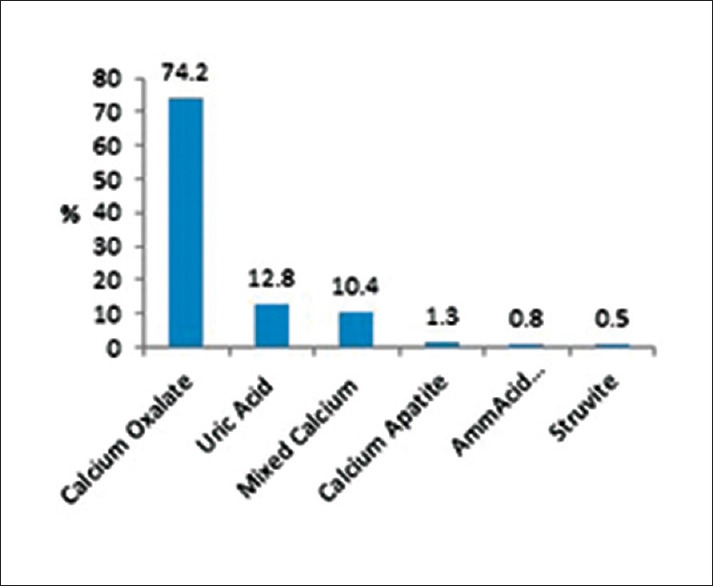
Chemical composition of the urinary stones. Amm Acid: Ammonium acid urate
Figure 2.
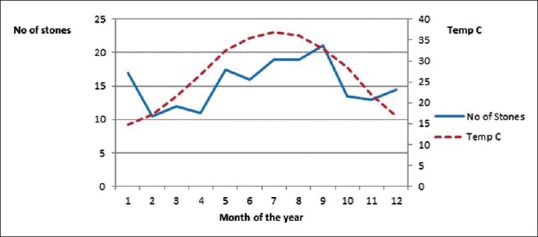
Monthly number of urinary stones in relation to the average monthly temperature from 1999 to 2010. Temp C: Temperature in celsius
DISCUSSION
Urolithiasis is a common problem with increasing incidence and prevalence worldwide.[1] There are several factors that contribute to the development of urolithiasis including genetic factors, dietary habits, water hardness, weather factors, race, gender, age, occupation, and body weight.[1,4,6,7] Besides the adverse health consequences of urolithiasis, there is a huge cost implication related to providing medical care to the affected individuals and loss of working hours. Identification of the chemical composition of stones is an essential step in the metabolic evaluation and treatment of urolithiasis.
Some earlier studies have investigated various aspects of kidney stones in the central and western regions of the country. Al-Hadramy looked at the seasonal variation of renal colics in the western region of Saudi Arabia as reported to the emergency department, and found more renal colic presentations during the hot summer months.[10] Khan et al. looked at the epidemiological risk factors and composition of urinary stones in the middle region of Saudi Arabia. In that analysis, the authors found a high male: female predominance of 5:1, and clear association with the hot months.[11] Similar to our report, calcium oxalate stones were found to be the most common followed by uric acid and phosphate stones.
Eastern Saudi Arabia is known for its extreme hot climate during the summer months with temperatures up to 50°C. We have observed a higher passage of urinary stones during the hot season. This observation has been previously reported by several investigators in other areas.[2,3,4,5,10,11,12,13] The explanation is that dehydration–with the consequent concentrated urine-promotes an increase in urinary supersaturation, crystallization, and stone formation.[3]
Due to the changes in lifestyle of the Saudi population, an alarming increase in the prevalence of obesity in all parts of the country has been observed.[14] Weight abnormality has reached an epidemic level, where, in some parts of the country, two-third of the population is either obese or overweight.[15] Besides the many health consequences associated with obesity, a rise in the prevalence of urinary stones will be expected.
In addition to obesity, the metabolic syndrome has been implicated as a risk factor for the formation of both calcium oxalate and uric acid kidney stones.[16,17,18] High urinary acid excretion that results in lowering the urine pH was found to be a feature of the metabolic syndrome and was associated with the degree of insulin resistance.[19] In addition to the weight abnormalities observed in our cohort, a substantial proportion of the patients had one or more metabolic abnormality such as HTN, DM, dyslipidemia or hyperuricemia.
This study has several limitations, mainly related to the retrospective nature of the study. Since stones may pass spontaneously and may be discarded by patients, the data presented herein may be biased toward the stones that were submitted for analysis, and do not necessarily represent the actual number of stones. Therefore, the incidence of urinary stones reported in our study may underestimate the true incidence of urolithiasis. The metabolic abnormalities and comorbidities found in patients with urinary stones were based on the recorded information in the digital data system. Failure to update the patients’ significant data would underestimate the true association between urinary stones and the metabolic abnormalities. However, the relatively large number of stones and patients included in the study would minimize the effect of these variables and should give a fair assessment of urinary stones and the associated comorbidities. A prospective study will more accurately answer some of the questions related to urolithiasis in this area.
CONCLUSION
This study is the first to address urolithiasis in Eastern Saudi Arabia. Our finding confirms that pure calcium oxalate was the dominant form of urolithiasis followed by uric acid stones and mixed calcium stones. The other types of stones were very rare. We also have observed a seasonal variation in the development of urolithiasis with more stones diagnosed during the hot season.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Romero V, Akpinar H, Assimos DG. Kidney stones: A global picture of prevalence, incidence, and associated risk factors. Rev Urol. 2010;12:e86–96. [PMC free article] [PubMed] [Google Scholar]
- 2.Soucie JM, Thun MJ, Coates RJ, McClellan W, Austin H. Demographic and geographic variability of kidney stones in the United States. Kidney Int. 1994;46:893–9. doi: 10.1038/ki.1994.347. [DOI] [PubMed] [Google Scholar]
- 3.Boscolo-Berto R, Dal Moro F, Abate A, Arandjelovic G, Tosato F, Bassi P. Do weather conditions influence the onset of renal colic?. A novel approach to analysis. Urol Int. 2008;80:19–25. doi: 10.1159/000111724. [DOI] [PubMed] [Google Scholar]
- 4.Elliott JP, Jr, Gordon JO, Evans JW, Platt L. A stone season. A 10-year retrospective study of 768 surgical stone cases with respect to seasonal variation. J Urol. 1975;114:574–7. doi: 10.1016/s0022-5347(17)67085-x. [DOI] [PubMed] [Google Scholar]
- 5.Brikowski TH, Lotan Y, Pearle MS. Climate-related increase in the prevalence of urolithiasis in the United States. Proc Natl Acad Sci U S A. 2008;105:9841–6. doi: 10.1073/pnas.0709652105. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Gault MH, Chafe L. Relationship of frequency, age, sex, stone weight and composition in 15,624 stones: Comparison of resutls for 1980 to 1983 and 1995 to 1998. J Urol. 2000;164:302–7. [PubMed] [Google Scholar]
- 7.Knoll T. Epidemiology, pathogenesis, and pathophysiology of urolithiasis. Eur Urol Suppl. 2010;9:802–6. [Google Scholar]
- 8.Hesse A, Bach D. Stone analysis by infrared, spectroscopy. In: Alan Rose., editor. Urinary stones. Baltimore: Aspects: University Park Press; 1982. pp. 87–105. [Google Scholar]
- 9.National Meteorology and Environment Center. 2014. [Last assessed date 2015 Feb 24]. Available from: http://www.jrcc.sa/
- 10.al-Hadramy MS. Seasonal variations of urinary stone colic in Arabia. J Pak Med Assoc. 1997;47:281–4. [PubMed] [Google Scholar]
- 11.Khan AS, Rai ME, Gandapur, Pervaiz A, Shah AH, Hussain AA, et al. Epidemiological risk factors and composition of urinary stones in Riyadh Saudi Arabia. J Ayub Med Coll Abbottabad. 2004;16:56–8. [PubMed] [Google Scholar]
- 12.Fujita K. Weather and the incidence of urinary stone colic. J Urol. 1979;121:318–9. doi: 10.1016/s0022-5347(17)56768-3. [DOI] [PubMed] [Google Scholar]
- 13.Chen YK, Lin HC, Chen CS, Yeh SD. Seasonal variations in urinary calculi attacks and their association with climate: A population based study. J Urol. 2008;179:564–9. doi: 10.1016/j.juro.2007.09.067. [DOI] [PubMed] [Google Scholar]
- 14.Al-Nozha MM, Al-Mazrou YY, Al-Maatouq MA, Arafah MR, Khalil MZ, Khan NB, et al. Obesity in Saudi Arabia. Saudi Med J. 2005;26:824–9. [PubMed] [Google Scholar]
- 15.Al-Othaimeen AI, Al-Nozha M, Osman AK. Obesity: An emerging problem in Saudi Arabia. Analysis of data from the National Nutrition Survey. East Mediterr Health J. 2007;13:441–8. [PubMed] [Google Scholar]
- 16.West B, Luke A, Durazo-Arvizu RA, Cao G, Shoham D, Kramer H. Metabolic syndrome and self-reported history of kidney stones: The National Health and Nutrition Examination Survey (NHANES III) 1988-1994. Am J Kidney Dis. 2008;51:741–7. doi: 10.1053/j.ajkd.2007.12.030. [DOI] [PubMed] [Google Scholar]
- 17.Taylor EN, Stampfer MJ, Curhan GC. Obesity, weight gain, and the risk of kidney stones. JAMA. 2005;293:455–62. doi: 10.1001/jama.293.4.455. [DOI] [PubMed] [Google Scholar]
- 18.Daudon M, Traxer O, Conort P, Lacour B, Jungers P. Type 2 diabetes increases the risk for uric acid stones. J Am Soc Nephrol. 2006;17:2026–33. doi: 10.1681/ASN.2006030262. [DOI] [PubMed] [Google Scholar]
- 19.Maalouf NM, Cameron MA, Moe OW, Adams-Huet B, Sakhaee K. Low urine pH: A novel feature of the metabolic syndrome. Clin J Am Soc Nephrol. 2007;2:883–8. doi: 10.2215/CJN.00670207. [DOI] [PubMed] [Google Scholar]