

Abstract
Background
Dysmenorrhea is a common gynecological complaint in adolescent and young females. The purpose of this study is to assess the efficacy of Shaofu Zhuyu (SFZY) decoctions as treatments for primary dysmenorrhea.
Methods/design
Fifteen (four English, seven Korean, three Chinese, and one Japanese) databases will be searched from their inception without a language restriction. These include PubMed, AMED, EMBASE, The Cochrane Library, seven Korean Medical Databases (Korean Studies Information, DBPIA, Oriental Medicine Advanced Searching Integrated System, Research Information Service System, KoreaMed, The Town Society of Science Technology, and the Korean National Assembly Library), three Chinese Medical Databases [the Chinese Medical Database (CNKI), Chongqing VIP Chinese Science and Technology Periodical Database (VIP), and WanFang Database], and one Japanese Database (J global). Randomized clinical trials (RCTs) included those that examined an SFZY decoction or a modified SFZY decoction. The control groups include no treatment, placebo, and medication. Trials testing a combination of SFZY decoction and medication compare to the same medication alone will be also included. Data extraction and risk of bias assessments will be performed by two independent reviewers. All statistical analyses will be conducted using Review Manager software (RevMan V.5.3.0). Methodological quality will be assessed with the Cochrane risk of bias tool.
Discussion
This systematic review will provide a detailed summary of the available evidence testing the effects of SFZY decoctions for the treatment of primary dysmenorrhea. The review will benefit patients and practitioners in the fields of traditional and complementary medicine.
Systematic review registration
PROSPERO registration number: CRD42015016386
Keyword: Herbal medicine, Shaofu Zhuyu decoction, Dysmenorrhea, Randomized controlled trials (RCTs), Systematic review
Background
Description of the condition
Dysmenorrhea is a common gynecological complaint in adolescent and young females. Dysmenorrhea is characterized by lower abdominal pain that occurs during menstruation [1]. Different types of studies have found a consistently high prevalence of dysmenorrhea in women of different ages and nationalities with an estimated prevalence ranging from 45 to 97 % [2]. Ten percent of these women suffer from symptoms severe enough to render them incapacitated for 1 to 3 days each menstrual cycle [3]. Period pain can lead to absences from school or work [4]. In the USA alone, it was estimated that in the mid-1980s, 600 million hours were lost from work, which led to an economic loss of two billion dollars; in today’s dollars, this figure would be much higher [5].
How the intervention might work
The mechanisms of primary dysmenorrhea have been attributed to high serum levels of prostaglandin E2 (PGE2), prostaglandin F2-α (PGF2-α), and leukotriene [6]. Severe myometrial contractions, vasoconstriction, uterine ischemia, and subsequent dysmenorrheic pain result from the release of these cytokines. Moreover, withdrawal of progesterone before the beginning of the menstrual cycle initiates arachidonic acid release and further elevates cytokine levels due to the degradation of arachidonic acid. Higher cytokine levels contribute to a higher intensity of dysmenorrheic pain and associated symptoms [7]. Non-steroid anti-inflammatory drugs (NSAIDs), therefore, are the primary treatment for this condition but are limited by inadequate pain control, gastrointestinal discomfort, and an impact on renal function. Combined oral contraceptives are also frequently used but are not universally accepted possibly due to their potential side effects including inducing endometriosis [8]. Therefore, complementary and alternative medicine (CAM) is in high demand in many countries [9]. In one large study, as many as 48 % of women reported the use of CAM as an alternative to prescription medication or to enhance the effectiveness of their prescription medications [10, 11]. Recenlty, it was reported that Shaofu Zhuyu (SFZY) decoction have the efficacy of uterine smooth muscle constriction and manifested an anti-inflammatory efficacy [12]. Also, SFZY decoction improved hemorheological factor of blood stasis and regulation for activity on rat ovary [13].
Description of the intervention
Herbal medicine is currently used in hospitals and clinics in Korea [14], China [2], Taiwan [15], and Japan [16] for the treatment of primary dysmenorrhea. SFZY decoction was first described in the Yi Lin Gai Cuo, which is a famous formula that has been used for treating primary dysmenorrhea in China since the Qing dynasty. This decoction is used, particularly in gynecology, for blood stasis accompanied by masses and gatherings in the lower abdomen [17]. Clinically, it has been used for the treatment of chronic pelvic inflammatory disease, infertility, endometrial hyperplasia, myoma uteri, and uterine cancer [18]. Many reports have described its efficacy for treating vascular disorders and pain [19], endometriosis [20], cancer [21], and menstrual irregularities in vivo [22]. SFZY decoction composed of ten herbs by Quin-ren Wang in Qing dynasty: Fructus Foeniculi, Zingiberis Rhizoma, Cinnamomi Cortex, Paeoniae Rubra Radix, Angelica Sinensis Radix, Carthami Flos, Myrrha, Corydalis Rhizoma, Typhae Pollen, and Trogopterori Faeces, in the ratio of 0.5:1:1:1:3:1:1:1:3:2 on a dry weight basis [12]. The detail of composition is shown Table 1. The composition of China came from Qing dynasty and decoction of Korean came from DongUiBoGam. SFZY decoctions have shown an effect on uterine muscles and may help to prevent and cure dysmenorrhea. SFZY decoctions are considered an effective prescription for treating primary dysmenorrhea [23], which has been reported as one of the most common gynecological disorders in young women [24].
Table 1.
Compositions of Shaofu Zhuyu decoction
| Name of herbs | Scientific name | Amount (g) | ||
|---|---|---|---|---|
| Chinaa | Modifyb | Koreac | ||
| Foeniculi Fructus | Foeniculum vulgare Mill. | 0.5 | 0.5 | 4.0 |
| Zingiberis Rhizoma | Zingiber officinale Roscoe | 1.0 | 1 | 0.8 |
| Carthami Flos | Corydalis ternata Nakai | 1.0 | 2 | 4.0 |
| Myrrha | Commiphora molmol Engler | 1.0 | 1 | 4.0 |
| Angelicae Sinens Radix | Angelica gigas N. | 3.0 | 3 | 12.0 |
| Cnidii Rhizoma | Cnidium officinale Makino | 1.0 | 1 | 4.0 |
| Cinnammomi Cortex | Cinnamomum loureirii Nees | 1.0 | 1 | 4.0 |
| Paeoniae Rubra Radix | Paeonia obovata Maxim | 1.0 | 2 | 8.0 |
| Typhae Pollen | Typha angustifolia L. | 3.0 | 1 | 12.0 |
| Trogopterori Faeces | Trogopterus xanthipes | 2.0 | 3 | 8.0 |
aQing-ren Wang, “Correction of Errors in Medical Classics”
bXiaochen Huang et al., J Chromatogr B Analyt Technol Biomed Life Sci. 2014; 1;962:75–81
cJun Heo, “DongUiBoGam”
Why is performing this review important?
Recently, many studies have reported treatments using herbal formulas. The Cochrane Review on Chinese herbal medicine showed promising evidence for the use of Traditional Chinese Medicine (TCM) in reducing menstrual pain in primary dysmenorrhea. Unfortunately, many of the studies supporting the use of Chinese herbs were of poor quality [25, 26].
Currently, no relevant systematic reviews of the efficacy of SFZY decoctions for treating primary dysmenorrhea are conducted.
Objectives
The aim of this study is to systematically review the available literature regarding the efficacy of SFZY decoctions in treating primary dysmenorrhea.
Methods/design
This study has been registered with international Prospective Register of Systematic Reviews (PROSPERO): CRD42015016386.
Criteria for including studies in this review
Type of studies
Only randomized controlled trials (RCTs) and quasi-RCTs will be included.
Type of participants
This study will include women of reproductive age with primary dysmenorrhea, i.e., individuals with no identifiable pelvic pathology as indicated by a pelvic examination, ultrasound scans and laparoscopy, or women self-reporting a diagnosis of primary dysmenorrhea.
Types of interventions
Studies that used an SFZY decoction or a modified SFZY decoction will be included. SFZY decoctions will include the following ten formulas: Fructus Foeniculi, Zingiberis Rhizoma, Cinnamomi Cortex, Paeoniae Rubra Radix, Angelica Sinensis Radix, Carthami Flos, Myrrha, Corydalis Rhizoma, Typhae Pollen, and Trogopterori Faeces [17]. Modified SFZY decoction formulas will be included as well. Modified SFZY decoctions prescribe according to TCM syndrome differentiation will be acceptable and be defined by practitioners as adding only herbs to the original herbs, resulting in nearly the same actions as the original SFZY decoction. All types of herbal medicines will be included. There is no limitation on the number of herbs, administration methods dosage, or duration of treatment.
Types of comparisons
The control groups will consist of no treatment, placebo, and medication. Trials examining a combination of SFZY decoctions and medication will compare to the same medication alone will be also included.
Outcome measures
Primary outcomes
Pain: a reduction in pain (i.e., menstrual pain) that occurs only during the intervention or occurred as a result of the intervention, measure by a visual analogue scale (VAS), other validated scales, or as a dichotomous outcome.
Response rate: an overall reduction in symptoms (other menstruation-related symptoms) that occurs only during the intervention or occurred as a result of the intervention, measure by changes in dysmenorrhea symptoms and treatment effectiveness, and is either self-reported, observed, or reported by other similar measures.
Secondary outcomes
Adverse effects: measured by any relevant incidence and duration of any side effects.
Quality of life: measured by a validated scale.
Search methods for identifying the studies
Electronic searches
The following databases will be searched from their inception: PubMed, AMED, EMBASE, The Cochrane Library, seven Korean Medical Databases (Korean Studies Information, DBPIA, Oriental Medicine Advanced Searching Integrated System, Research Information Service System, KoreaMed, The Town Society of Science Technology, and the Korean National Assembly Library), three Chinese Medical Databases [the Chinese Medical Database (CNKI), Chongqing VIP Chinese Science and Technology Periodical Database (VIP), and WanFang Database], and one Japanese Database (J global).
Other sources
Studies will also be obtained from the following sources:
The reference lists of all relevant articles
Hand searching of department files
Unpublished conference proceedings relevant to primary dysmenorrhoea will be reviewed, if available
Search strategy
The strategy for searching the databases is presented in Tables 2 and 3. Similar search strategies will be applied for all databases. In addition, the reference lists of all retrieved articles will be hand-searched for further relevant literature. Hard copies of all included articles will be read in full. Because all of the various databases use for this study possessed their own subject headings, each database will be searched independently.
Table 2.
Search strategy used in PubMed
| Number | Search items |
|---|---|
| 1 Related to intervention | 少腹逐瘀汤 |
| 2 | Shaofu Zhuyu decoction |
| 3 | Shaofu Zhuyu formula |
| 4 | Shaofu Zhuyu tang |
| 5 | 1 or 2–5 |
| 6 Related to disease | Dysmenorrhea |
| 7 | Menstruation disturbances |
| 8 | Menstrual disorder |
| 9 | Pelvic pain |
| 10 | Painful menstruation |
| 11 | Painful period |
| 12 | Period pain |
| 13 | Primary dysmenorrhea |
| 14 | 7 or 8–14 |
| 15 Related to study design | Randomized controlled trial |
| 16 | Controlled clinical trial |
| 17 | Randomized |
| 18 | Placebo |
| 19 | Drug therapy |
| 20 | Randomly |
| 21 | Trial |
| 22 | Groups |
| 23 | #15 OR #16 OR #17 OR #18 OR #19 OR #20 OR #21 OR #22 |
| 24 | Animals NOT humans |
| 25 | #23 NOT #25 |
Any words containing this searching item will be searched. This search strategy will be suitable for other electronic databases
Table 3.
Search strategy used in CNKI
| Number | Search items |
|---|---|
| 1 Related to intervention | 少腹逐瘀汤 |
| 2 | Shaofu Zhuyu decoction |
| 3 | Shaofu Zhuyu formula |
| 4 | Shaofu Zhuyu tang |
| 5 | 1 or 2–5 |
| 6 Related to disease | 痛经 |
| 7 | 原发性痛经 |
| 8 | 月经痛 |
| 9 | 经期腹痛 |
| 10 | 经痛 |
| 11 | Dysmenorrhea |
| 12 | Primary dysmenorrhea |
| 13 | Menstrual disorder |
| 14 | Pelvic pain |
| 15 | Menstruation disturbances |
| 16 | 6 or 7–15 |
| 17 Related to study design | 随机 |
| 18 | 对照 |
| 19 | 临床研究 |
| 20 | Controlled trial |
| 21 | Randomized controlled trial |
| 22 | 17 or 18–22 |
| 23 | 6 and 16 and 22 |
Data collection and analysis
Selection of studies
Two reviewers (HYL and TYC) will review and screen the titles and abstracts to identify eligible trials according to the inclusion criteria. Disagreements will be resolved by discussion, if necessary, by the arbiter (MSL). Details of the study selection procedure are shown in Fig. 1.
Fig. 1.
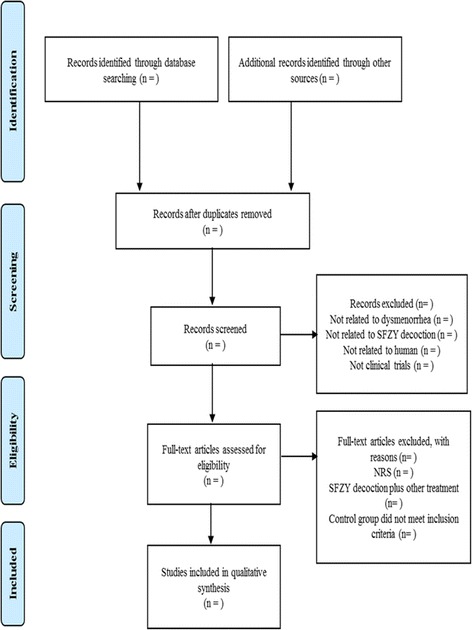
PRISMA diagram for the included studies. NRS non-randomized studies, SFZY Shaofu Zhuyu
Data extraction
All articles will be performed by two authors (HYL and TYC) who extract data according to pre-defined criteria. Information such as the participants, interventions, outcomes, and results will be obtained from each report. Any disagreement between the two authors will be resolved by discussion. Another author (MSL) will act as an arbiter for unresolved disagreements.
Assessment of bias in the included studies
Two authors (HYL and TYC) will assess the risk of bias using the following seven criteria from the Cochrane classification: (1) random sequence generation, (2) allocation concealment, (3) blinding of participants and personnel, (4) blinding of outcome assessment, (5) incomplete outcome data, (6) selective outcome reporting, and (7) other sources of bias (we evaluate baseline imbalance) [27]. This review uses “L, U and H” as judgments keys; “Low” indicates a low risk of bias (L), “Unclear” indicates that the risk of bias is uncertain (U), and “High” indicates a high risk of bias (H). Disagreements will be resolved by discussions between all reviewers.
Data synthesis
All statistical analyses will be conducted using the Cochrane Collaboration’s software program, Review Manager (RevMan), Version 5.3.0 for Windows (Copenhagen, The Nordic Cochrane Center). Differences between the intervention and control groups will be assessed. For the continuous data, we will use the mean difference (MD) with 95 % confidence intervals (CI) to measure the treatment effect. We will convert other forms of data into MDs. In the case of outcome variables with different scales, we will use the standardized mean difference (SMD) with 95 % Cis. For dichotomous data, we will present the treatment effects as a relative risk (RR) with 95 % Cis. We will convert other binary data into the RR form. For studies with insufficient information, we will contact the primary authors to acquire and verify data when possible. The chi-square test for heterogeneity and the I2 test will be used to evaluate the heterogeneity of the included studies. Unless excessive statistical heterogeneity is present, we will pool the data across studies for the meta-analysis using a fixed effects model.
Unit of analysis issues
For cross-over trials, data from the first treatment period will be used. For trials in which more than one control group will be assessed, the primary analysis will combine the data from each control group. Subgroup analyses of the control groups will also be performed. Each patient will be counted only once in the analysis.
Dealing with the missing data
Intention-to-treat analyses that include all of the randomized patients will be performed. For patients with missing outcome data, a carry-forward of the last observed response will be used. The individual patient data will be sought from the original source or the published trial reports when the individual patient data are unavailable.
Assessment of heterogeneity
We will use the random effects or fixed effects model for the meta-analysis according to the data analysis. If a meta-analysis is possible, we will use the I2 statistic to quantify the inconsistencies among the included studies. According to the guidance given in the Cochrane Handbook for Systematic Reviews of Interventions, as a general rule, I2 values of up to 25 % provide evidence of low heterogeneity; a value of 50 % is considered moderate heterogeneity and 75 % or above is considered as a high heterogeneity. In the presence of significant heterogeneity, the causes of heterogeneity will be examined by pre-specified subgroup analysis and also sensitivity analysis, if possible. Where subgroup analysis fails to explain the heterogeneity, then data will be analyzed using the random effects model. If heterogeneity is observed, we will conduct a subgroup analysis to explore the possible causes [28].
Assessment of reporting biases
If a sufficient number of included studies (at least ten trials) are available, we will use funnel plots to detect reporting biases. However, funnel plot asymmetry is not the same as publication bias; therefore, we will attempt to distinguish the possible reasons for the asymmetry, such as small-study effects, poor methodological quality, and true heterogeneity in the included [29, 30].
Subgroup analysis and investigation of heterogeneity
If there are an adequate number of studies, we will conduct subgroup analyses to interpret the heterogeneity between the studies, including the following:
Type of design: SFZY decoction treatment used alone or as combination therapy with SFZY decoction and conventional therapy
Type of intervention: type of herbal medicines (SFZY decoction or modified SFZY decoction)
Sensitivity analysis
We will conduct sensitivity analysis to test the robustness of the primary decisions of the review process. The principal decision nodes conclude methodological quality, sample size and the effect of missing data. The meta-analysis will be repeated, and studies of lower quality will be excluded. The result will be compared and discussed according to the results.
Ethics and dissemination
Ethical approval is not required, given that this protocol is for a systematic review. The findings of this review will be disseminated widely through peer-reviewed publications and conference presentations.
Discussion
As a primary data collection will not be undertaken, no additional formal ethical assessment or informed consent is required. The systematic review will be published in a peer-reviewed journal and disseminated electronically or in print. Updates of the review will be conducted to inform and guide healthcare practice and policy. In this review, we will collect data on the safety and efficacy of SFZY decoctions for treatment of primary dysmenorrhea. The review will fuel the development of treatment of primary dysmenorrhea patients using traditional and complementary medicine.
Acknowledgments
Funding
This research was supported by grants from Korea Institute of Oriental Medicine (#K15110).
Abbreviations
- CAM
complementary and alternative medicine
- CI
confidence intervals
- NSAIDs
non-steroid anti-inflammatory drugs
- PGE2
prostaglandin E2
- PGF2-α
prostaglandin F2-α
- RCTs
randomized controlled trials
- RR
relative risk
- SFZY
Shaofu Zhuyu
- TCM
Traditional Chinese Medicine
- VAS
visual analogue scale
Footnotes
Competing interests
The authors declare that they have no competing interests.
Authors’ contributions
All authors participated in the preparation of the research. HYL is TYC extracted the data according articles were read by two independent reviewers (HYL & TYC) who extracted data according to pre-defined criteria. MSL and CSM acted as an arbiter for unresolved disagreements. All authors read and approved the final.
Contributor Information
Hoyoung Lee, Email: lhoyoung@kiom.re.kr.
Tae-Young Choi, Email: superoung@kiom.re.kr.
Chang-Seon Myung, Phone: +82-42-821-5923, Email: cm8r@cnu.ac.kr.
Myeong Soo Lee, Phone: 82-(0)42-868-9266, Email: drmslee@gmail.com.
References
- 1.Tangchai K, Titapant V, Boriboonhirunsarn D. Dysmenorrhea in Thai adolescents: prevalence, impact and knowledge of treatment. J Med Assoc Thai. 2004;87(Suppl 3):S69–S73. [PubMed] [Google Scholar]
- 2.Chen Y, Cao Y, Xie Y, Zhang X, Yang Q, Li X, et al. Traditional Chinese medicine for the treatment of primary dysmenorrhea: how do Yuanhu painkillers effectively treat dysmenorrhea? Phytomedicine. 2013;20(12):1095–1104. doi: 10.1016/j.phymed.2013.05.003. [DOI] [PubMed] [Google Scholar]
- 3.Dawood M. Dysmenorrhea. Clin Obstet Gynecol. 1990;33(1):168–178. doi: 10.1097/00003081-199003000-00023. [DOI] [PubMed] [Google Scholar]
- 4.French L. Dysmenorrhoea. Am Fam Physician. 2005;71(2):285–291. [PubMed] [Google Scholar]
- 5.Dawood M. Ibuprofen and dysmenorrhoea. Am J Med. 1984;77(1A):87–94. doi: 10.1016/S0002-9343(84)80025-X. [DOI] [PubMed] [Google Scholar]
- 6.Lundstrom V, Green K. Endogenous levels of prostaglandin F2alpha and its main metabolites in plasma and endometrium of normal and dysmenorrheic women. Am J Obstet Gynecol. 1978;130(6):640–646. doi: 10.1016/0002-9378(78)90320-4. [DOI] [PubMed] [Google Scholar]
- 7.Lumsden MA, Kelly RW, Baird DT. Primary dysmenorrhoea: the importance of both prostaglandins E2 and F2 alpha. Br J Obstet Gynaecol. 1983;90:1135–1140. doi: 10.1111/j.1471-0528.1983.tb06460.x. [DOI] [PubMed] [Google Scholar]
- 8.Guo XL, Xia Y. Effect observation on modified Shaofu Zhuyu decoction in treating 46 cases of dysmenorrhea of cold coagulation and blood stasis type. Jilin J Tradit Chin Med. 2013;33(9):916–917. [Google Scholar]
- 9.Zhang XX. Clinical observation on modified Shaofu Zhuyu decoction for dysmenorrhea with cold coagulation and blood stasis. J Guangxi Tradit Chin Med Univ. 2011;14(1):15–16. [Google Scholar]
- 10.Eisenberg D, Davis R, Ettner S, Appel S, Wilkey S, Van Rompay M, et al. Trends in alternative medicine use in the United States, 1990–1997: results of a follow-up national survey. JAMA. 1998;280(18):1569–1575. doi: 10.1001/jama.280.18.1569. [DOI] [PubMed] [Google Scholar]
- 11.Lloyd K, Hornsby L. Complementary and alternative medications for women’s health issues. Nutr Clin Pract. 2009;24(5):589–608. doi: 10.1177/0884533609343001. [DOI] [PubMed] [Google Scholar]
- 12.Huang X, Su S, Cui W, Liu P, Duan JA, Guo J, et al. Simultaneous determination of paeoniflorin, albiflorin, ferulic acid, tetrahydropalmatine, protopine, typhaneoside, senkyunolide I in Beagle dogs plasma by UPLC-MS/MS and its application to a pharmacokinetic study after oral administration of Shaofu Zhuyu decoction. J Chromatogr B Anal Technol Biomed Life Sci. 2014;962:75–81. doi: 10.1016/j.jchromb.2014.05.032. [DOI] [PubMed] [Google Scholar]
- 13.Su S, Duan J, Wang T, Yu L, Hua Y, Tang Y. Evaluating the effects of Shaofu Zhuyu decoction on hemorheology and ovarian function in rat model of Han-Ning blood stasis. Chin J Exp Tradit Med Form. 2008;14(12):14–34. [Google Scholar]
- 14.Sun ZH, Zhao XY. Shaofu Zhuyu decoction for treatment of 60 cases of primary dysmenorrhea. J Commun Med. 2011;9(21):51. [Google Scholar]
- 15.Chen HY, Lin YH, Su IH, Chen YC, Yang SH, Chen JL. Investigation on Chinese herbal medicine for primary dysmenorrhea: implication from a nationwide prescription database in Taiwan. Complement Ther. 2014;22(1):116–125. doi: 10.1016/j.ctim.2013.11.012. [DOI] [PubMed] [Google Scholar]
- 16.Oya A, Oikawa T, Nakai A, Takeshita T, Hanawa T. Clinical efficacy of Kampo medicine (Japanese traditional herbal medicine) in the treatment of primary dysmenorrhea. J Obstetrics Gynaecol Res. 2008;34(5):898–908. doi: 10.1111/j.1447-0756.2008.00847.x. [DOI] [PubMed] [Google Scholar]
- 17.Gunter RN. Blood stasis: China’s classical concept in modern medicine. China: Elsvier; 2007. [Google Scholar]
- 18.YK K, YM A, SY A, HK S. The experimental studies of the kaejibokyungwhan, sobokchugeotang and dohongsamultang on the medangial cell proliferation and fibronectin synthesis. Korean J Orient Int Med. 2003;24(1):94–103. [Google Scholar]
- 19.Zhuo QH, Jiang XF, Zhang YM. Clinical observation of Shaofu Zhuyu decoction treating for dysmenorrhea with adolescent functional of 126 cases. Chin J Exp Tradit Med Formulae. 2002;8(4):58–59. [Google Scholar]
- 20.Yang SJ, Jin CS. A study on the effects of sobokchukeo-tang on the isolated uterine muscle of rats. J orient Obestetrics Gynecol. 2005;18(4):72–84. [Google Scholar]
- 21.Shin WW, Choi JS, Khil JH, Kim SH. Study on antitumor activity of sobokchukeotang and kamisocokchukeotang. J Korean Orient Med. 2001;22(2):22–30. [Google Scholar]
- 22.Yum YH, Lee DN, Seo IB, Kim HJ. Effects of sobokchukeo-tang on the development of experimentally induced endometriosis in rats. J Orent Obestet Gynecol. 2006;19(2):141–161. [Google Scholar]
- 23.Yuan YH. Integrated Chinese and Western medicine treated in primary dysmenorrhea in 47 cases. Hunan J Tradit Chin Med. 2010;26(2):37–38. [Google Scholar]
- 24.Harel Z. Dysmenorrhea in adolescents and young adults: from pathophysiology to pharmacological treatments and management strategies. Expert Opin Pharmacother. 2008;9(15):2661–2672. doi: 10.1517/14656566.9.15.2661. [DOI] [PubMed] [Google Scholar]
- 25.Pirotta M. Commentary on the Cochrane Review of Chinese herbal medicine for dysmenorrhea. Explore (New York, NY) 2008;4(6):389–391. doi: 10.1016/j.explore.2008.09.006. [DOI] [PubMed] [Google Scholar]
- 26.Zhu X, Proctor M, Bensoussan A, Wu E, Smith CA. Chinese herbal medicine for primary dysmenorrhoea. The Cochrane database of systematic reviews. 2008;(2):Cd005288. [DOI] [PubMed]
- 27.Higgins JPT, Altman DG, Sterne JAC. Chapter 8: Assessing risk of bias in included studies. In: Higgins JPT, Green S, editors. Cochrane handbook for systematic reviews of interventions version 5.1.0. The Cochrane Collaboration, http://handbook.cochrane.org/; 2011.
- 28.Deeks JJ, Higgins JPT, Altman DG. Chapter 9: Analysing data and undertaking meta-analyses. In: Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration. Available from http://handbook.cochrane.org/. 2011.
- 29.Sterne JAC, Egger M, Moher D. Chapter 10: Addressing reporting biases. In: Higgins JPT, Green S, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration. Available from http://handbook.cochrane.org/; 2011.
- 30.Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. BMJ. 1997;315(7109):629–634. doi: 10.1136/bmj.315.7109.629. [DOI] [PMC free article] [PubMed] [Google Scholar]