

Abstract
Purpose
We compared the predictive and prognostic values of leukocyte differential counts, systemic inflammatory (SIR) markers and cancer antigen 125 (CA-125) levels, and identified the most useful marker in patients with ovarian clear cell carcinoma (OCCC).
Materials and Methods
The study included 109 patients with OCCC who did not have any inflammatory conditions except endometriosis, and underwent primary debulking surgery between 1997 and 2012. Leukocyte differential counts (neutrophil, lymphocyte, monocyte, eosinophil, basophil, and platelet), SIR markers including neutrophil to lymphocyte ratio (NLR), monocyte to lymphocyte ratio (MLR), and platelet to lymphocyte ratio (PLR), and CA-125 levels were estimated to select potential markers for clinical outcomes.
Results
Among potential markers (neutrophil, monocyte, platelet, NLR, MLR, PLR, and CA-125 levels) selected by stepwise comparison, CA-125 levels were best at predicting advanced stage disease, suboptimal debulking and platinum-resistance (cut-off values, ≥ 46.5, ≥ 11.45, and ≥ 66.4 U/mL; accuracies, 69.4%, 78.7%, and 68.5%) while PLR ≥ 205.4 predicted non-complete response (CR; accuracy, 71.6%) most accurately. Moreover, PLR < 205.4 was an independent factor for the reduced risk of non-CR (adjusted odds ratio, 0.17; 95% confidence interval [CI], 0.04 to 0.69), and NLR < 2.8 was a favorable factor for improved progression-free survival (PFS; adjusted hazard ratio, 0.49; 95% CI, 0.25 to 0.99) despite lack of a marker for overall survival among the potential markers.
Conclusion
CA-125 levels may be the most useful marker for predicting advanced-stage disease. Suboptimal debulking and platinum-resistance, and PLR and NLR may be most effective to predict non-CR and PFS in patients with OCCC.
Keywords: Clear cell adenocarcinoma, Ovarian neoplasms, CA-125 antigen, Neutrophils, Blood platelets, Lymphocytes
Introduction
Ovarian clear cell carcinoma (OCCC) is the fourth most common of histologic types of epithelial ovarian cancer (EOC). OCCC prognosis is similar to other histologic types in early-stage disease but it has the worst prognosis in advanced stage disease [1]. In general, about two-thirds of patients with EOC including OCCC have advanced stage disease at diagnosis because the disease is typically symptomless and there is no effective screening method [2], resulting in 5-year survival of 18.6% in patients with advanced-stage disease [1]. To monitor tumor response and confirm relapse in patients with EOC, cancer antigen 125 (CA-125) levels are a highly useful surrogate in the clinical setting [3].
However, the prognostic value of CA-125 levels is less clear in OCCC. A limited number of studies found that CA-125 levels were lower in OCCC than in other histologic types, and did not reflect clinical outcomes of patients with OCCC [4,5]. To overcome these limitations, there is a growing interest in systemic inflammatory response (SIR) markers such as leukocyte differential counts to predict clinical outcomes in patients with EOC, because various types of malignancy are associated with systemic inflammation, which may contribute to secondary hematologic abnormalities [6,7]. SIR markers, including neutrophil to lymphocyte ratio (NLR), monocyte to lymphocyte ratio (MLR), and platelet to lymphocyte ratio (PLR), may be useful to predict clinical outcomes in patients with EOC [8,9]. Nevertheless, most pertinent studies included different histologic types of EOC, while there is a lack of studies where the efficacy of SIR markers was investigated in patients with OCCC. Thus, we conducted the current study to compare the predictive and prognostic values among leukocyte differential counts, SIR markers and CA-125 levels, and thereby to identify the most useful marker in patients with OCCC.
Materials and Methods
1. Study population
We collected clinico-pathologic data from a database of EOC registered from Seoul National University Hospital and Seoul National University Bundang Hospital between February 1997 and December 2012. The Institutional Review Board at our institution approved the current study, and the informed consent requirement was waived because the current study was conducted by a retrospective medical record review.
We included only patients with OCCC who underwent primary debulking surgery. Leukocyte differential counts including neutrophil, lymphocyte, monocyte, platelet, basophil, and eosinophil, SIR markers such as NLR, MLR, and PLR, CA-125 levels were measured within one week before staging laparotomy. However, patients with any inflammatory conditions or other malignancies that could affect the results of laboratory tests were excluded, except endometriosis proved by biopsy. Clinico-pathologic data collected included age, International Federation of Gynecology and Obstetrics (FIGO) stage, endometriosis, extent of debulking surgery, regimen and cycles of adjuvant chemotherapy, leukocyte differential counts, SIR markers, CA-125 levels, tumor response, platinum-resistance, progression-free survival (PFS), and overall survival (OS).
2. Data extraction
Leukocyte differential counts were estimated 1 week prior to surgery (SYSMEX XE-2100, TOA Medical Electronics, Kobe, Japan), and CA-125 levels were measured at the same time using a radioimmunoassay kit (Fujirebio Diagnostics, Malvern, PA). Optimal debulking was defined as a residual tumor ≤ 1 cm in a maximal diameter, and complete response (CR) was defined as the disappearance of all tumor burdens for at least 4 weeks with normalization of CA-125 levels. PFS was calculated as the time elapsed from the date of completion of primary treatment to the date of clinically proven recurrence, and platinum-resistance was defined as PFS less than 6 months. OS was defined as the length of time from the date of surgery to the date of cancer-related death or the end of study.
3. Statistical analysis
We compared leukocyte differential counts, SIR markers and CA-125 levels based on clinico-pathologic characteristics using Student’s t test and Mann-Whitney U test in patients with OCCC, and selected potential markers associated with the clinico-pathologic characteristics among them. We calculated the best cut-off values of potential markers based on the receiver operating characteristic (ROC) curve, and assessed the sensitivity (SN), specificity (SP), positive predictive value (PPV), negative predictive value (NPV), and accuracy to identify the best marker for predicting clinical outcomes.
Next, we investigated the best prognostic factors among the potential markers for tumor response and survival in the patients. To this end, we performed logistic regression and Cox’s proportional hazard analyses, and calculated odds ratio (OR), hazard ratio (HR) and 95% confidence interval (CI). Statistical analyses were performed with SPSS ver. 19.0 (SPSS Inc., Chicago, IL). We rejected null hypotheses of no difference if p-values were less than 0.05, or, equivalently, if the 95% CIs of risk point estimates excluded 1.
Results
1. Patient characteristics
One hundred and nine patients with OCCC were included, and Table 1 shows their clinico-pathologic characteristics. The median age was 53 years (range, 30 to 86 years), and the median duration of follow-up was 46 months (range, 6.1 to 192.9 months). One hundred and one patients (92.6%) had pure OCCC, whereas, of those with mixed OCCC, three (2.8%) had endometrioid and serous types, three (2.8%) endometrioid type, and two (1.8%) serous type in addition to clear cell carcinoma. After primary treatment, 89 patients (81.7%) showed CR while four (3.7%) demonstrated partial response, two (1.8%) had stable disease, and 14 (12.8%) suffered disease progression.
Table 1.
Clinico-pathologic characteristics of 109 patients with ovarian clear cell carcinoma
| Characteristic | No. of patients (%) |
|---|---|
| Age (yr) | |
| < 54 | 57 (52.3) |
| ≥ 54 | 52 (47.7) |
| FIGO stage | |
| I-II | 68 (62.4) |
| III-IV | 41 (37.5) |
| Histology | |
| Pure | 101 (92.6) |
| Mixed | 8 (7.4) |
| Endometriosis | |
| No | 62 (56.9) |
| Yes | 47 (43.1) |
| Optimal debulking | |
| No | 95 (87.2) |
| Yes | 14 (12.8) |
| Regimen of chemotherapy | |
| No | 6 (5.5) |
| Non-taxane and platinum | 17 (15.6) |
| Taxane and platinum | 86 (78.9) |
| Cycles of chemotherapy | |
| ≤ 6 | 93 (85.3) |
| 6-9 | 16 (14.7) |
| Platinum-resistance | |
| No | 89 (81.7) |
| Yes | 20 (18.3) |
| Tumor response | |
| Non-CR | 20 (18.3) |
| CR | 89 (81.7) |
FIGO, International Federation of Gynecology and Obstetrics; CR, complete response.
2. Prediction
When we compared leukocyte differential counts, SIR markers and CA-125 levels based on clinico-pathologic characteristics, neutrophila, monocytosis, thrombocytosis, elevated NLR, PLR, and CA-125 levels were associated with advanced-stage disease, non-CR, and platinum-resistance. Thrombocytosis, elevated NLR, PLR, and CA-125 levels were associated with suboptimal debulking, and elevated MLR was associated with non-CR and platinum-resistance (Table 2). We calculated the best cut-off values of the potential markers selected in Table 2 by ROC curves, and assessed SN, SP, PPV, NPV, and accuracy (Fig. 1). CA-125 levels were best at predicting advanced-stage disease (≥ 46.5 U/mL), suboptimal debulking (≥ 11.45 U/mL) and platinum-resistance (≥ 66.4 U/mL), while PLR ≥ 205.4 predicted non-CR most accurately (Table 3).
Table 2.
Leukocyte differential counts, systemic inflammatory response markers, and CA-125 levels based on clinico-pathologic characteristics of 109 patients with ovarian clear cell carcinoma
| Characteristic | Leukocyte differential counts |
SIR markers |
CA-125 (U/mL) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Neutrophil (cell/μL) | Lymphocyte (cell/μL) | Monocyte (cell/μL) | Eosinophil (cell/μL) | Basophil (cell/μL) | Platelet (×103/μL) | NLR | MLR | PLR | ||
| Age (yr) | ||||||||||
| < 54 | 4,481±1,863 | 1,691±713 | 396±189 | 27±17 | 109±107 | 308±100 | 3.1+1.7 | 0.3±0.1 | 206.4±103.7 | 163.1±436.7 |
| ≥ 55 | 4,355±1,729 | 1,715±532 | 381±151 | 26±16 | 133±106 | 318±95 | 2.9±1.7 | 0.2±0.1 | 204±93 | 412.9±1,270.8 |
| FIGO stage | ||||||||||
| I-II | 4,019±1,403a) | 1,787±718 | 359±152a) | 24±16 | 130±109 | 287±75a) | 2.6±1.4a) | 0.2±0.1a) | 181.3±80.4a) | 110.8±378.2a) |
| III-IV | 5,100±2,162 | 1,561±422 | 440±193 | 27±16 | 102±104 | 355±115 | 3.5±1.9 | 0.3±0.2 | 245.7±112.8 | 565.4±1,412.8 |
| Histology | ||||||||||
| Pure | 4,473±1,820 | 1,722±642 | 386±174 | 26±17 | 115±98 | 315±99 | 3.0±1.7 | 0.2±0.1 | 204.9±98.6 | 279.7±961.8 |
| Mixed | 3,724±1,275 | 1,449±426 | 439±141 | 18±8 | 182±191 | 274±49 | 3.0±2.1 | 0.3±0.2 | 210.1±102.2 | 329.1±648.3 |
| Endometriosis | ||||||||||
| No | 4,573±1,930 | 1,685±710 | 398±184 | 24±16 | 107±103 | 316±97 | 3.2±1.8 | 0.3±0.2 | 209.2±88.6 | 411±1212 |
| Yes | 4,214±1,586 | 1,725±513 | 376±154 | 26±17 | 137±111 | 307±99 | 2.7±1.4 | 0.2±0.1 | 199.8±111.1 | 117.8±298.9 |
| Optimal debulking | ||||||||||
| Yes | 4,207±1,494 | 1,710±661 | 381±159 | 25±16 | 127±112 | 297±83a) | 2.8±1.6a) | 0.3±0.1 | 196±93a) | 166.3±439.8a) |
| No | 5,890±2,831 | 1,653±387 | 448±243 | 30±19 | 72±34 | 419±120 | 3.8±2.3 | 0.3±0.2 | 270±114 | 1,069.8±2,263.3 |
| Tumor response | ||||||||||
| Non-CR | 5,644±2,419a) | 1,502±354 | 476±221a) | 26±17 | 91±54 | 401±118a) | 3.9±1.8a) | 0.3±0.1a) | 283.7±111.3a) | 781.1±1,931.5a) |
| CR | 4,142±1,500 | 1,748±673 | 370±154 | 25±16 | 126±115 | 292±79 | 2.8±1.6 | 0.2±0.1 | 187.3±86.2 | 170.3±449.4 |
| Platinum-resistance | ||||||||||
| Yes | 5,352±1,827a) | 1,552±473 | 461±180a) | 24±16 | 124±119 | 363±114a) | 3.7±1.8a) | 0.3±0.2a) | 259.2±120.9a) | 720.7±1,925.7a) |
| No | 4,209±1,727 | 1,737±661 | 373±167 | 25±16 | 119±105 | 301±90 | 2.8±1.6 | 0.2±0.1 | 192.9±88.7 | 184±471.9 |
CA-125, cancer antigen 125; SIR, systemic inflammatory response; NLR, neutrophil to lymphocyte ratio; MLR, monocyte to lymphocyte ratio; PLR, platelet to lymphocyte ratio; FIGO, International Federation of Gynecology and Obstetrics; CR, complete response.
p < 0.05.
Fig. 1.
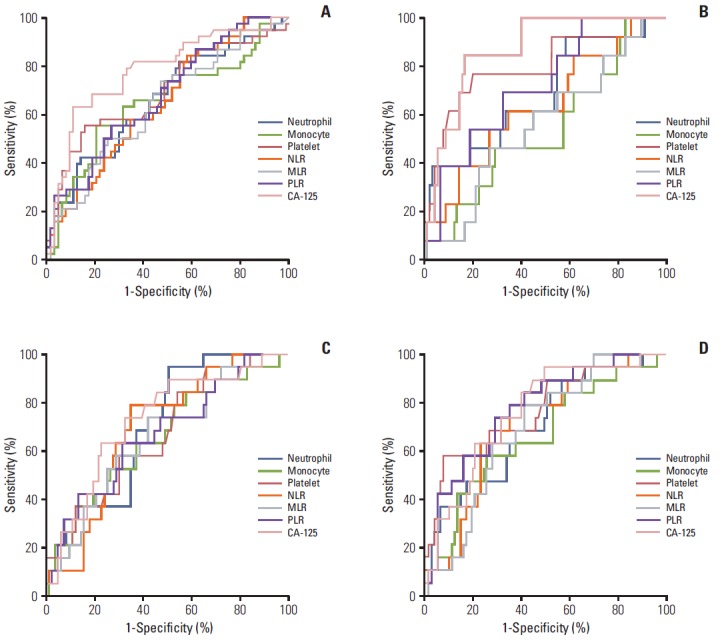
The receiver operating characteristic curves to determine the best cut-off values of leukocyte differential counts including neutrophil, monocyte and platelet, neutrophil to lymphocyte ratio (NLR), monocyte to lymphocyte ratio (MLR), platelet to lymphocyte ratio (PLR), and cancer antigen 125 (CA-125) levels for predicting International Federation of Gynecology and Obstetrics (FIGO) stage III-IV disease (A), suboptimal debulking (B), platinum-resistance (C), and non-complete response (D) in 109 patients with ovarian clear cell carcinoma.
Table 3.
SN, SP, PPV, NPV, and accuracy of leukocyte differential counts, systemic inflammatory response markers, CA-125 levels by the receiver operating characteristic curve
| Characteristic | Cut-off value | AUC | SN (%) | SP (%) | PPV (%) | NPV (%) | Accuracy (%) | p-value |
|---|---|---|---|---|---|---|---|---|
| FIGO stage III-IV disease | ||||||||
| Neutrophil (cell/μL) | ≥ 4,370 | 0.66 | 60.5 | 59.4 | 46.9 | 71.7 | 59.8 | < 0.01 |
| Monocyte (cell/μL) | ≥ 389 | 0.65 | 65.8 | 64.6 | 52.1 | 76.4 | 65 | 0.01 |
| Platelet (×103/μL) | ≥ 300 | 0.70 | 60.5 | 57.8 | 46 | 71.2 | 58.8 | < 0.01 |
| NLR | ≥ 2.4 | 0.65 | 60.5 | 56.3 | 45.1 | 70.6 | 57.8 | 0.01 |
| MLR | ≥ 0.2 | 0.64 | 60.5 | 60 | 46.9 | 72.2 | 60.2 | 0.02 |
| PLR | ≥ 178.3 | 0.68 | 60.5 | 57.8 | 46 | 71.2 | 58.8 | < 0.01 |
| CA-125 (U/mL) | ≥ 46.5 | 0.78 | 73.2 | 67.2 | 57.7 | 80.4 | 69.4 | < 0.01 |
| Suboptimal debulking | ||||||||
| Neutrophil (cell/μL) | ≥ 4,254 | 0.69 | 61.5 | 50.6 | 15.4 | 90 | 51.9 | 0.03 |
| Monocyte (cell/μL) | ≥ 354 | 0.54 | 61.5 | 43.3 | 13.6 | 88.6 | 45.6 | 0.65 |
| Platelet (×103/μL) | ≥ 295 | 0.80 | 76.9 | 51.7 | 18.9 | 93.9 | 54.9 | < 0.01 |
| NLR | ≥ 2.4 | 0.64 | 61.5 | 50.6 | 15.4 | 90 | 52 | 0.11 |
| MLR | ≥ 0.2 | 0.56 | 61.5 | 54.4 | 16.3 | 90.7 | 55.3 | 0.49 |
| PLR | ≥ 205.4 | 0.72 | 69.2 | 67.4 | 23.7 | 93.8 | 67.6 | 0.01 |
| CA-125 (U/mL) | ≥ 114.5 | 0.87 | 78.6 | 78.7 | 35.5 | 96.1 | 78.7 | < 0.01 |
| Non-CR | ||||||||
| Neutrophil (cell/μL) | ≥ 4,428 | 0.71 | 68.4 | 62.7 | 29.5 | 89.7 | 63.7 | < 0.01 |
| Monocyte (cell/μL) | ≥ 394 | 0.67 | 63.2 | 63.1 | 27.9 | 88.3 | 66 | 0.03 |
| Platelet (×103/μL) | ≥ 297 | 0.77 | 73.7 | 54.2 | 26.9 | 90 | 57.8 | < 0.01 |
| NLR | ≥ 2.7 | 0.71 | 73.7 | 65.1 | 32.6 | 91.5 | 66.7 | < 0.01 |
| MLR | ≥ 0.3 | 0.69 | 68.4 | 63.1 | 29.5 | 89.8 | 64.1 | < 0.01 |
| PLR | ≥ 205.4 | 0.78 | 73.7 | 71.1 | 36.8 | 92.2 | 71.6 | < 0.01 |
| CA-125 (U/mL) | ≥ 66.9 | 0.76 | 70 | 69.3 | 34.1 | 69.3 | 69.4 | < 0.01 |
| Platinum-resistance | ||||||||
| Neutrophil (cell/μL) | ≥ 4,436 | 0.70 | 63.2 | 62.7 | 27.9 | 88.1 | 62.7 | < 0.01 |
| Monocyte (cell/μL) | ≥ 394 | 0.65 | 63.2 | 63.1 | 27.9 | 88.3 | 63.1 | 0.04 |
| Platelet (×103/μL) | ≥ 297 | 0.67 | 63.2 | 51.8 | 23.1 | 86 | 53.9 | 0.02 |
| NLR | ≥ 2.8 | 0.69 | 68.4 | 65.1 | 31 | 90 | 65.7 | < 0.01 |
| MLR | ≥ 0.3 | 0.66 | 63.2 | 61.9 | 27.3 | 88.1 | 62.1 | 0.03 |
| PLR | ≥ 178.3 | 0.67 | 68.4 | 55.4 | 26 | 88.5 | 57.8 | 0.02 |
| CA-125 (U/mL) | ≥ 66.4 | 0.73 | 70 | 68.2 | 33.3 | 90.9 | 68.5 | < 0.01 |
SN, sensitivity; SP, specificity; PPV, positive predictive value; NPV, negative predictive value; AUC, area under curve; FIGO, International Federation of Gynecology and Obstetrics; NLR, neutrophil to lymphocyte ratio; MLR, monocyte to lymphocyte ratio; PLR, platelet to lymphocyte ratio; CA-125, cancer antigen 125.
3. Prognosis
To determine the best prognostic factors among the potential markers, we performed logistic regression analyses, which showed that optimal debulking (adjusted OR, 0.02; 95% CI, 0.01 to 0.12) and PLR < 205.4 (adjusted OR, 0.17; 95% CI, 0.04 to 0.69) were independent factors associated with the reduced risk of non-CR (Table 4). In terms of survival, early-stage disease, optimal debulking, taxane- and platinum-based chemotherapy and NLR < 2.8 were favorable factors for improved PFS (adjusted HRs, 0.18, 0.37, 0.36, and 0.49; 95% CIs, 0.08 to 0.41, 0.16 to 0.84, 0.15 to 0.89, and 0.25 to 0.99) while early-stage disease and optimal debulking were favorable factors for improved OS (adjusted HRs, 0.08 and 0.26; 95% CIs, 0.03 to 022 and 0.09 to 0.75) (Table 5).
Table 4.
Prognostic factors associated with the reduced risk of non-complete response after primary treatment in 109 patients with ovarian clear cell carcinoma
| Factor | Univariate |
Multivariate |
||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-value | Adjusted OR | 95% CI | p-value | |
| Age < 54 yr | 0.70 | 0.26-1.85 | 0.47 | - | - | - |
| FIGO stage I-II disease | 0.07 | 0.02-0.24 | < 0.01 | - | - | - |
| Pure OCCC | 0.65 | 0.12-3.49 | 0.62 | - | - | - |
| Optimal debulking | 0.02 | 0.01-0.08 | < 0.01 | 0.02 | 0.01-0.12 | < 0.001 |
| Taxane- and platinum-based chemotherapy | 0.61 | 0.16-2.29 | 0.46 | - | - | - |
| > 6 cycles of chemotherapy | 0.42 | 0.13-1.40 | 0.16 | - | - | - |
| PLR < 205.4 | 0.15 | 0.05-0.45 | < 0.01 | 0.17 | 0.04-0.69 | 0.01 |
| CA-125 < 66.9 (U/mL) | 0.19 | 0.07-0.55 | < 0.01 | - | - | - |
OR, odds ratio; CI, confidence interval; FIGO, International Federation of Gynecology and Obstetrics; OCCC, ovarian clear cell carcinoma; PLR, platelet to lymphocyte ratio; CA-125, cancer antigen 125.
Table 5.
Prognostic factors related with improved progression-free and overall survivals in 109 patients with ovarian clear cell carcinoma
| Factor | Univariate |
Multivariate |
||||
|---|---|---|---|---|---|---|
| HR | 95% CI | p-value | Adjusted HR | 95% CI | p-value | |
| Progression-free survival | ||||||
| Age < 54 yr | 1.14 | 0.60-2.17 | 0.68 | - | - | - |
| FIGO stage I-II disease | 0.15 | 0.08-0.31 | < 0.01 | 0.18 | 0.08-0.41 | < 0.01 |
| Pure OCCC | 0.56 | 0.20-1.59 | 0.28 | - | - | - |
| Optimal debulking | 0.13 | 0.06-0.27 | < 0.01 | 0.37 | 0.16-0.84 | 0.02 |
| Taxane- and platinum-based chemotherapy | 0.87 | 0.41-1.84 | 0.72 | 0.36 | 0.15-0.89 | 0.03 |
| > 6 cycles of chemotherapy | 1.79 | 0.82-3.93 | 0.14 | - | - | - |
| NLR < 2.8 | 0.34 | 0.18-0.67 | < 0.01 | 0.49 | 0.25-0.99 | 0.04 |
| CA-125 < 68.5 (U/mL) | 0.29 | 0.15-0.57 | < 0.01 | - | - | - |
| Overall survival | ||||||
| Age < 54 yr | 2.00 | 0.85-4.69 | 0.11 | - | - | - |
| FIGO stage I-II disease | 0.12 | 0.05-0.30 | < 0.01 | 0.08 | 0.03-0.22 | < 0.01 |
| Pure OCCC | 0.53 | 0.16-1.78 | 0.30 | - | - | - |
| Optimal debulking | 0.14 | 0.06-0.36 | < 0.01 | 0.26 | 0.09-0.75 | 0.01 |
| Taxane- and platinum-based chemotherapy | 0.69 | 0.29-1.65 | 0.40 | - | - | - |
| > 6 cycles of chemotherapy | 3.06 | 1.31-7.13 | 0.10 | - | - | - |
| NLR < 2.8 | 0.29 | 0.13-0.68 | < 0.01 | - | - | - |
| CA-125 < 68.5 (U/mL) | 0.26 | 0.11-0.59 | < 0.01 | - | - | - |
HR, hazard ratio; CI, confidence interval; FIGO, International Federation of Gynecology and Obstetrics; OCCC, ovarian clear cell carcinoma; NLR, neutrophil to lymphocyte ratio; CA-125, cancer antigen 125.
Discussion
SIR involves secondary changes in the levels of circulating leukocytes, which show neutrophilia, monocytosis, lymphocytopenia and thrombocytosis [10]. Thus, some leukocyte differential counts and SIR markers have been studied in relation with EOC because leukocyte-mediated inflammatory cytokines by tumor would inhibit apoptosis and promote angiogenesis, resulting in tumor growth, progression and metastasis [11]. In particular, neutrophilia, lymphocytopenia, NLR and PLR are prognostic of advance-stage disease, residual disease after surgery and survival in patients with EOC-like CA-125 levels [12-16].
In the current study, CA-125 levels were best for predicting advanced-stage disease, suboptimal debulking and platinum-resistance in patients with OCCC. Although most leukocyte differential counts and SIR markers were statistically significant for predicting advanced-stage disease, suboptimal debulking and platinum-resistance, we found that CA-125 levels had the highest SN, SP, PPV, NPV, and accuracy. Specific leukocyte differential counts (neutrophil, monocyte, and platelet), and SIR markers (NLR, MLR, and PLR) increase proportionally with a growing burden of inflammation such as cancer, whereas CA-125 levels are relatively low in early-stage OCCC in comparison with other histologic types of EOC because of the apparent initial smaller volume of disease as well as fundamental differences in the biology of malignancy [4,12,17]. However, CA-125 levels increase in advanced-stage disease because of an increase of tumor burden [18]. Thus, high levels of CA-125 can predict advanced-stage disease or suboptimal debulking more accurately compared with elevation of specific leukocyte differential counts and SIR markers. This hypothesis is supported indirectly by a study that found CA-125 levels to be a sensitive biomarker of tumor response in low-grade serous carcinoma showing a low level of CA-125 [19].
Furthermore, PLR was the most significant to predict tumor response after primary treatment among the potential markers. Platelets interact with tumor cells, and to contain factors contributing to tumor growth, invasion and angiogenesis [20]. Moreover, it can protect tumor cells from natural killer cell-mediated lysis, thereby facilitating metastasis [21]. Thus, thrombocytosis is also common in patients with EOC [13]. Since tumor cells secret thrombopoietic cytokines such as interleukin-6, thrombocytosis is related to poor response in solid tumors, combined with lymphocytopenia [22]. In the current study, we found PLR, among the potential markers, to be a better predictor of risk of non-CR in patients with OCCC, like previous studies [9,13]. However, all potential markers have modest predictive values to determine tumor response in patients with OCCC because common mechanisms lead to their coincident elevation. Thus, more focused studies are required to validate the role of PLR to predict tumor response in the patients.
Last, NLR was the most important prognostic factor for PFS despite there being no marker related to OS among the potential markers. Many studies reports that a higher neutrophil count or a lower lymphocyte predicts poorer survival in EOC [12]. Among blood components, the potential mechanism underlying the prognostic value of NLR may be an association between high NLR and inflammation. Neutrophilia produces inflammatory cytokines and chemokines by both the tumor and associated host cells such as leukocytes, and contributes to malignant progression by secreting tumor growth factors such as vascular endothelial growth factor [11]. However, neutrophilia as an inflammatory response by cancer inhibits the immune system by suppressing the cytotoxic activity of immune cells such as lymphocytes and natural killer cells [23]. NLR reflects these inflammatory changes, and therefore may be a useful marker in patients with a cancer for which reliable biomarkers are lacking [24]. A recent meta-analysis reported a similar result in that NLR was related to a higher risk of mortality than PLR in solid tumors because the broader properties of neutrophils, in comparison with platelets, may stimulate various cytokines [25]. Nevertheless, no potential markers have a significant impact on OS in the current study, which requires a new biomarker for predicting OS in the patients.
Whether the potential markers can be applied to predict clinical outcomes in patients with OCCC is controversial. Although recent meta-analyses emphasized the importance of SIR markers to predict prognosis of solid tumors, research that interprets their usefulness in EOC when compared with other malignancies is lacking [24,25]. Furthermore, OCCC cases in most studies comprise a small proportion, 5%-8%, among patients with EOC, making it difficult to evaluate prognostic values of the potential markers in patients with OCCC [4,19].
Conclusion
Although the current study has some limitations such as a retrospective design and unassessed possible confounders affecting SIR (e.g., smoking or oral contraceptive use) [12], we included a large number of patients with OCCC, and sought to identify the most dominant markers related to clinical outcomes by stepwise comparison of prognostic values among the potential markers. Conclusively, CA-125 levels may be the most useful marker for predicting advanced-stage disease, suboptimal debulking and platinum-resistance, and PLR and NLR may be the most effective to predict non-CR and PFS in patients with OCCC.
Acknowledgments
This research was supported by grants (No. 04-2012-0890; 03-2012-0170) from the Seoul National University Hospital research fund, and the Priority Research Centers Program (No. 2009-0093820), Basic Science Research Program (No. 2011-0025394), and BK21 plus program (No. 5256-20140100) through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology. Moreover, it was also supported by a grant of the Korean Health Technology R&D Project, Ministry of Health of Welfare (HI14C2404).
Footnotes
Conflict of interest relevant to this article was not reported.
References
- 1.Suh DH, Kim JW, Kang S, Kim HJ, Lee KH. Major clinical research advances in gynecologic cancer in 2013. J Gynecol Oncol. 2014;25:236–48. doi: 10.3802/jgo.2014.25.3.236. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kim JH, MacLaughlin DT, Donahoe PK. Mullerian inhibiting substance/anti-Mullerian hormone: A novel treatment for gynecologic tumors. Obstet Gynecol Sci. 2014;57:343–57. doi: 10.5468/ogs.2014.57.5.343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Rustin GJ, Vergote I, Eisenhauer E, Pujade-Lauraine E, Quinn M, Thigpen T, et al. Definitions for response and progression in ovarian cancer clinical trials incorporating RECIST 1.1 and CA 125 agreed by the Gynecological Cancer Intergroup (GCIG) Int J Gynecol Cancer. 2011;21:419–23. doi: 10.1097/IGC.0b013e3182070f17. [DOI] [PubMed] [Google Scholar]
- 4.Tian C, Markman M, Zaino R, Ozols RF, McGuire WP, Muggia FM, et al. CA-125 change after chemotherapy in prediction of treatment outcome among advanced mucinous and clear cell epithelial ovarian cancers: a Gynecologic Oncology Group study. Cancer. 2009;115:1395–403. doi: 10.1002/cncr.24152. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Eltabbakh GH, Mount SL, Beatty B, Simmons-Arnold L, Cooper K. Clinical and molecular differences between clear cell and papillary serous ovarian carcinoma. J Surg Oncol. 2006;93:379–86. doi: 10.1002/jso.20494. [DOI] [PubMed] [Google Scholar]
- 6.Shan W, Yang G, Liu J. The inflammatory network: bridging senescent stroma and epithelial tumorigenesis. Front Biosci (Landmark Ed) 2009;14:4044–57. doi: 10.2741/3511. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.den Ouden M, Ubachs JM, Stoot JE, van Wersch JW. Whole blood cell counts and leucocyte differentials in patients with benign or malignant ovarian tumours. Eur J Obstet Gynecol Reprod Biol. 1997;72:73–7. doi: 10.1016/s0301-2115(96)02662-0. [DOI] [PubMed] [Google Scholar]
- 8.Kim SI, Kim HS, Kim TH, Suh DH, Kim K, No JH, et al. Impact of underweight after treatment on prognosis of advanced-stage ovarian cancer. J Immunol Res. 2014;2014:349546. doi: 10.1155/2014/349546. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Asher V, Lee J, Innamaa A, Bali A. Preoperative platelet lymphocyte ratio as an independent prognostic marker in ovarian cancer. Clin Transl Oncol. 2011;13:499–503. doi: 10.1007/s12094-011-0687-9. [DOI] [PubMed] [Google Scholar]
- 10.Jilma B, Blann A, Pernerstorfer T, Stohlawetz P, Eichler HG, Vondrovec B, et al. Regulation of adhesion molecules during human endotoxemia. No acute effects of aspirin. Am J Respir Crit Care Med. 1999;159:857–63. doi: 10.1164/ajrccm.159.3.9805087. [DOI] [PubMed] [Google Scholar]
- 11.Balkwill F, Mantovani A. Inflammation and cancer: back to Virchow? Lancet. 2001;357:539–45. doi: 10.1016/S0140-6736(00)04046-0. [DOI] [PubMed] [Google Scholar]
- 12.Williams KA, Labidi-Galy SI, Terry KL, Vitonis AF, Welch WR, Goodman A, et al. Prognostic significance and predictors of the neutrophil-to-lymphocyte ratio in ovarian cancer. Gynecol Oncol. 2014;132:542–50. doi: 10.1016/j.ygyno.2014.01.026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Raungkaewmanee S, Tangjitgamol S, Manusirivithaya S, Srijaipracharoen S, Thavaramara T. Platelet to lymphocyte ratio as a prognostic factor for epithelial ovarian cancer. J Gynecol Oncol. 2012;23:265–73. doi: 10.3802/jgo.2012.23.4.265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cho H, Hur HW, Kim SW, Kim SH, Kim JH, Kim YT, et al. Pre-treatment neutrophil to lymphocyte ratio is elevated in epithelial ovarian cancer and predicts survival after treatment. Cancer Immunol Immunother. 2009;58:15–23. doi: 10.1007/s00262-008-0516-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Milne K, Alexander C, Webb JR, Sun W, Dillon K, Kalloger SE, et al. Absolute lymphocyte count is associated with survival in ovarian cancer independent of tumor-infiltrating lymphocytes. J Transl Med. 2012;10:33. doi: 10.1186/1479-5876-10-33. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bishara S, Griffin M, Cargill A, Bali A, Gore ME, Kaye SB, et al. Pre-treatment white blood cell subtypes as prognostic indicators in ovarian cancer. Eur J Obstet Gynecol Reprod Biol. 2008;138:71–5. doi: 10.1016/j.ejogrb.2007.05.012. [DOI] [PubMed] [Google Scholar]
- 17.Ho CM, Chien TY, Shih BY, Huang SH. Evaluation of complete surgical staging with pelvic and para-aortic lymphadenectomy and paclitaxel plus carboplatin chemotherapy for improvement of survival in stage I ovarian clear cell carcinoma. Gynecol Oncol. 2003;88:394–9. doi: 10.1016/s0090-8258(02)00156-7. [DOI] [PubMed] [Google Scholar]
- 18.Behbakht K, Randall TC, Benjamin I, Morgan MA, King S, Rubin SC. Clinical characteristics of clear cell carcinoma of the ovary. Gynecol Oncol. 1998;70:255–8. doi: 10.1006/gyno.1998.5071. [DOI] [PubMed] [Google Scholar]
- 19.Fader AN, Java J, Krivak TC, Bristow RE, Tergas AI, Bookman MA, et al. The prognostic significance of pre- and post-treatment CA-125 in grade 1 serous ovarian carcinoma: a gynecologic Oncology Group study. Gynecol Oncol. 2014;132:560–5. doi: 10.1016/j.ygyno.2013.11.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Jain S, Harris J, Ware J. Platelets: linking hemostasis and cancer. Arterioscler Thromb Vasc Biol. 2010;30:2362–7. doi: 10.1161/ATVBAHA.110.207514. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Nieswandt B, Hafner M, Echtenacher B, Mannel DN. Lysis of tumor cells by natural killer cells in mice is impeded by platelets. Cancer Res. 1999;59:1295–300. [PubMed] [Google Scholar]
- 22.Buergy D, Wenz F, Groden C, Brockmann MA. Tumor-platelet interaction in solid tumors. Int J Cancer. 2012;130:2747–60. doi: 10.1002/ijc.27441. [DOI] [PubMed] [Google Scholar]
- 23.Gooden MJ, de Bock GH, Leffers N, Daemen T, Nijman HW. The prognostic influence of tumour-infiltrating lymphocytes in cancer: a systematic review with meta-analysis. Br J Cancer. 2011;105:93–103. doi: 10.1038/bjc.2011.189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Templeton AJ, McNamara MG, Seruga B, Vera-Badillo FE, Aneja P, Ocana A, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014;106: doi: 10.1093/jnci/dju124. [DOI] [PubMed] [Google Scholar]
- 25.Templeton AJ, Ace O, McNamara MG, Al-Mubarak M, Vera-Badillo FE, Hermanns T, et al. Prognostic role of platelet to lymphocyte ratio in solid tumors: a systematic review and meta-analysis. Cancer Epidemiol Biomarkers Prev. 2014;23:1204–12. doi: 10.1158/1055-9965.EPI-14-0146. [DOI] [PubMed] [Google Scholar]