

Abstract
Background
The Global Roadmap for Health Measurement and Accountability sees integrated systems for health information as key to obtaining seamless, sustainable, and secure information exchanges at all levels of health systems. The Global Strategy for Women’s, Children’s and Adolescent’s Health aims to achieve a continuum of quality of care with effective coverage of interventions. The WHO and World Bank recommend that countries focus on intervention coverage to monitor programs and progress for universal health coverage. Electronic health registries - eRegistries - represent integrated systems that secure a triple return on investments: First, effective single data collection for health workers to seamlessly follow individuals along the continuum of care and across disconnected cadres of care providers. Second, real-time public health surveillance and monitoring of intervention coverage, and third, feedback of information to individuals, care providers and the public for transparent accountability. This series on eRegistries presents frameworks and tools to facilitate the development and secure operation of eRegistries for maternal and child health.
Methods
In this first paper of the eRegistries Series we have used WHO frameworks and taxonomy to map how eRegistries can support commonly used electronic and mobile applications to alleviate health systems constraints in maternal and child health. A web-based survey of public health officials in 64 low- and middle-income countries, and a systematic search of literature from 2005–2015, aimed to assess country capacities by the current status, quality and use of data in reproductive health registries.
Results
eRegistries can offer support for the 12 most commonly used electronic and mobile applications for health. Countries are implementing health registries in various forms, the majority in transition from paper-based data collection to electronic systems, but very few have eRegistries that can act as an integrating backbone for health information. More mature country capacity reflected by published health registry based research is emerging in settings reaching regional or national scale, increasingly with electronic solutions. 66 scientific publications were identified based on 32 registry systems in 23 countries over a period of 10 years; this reflects a challenging experience and capacity gap for delivering sustainable high quality registries.
Conclusions
Registries are being developed and used in many high burden countries, but their potential benefits are far from realized as few countries have fully transitioned from paper-based health information to integrated electronic backbone systems. Free tools and frameworks exist to facilitate progress in health information for women and children.
Electronic supplementary material
The online version of this article (doi:10.1186/s12884-016-0801-7) contains supplementary material, which is available to authorized users.
Keywords: Health systems, eRegistries, Women’s, Children’s and Adolescent’s Health, health surveillance, eHealth, mHealth
Background
Electronic health (eHealth) solutions, including mobile health technologies (mHealth), have the potential to improve quality of healthcare by addressing technical shortcomings embedded in health systems (Frame 1). Many eHealth initiatives in low and middle income countries (LMIC) have been fragmented [1, 2]. Now, global health agencies are moving towards more sustainable and holistic approaches for institutionalizing e- and mHealth into healthcare systems [1, 3–5].
Frame 1.
The new World Bank/WHO/USAID Roadmap for Health Measurement and Accountability Post-2015 (MA4Health) underlined that “Public health and clinical care cannot be delivered safely, with high quality, and in a cost-effective manner, without seamless, sustainable, and secure data and information exchanges at all levels of the health system” [5]. An effective healthcare system must therefore entail a seamless common or interoperable digital thread for health information so that the full range of uses can be driven by, or contribute to, an integrated backbone system [4, 5]. In line with this, MA4Health has outlined the importance of having all health information system (HIS) development initiatives aligned with a single operational country platform for data and indicators by 2020.
With the new United Nation’s Global Strategy for Women’s, Children’s and Adolescent’s Health (UN Global Strategy) [6], the global community for mothers’ and children’s health is converging on post-2015 policies for integrated care for the health and survival of the mother and her baby alike. This brings together multiple recent initiatives such as Strategies toward Ending Preventable Maternal Mortality [7] and the Every Newborn Action Plan [8], representing an integrated continuum of community and facility health promotion and care from family planning, thru periconception, pregnancy, childbirth and postpartum, to the newborn and child. The potential of health systems focusing on the continuum of care cannot come to fruition without integrated eHealth solutions [9]. When any isolated silo keeps its information separate, potential synergies within the system are being squandered. eHealth is the most frequently mentioned emerging opportunity for maternal health among international researchers [10].
Better data on health status and quality of healthcare are crucial to address bottlenecks in achieving universal health coverage (UHC) and producing better policies for health. Traditional measures of points of contact, such as attending antenatal care or having a skilled birth attendant, are far from sufficient measures of having received quality care [11, 12]. Pertaining to this, the WHO and the World Bank accentuate that in monitoring UHC, the coverage of health interventions should be at the center of countries’ attention [13–15].
In the maternal and child health context, primary data on coverage of interventions is typically created when a woman is booked for antenatal care, and data on her health and the services she receives is subsequently added, retrieved and reported from her personal file over a continuum of community and facility services. But without eHealth in many settings, paper registers and patient folders make no timely and actionable data available for program management and policy development, and subsequent extraction of data from paper files results in poor quality data and underutilized health information [16–19]. Information on the individual woman meant to allow personalized care throughout pregnancy and childbirth is often neither easily accessed at follow up visits, nor shared between levels of care, or shared with women themselves to improve self-care. When information is shared, it is often not under robust governance to secure privacy and safety (Myhre et al: eRegistries: Governance for maternal and child health registries, submitted). Most public health data collection strategies are inefficient reporting chores, where care providers are viewed only as data collectors, and women only as data points. Not harvesting the data created and registered at the point-of-care, LMIC spend scarce resources on expensive data collection either by duplicate data entry from paper files, or undertaking household surveys to collect information from the population, with little and biased information of moderate validity on coverage of health interventions [20, 21, Flenady et al: eRegistries: Indicators for the WHO Essential Interventions for reproductive, maternal, newborn, and child health, submitted].
The UN Global Strategy has not formulated a specific eHealth component to support its activities [6], but such eHealth solutions will have to provide seamless and secure information following individuals across health system levels to serve the uniquely longitudinal focus on continuity and quality of care. It will also need to enable regional and national monitoring of coverage of health interventions delivered at the point-of-care. The «integrated backbone systems» [4, 5] that can deliver on both, are electronic health registries – eRegistries (Frame 1). Unlike health information system architectures that manage only aggregate data or clinical health records with unstructured text or forms, eRegistries are based on systematic and uniform data on pre-defined health outcomes and determinants, including care provision. This represents a database that can drive multiple e- and mHealth applications for health systems, individual care providers, and the individual clients and patients.
This eRegistries initiative, led by the Norwegian Institute of Public Health and the WHO Department of Reproductive Health and Research (RHR), with Queensland University, the University of Oxford, and the Health Information Systems Program Vietnam, aimed to develop a common framework of evidence, guidance and technical tools to facilitate the development and country implementation of eRegistries for reproductive, maternal, newborn and child health (RMNCH) in LMIC. eRegistries only have value if they can alleviate health system constraints hampering UHC. In this first paper of the eRegistries Series, we use the WHO frameworks and taxonomy for mHealth and health systems constraints in RMNCH to review what eRegistries, acting as the backbone HIS, can and should contribute to facilitate achievement of UHC of high quality care. We report on a systematic review of scientific literature from registries for RMNCH in LMIC, and on a survey of country readiness to develop eRegistries for RMNCH.
In the second paper (Flenady et al, submitted), we review the current availability of data and indicator gaps for monitoring and evaluation of coverage of the WHO Essential Interventions, Commodities and Guidelines for RMNCH [22]. We present the process and results in the harmonization and development of a suite of process (or coverage) and outcome indicators for use in eRegistries.
In the third paper (Myhre et al, submitted), we report the current status of ethical and legal issues pertaining to eRegistries in LMIC. Given the highly sensitive nature of RMNCH data, we assess existing privacy legislation, access, and data security practices and report on the development of a governance toolkit that outlines best practices for responsible data stewardship.
In the fourth and last paper (Frost et al: eRegistries: Architecture and free open source software for maternal and child health registries, submitted), we draw on the first three papers’ findings of identified needs, to report on the formulation of minimum criteria for free and open source software for eRegistries as the integrating backbone for HIS in RMNCH. We review potential systems and their functionalities, and report on the eRegistries application - a customizable point-of-care registry using WHO Essential Interventions care algorithms developed in DHIS2, the most commonly nationally deployed free and open source software health management information system [23].
Methods
Framework for eHealth in RMNCH
The WHO RHR, the Johns Hopkins University Global mHealth Initiative, the United Nations Children’s Fund, and frog Design jointly developed the “mHealth and ICT [Information and Communication Technologies] Framework” to describe commonly used mHealth applications in RMNCH [24], and subsequently used for systematic review of evidence [25]. We used this framework and the taxonomy for primary health systems constraint categories developed by the WHO mHealth Technical and Evidence Review Group (mTERG) for RMNCH [26] to identify applications to alleviate common health systems constraints that can be supported by an eRegistry (Fig. 1).
Fig. 1.
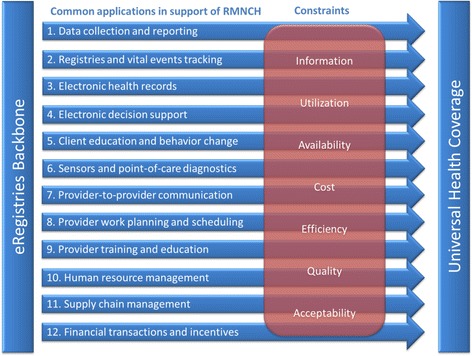
Framework for eRegistries in support of UHC in RMNCH. eRegistries in support of the 12 common electronic and mobile applications to overcome the seven principal constraints for universal health coverage in RMNCH, adapted from [24, 26]
Survey of public health officials
Health officials working in any of the 75 LMIC monitored by the Commission on Information and Accountability for Women’s and Children’s Health, and Palestine, were recruited by emails to RMNCH medical and health organizations, ministries of health, public health institutes, and other relevant government offices (e.g., statistics bureaus, RMNCH departments, etc.). The survey was reviewed and provided with a Letter of Exemption by the Regional Committees for Medical and Health Research Ethics in Norway, confirming that the anonymous survey was not medical research on human subjects, and did not need ethical approval (Reference number: IRB 0000 1870). Launched in November 2013, responses were accepted until February 2015. The sample consisted of 298 individuals from 64 countries. Approximately two-thirds of respondents worked at the national or regional level. The survey included questions on national registry infrastructure, reporting and dissemination practices, and data quality. Issues such as privacy legislation, access by individuals and professionals, and data security are presented in the third paper, as well as additional details on the survey methodology (Myhre et al, submitted).
Country-level values are presented for all results. Decision rules for combining multiple responses into a single country response were adapted for each question; country averages were calculated for continuous data. Generalized linear models (PROC GLIMMIX) were used for confidence intervals around continuous data, while exact confidence intervals were calculated around binary and categorical data using SAS 9.4.
Systematic search of literature
A systematic search of literature was conducted including papers from 2005–March 2015 using Medline, Embase, ISI Web of Science, Cochrane Library and Global Health. The searches used terms indicative of RMNCH registries and were limited to the 76 LMIC as above (Additional file 1). After de-duplication, 4237 articles were identified. We included studies based on longitudinal data collection systems for individual level RMNCH data, and excluded all alternative data collections such as cross sectional surveys and health record document reviews. Two investigators independently scored publications for inclusion and extracted data. We included the following data points (within the categories in parentheses): the country/-ies of operation, the extent of the registry data collection (in facilities only, in community services only, both, or not defined), the scale of the implementation of the registry (national, district, local, or not defined), the specified population captured by the registry data collection (a total population, only subgroups/select population, or not defined), the data collection method used (paper, electronic, both, or not defined), whether the primary data was collected and entered directly into the registry, or if the registry was based on a secondary/duplicate data collection from existing sources (direct, duplicated, or not defined). In cases of conflicting scores/data, consensus was reached after independent scoring by a third investigator. Full text was read for 302 publications with abstracts considered potentially relevant (Additional file 1).
Results and discussion
The systematic and uniform data in eRegistries allows eHealth functionalities that give registries the potential to go far beyond simple registration tools [9, 27], and constitute an entire ecosystem of public health information and communication strategies (Frame 1). We mapped the potential uses of eRegistries in RMNCH onto two mHealth frameworks (Fig. 1): First, a set of 12 applications commonly used in RMNCH reflecting domains of work with empirical evidence of pervasive utility [24], and second, seven primary constraints to UHC for health systems (Frame 2) [26]:
Frame 2.
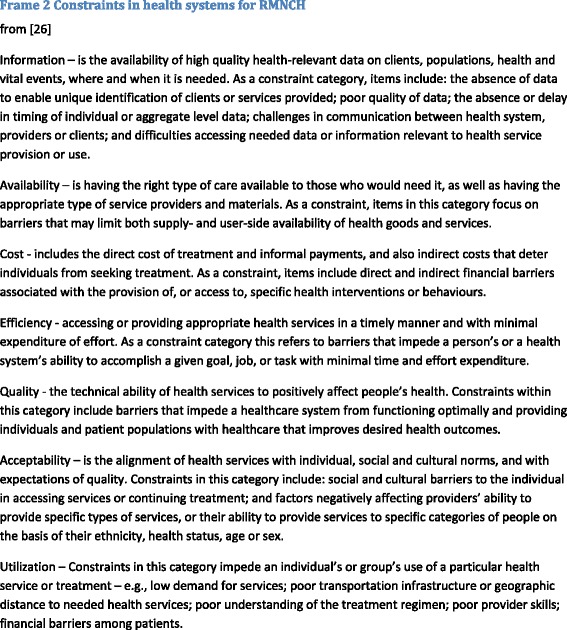
Constraints in health systems for RMNCH
Commonly used mHealth applications within RMNCH
Data collection and reporting
Electronic HIS are in widespread use in LMIC to lessen health systems’ information constraints (Frame 2). Primary data creation in RMNCH occurs at the point-of-care, where frontline health workers document their clients’ health, services provided, and any specific data required for reporting to managers or national health statistics. A well-designed electronic application for systematic data collection and management will correspond intimately to the health workers’ needs in care provision [28, 29]. It can, at the same time, upload all or selected data items to create a registry for use in the care system. Additional electronically derived geographic information systems [30], and linkage of individuals to households [31, 32], can add to outreach utility and potentially link data to non-health data sources. Integrated with the national HIS, it allows managers to safely monitor and assess programs (Frost et al, submitted). This eliminates duplicate data entry for reporting which often consumes large proportion of provider’s time in LMIC [28, 33], easing constraints of health systems’ costs, availability and efficiency (Frame 2).
In registries in LMIC, real-time health surveillance tools are used for rapid quality improvement cycles [31]. LMIC registries contribute to independent prospective monitoring of trials and interventions [34–36], and large data collections are exploited to study rare conditions [35, 37, 38] and drug exposure [35, 36], or conversely, register rare conditions only [37, 39, 40]. Registries in LMIC follow mothers to study recurrence of pregnancy outcomes [41, 42], link mothers with offspring [29, 43–45] with their subsequent newborn health records [46], and link children with siblings [47–49]; in some cases registries study long-term and family-based health determinants and recurrence [41, 42] or undertaking twin studies [48, 49].
The ease of electronic feedback of data to providers is associated with improved quality of data [16]. eRegistry forms improve data quality with functionalities such as logical checks and limitations, warning prompts for improbable or missing data entries [29, 50, Frost et al, submitted], or pre-defined algorithms to improve correct categorizations, e.g. for causes of death [31]. Prospective and longitudinal data collection in eRegistries can reduce reporting bias on intervention coverage. For example, an adverse outcome can bias any retrospective registration of health determinants and care provision, i.e. what risks and health conditions she experienced in pregnancy and what was done to identify and manage them. This bias can make real-life estimations of effect of intervention coverage unhelpful.
Registries and vital events tracking
Recognizing the critical position of civil registration and vital statistics (CRVS) data in alleviating information constraints (Frame 2), the poor quality and coverage in LMIC, and the modest progress over the last 30 years, universal coverage of CRVS systems is a key goal for the post-2015 agenda [4, 51–53]. Well-functioning CRVS are independently associated with improved health, in particular lower child mortality [54]. Electronic and mobile applications are in widespread use for CRVS in LMIC. In settings with high proportions of home deliveries, mobile phones can extend the infrastructure by engaging frontline health workers to register births in communities [55, 56].
Being born is an essential health determinant, and dying likewise an essential outcome. CRVS systems thus share many characteristics and data with eRegistries for RMNCH that track individuals with unique identifiers (i.e. personal identification numbers (PIN)), or if lacking, issue such identifiers for care provision [57, 58]. Both in sentinel sites and total populations, several LMIC have created seamless integration of CRVS and HIS to benefit both enumeration of the population and support care provision, health monitoring, identify service delivery gaps and inequities, and improve accountability [38, 59]. Lack of such information can add to constraints of cost, acceptability and utilization of services by restricting eligibility (Frame 2).
The voluntary registration of all pregnancies can improve accountability and quality of vital events tracking related to RMNCH in LMIC [27, 60]. As pregnancy and date of birth are key in defining maternal mortality, eRegistries of pregnancies and births can facilitate correct classification when integrated with a CRVS registering deaths of women in fertile age. Stillbirths and neonatal deaths are poorly registered in many settings with a high percentage of home deliveries, stigma, and a lack of incentives to register a dead baby, for either care professionals, or for parents. The magnitude of the issue can be unmasked by counting third trimester pregnancies registered in eRegistries with no subsequent report of a live infant, civil registration, vaccination or other incentivizing benefits that can be integrated or linked to the registry.
Electronic health records
As stated in MA4Health, quality, cost and efficiency constraints cannot be overcome without patient data being shared across sites and levels of care (Frame 2) [5]. RMNCH has a long tradition of using simplified client-held paper records of systematic and uniform data for communication along the continuity of care and to facilitate self-care [61]. This tradition makes RMNCH particularly fitting for the use of eRegistries where systematic and uniform data are the key to functionality, including the ability to manage data items such as unstructured text notes and narratives as in health records. Conversely, electronic health records built on an architecture of unstructured text and forms as data items can not support the functionalities of an eRegistry. In LMIC, the traditional maternity, child health and vaccination cards are valued, and while loss of records by women is not typically reported as a major problem, the communication flow can be broken as they are often not brought to care visits, and confidentiality has been questioned [61]. The value of information following the woman is evident in societies with traditions wherein women travel to their parental home to deliver. In such settings, single facility based or local electronic systems can not only be expensive and hard to maintain [62], but represents an inferior tool for information management – although some projects have provided women with printed versions [32] or uploaded records to a server for women themselves to have electronic access [58].
Even in settings of less mobility in care seeking, a backbone registry accessible across its regional or national jurisdiction supports continuity of health records at all levels of care, with secure governance and storage preventing irreversible loss or damage to facility or client-held paper records. An electronic version adds to patient safety by also making information available in emergencies when a paper card may be unavailable. Mobile units enable entries and access to health records from community and outreach activities. In LMIC, research based on registries often extract their data from electronic health records (Additional file 1). Some also link individuals’ records to biobanks and lab tests [49].
Electronic decision support
Best practice guidelines are well-established in RMNCH, and achieving effective coverage of interventions, i.e. high quality of care, is key in the post-2015 agenda [63–65]. Guidelines may appear straightforward, but are seldom followed in the correct and complete sequence. This know-do gap constrains quality of care services (Frame 2) [66, 67]. A commonly cited hindering factor is unavailability of guidelines in a user-friendly, readily accessible manner at the point-of-care [68, 69].
Checklists are informational job aids extracting vital elements of guidelines for clinical care to simplify the presentation and highlight actions required. They are in common use to reduce variation in performance and assist in improving quality of care in LMIC [69–71]. Corresponding intimately to the systematic and uniform approach to data in eRegistries, data entry at the point-of-care in eRegistries can be designed as interactive checklists, which integrate decision support for diagnosis, treatment and referral algorithms (Frame 1) [32, 69, Frost et al, submitted].
Integrated decision support and reminders for guideline adherence in preventive care are shown to strengthen health systems and link HIS to improved quality coverage of care [72–75]. Such tools are generally associated with high user satisfaction, but require training for use, and developing comprehensive tools for all essential interventions and guidelines in RMNCH requires substantial preparations to ensure that they reflect the actual work flow of providers [69, 76, 77, Frost et al, submitted]. However, most studies exploring these effects have been conducted in facility settings, and better evidence is needed to enhance community based RMNCH care in LMIC [78–80].
Client education and behavior change communication
Feeding back the registered information to individuals contributes by informing the public about the objectives and values of registration, as the UN recommends for CRVS. But the underutilization of data to empower women and communities has largely been overlooked. The use of registry data for community and client education and behavior change communication, has the potential to impact utilization and acceptability constraints, as well as empower women to demand improvements in health system quality, accessibility, cost and efficiency (Frame 2).
Women are principal stakeholders for their own information, and communicating it back to them should be personalized, timely and actionable. General pregnancy information can be of variable interest to the individual woman if not tailored to her needs, and mHealth solutions to communicate with her may not help much unless personalized [77]. Therefore, efforts have been made in LMIC to register women and children to deliver pregnancy stage and age appropriate messaging [81–83]. mHealth solutions building on eRegistries can communicate to her mobile phone or web-applications with personalized and culturally sensitive information according to the data registered about her. eRegistries can automate provision of information directly to women, or as a prompt to her care provider to send the information, to complement in-person approaches and assist in bridging communication barriers with multi-language support for messaging. For example, gestational age data can ensure timely advice for birth preparation, while risk or complication data can tailor information for high risk pregnancies, services or treatment data can prompt reminders of medications or appointments, and vaccination data and residential address can be used to inform of available outreach vaccination services. Such information on the importance and availability of services can empower the demand for services and improve health care utilization and acceptability (Frame 2). One of the most established applications of mHealth in LMIC is messaging of reminders for appointments and treatments, to improve care utilization and efficiency [80].
Crucially, reliance on mobile phone access for communication frequently raises questions about equity [25]. Not having access to a mobile phone is a significant marker of risk for poor outcomes that should be registered, and alternative communication methods should be provided [84].
Sensors and point-of-care diagnostics
The restriction of diagnostics to fixed site laboratories adds constraints of availability, cost, acceptability and utilization (Frame 2). Miniaturized point-of-care diagnostic tests and sensors combined with the computing, storage and communication power of mobile phones and tablets have led to a rapidly expanding range of mHealth innovations for diagnostic tests in communities [85]. Standard tests in RMNCH from blood and urine, and external sensors for fetal Doppler and blood pressure exist in low-cost mobile units for LMIC settings. The results of such tests is key information both for RMNCH care provision and health surveillance, and should be integrated in the backbone HIS. An example of such successful integration in LMIC is the implementation of Swasthya Slate, linking a small independent diagnostic unit to a tablet used by frontline community health workers to upload individual results to a cloud-based eRegistry available to care professionals, clients, and program managers [58].
Provider-to-provider communication
Insufficient communication at hand-offs and referrals significantly constrains quality and efficiency (Frame 2). An integrating backbone HIS for seamless information-sharing across multiple providers and levels of care is a key element in MA4Health’s global roadmap. Where disconnected cadres of providers interact with the same client, duplicating care, information and reporting efforts, shared health records implicitly constitute a key type of provider-to-provider communication. Within functioning health systems, shared information can cut delays and time spent in hand-offs and referrals to other providers—whether simplifying a traditional referral, or in the simplest form reduced to an automated transfer from one provider’s electronic work schedule to another’s. Mobile solutions can extend the reach of real-time information sharing e.g. of results from laboratories to frontline health workers.
Paper records are not only logistically difficult to share, but are reputed for illegibility and incompleteness [28]. From a client-held antenatal care paper record, it can be difficult to identify the care providers managing a woman, hampering their ability to communicate. For providers to be accredited as users in eRegistries, a unique user identification is created, and every entry of information logged to the individual provider (Frost et al, submitted). Their contact information can be available to others engaged in providing services to the client, and to the clients themselves, facilitating communication and identifying unwarranted “shopping” of services across providers.
Provider work planning and scheduling
Shortage of care providers in LMIC severely constrains availability, quality and efficiency of RMNCH services (Frame 2). Resources are wasted not only by underutilizing the time-saving benefits of electronic applications discussed here, but also by inefficiencies such as clients missing scheduled appointments or unneeded variation in daily work-load [80]. Likewise, systems become inefficient in providing adequate care when they are unaware of the time and location at which clients will require care. Optimizing the efficiency of the work force has therefore been a key element in many deployments of e- and mHealth programs in LMIC, including functionalities ranging from simple electronic scheduling, or household visit support with geographic information systems, to integration of messaging services to create mobile phone reminders about upcoming antenatal care visits, missed scheduled appointments, new deliveries and newborns eligible for postpartum and newborn care [31, 32, 86].
Provider training and education
Poorly performing providers cause quality, cost, efficiency, utilization and acceptability constraints (Frame 2). Interactive mHealth solutions are used for continued medical education and training support in LMIC—mostly in generic forms applied to a cadre of health workers. A standard course may not be professionally motivating for providers at different levels of performance. eRegistries create inherent accountability with data on the client population, care performance and outcomes, which facilitate individually targeted training, including the potential for automated audit and feedback [69, 87].
The variability in the approaches and results of audit and feedback interventions, including those specifically using registry data, might be explained by limited consensus and use of theories underlying multiple causal pathways [88–93]. Reviews in the framework of Feedback Intervention Theory have identified that verbal, discouraging, praising or self-esteem-affecting feedback attenuates beneficial effects on performance, while task-oriented computerized feedback augments it [94, 95]. Frequent, swift, and correct solution feedback, including a goal setting action plan, also augment effects. Effects are stronger for familiar memory tasks and weaker for following rules and completing complex tasks [94, 95]. The Model of Actionable Feedback further proposes that in order to be actionable, feedback must be timely, individualized, non-punitive and meaningful [96, 97]. These findings fit well with systematic reviews of feedback to healthcare providers that also identified larger effects if it was delivered to non-physicians by a supervisor or trustworthy colleague, in a domain where the recipient was underperforming [91, 92].
There is evident potential of eRegistries to deliver computerized, individualized, trustworthy, non-punitively neutral, timely, frequent and task-oriented feedback to health workers to focus attention to the largest quality gaps. However, stronger evidence is needed. Few studies have evaluated the effect of feedback on improving RMNCH, and studies from LMIC are lacking [91, 92, 98].
Human resource management
Closely linked to applications for work planning and scheduling, as well as those improving working conditions and satisfaction, better human resource management is needed to meet workforce constraints. Population-based data on health, health determinants and effective coverage of services is necessary for better and more targeted distribution of health workers. This is a critical issue in many LMIC settings where extremely low provider to client ratios remain a long-term problem. Monitoring and management of public health providers in LMIC is made more complex by prevalent dual practice—individual professionals providing services both privately and in the public health system—which in poorly regulated settings can add constraints to accessibility, cost, efficiency, quality, as well as equity (Frame 2) [99]. Information on actual performance of the workforce is therefore needed. As providers accessing individual patient data have unique user identities, eRegistries also represent provider registries, where their service provision is logged. Just as client data can be aggregated or disaggregated from national to individual level, so can provider data, joined with client data to support allocation of human resources needed to deliver services based on the number of beneficiaries [32]. Supportive supervision can enable program managers to identify lower quality of services than expected given the resources invested, and the real-time registration of services provided, can contribute in addressing absenteeism and enabling substitution when critical services are not provided.
Supply chain management
mHealth applications in Logistics Management Information Systems (LMIS) are widespread in LMIC to improve data visibility, enhance decision making, and address availability and cost constraints of health systems (Frame 2) [100]. Paper LMIS have low reporting rates in LMIC, due to e.g. unreliable postal systems, poor transport infrastructure, and a heavy workload among store managers. Electronic and mobile LMIS address these constraints, improving reporting rates, data visibility, and use [101].
eRegistries contain key data to combine with LMIS for improved quantification, forecasting and distribution of health commodities, including dispensed-to-users data, provider and client needs and preferences, and seasonality. The rich patient data available from eRegistries can also improve prediction of future needs, using better-quality information about population risk and demographics. Integration of HIS and LMIS is rarely seen [32], typically operating as isolated silos, but is recommended by the UN Commission on Life-Saving Commodities for Women and Children [102]. Combining eRegistry and LMIS data can provide another tool for transparency and accountability, comparing numbers of commodities issued from storage with those dispensed to users to identify potential theft/leakage.
Financial transactions and incentives
The use of mobile payments in LMIC bring financial services within reach of previously unbanked populations. Throughout LMIC, 60 % now have coverage of mobile financial services, and sub-Saharan Africa is leading other regions in the number of deployments [103]. This can assist in alleviating accessibility, acceptability and utilization constraints (Frame 2), and eRegistries in RMNCH can facilitate the use of such transactions and incentives. This includes making information available at point-of-care on eligibility for universal health insurance schemes, data on service delivery for performance based incentives, on registered conditions eligible for financial support such as transportation for institutional delivery, or incentives for child vaccination.
Country capacity for electronic health registries in RMNCH
While the potential of eRegistries are clear, the perceived needs and capacities in LMIC to deploy them are not. Unique identifier systems issuing PINs are a requirement for any population registry, enabling detection and elimination of duplicate records, or fraudulent identities. It also enables linkages through integrated backbone systems for multiple data entries and uses as in eRegistries.
According to the public health officials surveyed, 60 % (95 % confidence interval: 47–72) of LMIC issue PINs for both permanent and temporary residents while 17 % (9–29) of countries issue them to permanent residents only. A small percent (3 % (0–11)) indicated that the system was in an initial stage and one sixth indicated that they did not issue PINs; three percent did not know. Eight out of ten LMIC indicating that they do not issue PINs were located in the African region. In the vast majority of countries with PINs, the use was reported to be proof of citizenship (94 % (84–99)), or needed for access to education (57 % (42–71)), health services (51 % (36–65)), financial services (53 % (38–67)), and for taxation (45 % (31–60)). Few offer automatic registration at birth. Barriers to birth registration indicate that home delivery, cultural mores, societal taboos, and religious traditions all contribute to low registration practices at birth [104]. Adult applications are the most common method for acquiring a PIN. Half of countries offer only one option to obtain a PIN whereas 51 % (37–65) offer multiple options (Table 1).
Table 1.
Unique identity systems’ administrative oversight and acquisition
| Agency in charge | Frequency | Percenta |
|---|---|---|
| Ministry of Health | 7 | 14 % (6–26) |
| All other Ministry offices | 41 | 80 % (67–90) |
| National office/agencies | 34 | 67 % (52–79) |
| Local level offices/agencies | 13 | 25 % (14–40) |
| Acquisition | ||
| Application required at birth | 27 | 53 % (38–67) |
| Automatically issued at birth | 11 | 22 % (11–35) |
| Application required as an adultb | 30 | 59 % (44–72) |
| Automatically issued as an adultb | 6 | 12 % (4–24) |
| Other | 8 | 16 % (7–29) |
aPercent column does not add up to 100 % as the question asked respondents to check all that apply
bAdult was considered 16 years or older. 95 % confidence intervals in parentheses
The latest 2013 UNICEF report on birth registration, based on informants from household surveys with data on average from 2010, reported that about four in ten children under five were registered in CRVS in LMIC. A higher proportion of countries report in our survey that they do at least register births. Nearly half of countries report coverage greater than 90 % for registering birth, pregnancy and child health, but many regions still experience very low coverage, and a recorded birth does not translate to formal birth registration to acquire a PIN. Closer integration with birth registration in health systems may facilitate the registration process [104]. Cause of death registries are of notoriously poor coverage and quality in many regions (Table 2) [105].
Table 2.
Coverage of vital and health statistics in national registries
| Registry (Countries) | >90 % coverage | 50–89 % coverage | <50 % coverage | I don’t know | No national registry |
|---|---|---|---|---|---|
| Birth (N = 62) | 55 % (42–68) | 27 % (17–40) | 10 % (4–20) | 6 % (2–16) | 2 % (0–9) |
| Cause of death (N = 61) | 38 % (26–51) | 21 % (12–34) | 20 % (11–32) | 16 % (8–28) | 5 % (1–14) |
| Pregnancy (N = 61) | 43 % (30–56) | 34 % (23–48) | 11 % (5–22) | 10 % (4–20) | 2 % (0–9) |
| Child (N = 62) | 45 % (32–58) | 26 % (16–39) | 15 % (7–26) | 11 % (5–22) | 3 % (0–11) |
95 % confidence intervals in parentheses
Overall, the responding public health officials in LMIC rate the quality of their national health data quite modestly on a scale from 5 (excellent) to 1 (poor): A quarter of countries have health data scored as poor by their officials in terms of timeliness and security, one fifth as poor on completeness and update status, and across all domains of data quality (accuracy, completeness, integrity, access, security, timeliness, update status and utilization) average scores range from 2.3 to 2.5 ((95 % confidence interval: 2.1–2.6). Nonetheless, on a range from 5 (very influential) to 1 (not influential at all), public health officials generally score the influence of national data reports on public health decision-making highly. Data had the highest influence on planning public health programs and monitoring of the Millennium Development Goals (average score 4.3 (4.1–4.4)), somewhat less on monitoring, evaluation and improvement of health programs (3.9–4.1 (3.6–4.3)), and the least influence on budget allocations (3.4 (3.2–3.6)) and research (3.7 (3.4–3.9)). For other use of data for feedback to the health system, respondents generally score the quality as low as the quality of the data (same scale): The highest quality of feedback for effective coverage of antenatal care (2.7 (2.5–2.9)), and the lowest for quality of care in facilities (2.3 (2.1–2.5)).
Most LMICs are in a phase of transition from paper to mixed paper and electronic formats, and only a low percentage report using fully electronic registries (Table 3). With the tardiness of paper registrations, approximately half the countries have mortality figures updated annually, while one in five report a time lag from data collection to publicly available reports of more than three years on average. Data on intervention coverage in antenatal, delivery, postpartum and newborn care collected by health professionals fare similarly with two of three countries reporting having this publicly available within one year of data collection.
Table 3.
Data transmission format from health facilities to central data collection for registries
| Registry (Countries) | Electronic | Paper & Electronic | Paper | No national registry | I don’t know |
|---|---|---|---|---|---|
| Birth (N = 62) | 5 % (1–14) | 69 % (56–80) | 18 % (9–30) | 3 % (0–11) | 5 % (1–14) |
| Cause of death (N = 59) | 3 % (0–12) | 61 % (47–73) | 19 % (10–31) | 7 % (2–16) | 10 % (4–21) |
| Pregnancy (N = 61) | 3 % (0–11) | 61 % (47–73) | 25 % (15–37) | 5 % (1–14) | 7 % (2–16) |
| Child (N = 61) | 3 % (0–11) | 66 % (52–77) | 18 % (9–30) | 7 % (2–16) | 7 % (2–16) |
95 % confidence intervals in parentheses
Scientific capacity for electronic health registries in RMNCH
Capacity to operate eRegistries of high scientific quality in LMIC should be expected to be an important constraint given the slow emergence of such registries and the current status of data. From 2005 to 2015, we identified 66 publications from 32 health registries in 24 LMIC—from a broad search in LMIC literature in the field of RMNCH resulting in 4237 abstracts screened and 302 papers read in full. The registries identified are presented in Table 4.
Table 4.
RMNCH Registries with scientific publications
| Countries | Registry scope | Registry scale | Population | Data collection format | Data entry source | Health focusa | Registry name and operationb |
|---|---|---|---|---|---|---|---|
| Brazil | Community | National | Total | E & Paper | Duplicate | A + CRVS | Brazilian National Birth Registry (SINASC) - N |
| Peru | Facility | National | Total | Electronic | Primary | B + CRVS | Online Registration of Certificates of Live Births - N |
| China | Facility | National | Sample | E & Paper | Duplicate | B + Birth defects | Birth Defects Monitoring Network - I |
| Egypt | Community | National | Total | E & Paper | Duplicate | A + IVF | Egyptian IVF registry - N |
| Peru | Community | National | N/A | Electronic | Primary | ABC | Peruvian Perinatal Information System (SIP) -I |
| Ghana | Both C & F | Regional | Total | E & Paper | Duplicate | ABCD | Navrongo Health and Demographic Surveillance System-NI |
| Kenya | Community | Regional | Total | Electronic | Primary | ABD | KEMRI Centers for Disease Control & Prevention-NI |
| Yemen | Community | Regional | Total | Electronic | Duplicate | C + Cancer | Aden Cancer Registry- N |
| Kenya | Community | Regional | Total | E & Paper | Duplicate | ABD + Vaccines | Kilifi Health and Demographic Surveillance System -NI |
| Uganda | Community | Regional | Total | E & Paper | Duplicate | A + HDR | Health and Demographic Surveillance Site (HDSS) -NI |
| Guinea-Bissau | Facility | Regional | Total | E & Paper | Duplicate | AC + Twins, Vacc. | Bandim Health Project (BHP) - NI |
| Guinea-Bissau | Facility | Regional | Total | E & Paper | Duplicate | AC + Twins, Vacc. | Guinea-Bissau Twin Registry-NI |
| China | Community | Regional | Sample | Electronic | Primary | C + Vaccines | Zhejiang Immunization Information System (ZJIIS) - N |
| Bangladesh | Community | Regional | Sample | Paper | Duplicate | AB | A registry for the JiVitA 1 project - NI |
| Zambia | Facility | Regional | Sample | Electronic | Primary | AB | Zambia Electronic Perinatal Record System NI |
| Burkina Faso, Ghana, Tanzania | Facility | Regional | Sample | Electronic | Primary | AB | Quality of Prenatal & Maternal Care Clinical Decision Support (QUALMAT) - NI |
| Tanzania | Facility | Regional | Sample | Paper | Duplicate | ABC | KCMC Medical Birth Registry - NI |
| Chile | Facility | Regional | Sample | Electronic | Duplicate | A + ART | Latin American Registry (RLA) of assisted reprod. tech. - NI |
| Senegal | Community | Regional | Sample | E & Paper | Duplicate | ABD | Millennium Villages Project information system- NI |
| Indonesia | Community | Local | Total | E & Paper | Duplicate | ABC + Malaria | Sistem Informasi Kesehatan Daerah (SIKDA)- NI |
| China | Community | Local | Total | E & Paper | Duplicate | ABC | Gongcheng Maternal, Newborn and Child Health Information System - NI |
| Bangladesh | Both C & F | Local | Sample | E & Paper | Duplicate | A | Projahnmo-II Project - Pregnancy Registration - NI |
| Kenya, Pakist., Guatem., Zambia, India, Argent. | Both C & F | Local | Sample | E & Paper | Duplicate | ABC | Global Network Maternal and Newborn Health Registry - NI |
| Nigeria | Facility | Local | Sample | E & Paper | Duplicate | AC + Vaccines | OpenMRS for the Family Health Unit - NI |
| Kenya | Facility | Local | Sample | E & Paper | Duplicate | AB + HIV | Academic Model Providing Access to Healthcare (AMPATH)- NI |
| Cameroon | Facility | Local | Sample | E & Paper | Duplicate | AB | Obstetric health information system -NI |
| Nepal | Facility | Local | Sample | E & Paper | Primary | A + CVD | Prospective single-centre registry - NI |
| Brazil, Ghana, Kenya, Uganda, Tanzania | Community | Local | Total | E & Paper | Duplicate | A + Drug expo. | WHO Pregnancy Registry of drug exposures using OpenClinica - NI |
| Brazil | Facility | Local | Total | E & Paper | Primary | B + Vaccines | Quality-Health Card/Electronic Immunisation Registry-N |
| India | Facility | Local | Sample | E & Paper | Duplicate | ABC + Epilepsy | Indian Registry of Epilepsy and Pregnancy (IREP) -N |
a A Pregnancy, B Childbirth, C Infant/child, D Deaths
b N Operated nationally, I Operated by international organizations, NI Operated in collaboration between national and international organizations. N/A Not available information in publications. References in Additional file 1
The majority of health registries in RMNCH that have reached the mature stage of authoring scientific publications, operate at a scaled regional or national level, and they have come further in the transition from paper to electronic data capture than the national registration systems reported from national levels in the survey. Countries such as Kenya, Zambia, Burkina Faso, Ghana and Tanzania have all published research based on primary data entry in fully electronic registries at national or regional levels. While data collection format and the source of primary data is often poorly described in publications, it appears that in most countries, undertaking research in registry methodology still represents duplicate data collection efforts to transfer data from paper forms to an electronic database.
Conclusions
We find that purposefully designed eRegistries, acting as an integrating backbone HIS, can be the operative infrastructure for several commonly deployed applications to strengthen RMNCH, and offer crucial data and support for all. Collectively, they have the potential to alleviate the principal constraints of health systems for UHC in RMNCH. Yet, although many examples exist of successful implementation of individual applications based on registry functionalities, none have integrated more than a few within one single backbone system. While electronic solutions with registry functionalities are widely used in LMIC for data collection, reporting, CRVS, health records and clinical decision support, planning and scheduling, and inherently for communication of health information between providers, they appear underutilized for client behavior change communication, provider audit and feedback, and management of human resources, supply chains and financial incentives.
Almost all countries are investing resources into systems to support registration of births and vital events in RMNCH, and the majority are currently in transition from paper to a future of electronic HIS where eRegistries could become an integrating backbone and contribute to relieve the constraints they experience in data collection, management, analysis and dissemination. Public health officials in LMICs convey a strong message of the importance their national RMNCH-related data for country policies and program management, despite the many times mediocre coverage and quality, and long delays and suboptimal quality of feedback of data to the health system. The MA4Health post-2015 roadmap and action plan should further galvanize national investment and commitments to support the transition to electronic solutions [4, 106].
There is accumulating experience on operating health registries in LMIC to draw lessons from, and eRegistries are emerging at regional and national scale. While the finding for infrastructure capacities is encouraging for future emergence of eRegistries in RMNCH, the scientific activity is limited.
Capacity building and support for eRegistries is crucial to achieve the goals set for the post-2015 agenda reflected in the MA4Health roadmap. In this series, we offer tools and frameworks to achieve that end, including key considerations in the selection of data items and indicators, architectural standards and interoperability, and ethics and governance.
Acknowledgements
We thank Ameha Wudie Dammena, Elin Wyller, and staff members of Statistics Norway and the Norwegian Institute of Public Health for their technical support and advice, colleagues participating in consultation workshops in Thailand and Vietnam for their guidance, and survey respondents for their time and efforts.
The views expressed in this article do not necessarily represent the decisions, policy, or views of the authors’ affiliations.
Funding
The Norwegian Agency for Development Cooperation (Norad) funded the harmonized Reproductive Health Registries project (GLO-4279 QZA 12/0355 harmonized Reproductive Health Registries) that led to the eRegistries Initiative (QZA-14/0022 Every Mother and Child Counts). This was led in partnership by the Norwegian Institute of Public Health and the WHO Department for Reproductive Health and Research, with Queensland University (Australia), the University of Oxford (UK), and the Health Information Systems Program (Vietnam).
The contribution by JFF, JVJ and VN was supported in part by the Centre for Intervention Science in Maternal and Child Health (CISMAC; project number 223269), which is funded by the Research Council of Norway through its Centers of Excellence scheme and the University of Bergen, Norway.
Abbreviations
- CRVS
civil registration and vital statistics
- eHealth
(See Frame 1)
- eRegistries
(See Frame 1)
- HIS
Health information systems
- LMIC
Low- and middle-income countries
- LMIS
Logistics management information systems
- MA4Health
World Bank/WHO/USAID measurement and accountability for results in health: a common agenda for the post 2015 era
- mHealth
Mobile eHealth (See Frame 1)
- PIN
Personal identification numbers
- RMNCH
Reproductive, maternal, newborn and child health
- UHC
Universal health coverage
- UN Global Strategy
United Nations: Survive, Thrive, Transform. The Global Strategy for Women’s, Children’s and Adolescents’ Health
- WHO
World Health Organization
Additional file
Systematic review methodology supplementing information. (DOCX 141 kb)
Footnotes
Competing interests
The authors have no conflicts of interest to declare.
Authors’ contributions
JFF conceptualized and led the eRegistries initiative and drafting of the manuscript. SLM led the survey and drafted the report with IKF, JVJ and JFF. LN, HS and SLM undertook the systematic review and drafted the report with JFF. KM and MV reviewed literature and drafted reports on audit and feedback, and checklists and decision support, respectively. All authors contributed to the content of the paper, read, and approved the final version.
Contributor Information
J. Frederik Frøen, Email: frederik.froen@fhi.no.
Sonja L. Myhre, Email: sonja.myhre@fhi.no
Michael J. Frost, Email: michaeljames.frost@fhi.no
Doris Chou, Email: choud@who.int.
Garrett Mehl, Email: mehlg@who.int.
Lale Say, Email: sayl@who.int.
Socheat Cheng, Email: chengsocheat@gmail.com.
Ingvild Fjeldheim, Email: ingvild.fjeldheim@fhi.no.
Ingrid K. Friberg, Email: ingrid.friberg@fhi.no
Steve French, Email: steve.french@fhi.no.
Jagrati V. Jani, Email: jagrati.jani-bolstad@fhi.no
Jane Kaye, Email: jane.kaye@law.ox.ac.uk.
John Lewis, Email: johnlewis.hisp@gmail.com.
Ane Lunde, Email: ane.lunde@fhi.no.
Kjersti Mørkrid, Email: kjersti.morkrid@fhi.no.
Victoria Nankabirwa, Email: nankabirwav@gmail.com.
Linda Nyanchoka, Email: linda.nyanchoka@fhi.no.
Hollie Stone, Email: holliestone88@gmail.com.
Mahima Venkateswaran, Email: mahima.venkateswaran@fhi.no.
Aleena M. Wojcieszek, Email: aleena.wojcieszek@mater.uq.edu.au
Marleen Temmerman, Email: temmermanm@who.int.
Vicki J. Flenady, Email: vicki.flenady@mater.uq.edu.au
References
- 1.Wilson K, Gertz B, Arenth B, Salisbury N. The journey to scale: moving together past digital health pilots. Seattle: PATH; 2014. [Google Scholar]
- 2.WHO . Accountability for women’s and children’s health: report on progress to May 2014. Geneva: World Health Organization; 2014. [Google Scholar]
- 3.Principles for digital development [http://digitalprinciples.org]. Accessed 15 Sept 2015.
- 4.World Bank, USAID and WHO . The Roadmap for Health Measurement and Accountability. Washington, DC: MA4Health; 2015. [Google Scholar]
- 5.Haazen DS, Slote (USAID/Global Health) Al-Shorbaji N, D’Adamo M. eHealth Technical Paper for MA4Health - Measurement and Accountability for Results in Health: A Common Agenda for the Post 2015 Era. Washington, DC: MA4Health; 2015. [Google Scholar]
- 6.United Nations . Survive, Thrive, Transform. The Global Strategy for Women’s, Children’s and Adolescents’ Health. New York: United Nations; 2015. [Google Scholar]
- 7.WHO . Strategies toward ending preventable maternal mortality (EPMM) Geneva: World Health Organization; 2015. [Google Scholar]
- 8.WHO and UNICEF . Every Newborn: an action plan to end preventable deaths. Geneva: World Health Organization; 2014. [Google Scholar]
- 9.Mehl G, Labrique A. Prioritizing integrated mHealth strategies for universal health coverage. Science. 2014;345(6202):1284–1287. doi: 10.1126/science.1258926. [DOI] [PubMed] [Google Scholar]
- 10.Kendall T. Critical maternal health knowledge gaps in low- and middle-income countries for post-2015: Researchers’ perspectives. Boston, MA: Harvard T.H. Chan School of Public Health; 2015. [Google Scholar]
- 11.Marchant T, Tilley-Gyado RD, Tessema T, Singh K, Gautham M, Umar N, et al. Adding content to contacts: measurement of high quality contacts for maternal and newborn health in Ethiopia, North East Nigeria, and Uttar Pradesh, India. PLoS One. 2015;10(5):e0126840. doi: 10.1371/journal.pone.0126840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Hodgins S, D'Agostino A. The quality–coverage gap in antenatal care: toward better measurement of effective coverage. Glob Health Sci Pract. 2014;2(2):173–181. doi: 10.9745/GHSP-D-13-00176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.World Health Organization and World Bank Group . Monitoring progress towards universal health coverage at country and global levels. Framework, measures and targets. Geneva: World Health Organization; 2014. [Google Scholar]
- 14.Boerma T, AbouZahr C, Evans D, Evans T. Monitoring intervention coverage in the context of universal health coverage. PLoS Med. 2014;11(9):e1001728. doi: 10.1371/journal.pmed.1001728. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Boerma T, Eozenou P, Evans D, Evans T, Kieny MP, Wagstaff A. Monitoring progress towards universal health coverage at country and global levels. PLoS Med. 2014;11(9):e1001731. doi: 10.1371/journal.pmed.1001731. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ndabarora E, Chipps JA, Uys L. Systematic review of health data quality management and best practices at community and district levels in LMIC. Inform Dev. 2014;30(2):103–120. doi: 10.1177/0266666913477430. [DOI] [Google Scholar]
- 17.Lium JT, Tjora A, Faxvaag A. No paper, but the same routines: a qualitative exploration of experiences in two Norwegian hospitals deprived of the paper based medical record. BMC Med Inform Decis Mak. 2008;8:2. doi: 10.1186/1472-6947-8-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Corrao S, Arcoraci V, Arnone S, Calvo L, Scaglione R, Di Bernardo C, et al. Evidence-Based Knowledge Management: an approach to effectively promote good health-care decision-making in the Information Era. Intern Emerg Med. 2009;4(2):99–106. doi: 10.1007/s11739-008-0185-4. [DOI] [PubMed] [Google Scholar]
- 19.George A. ‘By papers and pens, you can only do so much’: views about accountability and human resource management from Indian government health administrators and workers. Int J Health Plann Manage. 2009;24(3):205–224. doi: 10.1002/hpm.986. [DOI] [PubMed] [Google Scholar]
- 20.Mbondji PE, Kebede D, Soumbey-Alley EW, Zielinski C, Kouvividila W, Lusamba-Dikassa P-S. Health information systems in Africa: descriptive analysis of data sources, information products and health statistics. J R Soc Med. 2014;107(1 suppl):34–45. doi: 10.1177/0141076814531750. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Liu L, Li M, Yang L, Ju L, Tan B, Walker N, et al. Measuring coverage in MNCH: a validation study linking population survey derived coverage to maternal, newborn, and child health care records in rural China. PLoS One. 2013;8(5):e60762. doi: 10.1371/journal.pone.0060762. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.WHO . Essential Interventions, Commodities and Guidelines for Reproductive, Maternal, Newborn and Child Health. Geneva: World Health Organization; 2012. [Google Scholar]
- 23.Health Information Systems Programme (HISP). DHIS 2 [https://www.dhis2.org/]. Accessed 15 Sept 2015.
- 24.Labrique AB, Vasudevan L, Kochi E, Fabricant R, Mehl G. mHealth innovations as health system strengthening tools: 12 common applications and a visual framework. Glob Health Sci Pract. 2013;1(2):160–171. doi: 10.9745/GHSP-D-13-00031. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Hall CS, Fottrell E, Wilkinson S, Byass P. Assessing the impact of mHealth interventions in low- and middle-income countries – what has been shown to work? Global Health Action. 2014;7:25606. doi: 10.3402/gha.v7.25606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Mehl G, Vasudevan L, Gonsalves L, Berg M, Seimon T, Temmerman M, et al. Harnessing mHealth in low-resource settings to overcome health system constraints and achieve universal access to healthcare. In: Marsch LA, Lord SE, Dallery J, et al., editors. Behavioral Healthcare and Technology Using Science-Based Innovations to Transform Practice. Oxford, UK: Oxford University Press; 2014. [Google Scholar]
- 27.Labrique AB, Pereira S, Christian P, Murthy N, Bartlett L, Mehl G. Pregnancy registration systems can enhance health systems, increase accountability and reduce mortality. Reprod Health Matters. 2012;20(39):113–117. doi: 10.1016/S0968-8080(12)39631-6. [DOI] [PubMed] [Google Scholar]
- 28.Thompson A, Castle E, Lubeck P, Makarfi PS. Experience implementing OpenMRS to support maternal and reproductive health in Northern Nigeria. Stud Health Technol Inform. 2010;160(PART 1):332–336. [PubMed] [Google Scholar]
- 29.Chi BH, Vwalika B, Killam WP, Wamalume C, Giganti MJ, Mbewe R, et al. Implementation of the Zambia Electronic Perinatal Record System for comprehensive prenatal and delivery care. Int J Gynecol Obstet. 2011;113(2):131–136. doi: 10.1016/j.ijgo.2010.11.013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Ebener S, Guerra-Arias M, Campbell J, Tatem AJ, Moran AC, Amoako Johnson F, et al. The geography of maternal and newborn health: the state of the art. Int J Health Geogr. 2015;14:19. doi: 10.1186/s12942-015-0012-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Moshabela M, Sene M, Nanne I, Tankoano Y, Schaefer J, Niang O, et al. Early detection of maternal deaths in Senegal through household-based death notification integrating verbal and social autopsy: a community-level case study. BMC Health Serv Res. 2015;15:9. doi: 10.1186/s12913-014-0664-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Siika AM, Rotich JK, Simiyu CJ, Kigotho EM, Smith FE, Sidle JE, et al. An electronic medical record system for ambulatory care of HIV-infected patients in Kenya. Int J Med Inform. 2005;74(5):345–355. doi: 10.1016/j.ijmedinf.2005.03.002. [DOI] [PubMed] [Google Scholar]
- 33.Ngana FR, Myers BA, Belton S. Health reporting system in two subdistricts in Eastern Indonesia: Highlighting the role of village midwives. Midwifery. 2012;28(6):809–815. doi: 10.1016/j.midw.2011.09.005. [DOI] [PubMed] [Google Scholar]
- 34.Bang A, Bellad R, Gisore P, Hibberd P, Patel A, Goudar S, et al. Implementation and evaluation of the Helping Babies Breathe curriculum in three resource limited settings: does Helping Babies Breathe save lives? A study protocol. BMC Pregnancy Childbirth. 2014;14:116. doi: 10.1186/1471-2393-14-116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Odhiambo FO, Laserson KF, Sewe M, Hamel MJ, Feikin DR, Adazu K, et al. Profile: The KEMRI/CDC health and demographic surveillance system-Western Kenya. Int J Epidemiol. 2012;41(4):977–987. doi: 10.1093/ije/dys108. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Mehta U, Clerk C, Allen E, Yore M, Sevene E, Singlovic J, et al. Protocol for a drugs exposure pregnancy registry for implementation in resource-limited settings. BMC Pregnancy Childbirth. 2012;12:89. doi: 10.1186/1471-2393-12-89. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Ba-Saddik IA. Childhood cancer in Aden, Yemen. Cancer Epidemiol. 2013;37(6):803–806. doi: 10.1016/j.canep.2013.10.001. [DOI] [PubMed] [Google Scholar]
- 38.Nhoncanse GC, Melo DG. Reliability of birth certificates as a source of information on congenital defects in the City of Sao Carlos, Sao Paulo, Brazil. Cien Saude Colet. 2012;17(4):955–963. doi: 10.1590/s1413-81232012000400017. [DOI] [PubMed] [Google Scholar]
- 39.Li X, Zhu J, Wang Y, Mu D, Dai L, Zhou G, et al. Geographic and urban-rural disparities in the total prevalence of neural tube defects and their subtypes during 2006-2008 in China: a study using the hospital-based birth defects surveillance system. BMC Public Health. 2013;13:161. doi: 10.1186/1471-2458-13-161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Chhetri S, Shrestha NR, Pilgrim T. Pregnancy complicated by heart disease in Nepal. Heart Asia. 2014;6(1):26–29. doi: 10.1136/heartasia-2013-010396. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Mahande MJ, Daltveit AK, Mmbaga BT, Obure J, Masenga G, Manongi R, et al. Recurrence of perinatal death in Northern Tanzania: a registry based cohort study. BMC Pregnancy Childbirth. 2013;13:166. doi: 10.1186/1471-2393-13-166. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42.Mahande MJ, Daltveit AK, Obure J, Mmbaga BT, Masenga G, Manongi R, et al. Recurrence of preterm birth and perinatal mortality in northern Tanzania: registry-based cohort study. Trop Med Int Health. 2013;18(8):962–967. doi: 10.1111/tmi.12111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Welaga P, Moyer CA, Aborigo R, Adongo P, Williams J, Hodgson A, et al. Why are babies dying in the first month after birth? A 7-year study of neonatal mortality in northern Ghana. PLoS One. 2013;8(3):e58924. doi: 10.1371/journal.pone.0058924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44.Bergsjo P, Mlay J, Lie RT, Lie-Nielsen E, Shao JF. A medical birth registry at Kilimanjaro Christian Medical Centre. East Afr J Public Health. 2007;4(1):1–4. [PubMed] [Google Scholar]
- 45.Abu Habib N, Wilcox AJ, Daltveit AK, Basso O, Shao J, Oneko O, et al. Birthweight, preterm birth and perinatal mortality: a comparison of black babies in Tanzania and the USA. Acta Obstet Gynecol Scand. 2011;90(10):1100–1106. doi: 10.1111/j.1600-0412.2011.01195.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Mmbaga BT, Lie RT, Olomi R, Mahande MJ, Kvale G, Daltveit AK. Cause-specific neonatal mortality in a neonatal care unit in Northern Tanzania: a registry based cohort study. BMC Pediatr. 2012;12:116. doi: 10.1186/1471-2431-12-116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Chiwanga ES, Massenga G, Mlay P, Obure J, Mahande MJ. Maternal outcome in multiple versus singleton pregnancies in Northern Tanzania: a registry-based case control study. Asian Pac J Reprod. 2014;3(1):46–52. doi: 10.1016/S2305-0500(14)60001-4. [DOI] [Google Scholar]
- 48.Bjerregaard-Andersen M, Biering-Sorensen S, Gomes GM, Bidonga A, Jensen DM, Rodrigues A, et al. Infant twin mortality and hospitalisations after the perinatal period - a prospective cohort study from Guinea-Bissau. Trop Med Int Health. 2014;19(12):1477–1487. doi: 10.1111/tmi.12388. [DOI] [PubMed] [Google Scholar]
- 49.Bjerregaard-Andersen M, Gomes MA, Joaquim LC, Rodrigues A, Jensen DM, Christensen K, et al. Establishing a twin registry in Guinea-Bissau. Twin Res Hum Genet. 2013;16(1):179–184. doi: 10.1017/thg.2012.90. [DOI] [PubMed] [Google Scholar]
- 50.Haskew J, Ro G, Saito K, Turner K, Odhiambo G, Wamae A, et al. Implementation of a cloud-based electronic medical record for maternal and child health in rural Kenya. Int J Med Inform. 2015;84(5):349–354. doi: 10.1016/j.ijmedinf.2015.01.005. [DOI] [PubMed] [Google Scholar]
- 51.Okoko L: Mapping HIS software platforms in West Africa - Real Time Data For Ebola Response. In USAID Google Docs. Retrieved 15 Sept 2015 from https://docs.google.com/spreadsheets/d/1CUA2aiSC4D-Q6ePN1RBm848Ux9KTi=Tadr8GKV5le8/edit?pli=1#gid=45737138.
- 52.AbouZahr C, de Savigny D, Mikkelsen L, Setel PW, Lozano R, Lopez AD. Towards universal civil registration and vital statistics systems: the time is now. Lancet. 2015;386(10001):1407–18. doi: 10.1016/S0140-6736(15)60170-2. [DOI] [PubMed] [Google Scholar]
- 53.Mikkelsen L, Phillips DE, AbouZahr C, Setel PW, de Savigny D, Lozano R, et al. A global assessment of civil registration and vital statistics systems: monitoring data quality and progress. Lancet. 2015;386(10001):1395–406. doi: 10.1016/S0140-6736(15)60171-4. [DOI] [PubMed] [Google Scholar]
- 54.Phillips DE, AbouZahr C, Lopez AD, Mikkelsen L, de Savigny D, Lozano R, et al. Are well functioning civil registration and vital statistics systems associated with better health outcomes? Lancet. 2015;386(10001):1386–94. doi: 10.1016/S0140-6736(15)60172-6. [DOI] [PubMed] [Google Scholar]
- 55.Kabadi GS, Mwanyika H, de Savigny D. Innovations in monitoring vital events: a scalable intervention using mobile phone messaging (SMS) support for vital registration coverage. Lancet. 2013;381:S69. doi: 10.1016/S0140-6736(13)61323-9. [DOI] [Google Scholar]
- 56.Oomman N, Mehl G, Berg M, Silverman R. Modernising vital registration systems: why now? Lancet. 2013;381(9875):1336–1337. doi: 10.1016/S0140-6736(13)60847-8. [DOI] [PubMed] [Google Scholar]
- 57.Li Q, Hu Y, Zhong YP, Chen YP, Tang XW, Guo J, et al. Using the immunization information system to determine vaccination coverage rates among children aged 1-7 years: a report from Zhejiang Province, China. Int J Environ Res Public Health. 2014;11(3):2713–2728. doi: 10.3390/ijerph110302713. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Swasthya Slate [http://www.swasthyaslate.org/]. Accessed 15 Sept 2015.
- 59.Curioso WH, Pardo K, Loayza M. Transforming the Peruvian birth information system. Rev Peru Med Exp Salud Publica. 2013;30(2):303–307. [PubMed] [Google Scholar]
- 60.Goudar SS, Carlo WA, McClure EM, Pasha O, Patel A, Esamai F, et al. The maternal and newborn health registry study of the global network for Women’s and children’s health research. Int J Gynaecol Obstet. 2012;118(3):190–193. doi: 10.1016/j.ijgo.2012.04.022. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Turner KE, Fuller S: Patient-Held Maternal and/or Child Health Records: Meeting the Information Needs of Patients and Healthcare Providers in Developing Countries? Online J Public Health Inform. 2011;3(2). doi:10.5210/ojphi.v3i2.3631. [DOI] [PMC free article] [PubMed]
- 62.Kihuba E, Gathara D, Mwinga S, Mulaku M, Kosgei R, Mogoa W, et al. Assessing the ability of health information systems in hospitals to support evidence-informed decisions in Kenya. Global Health Action. 2014;7:24859. doi: 10.3402/gha.v7.24859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Requejo JH, Bhutta ZA. The post-2015 agenda: staying the course in maternal and child survival. Arch Dis Child. 2015;100(Suppl 1):S76–S81. doi: 10.1136/archdischild-2013-305737. [DOI] [PubMed] [Google Scholar]
- 64.WHO . Global Strategy for Women’s, Children’s and Adolescents’ Health. Zero draft for consultation. Geneva: World Health Organization; 2015. [Google Scholar]
- 65.Bryce J, Arnold F, Blanc A, Hancioglu A, Newby H, Requejo J, et al. Measuring coverage in MNCH: new findings, new strategies, and recommendations for action. PLoS Med. 2013;10(5):e1001423. doi: 10.1371/journal.pmed.1001423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.World Health Organization . Bridging the “Know–Do” Gap, Meeting on Knowledge Translation in Global Health. Geneva: World Health Organization; 2005. [Google Scholar]
- 67.Pablos-Mendez A, Shademani R. Knowledge translation in global health. J Contin Educ Health Prof. 2006;26(1):81–86. doi: 10.1002/chp.54. [DOI] [PubMed] [Google Scholar]
- 68.Francke AL, Smit MC, de Veer AJ, Mistiaen P. Factors influencing the implementation of clinical guidelines for health care professionals: a systematic meta-review. BMC Med Inform Decis Mak. 2008;8:38. doi: 10.1186/1472-6947-8-38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 69.Blank A, Prytherch H, Kaltschmidt J, Krings A, Sukums F, Mensah N, et al. “Quality of prenatal and maternal care: bridging the know-do gap” (QUALMAT study): an electronic clinical decision support system for rural Sub-Saharan Africa. BMC Med Inform Decis Mak. 2013;13:44. doi: 10.1186/1472-6947-13-44. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 70.Necochea E, Tripathi V, Kim Y-M, Akram N, Hyjazi Y, da Luz Vaz M, et al. Implementation of the Standards-Based Management and Recognition approach to quality improvement in maternal, newborn, and child health programs in low-resource countries. Int J Gynecol Obstet. 2015;130(Supplement 2):S17–S24. doi: 10.1016/j.ijgo.2015.04.003. [DOI] [PubMed] [Google Scholar]
- 71.Braham DL, Richardson AL, Malik IS. Application of the WHO surgical safety checklist outside the operating theatre: medicine can learn from surgery. Clin Med. 2014;14(5):468–474. doi: 10.7861/clinmedicine.14-5-468. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72.Lau F, Kuziemsky C, Price M, Gardner J. A review on systematic reviews of health information system studies. J Am Med Inform Assoc. 2010;17(6):637–645. doi: 10.1136/jamia.2010.004838. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Main EK, Bingham D. Quality improvement in maternity care: promising approaches from the medical and public health perspectives. Curr Opin Obstet Gynecol. 2008;20(6):574–580. doi: 10.1097/GCO.0b013e3283184040. [DOI] [PubMed] [Google Scholar]
- 74.Osheroff JA, Teich JM, Middleton B, Steen EB, Wright A, Detmer DE. A roadmap for national action on clinical decision support. J Am Med Inform Assoc. 2007;14(2):141–145. doi: 10.1197/jamia.M2334. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Kawamoto, K, Houlihan, CA, Balas, EA, Lobach, DF. Improving clinical practice using clinical decision support systems: review of trials to identify features critical to success. BMJ (Clinical research ed). 2005;330(7494):765. [DOI] [PMC free article] [PubMed]
- 76.Zakane SA, Gustafsson LL, Tomson G, Loukanova S, Sié A, Nasiell J, et al. Guidelines for maternal and neonatal “point of care”: Needs of and attitudes towards a computerized clinical decision support system in rural Burkina Faso. Int J Med Inform. 2014;83(6):459–469. doi: 10.1016/j.ijmedinf.2014.01.013. [DOI] [PubMed] [Google Scholar]
- 77.Nair M, Yoshida S, Lambrechts T, Boschi-Pinto C, Bose K, Mason EM, et al. Facilitators and barriers to quality of care in maternal, newborn and child health: a global situational analysis through meta-review. BMJ Open. 2014;4(5):e004749. doi: 10.1136/bmjopen-2013-004749. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Fausett MB, Propst A, Van Doren K, Clark BT. How to develop an effective obstetric checklist. Am J Obstet Gynecol. 2011;205(3):165–170. doi: 10.1016/j.ajog.2011.06.003. [DOI] [PubMed] [Google Scholar]
- 79.Moja L, Kwag KH, Lytras T, Bertizzolo L, Brandt L, Pecoraro V, et al. Effectiveness of computerized decision support systems linked to electronic health records: a systematic review and meta-analysis. Am J Public Health. 2014;104(12):e12–22. doi: 10.2105/AJPH.2014.302164. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 80.Free C, Phillips G, Watson L, Galli L, Felix L, Edwards P, et al. The effectiveness of mobile-health technologies to improve health care service delivery processes: a systematic review and meta-analysis. PLoS Med. 2013;10(1):e1001363. doi: 10.1371/journal.pmed.1001363. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.MacLeod B, Phillips J, Stone AE, Walji A, Awoonor-Williams JK: The Architecture of a Software System for Supporting Community-based Primary Health Care with Mobile Technology: The Mobile Technology for Community Health (MoTeCH) Initiative in Ghana. Online J Public Health Inform. 2012; 4(1). doi:10.5210/ojphi.v4i1.3910. [DOI] [PMC free article] [PubMed]
- 82.Crawford J, Larsen-Cooper E, Jezman Z, Cunningham SC, Bancroft E. SMS versus voice messaging to deliver MNCH communication in rural Malawi: assessment of delivery success and user experience. Glob Health Sci Pract. 2014;2(1):35–46. doi: 10.9745/GHSP-D-13-00155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.The power of health in every mama’s hand [http://www.mobilemamaalliance.org/]. Accessed 15 Sept 2015.
- 84.Jennings L, Omoni A, Akerele A, Ibrahim Y, Ekanem E. Disparities in mobile phone access and maternal health service utilization in Nigeria: a population-based survey. Int J Med Inform. 2015;84(5):341–348. doi: 10.1016/j.ijmedinf.2015.01.016. [DOI] [PubMed] [Google Scholar]
- 85.Vashist SK, Mudanyali O, Schneider E, Zengerle R, Ozcan A. Cellphone-based devices for bioanalytical sciences. Anal Bioanal Chem. 2014;406(14):3263–3277. doi: 10.1007/s00216-013-7473-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Luhm KR, Cardoso MRA, Waldman EA. Vaccination coverage among children under two years of age based on electronic immunization registry in Southern Brazil. Rev Saude Publica. 2011;45(1):90–98. doi: 10.1590/S0034-89102010005000054. [DOI] [PubMed] [Google Scholar]
- 87.Jamtvedt G, Young JM, Kristoffersen DT, O'Brien MA, Oxman AD. Audit and feedback: effects on professional practice and health care outcomes. Cochrane Database Syst Rev (Online) 2006;2:Cd000259. doi: 10.1002/14651858.CD000259.pub2. [DOI] [PubMed] [Google Scholar]
- 88.Colquhoun HL, Brehaut JC, Sales A, Ivers N, Grimshaw J, Michie S, et al. A systematic review of the use of theory in randomized controlled trials of audit and feedback. Implement Sci. 2013;8:66. doi: 10.1186/1748-5908-8-66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Larson EL, Patel SJ, Evans D, Saiman L. Feedback as a strategy to change behaviour: the devil is in the details. J Eval Clin Pract. 2013;19(2):230–234. doi: 10.1111/j.1365-2753.2011.01801.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Ivers NM, Sales A, Colquhoun H, Michie S, Foy R, Francis JJ, et al. No more ‘business as usual’ with audit and feedback interventions: towards an agenda for a reinvigorated intervention. Implement Sci. 2014;9:14. doi: 10.1186/1748-5908-9-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Ivers N, Jamtvedt G, Flottorp S, Young JM, Odgaard-Jensen J, French SD, et al. Audit and feedback: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev (Online) 2012;6:Cd000259. doi: 10.1002/14651858.CD000259.pub3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Ivers NM, Grimshaw JM, Jamtvedt G, Flottorp S, O'Brien MA, French SD, et al. Growing literature, stagnant science? Systematic review, meta-regression and cumulative analysis of audit and feedback interventions in health care. J Gen Intern Med. 2014;29(11):1534–1541. doi: 10.1007/s11606-014-2913-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.van der Veer SN, de Keizer NF, Ravelli ACJ, Tenkink S, Jager KJ. Improving quality of care. A systematic review on how medical registries provide information feedback to health care providers. Int J Med Inform. 2010;79(5):305–323. doi: 10.1016/j.ijmedinf.2010.01.011. [DOI] [PubMed] [Google Scholar]
- 94.Carver CS, Scheier MF. Control theory: a useful conceptual framework for personality-social, clinical, and health psychology. Psychol Bull. 1982;92(1):111–135. doi: 10.1037/0033-2909.92.1.111. [DOI] [PubMed] [Google Scholar]
- 95.Kluger AN, DeNisi A. The effects of feedback interventions on performance: A historical review, a meta-analysis, and a preliminary feedback intervention theory. Psychol Bull. 1996;119(2):254–284. doi: 10.1037/0033-2909.119.2.254. [DOI] [Google Scholar]
- 96.Hysong SJ, Best RG, Pugh JA. Audit and feedback and clinical practice guideline adherence: making feedback actionable. Implement Sci. 2006;1:9. doi: 10.1186/1748-5908-1-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 97.Hysong SJ, Teal CR, Khan MJ, Haidet P. Improving quality of care through improved audit and feedback. Implement Sci. 2012;7:45. doi: 10.1186/1748-5908-7-45. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 98.Salam RA, Lassi ZS, Das JK, Bhutta ZA. Evidence from district level inputs to improve quality of care for maternal and newborn health: interventions and findings. Reprod Health. 2014;11(Suppl 2):S3. doi: 10.1186/1742-4755-11-S2-S3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 99.Hipgrave DB, Hort K. Dual practice by doctors working in South and East Asia: a review of its origins, scope and impact, and the options for regulation. Health Policy Plan. 2013;29(6):703–16. doi: 10.1093/heapol/czt053. [DOI] [PubMed] [Google Scholar]
- 100.Mendoza G, Okoko L, Konopka S, Jonas E. mHealth Compendium. Arlington: African Strategies for Health project, Management Sciences for Health; 2013. [Google Scholar]
- 101.Shieshia M, Noel M, Andersson S, Felling B, Alva S, Agarwal S, et al. Strengthening community health supply chain performance through an integrated approach: Using mHealth technology and multilevel teams in Malawi. J Glob Health. 2014;4(2):020406. doi: 10.7189/jogh.04.020406. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 102.Management Sciences for Health . Systems for Improved Access to Pharmaceuticals and Services (SIAPS) Program. Considerations for the Integration of HMIS and LMIS. Arlington: Management Sciences for Health; 2014. [Google Scholar]
- 103.GSMA . Mobile Financial Services for the Unbanked. State of the Industry 2014. London: GSMA; 2014. [Google Scholar]
- 104.Muzzi M. UNICEF Good Practices in Integrating Birth Registration into Health Systems (2000–2009); Case Studies: Bangladesh, Brazil, the Gambia and Delhi, India. New York: UNICEF; 2009. [Google Scholar]
- 105.Phillips DE, Lozano R, Naghavi M, Atkinson C, Gonzalez-Medina D, Mikkelsen L, et al. A composite metric for assessing data on mortality and causes of death: the vital statistics performance index. Popul Health Metr. 2014;12:14. doi: 10.1186/1478-7954-12-14. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.World Bank, USAID and WHO . Health Measurement and Accountability Post 2015: Five-Point Call to Action. Washington, DC: MA4Health; 2015. [Google Scholar]
- 107.WHO . World Health Assembly Resolution 58.28: eHealth. Geneva: World Health Organization; 2005. [Google Scholar]
- 108.Brooke EM. The current and future use of registers in health information systems. Geneva: World Health Organization; 1974. [Google Scholar]
- 109.Agency for Healthcare Research and Quality . Registries for Evaluating Patient Outcomes: A User’s Guide. 3. Rockville: Agency for Healthcare Research and Quality; 2014. [PubMed] [Google Scholar]