

Abstract
Congenital diaphragmatic hernia (CDH) is a known cause of secondary gastric volvulus. It is also known that bronchopulmonary sequestration (BPS) may be associated with CDH. An extremely rare case of BPS associated with gastric volvulus in a girl with left sided CDH is being reported.
KEY WORDS: Diaphragmatic hernia, eventration, gastric volvulus, pulmonary sequestration
INTRODUCTION
Gastric volvulus can be acute, acute on chronic or chronic, and may be primary or secondary to anomalies that affect the fixity of the stomach like hiatus hernia, eventration of diaphragm or congenital diaphragmatic hernia (CDH). The association of bronchopulmonary foregut malformations such as congenital cystic adenomatoid malformation of lung and bronchopulmonary sequestration (BPS) with CDH has also been well described in the literature. Herein, we describe a 4-year-old girl with a rare presentation of gastric volvulus and pulmonary sequestration in association with CDH.
CASE REPORT
A 4-year-old girl presented to our casualty with upper abdominal pain, distension, and nonbilious vomiting for the last two days. Her mother gave a history of recurrent episodes of similar symptoms every month for the last six months, and each episode lasted for 4-5 h.
The symptoms used to diminish spontaneously. Her perinatal history was unremarkable. A preliminary work up for her past symptoms in another hospital revealed that she had a suspected left sided eventration as seen on the chest X-ray [Figure 1a]. On examination, the child was lethargic, obtunded, had cold peripheries with tachycardia, hypotension, and feeble pulse. Her abdomen was distended, tense and tender especially in the upper half. A nasogastric tube insertion was attempted that failed initially but subsequently drained hemorrhagic gastric contents. A skiagram [Figure 1b] at this stage revealed a gastric bubble, with a paucity of distal bowel gas and a raised left hemi diaphragm.
Figure 1.
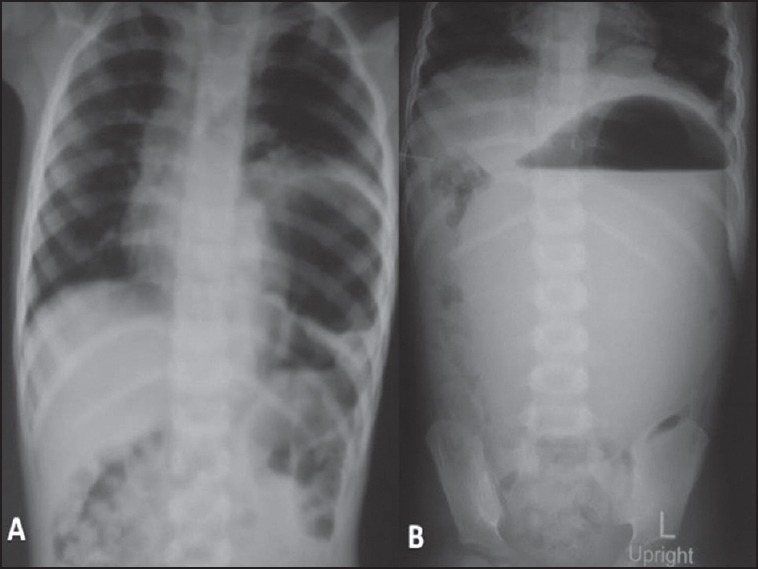
(a) Radiograph of the abdomen prior to presentation at our institute showing evidence of viscus in left hemithorax. (b) The radiograph when the child presented to us. Note the paucity of bowel gas excluding the single stomach gas shadow suggesting the possibility of a volvulus
After adequate resuscitation, the child was explored, and the intra-operative findings revealed a mesoaxial gastric volvulus. After successful reduction, it was noted that the stomach was grossly healthy except the greater curvature, which was congested. There was a large defect in the posterolateral aspect of the left hemi-diaphragm, which was covered with a sac and the diaphragm had a reasonably well-developed rim of muscle along the anterior segment [Figure 2a].
Figure 2.
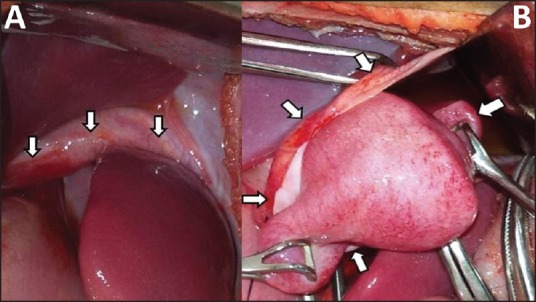
(a) Defect in the diaphragm is seen with well-defined anterior lip (arrows). (b) Intraoperative image of the mass seen to occupy the cranial aspect of the diaphragmatic hernia sac (cut edges indicated by arrows)
To repair the defect the sac was excised and it was noted that the cephalic surface of the sac had a lobular 6 cm × 3 cm fleshy pedicled mass flimsily attached to it [Figure 2b].
The pedicle of the blood supply was traced and it was found to be entering the mediastinum. The pedicle was separate from the inferior pulmonary ligament. The lung was well developed and was anatomically unrelated to the mass. The pedicle was ligated, and the mass excised and sent for histopathological examination. The repair was completed by primary interrupted sutures, and a three-point gastropexy was done to prevent recurrences. The child recovered uneventfully and is currently under our follow-up. The histopathology report of the mass indicated that it was an extra-pulmonary BPS.
DISCUSSION
The stomach is prevented from rotating along its axis by the ligamentous supports like the gastrocolic, gastrohepatic, gastrophrenic and the gastrosplenic ligaments. The gastroesophageal junction and the pylorus are two additional fixed points that afford protection against volvulus. When there is a laxity in these supports and the stomach rotates more than 180°, a primary gastric volvulus results. Other conditions like hiatus hernia and CDH predisposes to secondary volvulus. Based on the two axes along which this rotation takes place it could produce either an organo-axial, mesentero-axial or a mixed volvulus. It has been noted from the literature that the secondary gastric volvulus in children usually is associated with the mesentero-axial type of volvulus as was seen in our case.[1] An astute clinician can diagnose acute gastric volvulus by the typical complaint of sudden onset upper abdominal pain with retching and inability to pass a nasogastric tube-the Borchardt's triad.[2] This symptom complex was also present in our case except for retching, but the radiographs endorsed our clinical suspicion.
The exploration revealed a mass on the superior aspect of the sac, which looked like an extrapulmonary bronchopulmonary sequestration (EBPS). Excision of this structure was important to secure an uninterrupted smooth suture line. These are non-functional pulmonary tissues with the systemic blood supply that seldom communicate with the tracheobronchial tree. BPS comprise approximately 6% of all congenital malformations, and these are associated with CDH in 30-40% of cases.[3,4] Intralobar sequestrations are far more common and account for 75% of the sequestrations.[3] This distinction is made depending on whether or not the visceral pleura invests the sequestered lesion, with the latter referred to as EBPS.
Although the above associations with CDH are common but CDH presenting with acute gastric volvulus and with an underlying EBPS is very rare in pediatric age group and is described only once in English literature.[5] Brara et al. had reported a case similar to ours except that the child had an eventration of the diaphragm.[5] Another case report in Spanish describes an adult with Bochdalek's hernia with stomach volvulus and extrapulmonary sequestration presenting as acute respiratory distress.[6]
The aim of this report is to reinforce pediatric surgeons to look for underlying secondary causes of gastric volvulus as most of them can be tackled simultaneously. An awareness of this triad of CDH, gastric volvulus, and BPS can result in early detection and safe resection of BPS and thus avoid future diagnostic dilemmas.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Mayo A, Erez I, Lazar L, Rathaus V, Konen O, Freud E. Volvulus of the stomach in childhood: The spectrum of the disease. Pediatr Emerg Care. 2001;17:344–8. doi: 10.1097/00006565-200110000-00006. [DOI] [PubMed] [Google Scholar]
- 2.Rashid F, Thangarajah T, Mulvey D, Larvin M, Iftikhar SY. A review article on gastric volvulus: A challenge to diagnosis and management. Int J Surg. 2010;8:18–24. doi: 10.1016/j.ijsu.2009.11.002. [DOI] [PubMed] [Google Scholar]
- 3.Frazier AA, Rosado de Christenson ML, Stocker JT, Templeton PA. Intralobar sequestration: Radiologic-pathologic correlation. Radiographics. 1997;17:725–45. doi: 10.1148/radiographics.17.3.9153708. [DOI] [PubMed] [Google Scholar]
- 4.Grethel EJ, Farrell J, Ball RH, Keller RL, Goldstein RB, Lee H, et al. Does congenital diaphragmatic hernia associated with bronchopulmonary sequestration portend a better prognosis? Fetal Diagn Ther. 2008;23:250–3. doi: 10.1159/000123609. [DOI] [PubMed] [Google Scholar]
- 5.Brara BS, Rossiter M, Moore KA. Eventration of diaphragm with volvulus of stomach and extralobar sequestration of the lung. Proc R Soc Med. 1977;70:725–6. [PMC free article] [PubMed] [Google Scholar]
- 6.Carvajal Balaguera JJ, Mallagray Casas S, Peña Gamarra L, Gómez Maestro P, Monterde García G, Tello López I. Bochdalek's hernia in an adult with stomach volvulus and extrapulmonary sequestration. Arch Bronconeumol. 1995;31:287–9. [PubMed] [Google Scholar]