

Abstract
Background
Environmental contexts have been shown to predict health behaviours and outcomes either directly or via interaction with individual risk factors. In this paper, we created indexes of socioeconomic disadvantage (SEDI) and socioeconomic advantage (SAI) in Singapore to test the applicability of these concepts in an Asian context. These indices can be used for health service resource allocation, research and advocacy.
Methods
We used principal component analysis (PCA) to create SEDI and SAI using a structured and iterative process to identify and include influential variables in the final index. Data at the master plan geographical level was obtained from the most recent Singapore census 2010.
Results
The 3 areas with highest SEDI scores were Outram (120.1), followed by Rochor (111.0) and Downtown Core (110.4). The areas with highest SAI scores were Tanglin, River Valley and Newton. The SAI had 89.6% of variation explained by the final model, as compared to 67.1% for SEDI, and we recommend using both indices in any analysis.
Conclusion
These indices may prove useful for policy-makers to identify spatially varying risk factors, and in turn help identify geographically targeted intervention programs, which can be more cost effective to conduct.
Keywords: Principal component analysis, Socio-economic index, Small area health outcomes, Policy, Health care utilization, Asia
Highlights
-
•
Areal measures of socioeconomic status can help in resource allocation.
-
•
Our study creates such indices in an Asian context.
-
•
These indices can be used for health service research in Asian countries.
Introduction
In developed countries, various areal measures of socioeconomic status have been created, such as the Socio-Economic Indices for Australia (SEIFA) in Australia (Castles, 1994), Carstairs index in the UK (Carstairs, 1995, Morris and Carstairs, 1991), as well as indices in United States (Krieger et al., 1997) and New Zealand (Crampton et al., 1997). Such indices are useful to health practitioners and administrators for a number of reasons; mainly in the areas of resource allocation, research and advocacy. They can be used to determine funding formula for primary healthcare services, social services, relating socioeconomic status with health outcomes and risk factors/behaviours, as well as aid community-based service providers in terms of pricing and pitching the appropriate services for communities with different socioeconomic status. The use of such indices has not been studied in an Asian context where cultural norms and environmental contexts may significantly alter the usefulness of SEDI or SAI. We use Singapore as an example for testing the conceptual applicability of these indices in a highly urban, Asian setting.
In Australia, increasing geographical socioeconomic disadvantage has been shown to be positively associated with mortality as well as hospital admissions for acute coronary syndromes, lower rates of interventions such as angiographies and interventional angiographies (Beard et al., 2008). Geographical socioeconomic disadvantage has also been shown to be related to small-for-gestational age births (Beard et al., 2009), subjects who are overweight (van Lenthe and Mackenbach, 2002), children's mental health use (van der Linden et al., 2003), incidence of coronary heart disease (Sundquist et al., 2004), maternal depressive symptoms (Mulvaney and Kendrick, 2005) as well as risk factors for adverse health outcomes such as smoking (Duncan et al., 1999). However, there have also been negative findings in studies examining the association between neighbourhood deprivation and health outcomes. An English study found that the neighbourhood context in which a mother lives has no impact on the risk of gestational diabetes (Janghorbani et al., 2006), while another study found no effect of neighbourhood deprivation and health behaviours such as exercise levels among older people (Fox et al., 2011).
Individual and areal measures may also measure different aspects of socioeconomic status that may be positively or negatively correlated with health outcomes. For instance, two birth defect studies compared individually measured socioeconomic status (SES) with areal measures, and concluded that the effects of individual versus areal measures were mixed. One study found a significant effect of lower individual socioeconomic status and residence in an SES-lower neighbourhood on the occurrence of neural tube defects (Wasserman et al., 1998). On the other hand, a study of neural tube and facial clefts showed an increased risk for low SES households but not at the individual level (Croen and Shaw, 1995).
The motivation for this research came from our earlier attempt to model the association between individual items of socioeconomic status from the Singapore census with Out-of-Hospital Cardiac Arrests (OHCA) from a nation-wide registry (Ong et al., 2011). We found that demographic variables, but not individual socioeconomic variables, to be associated with OHCA, which was contrary to our initial hypothesis. We suspect this was due to a large number of individual variables included in the model, and highlighted the need for an index to measure areal disadvantage. Such an index has not been developed for Asian countries, and its applicability/validity therefore remains unproven. The aim of our study was therefore to create a small area socioeconomic disadvantage index (SEDI), as well as an index of socioeconomic advantage (SAI) for Singapore, and to assess the validity of such indices in an Asian socio-cultural context.
Materials and methods
We obtained socioeconomic data from the most recent Singapore census done in 2010. The Census of Population is conducted once in 10 years by the Singapore Department of Statistics, and data is based on a person's place of usual residence. To collect additional information not available from administrative sources, some 200,000 households were selected to participate in the sample enumeration via telephone, face-to-face interviews as well as the internet, and the census data was subjected to strict quality control checks and audits (Department of Statistics, Ministry of Trade and Industry, 2010).
For the purposes of our analysis, we used the following variables, which were indicative of socioeconomic status: housing type, highest educational level, literacy level, occupational categories, industries employed in, and personal and household income. For creating the SEDI index, we started with 23 variables, while for the SAI index, 11 variables were initially included. The SEDI has more variables mainly because there were more occupational categories for the lower socioeconomic group (Appendix 1).
The data was available at the Singapore Master Plan geographical boundary level, which is used by the Urban Redevelopment Plan (URA) authorities for town planning purposes. The URA, which is the government agency responsible for the urban planning of Singapore, released a geographical map of Singapore with demarcations of the various towns (also called master plan areas) in 2008 (Urban Redevelopment Authority, Singapore). The areal zones represented mainly residential areas (32 towns), as well as water catchment areas and smaller islands which are primarily used for commercial/army training purposes.
We used principal component analysis (PCA) to create the SEDI and SAI (Jollife, 1986). PCA is a data reduction technique that is used to summarise a large number of variables into a smaller group, collectively known as a principal component. A structured and iterative process was used to identify and include influential variables for inclusion in the final index as described below, mostly similar to that used in Australia (Statistics, 2006):
-
Step 1.
Initial variable list
For each index, we created an initial variable list, which was based on information available from the census stratified by the geographical master plan regions. These were variables that were areal measures of socioeconomic disadvantage/disadvantage
-
Step 2.
Creating variables
For each master plan, we computed variables as proportions. For instance, in Ang Mo Kio, we calculated the proportion of residents living in public housing 3 rooms or below. These proportions were then standardised to have a mean of 0 and standard deviation of 1. This was done to prevent variables with larger prevalence from having an undue influence on the overall index.
-
Step 3.
Removing correlated variables
Next, highly correlated variables were removed to prevent instability in the variable weights. Generally, when two variables had a correlation coefficient greater than |0.9|, we removed one of them. However, in cases where we hypothesised that two different aspects of socioeconomic status were being represented, e.g. proportion cleaners and labourers (education) with proportion with household income less than S$4000 (income), we included both variables.
-
Step 4.
Principal component analysis (PCA)
The next step involved conducting the PCA on the set of variables identified from above, to obtain the variable loading for each variable on the first principal component. We opted not to perform component rotation, as a previous paper had found limited usefulness in creating these indices (Australian Bureau of Statistics, 2006). The variable loading is essentially the correlation coefficient between each variable and the component.
-
Step 5.
Removing low loading variables
Starting from the variable with the lowest loading, we removed variables one at a time whenever their loading was below |0.2|. We used a threshold of 0.2 instead of 0.3 as suggested in the Australian model, in order to preserve known markers of socioeconomic status (such as proportion of people staying in a 3-room and below type of housing) in the model.
-
Step 6.
Standardising the indices
The first principal component score for each master plan area was derived by taking the product of each standardised variable with its respective weight, and then summing across all variables. We standardised the scores across all master plan areas in Singapore, to a mean of 100 and standard deviation of 10 for ease of presentation. Due to the small sample size, we also performed bootstrap analysis to calculate the bias-corrected 95% confidence intervals for the scores.
The above steps were undertaken to create both the SEDI and SAI. We also performed a range of sensitivity analyses by categorising the variables with the different categories, and examining model fit via computing the proportion of variation explained by the model. The final indices were then grouped into quartiles, and the results displayed in maps for ease of presentation. In order to validate the indices, we correlated our data with the Singapore Residential Price Index (SRPI) (Institute of Real Estate Studies, National University of Singapore, 2010), which contained non-landed private residential market capitalisation by value, stratified by postal districts. Data analysis was performed in Stata V11.0 (Stata Corp, College Station, Tx, USA), and level of significance set at 5%. Maps were created using Arc-GIS software (ArcGIS9, ESRI, Redlands, California).
Results
Singapore is an island state with a total land area of 700 km2. Based on the latest census data, Singapore's total population was 5.08 million as at end-June 2010, out of which there were 3.77 million Singapore residents. The areas with the largest group of Singapore residents are Bedok (294,500), followed by Jurong West (267,500) and Tampines (261,700), and areas like Sengkang, Jurong West and Punggol registering high rate of population growth between 2000 and 2010 (Department of Statistics, Ministry of Trade and Industry, 2010).
For the socioeconomic disadvantage index (SEDI), we started with 23 variables from the census (Appendix 1). Proportion working in the services sector was removed as it was highly negatively correlated with proportion working in the goods-producing industry (rho = − 1). Proportion working as production craftsmen and related workers was also removed because it was highly positively correlated with proportion working as plant & machine operators & assemblers (rho = 0.96).
After a series of principal component analyses, the number of variables was reduced to the following 12 variables, namely proportion: 1) living in public housing 3 rooms and below, 2) educational level primary and below, 3) illiterate, 4) unemployed, 5) working in construction industry, 6) working in hotels and restaurants, 7) clerical workers, 8) service and sales workers, 9) plant & machine operators & assemblers, 10) cleaners, labourers & related workers, 11) monthly personal income less than S$2500 and 12) household monthly income less than S$4000.
Collectively, the variables explained about 67.1% of the total variation. The areas with the 3 highest SEDI values were Outram (120.1), followed by Rochor (111.0) and Downtown Core (110.4) (Table 1). On the other end of the scale, areas with a lowest scores were Newton (79.0), followed by Tanglin (79.3) and River Valley (79.4) (Fig. 1).
Table 1.
Summary of socioeconomic disadvantage by planning areas.
| Planning Areas | SEDI | 95% CI | |
|---|---|---|---|
| Newton | 79 | 72.8 | 83.9 |
| Tanglin | 79.3 | 75.7 | 82.3 |
| River Valley | 79.4 | 74.5 | 78.8 |
| Bukit Timah | 79.8 | 74.5 | 83.4 |
| Pasir Ris | 90.7 | 75.7 | 95.8 |
| Bishan | 92.8 | 76.8 | 101.3 |
| Serangoon | 94.2 | 75.5 | 105.6 |
| Marine Parade | 94.5 | 74.9 | 109.4 |
| Novena | 96.3 | 66.6 | 107.1 |
| Choa Chu Kang | 97.6 | 72.8 | 108.5 |
| Tampines | 99.8 | 77.7 | 110.9 |
| Jurong East | 99.9 | 73.6 | 109.3 |
| Sengkang | 100.2 | 77.8 | 111.8 |
| Clementi | 100.3 | 77.2 | 117.9 |
| Bukit Batok | 100.6 | 79.6 | 112.8 |
| Sembawang | 100.8 | 74.5 | 111.8 |
| Bukit Panjang | 100.9 | 79.4 | 113.8 |
| Jurong West | 101.6 | 78.9 | 112.2 |
| Bedok | 102 | 78.2 | 121.8 |
| Woodlands | 102.7 | 83.7 | 121.0 |
| Hougang | 102.8 | 88.7 | 116.4 |
| Yishun | 105.6 | 80.4 | 122.0 |
| Changi | 106.3 | 97.3 | 122.8 |
| Queenstown | 106.9 | 97.0 | 122.7 |
| Toa Payoh | 107.2 | 97.6 | 119.4 |
| Ang Mo Kio | 107.9 | 97.4 | 121.8 |
| Geylang | 109.3 | 103.9 | 123.0 |
| Bukit Merah | 110.1 | 107.2 | 122.0 |
| Kallang | 110.1 | 102.0 | 121.7 |
| Downtown Core | 110.4 | 103.5 | 121.9 |
| Rochor | 111 | 107.0 | 119.7 |
| Outram | 120.1 | 78.7 | 122.0 |
Note: 95% CI denotes bias-corrected confidence intervals derived from bootstrap samples.
SEDI: socioeconomic disadvantage index.
Fig. 1.

Map of socioeconomic disadvantage in Singapore.
Our creation of the socioeconomic advantage index (SAI), began with 11 variables measuring a number of dimensions of socioeconomic well-being. Several variables were significantly associated with each other (e.g. education and personal income, rho = 0.99), but we opted to keep them in, as they were measuring different dimensions of SES. After several iterations of PCA, we were left with the following 9 variables, namely proportion: 1) polytechnic/degree education and above, 2) monthly household income more than S$8000, 3) monthly personal income more than S$6000, 4) literate, 5) working in financial services, 6) working in business services, 7) senior officers and managers, 8) professionals and 9) condominiums and landed properties. These variables accounted for a total of 89.6% of variation in the outcome. Further details on the PCA, including factor loadings, eigenvalues, etc are provided in Appendix 2.
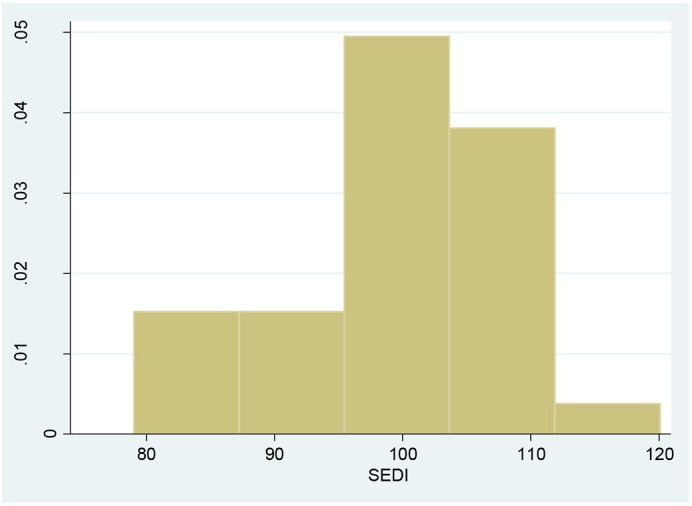
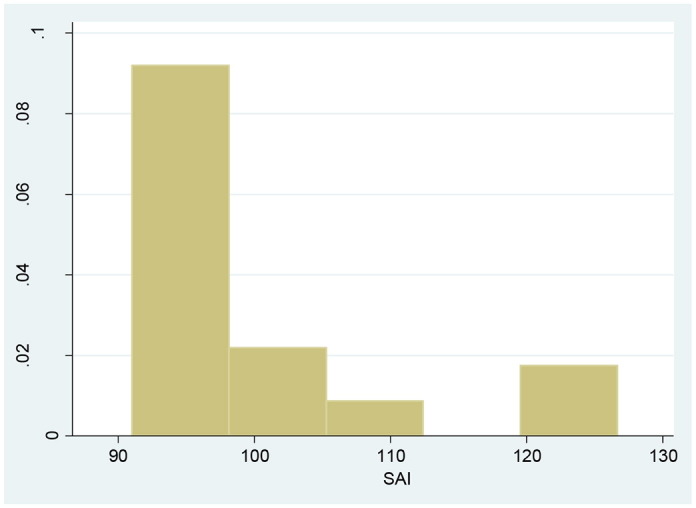
Areas with the top 3 SAI scores were Tanglin (126.7), River Valley (123.7) and Newton (123.5) (Table 2). On the other end of the scale, areas like Changi (91.0), Outram (91.5) and Rochor (93.1) scored the lowest, indicating lack of socioeconomic advantage (Fig. 2). Histograms of SEDI and SAI are provided in Appendix 3.
Table 2.
Summary of socioeconomic advantage by planning areas.
| Planning areas | SAI | 95% CI | |
|---|---|---|---|
| Tanglin | 126.7 | 118.9 | 134.1 |
| River Valley | 123.7 | 118.3 | 146.1 |
| Newton | 123.5 | 116.3 | 132.9 |
| Bukit Timah | 122.2 | 107.9 | 144.1 |
| Marine Parade | 107.4 | 100.2 | 125.4 |
| Novena | 105.8 | 94.5 | 149.9 |
| Bishan | 103.4 | 93.6 | 128.9 |
| Serangoon | 102.7 | 94.7 | 138.7 |
| Pasir Ris | 100.2 | 92.9 | 136.8 |
| Clementi | 99.5 | 93.5 | 134.1 |
| Bedok | 98.8 | 92.9 | 135.1 |
| Bukit Batok | 98 | 93.9 | 134.9 |
| Queenstown | 97.2 | 93.0 | 126.1 |
| Choa Chu Kang | 95.7 | 91.6 | 131.5 |
| Jurong East | 95.6 | 92.6 | 130.2 |
| Hougang | 95.5 | 90.9 | 122.7 |
| Tampines | 95.4 | 90.3 | 125.5 |
| Bukit Panjang | 95.2 | 88.2 | 110.2 |
| Toa Payoh | 95.1 | 90.0 | 105.2 |
| Ang Mo Kio | 95 | 90.7 | 120.0 |
| Downtown Core | 95 | 90.6 | 117.3 |
| Sembawang | 94.9 | 90.4 | 119.3 |
| Geylang | 94.4 | 91.1 | 105.4 |
| Kallang | 94.4 | 88.9 | 102.0 |
| Yishun | 94.3 | 90.5 | 99.4 |
| Bukit Merah | 94.3 | 89.9 | 103.1 |
| Jurong West | 93.5 | 89.1 | 101.0 |
| Sengkang | 93.5 | 88.9 | 97.9 |
| Woodlands | 93.3 | 90.7 | 95.2 |
| Rochor | 93.1 | 91.0 | 94.4 |
| Outram | 91.5 | 91.5 | 91.5 |
| Changi | 91 | 90.7 | 90.7 |
Note: 95% CI denotes bias-corrected confidence intervals derived from bootstrap samples.
SAI: socioeconomic advantage index.
Fig. 2.

Map of socioeconomic advantage in Singapore.
For both indices, we performed several sensitivity analyses to assess whether the findings would differ if we had used different cut-offs for the income data, and inclusion/exclusion of categories within each variable. For SEDI, when we varied personal income (< S$2000 and < S$3000) and household income (< S$2000 and < S$3000), we found that the model only accounted for up to 66.3% of variation in data, as compared to the original 67.1%. When we substituted with 1–2 room flats and secondary education and below, the proportion was lower at 66.1% and 66.3% respectively. Similarly for SAI, there were marginal differences in the proportion of variation explained by the model when we varied household and personal income. Substituting with university education and 5 rooms and above resulted in poorer performances of the model (proportion of variation 89.2% versus 80.1% respectively).
There was a moderately strong negative correlation between SEDI and market capitalisation (rho = − 0.63, p < 0.001), as well as a positive correlation between SAI and market capitalisation (rho = 0.69, p < 0.001), indicating that our indices are fairly robust in terms of measuring socioeconomic status of regions in Singapore (Fig. 3).
Fig. 3.

Private market capitalisations (in S$000) by DGP.
Discussion
We believe that indices of socioeconomic disadvantage as well as advantage have not been created before in Asia, and our research bridges this gap in the literature by demonstrating the applicability of such indices in an Asian socio-cultural context. Publishing the data as well as maps will allow other local researchers to use this data in the analysis of disease outcomes as well as risk factors for disease. We expect that these indices may be useful in analyses of healthcare utilisation and resource allocation in similar dense metropolitan settings in Asia. Other indices such as the Townsend, Carstairs and SEIFA also make use of similar data reduction techniques such as the PCA, but have included different items available from their census data, depending on differing geographical and cultural needs. The following is a hypothetical example of the application of our indices to health service delivery in Singapore.
Hypothetical application of SEDI and SAI
Participants of the national Health Promotion Board's various health screening activities (e.g. breast cancer, diabetes, and hypertension) can have their residential addresses geocoded onto the Singapore master plan regions. Suppose, we find that residents from Changi and Bukit Merah have a relatively higher risk of non-participation based on a spatial analysis. Let us also assume that a subsequent correlation was found with our indices of socioeconomic status. This provides useful evidence to policy-makers in two areas. Firstly, they can geographically target these two areas to improve on the uptake of future health screening activities. Secondly, they can rank and prioritise areas according to their socioeconomic score, so as to maximize their outreach programmes. This is especially useful when resources are limited and programmes may need to be implemented over a course of time.
We would like to add a word of caution in the interpretation of these indices. It should be noted that these scores reflect the disadvantage of areas that individuals reside in, rather than the individuals themselves. We did not include demographic variables such as age, sex and race in creating the disadvantage index, although these were available in the census data. The main reasons were because these are not directly amenable to change or influence, and were also not direct markers of deprivation (Australian Bureau of Statistics, 2006). We analysed data at a relatively large areal level, when compared to the Australian data. It would have been ideal to analyse or create the indices at a finer postal code level. However, such data is not made available to researchers in Singapore. Thus, it is unlikely that the heterogeneity within each planning area can be demonstrated in our data. We have used the aggregated household income data in our analysis, but are unable to account for varying household needs (e.g. differing family size) in the model as we do not have access to the individual level census data.
Our sensitivity analyses showed that the models did not improve when we considered alternative cut-offs for personal and household income levels for both indices. Based on the latest household expenditure survey (Department of Statistics, Ministry of Trade and Investment, 2009), around 41% of households had household income of less than S$4000, which was the cut-off we used in our study, and the average monthly household expenditure was about S$3760. Changes to the categories included for the other variables like education and housing type also did not significantly change the findings.
We created two different indices that purportedly measure different aspects of socioeconomic well-being. The SEDI was created to measure socioeconomic disadvantage, while the SAI measures socioeconomic advantage. Despite the high negative correlation of − 0.807 (Spearman correlation coefficient) between the two variables, a lack of disadvantage does not necessarily equate to advantage. We would recommend that investigators include both indices in their analysis, and let the data decide the relative contribution of each index. Due to the non-linear distribution, we also recommend that these indices be categorised into quartiles or quintiles in the analysis, depending on the aim of the study and nature of data available.
Conclusion
We have successfully created indices to measure areal levels of socioeconomic disadvantage as well as advantage for Singapore, and have demonstrated their potential applicability in an Asian context. These indices can be used by clinicians and researchers, who can study the associations between morbidity and mortality of diseases as well as risk factors with socioeconomic status. In turn, this will help in resource allocation and geographically targeted health education/intervention programmes.
Conflict of interest
The authors declare that there are no conflict of interests.
Authors' contributions
AE, MEHO and JT contributed towards the conceptualisation of the study, design, analysis and writing of manuscript. NS created the maps and helped with data collection and data analysis. AC and WW contributed towards manuscript writing.
Appendix 1. Variables initially included in the construct of the SEDI and SAI indices
| Number | SEDI | SAI |
|---|---|---|
| 1 | Proportion living in HDB 3-room and below | Proportion polytechnic/university education and above |
| 2 | Proportion of students with primary education and below | Proportion living in condominium and landed properties |
| 3 | Proportion not literate | Proportion monthly household income more than S$8000 |
| 4 | Proportion unemployed | Proportion monthly personal income more than S$6000 |
| 5 | Proportion economically inactive | Proportion literate |
| 6 | Proportion primary education and below | Proportion working |
| 7 | Proportion goods-producing industry | Proportion in financial services industry |
| 8 | Proportion manufacturing industry | Proportion in business services industry |
| 9 | Proportion construction industry | Proportion senior officers and managers |
| 10 | Proportion other goods industry | Proportion working as professionals |
| 11 | Proportion services-producing industry | Proportion house owners |
| 12 | Proportion wholesale and retail trade | |
| 13 | Proportion hotels and restaurants industry | |
| 14 | Proportion transport and communications industry | |
| 15 | Proportion clerical workers | |
| 16 | Proportion service and sales workers | |
| 17 | Proportion agricultural and fisheries workers | |
| 18 | Proportion production craftsmen & related workers | |
| 19 | Proportion plant & machine operators & assemblers | |
| 20 | Proportion cleaners, labourers & related workers | |
| 21 | Proportion house tenants | |
| 22 | Proportion monthly personal income less than S$2500 | |
| 23 | Proportion monthly household income less than S$4000 |
SEDI: socioeconomic disadvantage index, SAI: socioeconomic advantage index.
Appendix 2. Factor loadings, eigenvalues and variance explained for the final models (SEDI and SAI)
| Factors | Loadings | Eigenvalues | Proportion variance |
|---|---|---|---|
| SEDI | |||
| Proportion living in public housing 3 rooms and below | 0.2561 | 8.0544 | 0.6712 |
| Proportion illiterate | 0.3271 | 1.6508 | 0.1376 |
| Proportion unemployed | 0.2658 | 0.9996 | 0.0833 |
| Proportion educational level primary and below | 0.3496 | 0.6331 | 0.0528 |
| Proportion working in construction industry | 0.2290 | 0.3237 | 0.0270 |
| Proportion working in hotels and restaurants | 0.2995 | 0.1643 | 0.0137 |
| Proportion clerical workers | 0.2273 | 0.0767 | 0.0064 |
| Proportion service and sales workers | 0.2324 | 0.0516 | 0.0043 |
| Proportion plant & machine operators & assemblers | 0.2062 | 0.0205 | 0.0017 |
| Proportion cleaners, labourers & related workers | 0.3374 | 0.0179 | 0.0015 |
| Proportion monthly personal income less than S$2500 | 0.3353 | 0.0044 | 0.0004 |
| Proportion household monthly income less than S$4000 | 0.3433 | 0.0029 | 0.0002 |
| SAI | |||
| Proportion polytechnic/degree education and above | 0.3504 | 8.0600 | 0.8956 |
| Proportion condominiums and landed properties | 0.3448 | 0.5540 | 0.0616 |
| Proportion monthly household income more than S$8000 | 0.3478 | 0.1881 | 0.0209 |
| Proportion monthly personal income more than S$6000 | 0.3489 | 0.1208 | 0.0134 |
| Proportion literate | 0.2541 | 0.0375 | 0.0042 |
| Proportion working in financial services | 0.3351 | 0.0232 | 0.0026 |
| Proportion working in business services | 0.3194 | 0.0114 | 0.0013 |
| Proportion working as senior officers and managers | 0.3459 | 0.0038 | 0.0004 |
| Proportion working as professionals | 0.3422 | 0.0013 | 0.0001 |
Appendix 3. Distribution of SEDI and SAI
References
- Australian Bureau of Statistics . Socio-Economic Indexes for Areas (SEIFA)—Technical Paper Report No. 2039.0.55.001. 2006. [Google Scholar]
- Beard J.R., Earnest A., Morgan G. Socioeconomic disadvantage and acute coronary events: a spatiotemporal analysis. Epidemiology. 2008;19:485–492. doi: 10.1097/EDE.0b013e3181656d7f. [DOI] [PubMed] [Google Scholar]
- Beard J.R., Lincoln D., Donoghue D. Socioeconomic and maternal determinants of small-for-gestational age births: patterns of increasing disparity. Acta Obstet. Gynecol. Scand. 2009;88:575–583. doi: 10.1080/00016340902818170. [DOI] [PubMed] [Google Scholar]
- Carstairs V. Deprivation indices: their interpretation and use in relation to health. J. Epidemiol. Community Health. 1995;49(Suppl. 2):S3–S8. doi: 10.1136/jech.49.suppl_2.s3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Castles I. Information Paper. Australian Bureau of Statistics; Canberra: 1994. 1991 Census Socio-Economic Indexes for Areas. [Google Scholar]
- Crampton P., S.C., Sutton F. NZDep91: a new index of deprivation. Soc. Policy J. N. Z. 1997;9:186–193. [Google Scholar]
- Croen L.A., Shaw G.M. Young maternal age and congenital malformations: a population-based study. Am. J. Public Health. 1995;85:710–713. doi: 10.2105/ajph.85.5.710. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Department of Statistics, Ministry of Trade and Industry . Advance Census Release. Aug 2010. Census of Population 2010. [Google Scholar]
- Department of Statistics, Ministry of Trade and Investment . Report on the Household Expenditure Survey 2007/08. 2009. [Google Scholar]
- Duncan C., Jones K., Moon G. Smoking and deprivation: are there neighbourhood effects? Soc. Sci. Med. 1999;48:497–505. doi: 10.1016/s0277-9536(98)00360-8. [DOI] [PubMed] [Google Scholar]
- Fox K.R., Hillsdon M., Sharp D. Neighbourhood deprivation and physical activity in UK older adults. Health Place. 2011;17(2):633–640. doi: 10.1016/j.healthplace.2011.01.002. [DOI] [PubMed] [Google Scholar]
- Institute of Real Estate Studies, National University of Singapore . 2010. The Singapore Residential Price Index (SRPI) White Paper. [Google Scholar]
- Janghorbani M., Stenhouse E.A., Jones R.B., Millward B.A. Is neighbourhood deprivation a risk factor for gestational diabetes mellitus? Diabet. Med. 2006;23:313–317. doi: 10.1111/j.1464-5491.2006.01774.x. [DOI] [PubMed] [Google Scholar]
- Jollife I. Springer Verlag; New York: 1986. Principal Component Analysis. [Google Scholar]
- Krieger N., Williams D.R., Moss N.E. Measuring social class in US public health research: concepts, methodologies, and guidelines. Annu. Rev. Public Health. 1997;18:341–378. doi: 10.1146/annurev.publhealth.18.1.341. [DOI] [PubMed] [Google Scholar]
- Morris R., Carstairs V. Which deprivation? A comparison of selected deprivation indexes. J. Public Health Med. 1991;13:318–326. [PubMed] [Google Scholar]
- Mulvaney C., Kendrick D. Depressive symptoms in mothers of pre-school children—effects of deprivation, social support, stress and neighbourhood social capital. Soc. Psychiatry Psychiatr. Epidemiol. 2005;40:202–208. doi: 10.1007/s00127-005-0859-4. [DOI] [PubMed] [Google Scholar]
- Ong M.E., Earnest A., Shahidah N., Ng W.M., Foo C., Nott D.J. Spatial variation and geographic-demographic determinants of out-of-hospital cardiac arrests in the city-state of Singapore. Ann. Emerg. Med. 2011;58(4):342–351. doi: 10.1016/j.annemergmed.2010.12.014. [DOI] [PubMed] [Google Scholar]
- Singapore, U.R.A. Singapore Master Plan 2008. http://www.ura.gov.sg/MP2008/intro.htm (Accessed 27 July 2011)
- Sundquist K., Malmstrom M., Johansson S.E. Neighbourhood deprivation and incidence of coronary heart disease: a multilevel study of 2.6 million women and men in Sweden. J. Epidemiol. Community Health. 2004;58:71–77. doi: 10.1136/jech.58.1.71. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van der Linden J., Drukker M., Gunther N., Feron F., van Os J. Children's mental health service use, neighbourhood socioeconomic deprivation, and social capital. Soc. Psychiatry Psychiatr. Epidemiol. 2003;38:507–514. doi: 10.1007/s00127-003-0665-9. [DOI] [PubMed] [Google Scholar]
- Van Lenthe F.J., Mackenbach J.P. Neighbourhood deprivation and overweight: the GLOBE study. Int. J. Obes. Relat. Metab. Disord. 2002;26:234–240. doi: 10.1038/sj.ijo.0801841. [DOI] [PubMed] [Google Scholar]
- Wasserman C.R., Shaw G.M., Selvin S., Gould J.B., Syme S.L. Socioeconomic status, neighborhood social conditions, and neural tube defects. Am. J. Public Health. 1998;88:1674–1680. doi: 10.2105/ajph.88.11.1674. [DOI] [PMC free article] [PubMed] [Google Scholar]